In April 2013, a 76 year old male patient presented
to the Department of Oncology, University Hospital in Olomouc
(Olomouc, Czech Republic), with renal cell cancer after resection
of the primary renal tumor and also surgical resection of brain
metastases within right temporal lobe. The pathology report
demonstrated the patient had metastatic clear cell renal carcinoma.
Brain recurrence had occurred after the primary treatment (3
metastases in right temporal lobe) 4 months after surgical
resection. Computed tomography (CT) ruled out any additional extra
cranial disease. The patient was considered to be fit (performance
status 1) without significant co-morbidities and SRT radiotherapy
with hippocampal avoidance-whole brain radiotherapy (HA-WBRT) was
indicated as the appropriate treatment modality after discussion on
institutional multidisciplinary board. The patient did not receive
any targeted therapy prior to or during the radiotherapy dose
delivery. Planning CT scans with 2 mm slide thickness were created.
The International Commission on Radiation Units and Measurements
(ICRU) recommendations number 50, 62, 83 were followed during the
target volumes delineation, treatment plan calculation and plan
approving process (10–12). For SRT, the metastatic disease was
contoured based on the fusion with T1 weighted sequences magnetic
resonance imaging (MRI) as gross tumor volume (GTV) with adding the
2 mm margin to create the clinical target volume (CTV) and the
planning target volume (PTV). The Monaco planning system (IMPAC
Medical Systems, Maryland Heights, MO, USA) with Monte Carlo
computing software (version 3.30.01; Elekta, Stockholm, Sweden) was
used for treatment plan calculation and Elekta Synergy linear
accelerator (Elekta) with single arc volumetric arc radiotherapy
(VMAT) with 6MV photon energy was used for treatment dose delivery.
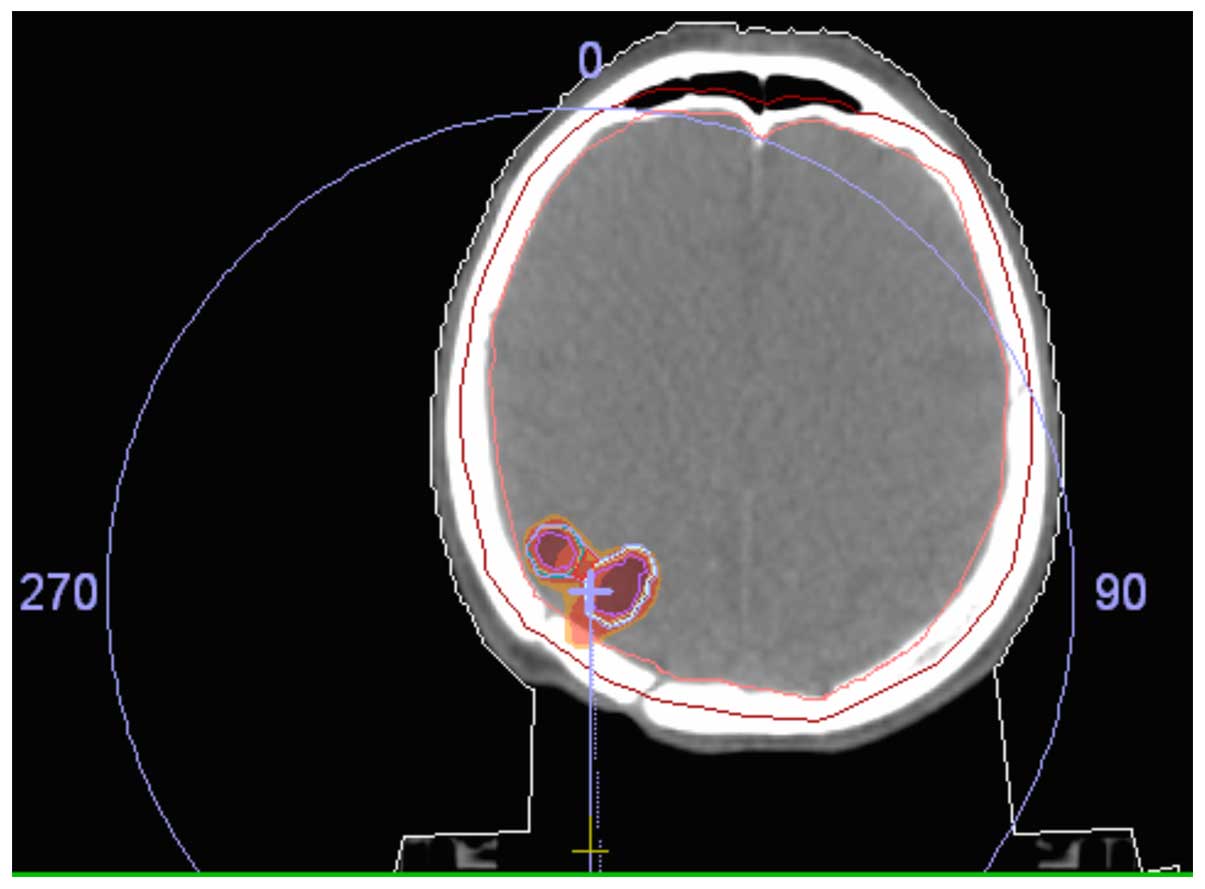
The prescribed dose was 21 Gy in 3 fractions delivered on 3
consecutive days with a biologically effective dose (BED10) of 35.7
Gy. The dose was prescribed on isodose selected as isodose most
accordingly encompasses the PTV without any limitation regarding
the maximum dose within the PTV (Fig.
1) and with the maximum dose drop off towards the surrounding
normal structures. A HeadSTEP system with thermoplastic mask
(Elekta) was used for patient immobilization. Patient position
verification was achieved by three cone-beam CT (CBCT) every single
day of the treatment. First CBCT was carried out after patient
placement on the treatment table and position was adjusted using
HexaPOD setup system (Elekta), a second round of CBCT followed
after position adjustment to confirm proper positioning and a third
round of CBCT followed the delivery of the treatment to rule out
any intrafractional (during the dose delivery) shifts. The volume
of final PTV was 3,736 cm3, created as the sum of 3
metastases volumes, with a minimum dose covering 100% of the PTV
D100=20.95 Gy and only 0.11% of the PTV volume being irradiated to
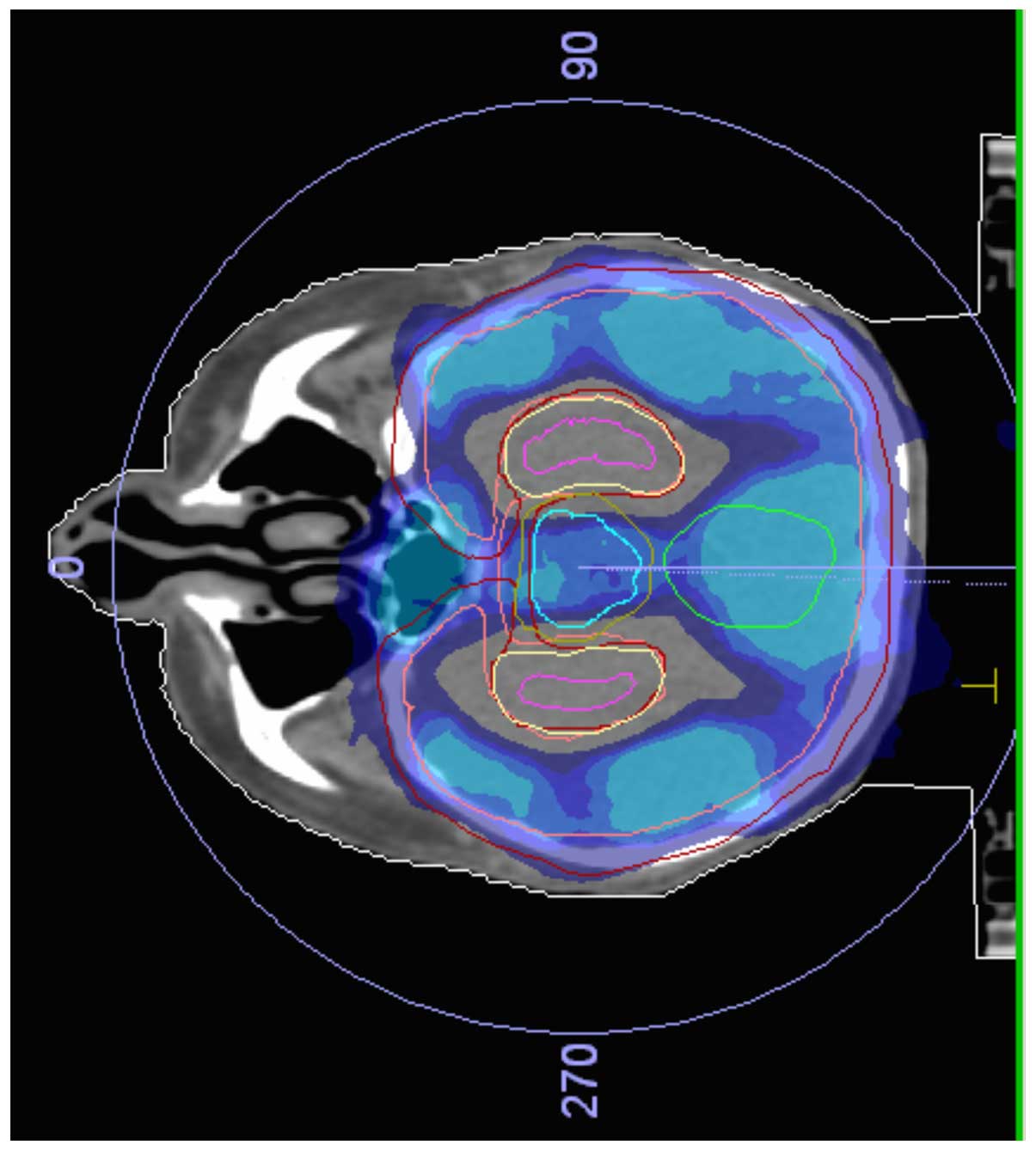
dose bellow prescribed dose. HA-WBRT was continued after completion
of SRT. For contouring and plan review purposes RTOG 0933 ‘(a phase
II trial of hippocampal avoidance during whole brain radiotherapy
for brain metastases)’ proposals were followed aiming to reach the
limit to the maximum dose to hippocampal structures to 17 Gy and
D100 to <10 Gy (the dose to 100% of hippocampus should be kept
under 10 Gy) (13). Hippocampal
structures were delineated after fusion with MRI and a 5 mm margin
was added to the final contours of the hippocampus. The whole brain
CTV was contoured manually including the whole brain and an
additional margin of 5 mm was added to create PTV. The WBRT PTV
excluded hippocampal structures within the 5 mm margin creating the
HA-WBRT PTV. The prescribed treatment dose was 30 Gy in 10
fractions (Fig. 2). The
immobilization techniques for HA-WBRT were the same as for SRT and
the treatment plan was prepared with similar planning systems as
described above for SRT with following results: (near max) D2=33.91
Gy, (near min) D98=25.20 Gy, D100=14.18 Gy, D50=31.26 Gy,
homogeneity index (HI) calculated as D 2-D 98/D 50 was 0.278. The
maximum dose for hippocampus was 17.50 Gy and the mean dose of
11.59 Gy did not exceed the RTOG 0933 trial constrains. The
following doses to OAR were achieved: Right optic nerve D max 31.96
Gy, left optic nerve D max 30.96 Gy, chiasma D max 32.76 Gy. The
dose was delivered in 10 consecutive working days within 2 weeks
without any unintentional time gaps. CBCT was performed weekly to
verify patient positioning on the treatment table. A low dose of
oral steroids (dexamethasone, 3 mg/day) was administered during the
whole duration of radiotherapy. As a part of quality assurance
process in the department all contours and treatment plans were
reviewed by a second experienced clinical oncologist. The patient
received the treatment without significant acute toxicity however
longer follow up regarding late toxicity, progression free survival
and overall survival is needed to confirm the long term safety and
effectivity of this treatment technique.
Expected patient survival may be used to guide
clinicians about proper treatment strategy. Generally patients with
an expected median survival <3 months should not be exposed to
potential risks of surgery or stereotactic radiotherapy since the
cost/benefit ratio of these treatment modalities is questionable in
this group of patients and simple radiotherapy technique such as
two opposed lateral fields using conventional simulator should be
considered. Several clinical trials have evaluated which treatment
option or their combination is most appropriate for patients with
brain metastatic disease (3).
Surgery represents the mainstay of local treatment
of brain metastatic disease. Surgical resection may be used as the
sole technique or in combination with WBRT after resection or SRT;
SRS may be used on the surgical cavity after the resection. WBRT
after the surgical resection decreases the risk of disease
recurrence however this advantage doesn't project into overall
survival benefit suggesting the possibility of deferring the WBRT,
SRS or SRT for the time of disease recurrence (14–18). By
contrast, SRT with WBRT compared with WBRT alone increases the
overall survival of treated patients, indicating that these
treatment modalities should be combined. Again when comparing SRS
alone with SRT, and SRS with WBRT, the overall survival rate
remains the same, however the chance of local recurrence decreases
by ~30% when WBRT is added (19–30).
Another issue related to WBRT is the potentially increased risk of
cognitive function impairment (30).
There are data suggesting that hippocampal structures (mainly the
subgranular zone of the hippocampus) are highly susceptible to
radiotherapy injury and these changes may be responsible for
cognitive (learning, memory and judgement) worsening after WBRT
(31–33). Cognitive impairment in patients
achieving longer survival may significantly deteriorate the patient
quality of life even if actual function tests to accordingly assess
neurocognitive functions are questionable (mini mental status exam,
Hopkins Verbal Learning Test, CogState computerized neurocognitive
tests) and one can suggest that the neurocognitive deterioration
may be caused by subclinical metastatic disease progression in the
brain which is indistinguishable from radiotherapy toxicity.
Similar to SRT, SRS may be used as the sole technique or in
combination with WBRT with similar advantages and disadvantages. It
is important to note that the dose of the SRT or SRS should be
decreased by 10–20% when combined with WBRT to avoid extensive
brain toxicity. Clinical trials directly comparing surgery and SRT
are not convincing for preference of either of these techniques
(34), however one has to consider
the morbidity of brain surgery with respect to patient overall
fitness and co-morbidities. In addition, the optimum timing for
SRT, SRS, WBRT, and HA-WBRT is not very clear considering that
immediate WBRT following SRT, or SRS, may significantly increase
the toxicity of radiotherapy. In cases of WBRT preceding SRT/SRS,
complete remission of certain small metastatic lesions may occur
and thus, no metastasis may be visible on planning scans for
SRT/SRS and the opportunity for SRT/SRS could be missed. There are
data suggesting that deferred WBRT may not reverse neurological
deficit caused by brain recurrence (35) making the decision about proper WBRT
timing even more difficult. The most recent recommendation
regarding WBRT published in The Lancet Oncology suggested
indication of SRS, SRT without WBRT as the preferred technique if
feasible (36).
For patients with an expected survival time of <3
months, WBRT or best supportive care (BSC) with oral steroids
remains a viable option (3,37). The dose of the steroids is another
possible issue without clear recommendation however the dose should
be driven by neurological symptoms also taking into account the
side effects of long term steroid treatment. One of the possible
technique how to avoid above mentioned unwanted side effect of WBRT
is to perform HA-WBRT avoidance (35,38).
Considering radiotherapy of hippocampal structures is considered to
be responsible for cognitive impairment its avoidance could
possibly preserve the cognitive functions. One argument against
this technique is that there is an increased risk of disease
recurrence in the areas that radiation is avoided. However, Ghia
et al (39) concluded that the
risk is low and clinically insignificant after assessing the risk
or metastatic disease in the hippocampus with 5 mm margin.
Furthermore, the potential recurrence in this area may be treated
by SRT or SRS. The Clinical trial Radiation Therapy Oncology Group
RTOG 0933 was initiated to confirm this expectation utilizing
HA-WBRT (excluding germ cell tumors, small cell lung cancer and
hematologic malignancies) using Hopkins Verbal Learning
Test-Revised for cognitive functions assessment (13), however no final results are published
at present. When considering bringing HA-WBRT into daily practice
one has to take into account the departmental equipment, staff time
and experience resulting in the significantly higher cost required
for target volumes delineation, calculation of VMAT treatment plan
and treatment delivery comparing with simple and quick technique
such as 2 lateral opposed fields using conventional simulator for
WBRT. This decision should be guided by best clinical judgement,
the above mentioned prognostic indexes with respect to expected
patient survival and departmental technical equipment. One of the
unanswered question in the case of SRT indication is the role of
systemic treatment. More specifically if the management should
follow the guidelines for surgical resection, which means in the
case of renal cell cancer metastasis continuing with observation
and waiting to administer systemic treatment only in the case of
disease progression or commencing targeted therapy immediately
after ablative radiotherapy. No randomized data or recommendations
exists regarding this issue and decision should be made on an
individual basis (27,40).
SRT with HA-WBRT represents a feasible and safe
technique for the management of brain metastatic disease. Due to
the increasing overall survival rates among cancer patients,
sparing of cognitive functions may be even more significant in the
future.
|
1
|
Culine S, Bekradda M, Kramar A, Rey A,
Escudier B and Droz JP: Prognostic factors for survival in patients
with brain metastases from renal cell carcinoma. Cancer.
83:2548–2553. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Escudier B, Porta C, Schmidinger M, Algaba
F, Patard JJ, Khoo V, Eisen T and Horwich A: ESMO Guidelines
Working Group: Renal cell carcinoma: ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up. Ann Oncol.
25(Suppl 3): iii49–iii56. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tsao MN, Rades D, Wirth A, Lo SS,
Danielson BL, Gaspar LE, Sperduto PW, Vogelbaum MA, Radawski JD,
Wang JZ, et al: Radiotherapeutic and surgical management for newly
diagnosed brain metastasis(es): An American Society for Radiation
Oncology evidence-based guideline. Pract Radiat Oncol. 2:210–225.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Minniti G, D'Angelillo RM, Scaringi C,
Trodella LE, Clarke E, Matteucci P, Osti MF, Ramella S, Enrici RM
and Trodella L: Fractionated stereotactic radiosurgery for patients
with brain metastases. J Neurooncol. 117:295–301. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kim YJ, Cho KH, Kim JY, Lim YK, Min HS and
Lee SH, Kim HJ, Gwak HS, Yoo H and Lee SH: Single-dose versus
fractionated stereotactic radiotherapy for brain metastases. Int J
Radiat Oncol Biol Phys. 81:483–489. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gaspar L, Scott C, Rotman M, Asbell S,
Phillips T, Wasserman T, McKenna WG and Byhardt R: Recursive
partitioning analysis (RPA) of prognostic factors in three
Radiation Therapy Oncology Group (RTOG) brain metastases trials.
Int J Radiat Oncol Biol Phys. 37:745–751. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nieder C, Marienhagen K, Geinitz H and
Molls M: Validation of the graded prognostic assessment index for
patients with brain metastases. Acta Oncol. 48:457–459. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Villà S, Weber DC, Moretones C, Mañes A,
Combescure C, Jové J, Puyalto P, Cuadras P, Bruna J, Verger E, et
al: Validation of the new graded prognostic assessment scale for
brain metastases: A multicenter prospective study. Radiat Oncol.
6:232011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nieder C, Andratschke NH, Geinitz H and
Grosu AL: Diagnosis-specific graded prognostic assessment score is
valid in patients with brain metastases treated in routine clinical
practice in two European countries. Med Sci Monit. 18:CR450–CR455.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
International Commission on Radiation
Units and Measurements: Prescribing, Recording and Reporting Photon
Beam Therapy (Report 50). Bethesda: 1993.
|
|
11
|
International Commission on Radiation
Units and Measurements: Prescribing, Recording and Reporting Photon
Beam Therapy (Report 62). Bethesda: 1999.
|
|
12
|
International Commission on Radiation
Units and Measurements: Prescribing, Recording and Reporting
Intensity-Modulated Photon-Beam Therapy (IMRT) (ICRU Report 83).
Washington: 2010.
|
|
13
|
Gondi V, Pugh SL, Tome WA, Caine C, Corn
B, Kanner A, Rowley H, Kundapur V, DeNittis A, Greenspoon JN, et
al: Preservation of memory with conformal avoidance of the
hippocampal neural stem-cell compartment during whole-brain
radiotherapy for brain metastases (RTOG 0933): A phase II
multi-institutional trial. J Clin Oncol. 32:3810–3816. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rades D, Bohlen G, Pluemer A, Veninga T,
Hanssens P, Dunst J and Schild SE: Stereotactic radiosurgery alone
versus resection plus whole-brain radiotherapy for 1 or 2 brain
metastases in recursive partitioning analysis class 1 and 2
patients. Cancer. 109:2515–2521. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Karlovits BJ, Quigley MR, Karlovits SM,
Miller L, Johnson M, Gayou O and Fuhrer R: Stereotactic
radiosurgery boost to the resection bed for oligometastatic brain
disease: Challenging the tradition of adjuvant whole-brain
radiotherapy. Neurosurg Focus. 27:E72009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kocher M, Soffietti R, Abacioglu U, Villà
S, Fauchon F, Baumert BG, Fariselli L, Tzuk-Shina T, Kortmann RD,
Carrie C, et al: Adjuvant whole-brain radiotherapy versus
observation after radiosurgery or surgical resection of one to
three cerebral metastases: Results of the EORTC 22952–26001 study.
J Clin Oncol. 29:134–141. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Iwadate Y, Namba H and Yamaura A:
Whole-brain radiation therapy is not beneficial as an adjuvant
therapy for brain metastases compared with localized irradiation.
Anticancer Res. 22:325–330. 2002.PubMed/NCBI
|
|
18
|
Mintz A, Perry J, Spithoff K, Chambers A
and Laperriere N: Management of single brain metastasis: A practice
guideline. Curr Oncol. 14:131–143. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Aoyama H, Shirato H, Tago M, Nakagawa K,
Toyoda T, Hatano K, Kenjyo M, Oya N, Hirota S, Shioura H, et al:
Stereotactic radiosurgery plus whole-brain radiation therapy vs
stereotactic radiosurgery alone for treatment of brain metastases:
A randomized controlled trial. JAMA. 295:2483–2491. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tsao MN, Lloyd NS and Wong RK: Supportive
Care Guidelines Group of Cancer Care Ontario's Program in
Evidence-based Care: Clinical practice guideline on the optimal
radiotherapeutic management of brain metastases. BMC Cancer.
5:342005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Khuntia D, Brown P, Li J and Mehta MP:
Whole-brain radiotherapy in the management of brain metastasis. J
Clin Oncol. 24:1295–1304. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Soon YY, Tham IW, Lim KH, Koh WY and Lu
JJ: Surgery or radiosurgery plus whole brain radiotherapy versus
surgery or radiosurgery alone for brain metastases. Cochrane
Database Syst Rev. 3:CD0094542014.PubMed/NCBI
|
|
23
|
Kocher M, Maarouf M, Bendel M, Voges J,
Müller RP and Sturm V: Linac radiosurgery versus whole brain
radiotherapy for brain metastases. A survival comparison based on
the RTOG recursive partitioning analysis. Strahlenther Onkol.
180:263–267. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rades D and Schild SE: Do patients with a
limited number of brain metastases need whole-brain radiotherapy in
addition to radiosurgery? Strahlenther Onkol. 188:702–706. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Golden DW, Lamborn KR, McDermott MW,
Kunwar S, Wara WM, Nakamura JL and Sneed PK: Prognostic factors and
grading systems for overall survival in patients treated with
radiosurgery for brain metastases: Variation by primary site. J
Neurosurg. 109(Suppl): S77–S86. 2008.
|
|
26
|
Kocher M, Wittig A, Piroth MD, Treuer H,
Seegenschmiedt H, Ruge M, Grosu AL and Guckenberger M: Stereotactic
radiosurgery for treatment of brain metastases. A report of the
DEGRO working group on stereotactic radiotherapy. Strahlenther
Onkol. 190:521–532. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bates JE, Youn P, Peterson CR III, Usuki
KY, Walter KA, Okunieff P and Milano MT: Radiotherapy for brain
metastases from renal cell carcinoma in the targeted therapy Era:
The university of Rochester experience. Am J Clin Oncol. 2015 Feb
26;(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fokas E, Henzel M, Hamm K, Surber G,
Kleinert G and Engenhart-Cabillic R: Radiotherapy for brain
metastases from renal cell cancer: Should whole-brain radiotherapy
be added to stereotactic radiosurgery? Analysis of 88 patients.
Strahlenther Onkol. 186:210–217. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Rades D, Kueter JD, Hornung D, Veninga T,
Hanssens P, Schild SE and Dunst J: Comparison of stereotactic
radiosurgery (SRS) alone and whole brain radiotherapy (WBRT) plus a
stereotactic boost (WBRT+SRS) for one to three brain metastases.
Strahlenther Onkol. 184:655–662. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chang EL, Wefel JS, Hess KR, Allen PK,
Lang FF, Kornguth DG, Arbuckle RB, Swint JM, Shiu AS, Maor MH and
Meyers CA: Neurocognition in patients with brain metastases treated
with radiosurgery or radiosurgery plus whole-brain irradiation: A
randomised controlled trial. Lancet Oncol. 10:1037–1044. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Mizumatsu S, Monje ML, Morhardt DR, Rola
R, Palmer TD and Fike JR: Extreme sensitivity of adult neurogenesis
to low doses of X-irradiation. Cancer Res. 63:4021–4027.
2003.PubMed/NCBI
|
|
32
|
Collier TJ, Quirk GJ and Routtenberg A:
Separable roles of hippocampal granule cells in forgetting and
pyramidal cells in remembering spatial information. Brain Res.
409:316–328. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Raber J, Rola R, LeFevour A, Morhardt D,
Curley J, Mizumatsu S, VandenBerg SR and Fike JR: Radiation-induced
cognitive impairments are associated with changes in indicators of
hippocampal neurogenesis. Radiat Res. 162:39–47. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Rades D, Kueter JD, Pluemer A, Veninga T
and Schild SE: A matched-pair analysis comparing whole-brain
radiotherapy plus stereotactic radiosurgery versus surgery plus
whole-brain radiotherapy and a boost to the metastatic site for one
or two brain metastases. Int J Radiat Oncol Biol Phys.
73:1077–1081. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Suh JH: Hippocampal-avoidance whole-brain
radiation therapy: A new standard for patients with brain
metastases? J Clin Oncol. 32:3789–3791. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sahgal A, Larson D and Knisely J:
Stereotactic radiosurgery alone for brain metastases. Lancet Oncol.
16:249–250. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Langley RE, Stephens RJ, Nankivell M, Pugh
C, Moore B, Navani N, Wilson P, Faivre-Finn C, Barton R, Parmar MK
and Mulvenna PM: QUARTZ Investigators: Interim data from the
Medical Research Council QUARTZ Trial: does whole brain
radiotherapy affect the survival and quality of life of patients
with brain metastases from non-small cell lung cancer? Clin Oncol
(R Coll Radiol). 25:e23–e30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Prokic V, Wiedenmann N, Fels F, Schmucker
M, Nieder C and Grosu AL: Whole brain irradiation with hippocampal
sparing and dose escalation on multiple brain metastases: A
planning study on treatment concepts. Int J Radiat Oncol Biol Phys.
85:264–270. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ghia A, Tomé WA, Thomas S, Cannon G,
Khuntia D, Kuo JS and Mehta MP: Distribution of brain metastases in
relation to the hippocampus: Implications for neurocognitive
functional preservation. Int J Radiat Oncol Biol Phys. 68:971–977.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Antonadou D, Coliarakis N, Paraskevaidis
M, Athanasiou H, Sarris G, Synodinou M, Skarlatos I, Sagriotis A,
Georgakopoulos G, Beroukas C, et al: Whole brain radiotherapy alone
or in combination with temazolamide for brain metastases. A phase
III study. Int J Radiat Oncol Biol Phys. 54:932002. View Article : Google Scholar
|