Introduction
Anthracycline agents are effective drugs utilized
for a variety of solid and haematological malignancies (1,2).
Anthracyclines significantly improve the overall 5-year survival
(>80%) in pediatric cancers (3,4).
Nevertheless, anthracyclines are capable of inducing short- and
long-term cardiotoxicity (2,5). In the clinic, anthracycline-induced
cardiotoxicity (AIC) is characterized as ventricular dysfunction
with no symptoms in ≤57% of patients, and clinical heart failure
after cardiomyopathy in ≤16% of the patients (3,6,7). In general, the risk of developing AIC is
closely linked to the cumulative dose of anthracyclines (8,9).
Furthermore, other factors such as age and gender may also
contribute to the occurrence of AIC (1). Once patients exhibit symptoms of cardiac
failure, reversal of the condition via termination of anthracycline
therapy may become impossible (10).
Thus, it is important to detect AIC as early as possible (9). Multiple studies have demonstrated that
B-type natriuretic peptide (BNP), a neurohormone secreted in the
cardiac ventricles, reflect left ventricular (LV) end diastolic
pressure and pulmonary capillary wedge pressure, and may
independently predict AIC (1,11).
BNP, originally observed in extracts of porcine
brain, belongs to the family of natriuretic peptides (NPs), and
possesses the ability to promote diuresis, natriuresis,
vasodilatation and repress the renin-angiotensin-aldosterone system
(RAAS) (12). BNP regulates
homeostasis of water and salt excretion, and maintains blood
pressure largely through suppressing the RAA axis and damaging the
cardiac sympathetic nerve activity (13). Measurement of NPs has been widely
utilized for the detection and monitoring of patients with systolic
dysfunction (14,15). As an important member of NPs, BNP is
found up-regulated in a number of cardiac pathologies related to
hemodynamic overload and elevated cardiac fibrosis (16–18). In
addition, serum BNP levels are increased in patients with
symptomatic LV dysfunction, indicating that BNP may be linked to
the prognosis of heart failure (19).
In recent years, serum BNP level was demonstrated to have relevance
to the pathogenesis of AIC (9,11). BNP is
secreted by ventricular cardiac cells and released into the blood
in response to myocardial stretch, ventricular dilatation and
increased pressure load of LV chambers, which are influenced by LV
diastolic dysfunction (20–22). Elevated synthesis of BNP may be
stimulated by myocardial ischemia, LV wall tension and pressure
overload, all of which could reflect alterations in ventricular
function in heart failure patients (23–25). On
the other hand, anthracyclines cause degeneration of ventricular
muscles and consequently exhibit characteristics of congestive
heart failure (26). More notably,
anthracyclines can induce myocardial ischemia and increase pressure
load (8). From these aspects, it is
rational to postulate that serum BNP levels may be associated with
AIC. Previous studies investigated the impact of serum BNP levels
on the detection and prognosis of AIC, but their findings are
contradictory (8,25), the present study endeavored to use a
meta-analysis approach to examine the clinical value of serum BNP
levels on the prediction and management of AIC.
Materials and methods
Search strategy
Relevant studies were identified by searching the
medical literature databases China National Knowledge
Infrastructure (CNKI; available from www.cnki.net),
Web of Science (available from webofknowledge.com), PubMed (available from www.ncbi.nlm.nih.gov/pubmed), Google Scolar
(available from scholar.google.com and China BioMedicine (CBM;
available from www.sinomed.ac.cn) databases. The following key terms
were used for the systematic search: (‘Anthracyclines’ or
‘Anthracycline cardiotoxicity’ or ‘Anthracycline’ or ‘Anthracycline
antibiotics’ or ‘Anthracycline-induced cardiotoxicity’ or
‘Anthracycline-Induced Cardiomyopathy’ or ‘anthracycline-induced
cardiac toxicity’) and (‘Natriuretic Peptide, Brain’ or ‘BNP 32’ or
‘Nesiritide’ or ‘Type B Natriuretic Peptide’ or ‘B Type Natriuretic
Peptide’ or ‘BNP’ or ‘B-Type Natriuretic Peptide’ or ‘Brain
Natriuretic Peptide 32’ or ‘Natrecor’ or ‘pro-brain natriuretic
peptide (1–76)’ or ‘N-terminal pro-BNP’ or ‘proBNP (1–76)’ or
‘NTproBNP’ or ‘NT-BNP’ or ‘Amino-terminal pro-brain natriuretic
peptide’ or ‘NT-pro-BNP’ or ‘aminoterminal pro-B-type natriuretic
peptide’ or ‘pro-B-type natriuretic peptide’ or ‘N-Terminal
Pro-B-Type Natriuretic Peptide’ or ‘Brain Natriuretic Peptide’). No
language restrictions were imposed in the current meta-analysis.
Other potentially relevant studies were also identified by a manual
search of the reference list of original reports.
Selection criteria
The following criteria were used to select published
articles in our present meta-analysis: i) Human-associated
case-control studies focused on the relationship between the serum
levels of BNP and AIC; ii) sufficient information on the serum
levels of BNP and sample number must be supplied; iii) the article
must be published with full text. By contrast, published articles
were excluded based upon at least one of the following reasons: i)
Articles did not satisfy the inclusion criteria of the current
study; ii) studies were letters, reviews and meta-analyses; iii)
articles were duplication publications or had overlapping data.
After careful reexamination with the search strategy and
inclusion/exclusion criteria, only the most recent or complete
studies were included in the current meta-analysis.
Data extraction and quality
assessment
In order to enhance the credibility and reduce bias,
the following relevant data were extracted from each included
study: i) Baseline demographics: Year of publication, surname and
initials of the first author, country and ethnicity of publication;
ii) Participants: Number of cases and controls, sample size, gender
and age of subjects and iii) Detection method of serum BNP
levels.
The Newcastle-Ottawa Scale (NOS), was used as the
criteria for assessment of study quality (27). The NOS criteria were scored based on
three perspectives: Subject selection (0–4); comparability of
subject (0–2) and clinical outcome (–3). Total NOS scores ranged
from 0 (lowest) to 9 (highest). The included studies were viewed as
high quality when score was ≥7. Additional reassessment was
performed by authors to resolve discrepancies on NOS scores.
Statistical analysis
The STATA statistical software (Version 12.0, Stata
Corporation, College Station, TX, USA) was used for all analyses in
this meta-analysis. The association between the serum levels of BNP
and AIC was estimated by summary standardized mean difference (SMD)
with 95% confidence intervals (CIs). Statistical significance of
pooled SMDs was estimated by the Z test, the heterogeneity among
studies was quantified by Cochran's Q-statistic and I2
tests (28). If the Q-test showed
P<0.05 or I2 test exhibited >50%, indicating
significant heterogeneity, random effects model was applied,
otherwise fixed-effects model was conducted in case of no
statistical heterogeneity (29,30). In
addition, subgroup analyses were performed on the basis of
ethnicity and method to explore potential explanatory variables for
the association between the serum levels of BNP and AIC.
Sensitivity analysis was conducted to assess the stability of the
present study. To reveal possible publication bias, the funnel plot
and Egger's linear regression test were performed (31,32). All
tests were two-sided and a P-value <0.05 was considered to
indicate a statistically significant difference.
Results
Description and characteristics of
included studies
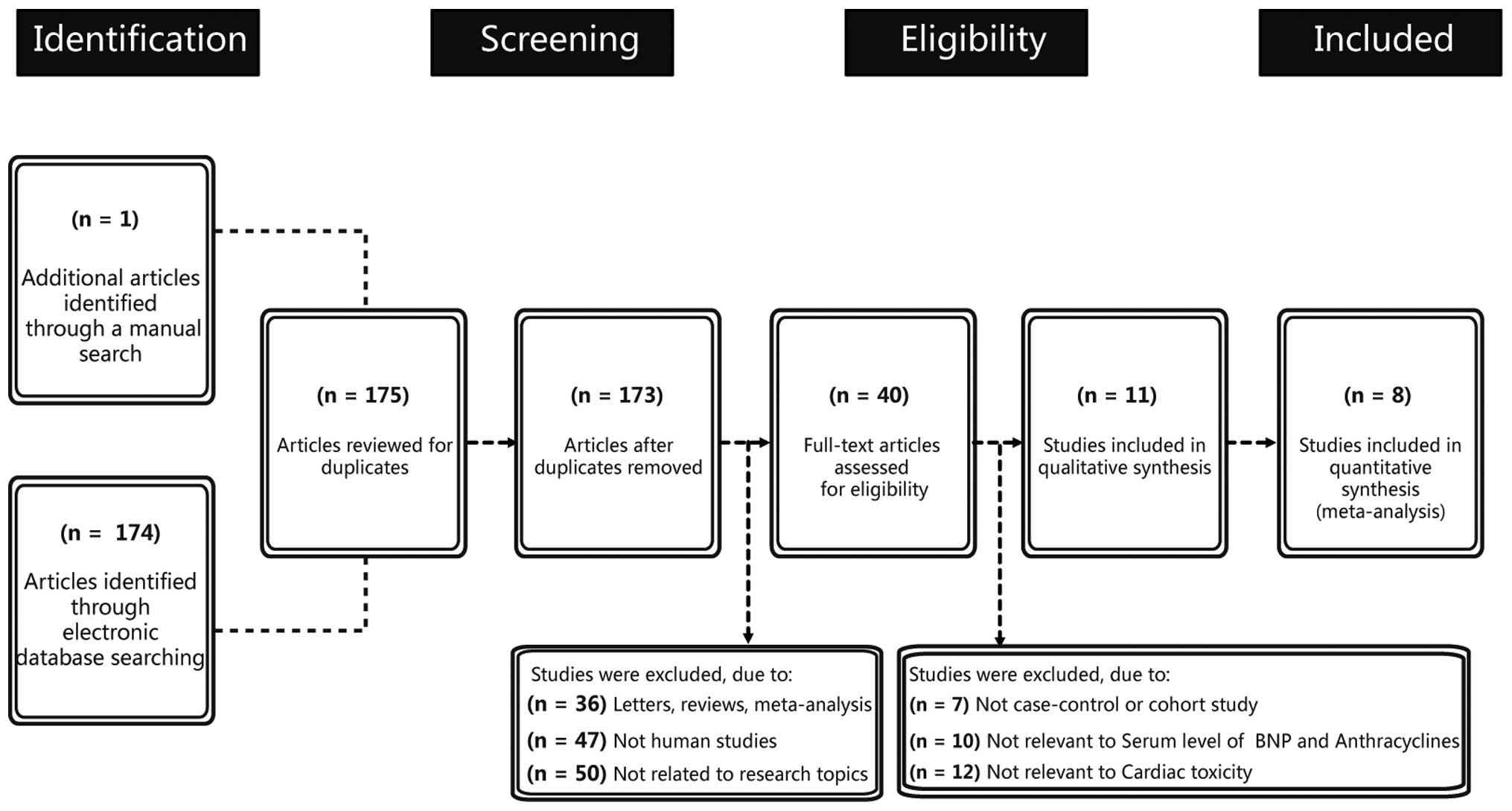
Figure 1 presents the
study selection process and the reasons for exclusion. Initially, a
combination of electronic database search and manual search
resulted in 175 articles being retrieved. At the screening stage,
two articles were excluded due to duplication and 133 articles were
excluded because of the article types (letters, reviews and
meta-analyses), if they were not human studies and if they were not
related to research topics. Subsequently, another 29 articles were
excluded because they were not case-control or cohort studies, or
not relevant to serum level of BNP and anthracyclines or not
relevant to cardiac toxicity. Finally, three articles with
incomplete data were excluded. The remaining 8 articles met all the
inclusion criteria and the studies were, published between 2001 and
2014, with moderate-high study quality (1,8–11,33–35).
Table I shows the basic
characteristics of included studies on the BNP serum level. The
eight cohort studies contained 126 AIC patients and 569 normal
participants, with sample size varying from 5–312 participants.
Five studies were performed in Asian individuals with two in China,
one each in Korea, Thailand and Japan. Three studies were performed
in the Caucasian population, with one each in Denmark, Italy and
USA. Two studies (Skovgaard D; Cao S) lacked gender information and
three studies (Skovgaard D, Lee HS, Aggarwal S) lacked age
information. The detection methods included enzyme multiplied
immunoassay technique (EMIT), chemiluminescence technology (CIT),
indirect immunofluorescence (IFT), fluorescence immunoassay
analysis (FIA), chemiluminescence immunoassay (CLIA) and
radioimmunoassay (RIA). The follow-up time was 3, 4, 18, 48 and 96
weeks. The serum BNP level of cardiotoxic patients and normal
participants were expressed as the mean ± standard deviation.
 | Table I.Characteristics of included studies
focused on serum level of BNP. |
Table I.
Characteristics of included studies
focused on serum level of BNP.
|
| Post-treatment serum
level of BNP |
|
|---|
|
|
|
|
|---|
|
|
| Sample size, n | Gender, M/F | Age, years |
|
| Cardiotoxic,
pg/ml | Normal, pg/ml |
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|---|
| First author,
year | Ethnicity | Case | Control | Case | Control | Case | Control | Method | Follow
upa | N | Mean | SD | N | Mean | SD | Refs |
|---|
| Skovgaard et
al, 2014 | Caucasian | 21 | 312 | – | – | – | – | EMIT | – | 21 | 267.80 | 107.00 | 312 |
41.30 |
4.00 | (11) |
| Cao et al,
2013 | Asian | 11 | 35 | – | – | 18–70 |
| ECIA | 3 | 11 | 102.00 |
74.00 | 35 |
69.00 |
54.00 | (35) |
| Cao et al,
2013 | Asian | 11 | 35 | – | – |
|
|
| 18 | 11 | 107.00 |
56.00 | 35 |
58.00 |
35.00 | (35) |
| Pongprot et
al, 2012 | Asian | 5 | 25 | 18/12 |
| 10±4 |
| CIT | – | 5 | 363.50 |
78.30 | 25 | 148.80 | 173.20 | (9) |
| Zhang et al,
2011 | Asian | 12 | 38 |
0/12 |
0/38 | 33–62 |
| IFT | 3 | 12 | 102.00 |
75.00 | 38 |
69.00 |
56.00 | (35) |
| Zhang et al,
2011 | Asian | 12 | 38 |
0/12 |
0/38 | 33–62 |
| IFT | 18 | 12 | 107.00 |
57.00 | 38 |
59.00 |
36.00 | (35) |
| Feola et al,
2011 | Caucasian | 13 | 40 |
1/52 |
| 28–73 |
| FIA | 4 | 13 |
94.30 | 166.20 | 40 |
47.10 |
45.30 | (8) |
| Feola et al,
2011 | Caucasian | 13 | 40 |
1/52 |
| 28–73 |
| FIA | 48 | 13 | 111.30 | 186.20 | 40 |
36.90 |
33.80 | (8) |
| Feola et al,
2011 | Caucasian | 13 | 40 |
1/52 |
| 28–73 |
| FIA | 96 | 13 | 107.50 | 169.10 | 40 |
38.70 |
39.40 | (8) |
| Lee et al,
2008 | Asian | 19 | 67 | 49/37 |
| – | – | CLIA | – | 19 | 305.80 |
21.44 | 67 |
64.20 |
13.36 | (1) |
| Aggarwal et
al, 2007 | Caucasian | 37 | 26 | 11/15 | 26/11 | – | – | CLIA | – | 26 |
23.40 |
25.30 | 37 |
14.20 |
8.90 | (34) |
| Hayakawa et
al, 2001 | Asian | 8 | 26 | 18/16 |
| 6.9±20.2 | 0.7±21.7 | RIA | – | 8 |
29.00 |
31.20 | 26 |
9.00 |
14.80 | (10) |
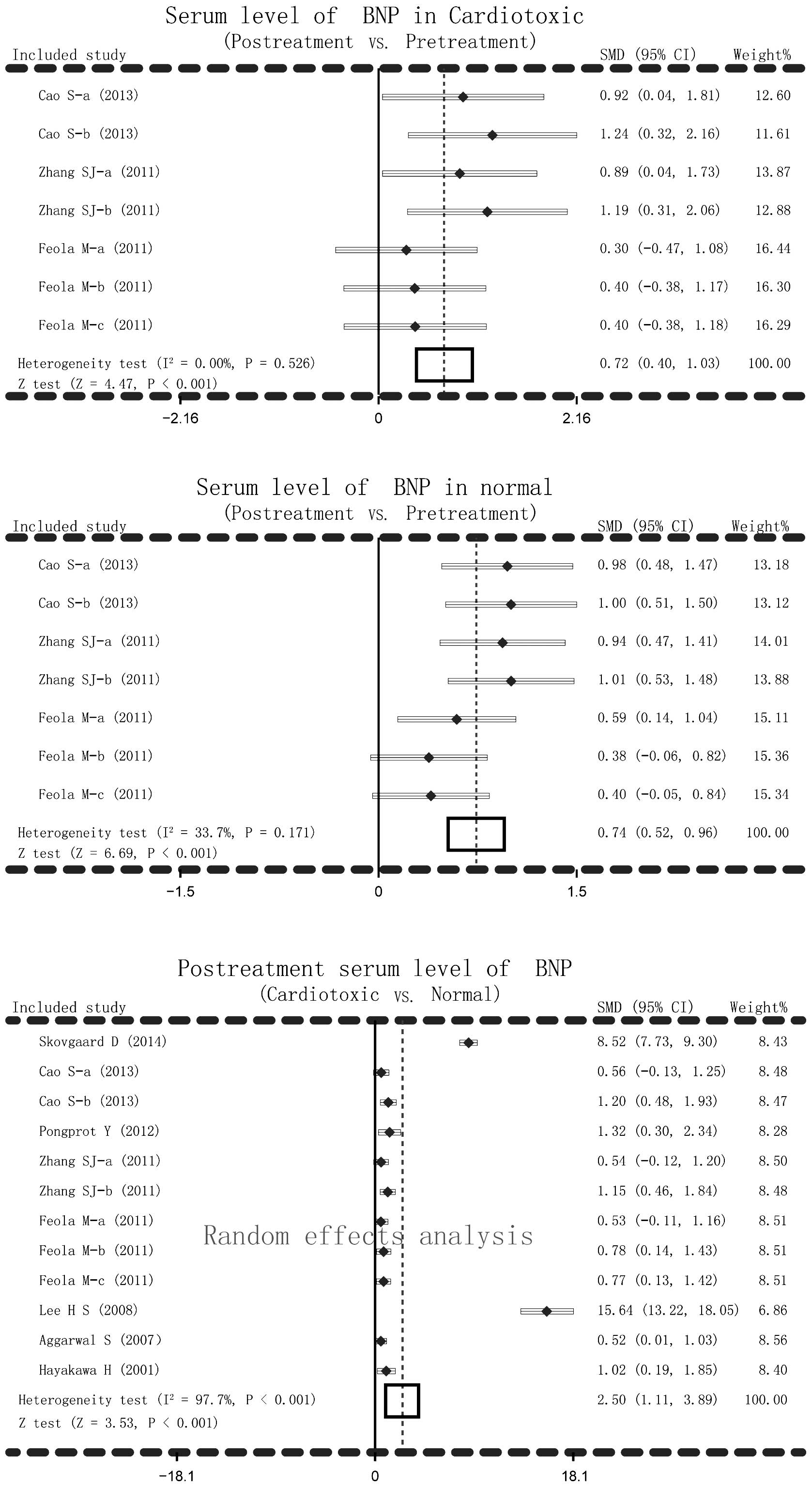
Quantitative data synthesis
The main result of the present meta-analysis on the
relationship between post-treatment serum BNP levels and AIC in
cardiotoxic group and normal group was based on random-effects
analysis due to I2 >50% and P<0.001. Significant
differences in serum BNP levels in cardiotoxic group and normal
group between post-treatment and pretreatment of anthracyclines
were detected (cardiotoxic group: SMD=0.72, 95% CI=0.40–1.03,
P<0.001; normal group: SMD=0.74, 95% CI=0.52–0.96, P<0.001).
Serum levels of BNP after anthracycline treatment increased
remarkably in cardiotoxic group compared with the normal group
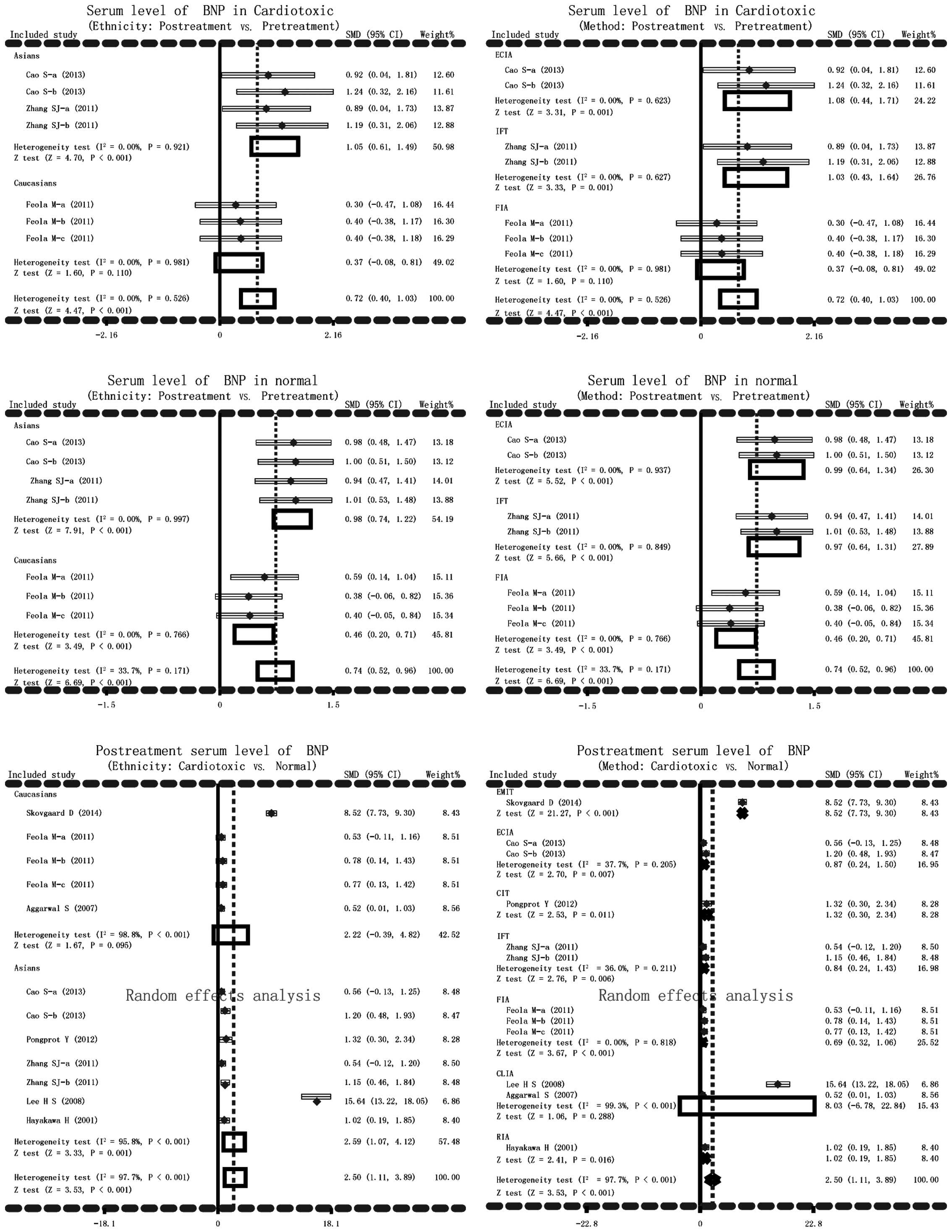
(SMD=2.50, 95% CI=1.11–3.89, P<0.001) (Fig. 2). In addition, subgroup analysis based
on ethnicity and detection methods were performed to explore the
potential influential factors on the relationship between serum
levels of BNP and AIC. Ethnicity stratified analysis showed
significantly higher BNP serum levels in post-treatment
anthracyclines patients compared with the pretreatment patients in
the cardiotoxic group in the Asian, but not in the Caucasian,
population (Asian: SMD=1.05, 95% CI=0.61–1.49, P<0.001;
Caucasian: SMD=0.37, 95% CI=−0.08–0.81, P=0.110). Significantly
higher BNP serum levels after anthracyclines treatment were
observed compared to pretreatment with anthracyclines in both Asian
and Caucasian patients (all P>0.05). The serum level of BNP
after anthracyclines treatment was notably higher in the
cardiotoxic group than the normal group. As for stratified analysis
on the basis of detection method, higher BNP serum level was found
after anthracyclines treatment in cardiotoxic group with ECIA, IFT
method (P>0.05) but not with FIA method (SMD=0.37, 95%
CI=−0.08–0.81, P=0.110). While higher BNP serum levels were
observed after anthracyclines treatment in the normal group with
ECIA, IFT and FIA methods (all P<0.05). Post-treatment serum
level of BNP was notably higher in the cardiotoxic group compared
with the normal group with EMIT, ECIA, CIT, IFT, FIA, RIA (all
P<0.05) but not with CLIA (SMD=8.03, 95% CI=−6.78–22.84,
P=0.288) (Fig. 3).
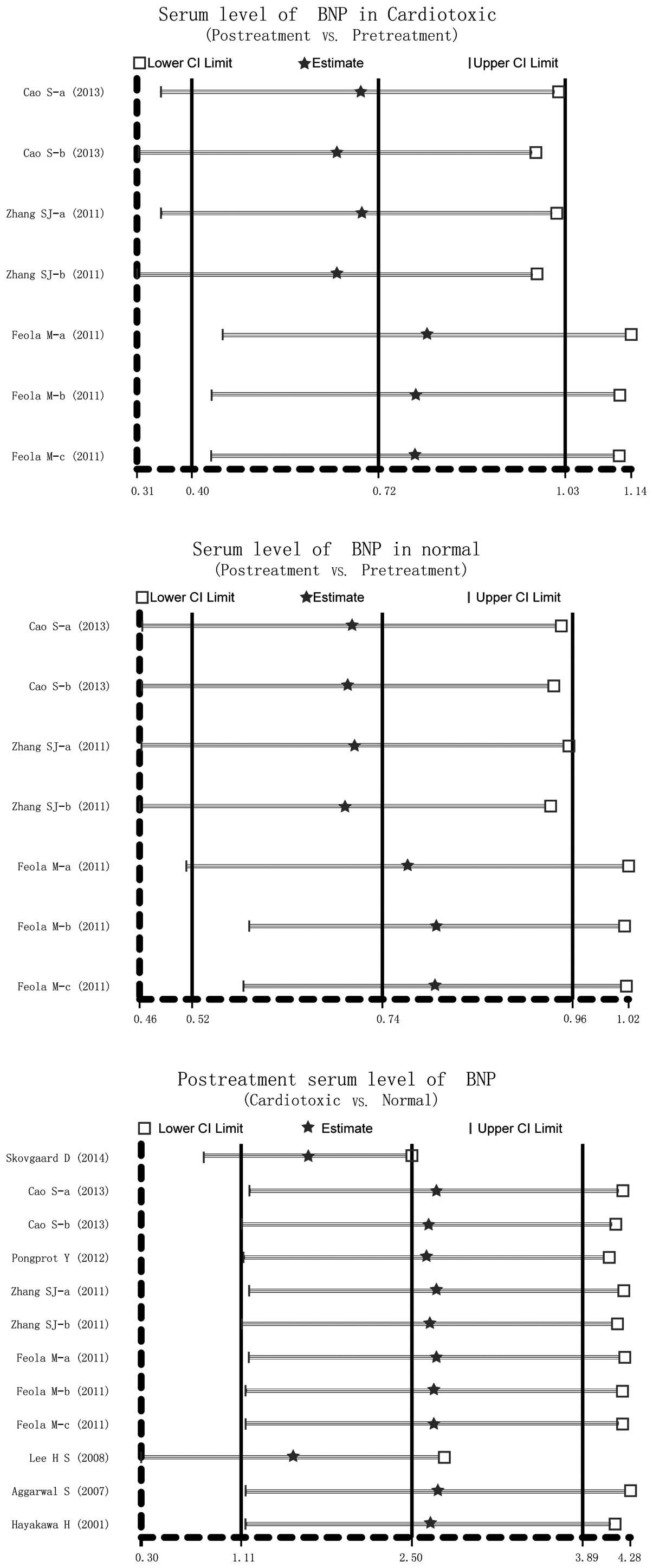
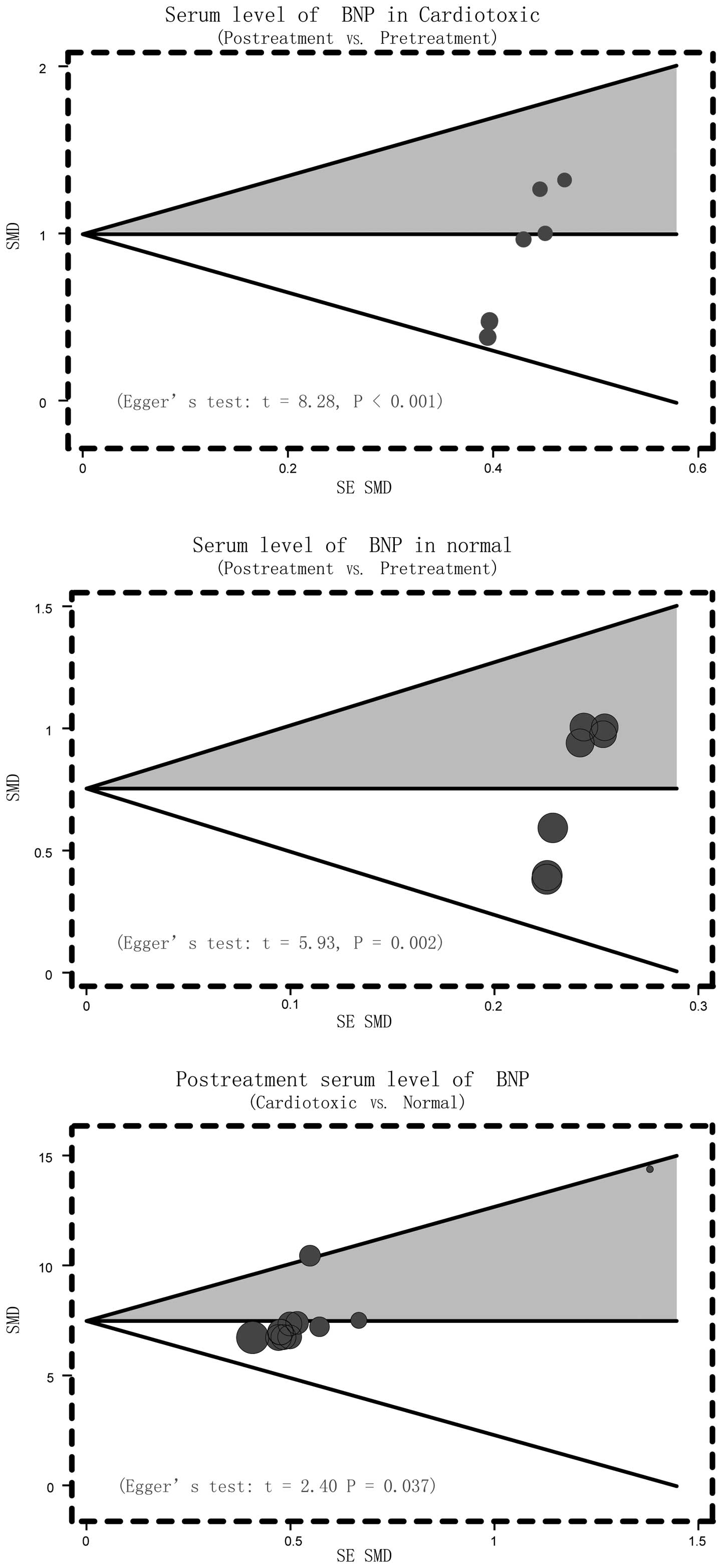
Sensitivity analysis and publication
bias
Sensitivity analysis was conducted to determine the
influence of one single study on the whole result of the analysis,
which could indicate the stability of the study. It demonstrated
that no single study affected the pooled SMDs in the meta-analysis
of anthracyclines treatment and cardio toxicity (Fig. 4). Finally, the Egger's regression test
was applied to detect the publication bias. The result showed
symmetrical distributions in the funnel-plot, indicating
publication bias in the systematic reviews (Cardiotoxic: Egger's
test: t=8.28, P<0.001; Normal: Egger's test: t=5.93, P=0.002;
Cardiotoxic vs. Normal: Egger's test: t=2.40, P=0.037) (Fig. 5).
Discussion
The present meta-analysis was performed to evaluate
the adverse effects of anthracyclines in cancer patients and to
determine the relationship between serum BNP levels and
cardiotoxicity. The findings demonstrated that patients with
cardiotoxicity displayed increased serum BNP levels after
anthracycline treatment compared to pretreatment, the normal people
treated by anthracyclines also have higher serum levels of BNP, and
patients with AIC have much higher BNP levels than normal
individuals. Anthracyclines have the adverse effects of causing
cardiotoxic events in cancer patients and BNP responds to
end-diastolic pressure. Slight increases in BNP serum levels
identify a risk of cardiac dysfunction, suggesting that increased
BNP levels can be a diagnostic marker for the risk of
cardiotoxicity and even for improving the diagnostic performance of
cardiac disease induced by anthracycline-like chemotherapy
(11). Low dose of anthracyclines
contribute to deterioration of cardiac function in patients with
acute lymphoblastic leukemia, and is readily detected by the
cardiac biomarker BNP (36). AIC has
a vital impact on cardiac failure, and elevated BNP serum levels in
cardiotoxic patients signify compensatory mechanisms to alleviate
the severity of myocardial damage, thus BNP could serve as a useful
factor in indicating cardiotoxicity incidence (37). On account of the above working
mechanisms of BNP, the meta-analysis results conclude that
up-regulated BNP serum levels are observed in cardiotoxic patients
induced by anthracycline chemotherapy, and BNP serum levels are
helpful for predicting, diagnosing and preventing cardiotoxicity.
In accordance with the present results, Feola et al
(8), supported that the toxic effects
following chemotherapy in breast cancer patients may be observed
with plasma markers, including BNP, to detect left ventricular
dysfunction that could provoke cardiac dysfunction (8).
Subgroup analysis was performed in order to take
account of other factors that may affect the relationship between
BNP serum levels and AIC. The other factors included ethnicity and
the detection method. Serum levels of BNP after anthracyclines
treatment in cardiotoxic patients were increased among Asian
patients, not among Caucasian patients, and the result may be
affected by the methods of ECIA and IFT, but not by FIA method,
implying that ethnicity and method in the study may be
heterogeneity sources. Normal individuals that received
anthracycline chemotherapy also exhibited higher serum levels of
BNP. BNP detection was obvious among both Asian and Caucasian
patients and the three methods of ECIA, IFT and FIA all had the
impact on the accuracy of detection. However, when comparing
cardiotoxic patients and normal people, increased BNP serum levels
were associated with the incidence rates of cardiotoxicity among
Caucasian, not among Asian, patients. The association may be
influenced by the applied methods like EMIT, ECIA, CIT, IFT, FIA
and RIA. Only CLIA method had no effect on the association between
BNP levels and cardiotoxicity. The present study revealed that the
onset of cardiotoxicity is related with elevated BNP serum levels,
and BNP has remarkable clinical value in early diagnosis of AIC
patients, improving the overall predictive efficacy in toxic events
of the heart.
Limitations in the present study should also be
considered. First, there were only 8 articles included, which may
not supply sufficient statistical power to estimate the association
between the serum levels of BNP and AIC. Second, unpublished
studies and articles in languages other than English and Chinese
could not be included due to restriction of the inclusion and
exclusion criteria, therefore potential heterogeneity and bias may
exist. Third, according to the baseline characteristic table, the
current meta-analysis only focused on Asian and Caucasian
populations, which may also lead to bias. Besides, the sample size
and the number of cases were relatively small; the majority were
<20. In addition, some articles did not contain information
about gender, age and follow-up periods. Finally, there may be
potential factors that were not taken into account, which may have
influenced the results despite all participants of each study were
well-defined with similar inclusion criteria, so the results in the
current meta-analysis should be interpreted with caution owing to
the potential heterogeneity among trials. Despite the described
limitations, the current meta-analysis is an important example on
the association between the serum levels of BNP and AIC. Of note, a
more reliable conclusion was drawn in the meta-analysis, because
the inconsistent results were rigorously quantified and
analyzed.
In conclusion, the present meta-analysis indicates
that the serum level of BNP is associated with AIC. Therefore,
serum levels of BNP may be a useful index for monitoring AIC at an
early stage. However, further in-depth studies are still required
to confirm these findings due to the above limitations.
References
|
1
|
Lee HS, Son CB, Shin SH and Kim YS:
Clinical correlation between brain natriutetic peptide and
anthracyclin-induced cardiac toxicity. Cancer Res Treat.
40:121–126. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Aapro M, Bernard-Marty C, Brain EG, Batist
G, Erdkamp F, Krzemieniecki K, Leonard R, Lluch A, Monfardini S,
Ryberg M, et al: Anthracycline cardiotoxicity in the elderly cancer
patient: A SIOG expert position paper. Ann Oncol. 22:257–267. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Visscher H, Ross CJ, Rassekh SR, Barhdadi
A, Dubé MP, Al-Saloos H, Sandor GS, Caron HN, van Dalen EC, Kremer
LC, et al: Pharmacogenomic prediction of anthracycline-induced
cardiotoxicity in children. J Clin Oncol. 30:1422–1428. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lipshultz SE, Alvarez JA and Scully RE:
Anthracycline associated cardiotoxicity in survivors of childhood
cancer. Heart. 94:525–533. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ewer MS and Lenihan DJ: Left ventricular
ejection fraction and cardiotoxicity: Is our ear really to the
ground? J Clin Oncol. 26:1201–1203. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
van der Pal HJ, van Dalen EC, Hauptmann M,
Kok WE, Caron HN, van den Bos C, Oldenburger F, Koning CC, van
Leeuwen FE and Kremer LC: Cardiac function in 5-year survivors of
childhood cancer: A long-term follow-up study. Arch Intern Med.
170:1247–1255. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kremer LC, van der Pal HJ, Offringa M, van
Dalen EC and Voûte PA: Frequency and risk factors of subclinical
cardiotoxicity after anthracycline therapy in children: A
systematic review. Ann Oncol. 13:819–829. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Feola M, Garrone O, Occelli M, Francini A,
Biggi A, Visconti G, Albrile F, Bobbio M and Merlano M:
Cardiotoxicity after anthracycline chemotherapy in breast
carcinoma: Effects on left ventricular ejection fraction, troponin
I and brain natriuretic peptide. Int J Cardiol. 148:194–198. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pongprot Y, Sittiwangkul R, Charoenkwan P
and Silvilairat S: Use of cardiac markers for monitoring of
doxorubixin-induced cardiotoxicity in children with cancer. J
Pediatr Hematol Oncol. 34:589–595. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hayakawa H, Komada Y, Hirayama M, Hori H,
Ito M and Sakurai M: Plasma levels of natriuretic peptides in
relation to doxorubicin-induced cardiotoxicity and cardiac function
in children with cancer. Med Pediatr Oncol. 37:4–9. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Skovgaard D, Hasbak P and Kjaer A: BNP
predicts chemotherapy-related cardiotoxicity and death: Comparison
with gated equilibrium radionuclide ventriculography. PLoS One.
9:e967362014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Beleigoli AM, Boersma E, de Diniz MF,
Vidigal PG, Lima-Costa MF and Ribeiro AL: C-reactive protein and
B-type natriuretic peptide yield either a non-significant or a
modest incremental value to traditional risk factors in predicting
long-term overall mortality in older adults. PLoS One.
8:e758092013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Khalaf MA, Abdelrahman TM and Abbas MF:
Values of using QTc and N-terminal fragment of B-type natriuretic
peptide as markers for early detection of acute antipsychotic
drugs-induced cardiotoxicity. Cardiovasc Toxicol. 11:10–17. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Maisel AS, Krishnaswamy P, Nowak RM,
McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu
AH, et al: Rapid measurement of B-type natriuretic peptide in the
emergency diagnosis of heart failure. N Engl J Med. 347:161–167.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Troughton RW, Frampton CM, Yandle TG,
Espiner EA, Nicholls MG and Richards AM: Treatment of heart failure
guided by plasma aminoterminal brain natriuretic peptide (N-BNP)
concentrations. Lancet. 355:1126–1130. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Geske JB, McKie PM, Ommen SR and Sorajja
P: B-type natriuretic peptide and survival in hypertrophic
cardiomyopathy. J Am Coll Cardiol. 61:2456–2460. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gerber IL, Stewart RA, Legget ME, West TM,
French RL, Sutton TM, Yandle TG, French JK, Richards AM and White
HD: Increased plasma natriuretic peptide levels reflect symptom
onset in aortic stenosis. Circulation. 107:1884–1890. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Morrow DA, de Lemos JA, Sabatine MS,
Murphy SA, Demopoulos LA, Di Battiste PM, McCabe CH, Gibson CM,
Cannon CP and Braunwald E: Evaluation of B-type natriuretic peptide
for risk assessment in unstable angina/non-ST-elevation myocardial
infarction: B-type natriuretic peptide and prognosis in
TACTICS-TIMI 18. J Am Coll Cardiol. 41:1264–1272. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Berger R, Huelsman M, Strecker K, Bojic A,
Moser P, Stanek B and Pacher R: B-type natriuretic peptide predicts
sudden death in patients with chronic heart failure. Circulation.
105:2392–2397. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Daniels LB and Maisel AS: Natriuretic
peptides. J Am Coll Cardiol. 50:2357–2368. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Costa VN, Nomura RM, Miyadahira S, Vieira
Francisco RP and Zugaib M: Cord blood B-type natriuretic peptide
levels in placental insufficiency: Correlation with fetal Doppler
and pH at birth. Eur J Obstet Gynecol Reprod Biol. 171:231–234.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Esteves WA, Lodi-Junqueira L, Neto CP, Tan
TC, Nascimento BR, Mehrotra P, Barbosa MM, Ribeiro AL and Nunes MC:
The impact of right ventricular stroke work on B-type natriuretic
peptide levels in patients with mitral stenosis undergoing
percutaneous mitral valvuloplasty. J Interv Cardiol. 26:501–508.
2013.PubMed/NCBI
|
|
23
|
Jan SL, Lin SJ, Fu YC, Lin MC, Chan SC and
Hwang B: Plasma B-type natriuretic peptide study in children with
severe enterovirus 71 infection: A pilot study. Int J Infect Dis.
17:e1166–e1171. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Vila G, Resl M, Stelzeneder D, Struck J,
Maier C, Riedl M, Hülsmann M, Pacher R, Luger A and Clodi M: Plasma
NT-proBNP increases in response to LPS administration in healthy
men. J Appl Physiol (1985). 105:1741–1745. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Clerico A, Giannoni A, Vittorini S and
Passino C: Thirty years of the heart as an endocrine organ:
Physiological role and clinical utility of cardiac natriuretic
hormones. Am J Physiol Heart Circ Physiol. 301:H12–H20. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hequet O, Le QH, Moullet I, Pauli E,
Salles G, Espinouse D, Dumontet C, Thieblemont C, Arnaud P, Antal
D, et al: Subclinical late cardiomyopathy after doxorubicin therapy
for lymphoma in adults. J Clin Oncol. 22:1864–1871. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zintzaras E and Ioannidis JP: HEGESMA:
Genome search meta-analysis and heterogeneity testing.
Bioinformatics. 21:3672–3673. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zintzaras E and Ioannidis JP:
Heterogeneity testing in meta-analysis of genome searches. Genet
Epidemiol. 28:123–137. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Song F and Gilbody S: Bias in
meta-analysis detected by a simple, graphical test. Increase in
studies of publication bias coincided with increasing use of
meta-analysis. BMJ. 316:4711998.PubMed/NCBI
|
|
32
|
Peters JL, Sutton AJ, Jones DR, Abrams KR
and Rushton L: Comparison of two methods to detect publication bias
in meta-analysis. JAMA. 295:676–680. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Aggarwal S, Pettersen MD, Bhambhani K,
Gurczynski J, Thomas R and L'Ecuyer T: B-type natriuretic peptide
as a marker for cardiac dysfunction in anthracycline-treated
children. Pediatr Blood Cancer. 49:812–816. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhang SJ and Cui YZ: Measurement of brain
natriuretic peptide ring based chemotherapy in patients with
cardiac toxicity in anthracene. Chinese Journal of Difficult and
Complicated Cases. 10:444–445. 2011.
|
|
35
|
Cao S, Pang DM, Duan HB, Lin YD and Li LT:
Application value in the levels of plasma NTproBNP in patients with
cardiac toxicity. Modern Diagnosis & Treatment. 303–304.
2013.
|
|
36
|
Mavinkurve-Groothuis AM, Marcus KA,
Pourier M, Loonen J, Feuth T, Hoogerbrugge PM, de Korte CL and
Kapusta L: Myocardial 2D strain echocardiography and cardiac
biomarkers in children during and shortly after anthracycline
therapy for acute lymphoblastic leukaemia (ALL): A prospective
study. Eur Heart J Cardiovasc Imaging. 14:562–569. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Krawczuk-Rybak M, Dakowicz L, Hryniewicz
A, Maksymiuk A, Zelazowska-Rutkowska B and Wysocka J: Cardiac
function in survivors of acute lymphoblastic leukaemia and
Hodgkin's lymphoma. J Paediatr Child Health. 47:455–459. 2011.
View Article : Google Scholar : PubMed/NCBI
|