Introduction
Chronic myelogenous leukemia (CML) is characterized
by the presence of the Philadelphia chromosome, which is generated
by the reciprocal translocation, t(9;22) (1). This abnormality is found in >90% of
CML cases, in 15–20% of acute lymphoblastic leukemia cases, and a
small number of acute myeloid leukemia cases (1). Recently, certain studies have reported
that patients with t(8;22) exhibit similar morphological and
clinical features to those observed in CML patients (2–4). Since the
first case reported by Fioretos in 2001 (5), to the best of our knowledge,
t(8;22)(p11;q11) has been reported in only 17 cases with
hematological malignancies (2–17). Of
these, 6 cases presented with atypical CML (2–4,6,7), 3 with
myeloproliferative neoplasms (5,8,9), 3 with B-cell acute lymphoblastic
leukemia (10–12) and 5 with other types of hematological
neoplasms (13–17). t(8;22) results in an in-frame fusion
of FGFR1 on 8p11 and BCR on 22q11, and causes constitutive
activation of the tyrosine kinase of the breakpoint cluster
region/fibroblast growth factor receptor 1 (BCR/FGFR1) chimera
protein, similar to Abelson murine leukemia viral oncogene homolog
1 (ABL) kinase activity in the BCR/ABL chimera (2,18).
The present study reports the 18th case of a
CML-like hematological tumor bearing t(8;22)(p11;q11) with no other
cell lineages involved.
Case report
On February 23, 2013, a 26-year-old woman who was
4-weeks pregnant, with no history of hematological disease, was
found to exhibit an increased white blood cell (WBC) count
(4.0×1010/l; normal range, 0.37–0.92×1010/l)
upon physical examination. Cytogenetic study on the patient's bone
marrow (BM) cells showed a normal female karyotype in all
metaphases. Tests for the BCR/ABL fusion gene and the Janus kinase
2 (JAK2)/Val617Phe mutation were negative. Based on the
morphological examination of the BM, the patient was diagnosed with
CML in Jiangsu Province People's Hospital (Nanjing, China).
On April 9, 2013, the patient was transferred to
Shanghai First People's Hospital (Shanghai, China). Apart from
general fatigue, no other clinical symptoms were apparent.
Laboratory data were as follows: Hemoglobin (Hb), 120 g/l (normal
range, 113–151 g/l); hematocrit, 33.4% (normal range, 35–47%); WBC
count, 3.46×109/l (normal range,
0.37–0.92×109/l); and platelet (Plt) count,
233×109/l (normal range, 100–400×109/l). The
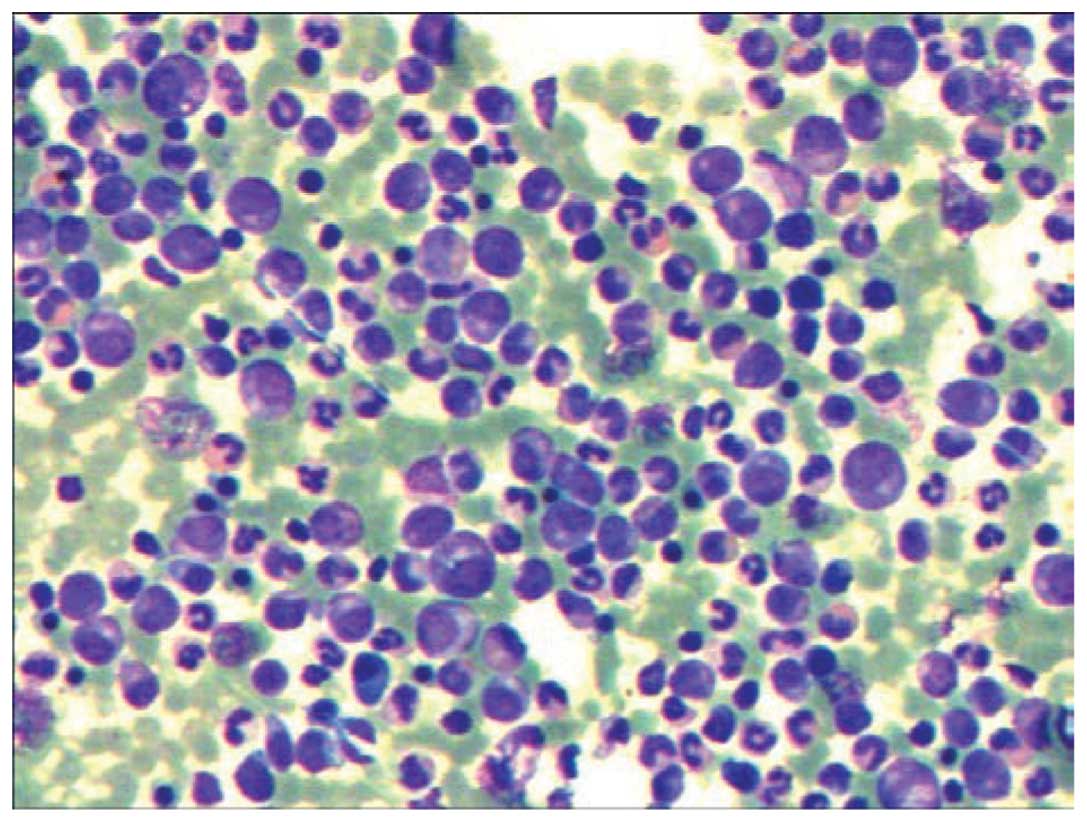
BM differential count was as follows: 3% blasts (normal range,
0.3–2.0%), 2% promyelocytes (normal range, 1–8%), 18% neutrophilic
myelocytes (normal range, 5–20%), 16% neutrophilic metamyelocytes
(normal range, 9–18%), 9% banded neutrophils (normal range, 4–14%),
15% segmented neutrophils (normal range, 7–30%), 13% eosinophils
(normal range, 0.5–4.0%), 2% basophils (normal range, 0–1%), 10%
erythrocytes (normal range, 18.5–39.0%), 7% monocytes (normal
range, 0.5–5.0%) and 5% lymphocytes (normal range, 3–20%) (Fig. 1). The myeloid and erythroid ratio was
increased to 7.8:1 (normal range, 3–5:1), and the neutrophil
alkaline phosphatase score was 4 (normal range, 35–70). No other
cell lineages were proved to be involved, as determined by
multicolor flow cytometry (FCM).
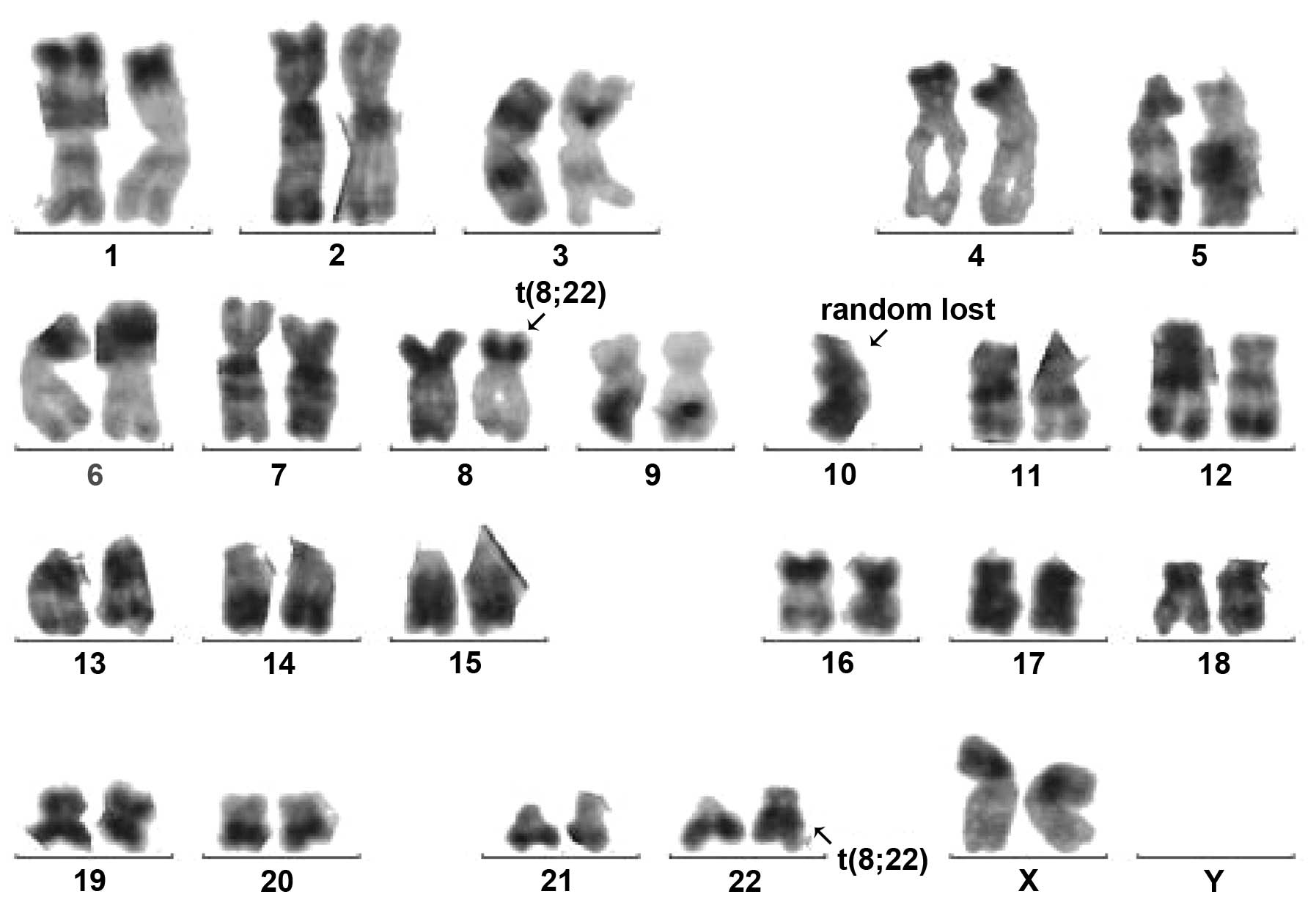
Conventional R-banding analysis of the BM cells
showed 46,XX,t(8;22)(p11;q11) in 9 out of 10 metaphases (Fig. 2). Transcripts of BCR/ABL p210 and p190
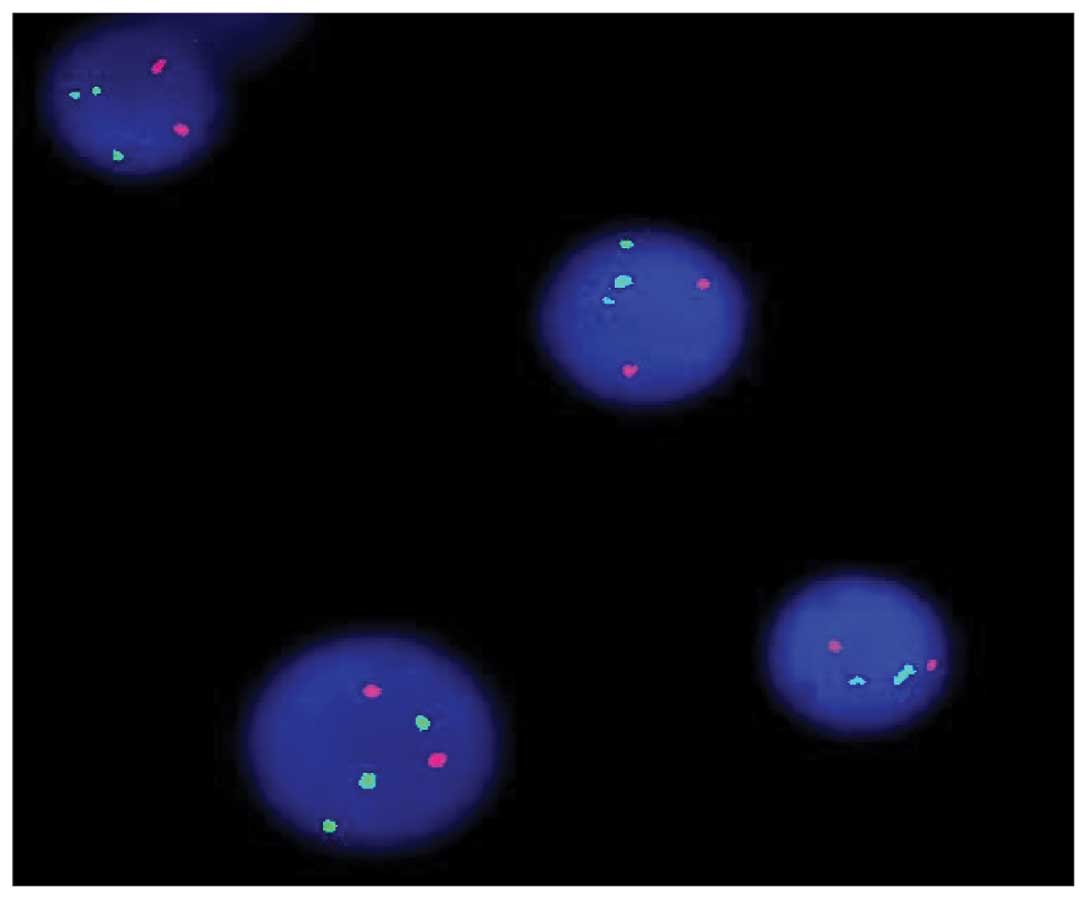
were all negative. Using the LSI BCR/ABL Dual-Color Dual-Fusion
Translocation Probe (Vysis, Downers Grove, IL, USA), fluorescence
in situ hybridization indicated a negative result for the
BCR-ABL fusion, but the BCR probe displayed a split signal, which
suggested that the BCR gene was disrupted (Fig. 3). Reverse transcription-polymerase
chain reaction using primers specific for BCR exon 4 and FGFR1 exon
9 [BCR-E1+ and FGFR9− (2)] confirmed the presence of BCR/FGFR1
transcripts at the molecular level. This result was confirmed by
direct sequencing of the amplified fragment. The diagnosis of
atypical CML was formed once again and hydroxyurea therapy (3 g,
daily, for 3 weeks) was started. However, the patient underwent an
abortion 2 weeks later and returned home to receive further
therapy. The patient was experiencing progression-free survival
with a partial hematological response at the time of
publication.
Discussion
To date, the recurrent t(8;22)(p11;q11)
translocation, which results in a BCR/FGFR1 fusion, has been
reported in 17 patients (2–17), including 16 adult patients (2–8,10–17) and 1
pediatric patient (9); 10 females and
7 males. Of these patients, 14 (82.4%) were >50 years old.
Laboratory data were not available in 2 out of 17 cases (6,8). Of the 15
patients with laboratory data, 13 patients showed an increased WBC
count (median, 5.56×1010/l; range,
1.84–19.8×1010/l), while the remaining 2 displayed a
normal and a decreased WBC count of 5.1×109/l (13) and 1.5×109/l (16), respectively. Among the 15 cases, 10
displayed a decreased Hb level (median, 108 g/l; range, 72–131 g/l)
(4,5,9–11,13–17), and
the majority of these cases exhibited a marginal decrease in Hb
levels. While 2 out of the 15 patients showed increased Plt levels
(9,13), decreased levels were observed in 4
cases (11,14–16) and
the remaining 9 displayed normal levels.
The clinical features reported in the 6 atypical CML
cases with t(8;22) (2–4,6,7) included an older age, systemic symptoms
(fatigue, night sweats and weight loss) and splenomegaly. In the
present case, however, no clinical symptoms were observed upon
physical examination and the patient had been in fair health. In
agreement with the previously described 6 cases, the morphological
picture of the present case was indistinguishable from typical CML.
In the present case, and also in the previously reported 6 cases,
no other additional chromosomal abnormalities were observed except
for t(8;22). FCM also did not show any positive immunophenotype in
the present and previous cases. These results highlight the
importance of cytogenetic and molecular analysis in patients that
present with features of atypical CML. Subsequently, detection of
the genes involved in tyrosine kinase pathways may become an
increasingly important feature of diagnosis.
The clinical features of the remaining 11 cases are
heterogeneous. Among these cases, 9 exhibited a complex karyotype.
The immunophenotypic data of 6 patients had not been described in
the literature (2,3,6,8,9,13). A total of 10 cases exhibited aberrant
proliferation of myeloid and B-lymphoid cells, and T-lymphoid cells
were involved in 1 case (14).
Additional chromosomal abnormalities may explain the observed
heterogeneity with regard to the clinical features and affected
lineages in these patients. These reported cases suggest that
t(8;22) usually presents as CML-like disease, however, it may also
present as AML, T or B lymphoblastic lymphoma/leukemia or a mixed
phenotype acute leukemia. Furthermore, we hypothesize that the
multiphenotypic nature of the disease indicates that the disease
may originate from early progenitor cells, which retain the
potential for both myeloid and lymphoid differentiation. Further
identification and characterization are required to elucidate the
possible molecular mechanisms underlying the disease.
In conclusion, the current study presented a case of
a CML-like patient with t(8;22)(p11;q11) translocation. Detection
of this translocation at diagnosis may become increasingly
important, considering the recent promising development of tyrosine
kinase inhibitory agents.
References
|
1.
|
Wong S and Witte ON: The BCR-ABL story:
Bench to bedside and back. Annu Rev Immunol. 22:247–306. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Demiroglu A, Steer EJ, Heath C, Taylor K,
Bentley M, Allen SL, Koduru P, Brody JP, Hawson G, Rodwell R, et
al: The t(8;22) in chronic myeloid leukemia fuses BCR to FGFR1:
Transforming activity and specific inhibition of FGFR1 fusion
proteins. Blood. 98:3778–3783. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Pini M, Gottardi E, Scaravaglio P,
Giugliano E, Libener R, Baraldi A, Muzio A, Cornaglia E, Saglio G
and Levis A: A fourth case of BCR-FGFR1 positive CML-like disease
with t(8;22) translocation showing an extensive deletion on the
derivative chromosome 8p. Hematol J. 3:315–316. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Murati A, Arnoulet C, Lafage-Pochitaloff
M, Adélaide J, Derré M, Slama B, Delaval B, Popovici C, Vey N,
Xerri L, et al: Dual lympho-myeloproliferative disorder in a
patient with t(8;22) with BCR-FGFR1 gene fusion. Int J Oncol.
26:1485–1492. 2005.PubMed/NCBI
|
|
5.
|
Fioretos T, Panagopoulos I, Lassen C,
Swedin A, Billström R, Isaksson M, Strömbeck B, Olofsson T,
Mitelman F and Johansson B: Fusion of the BCR and the fibroblast
growth factor receptor-1 (FGFR1) genes as a result of
t(8;22)(p11;q11) in a myeloproliferative disorder: The first fusion
gene involving BCR but not ABL. Genes Chromosomes Cancer.
32:302–310. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Agerstam H, Lilljebjörn H, Lassen C,
Swedin A, Richter J, Vandenberghe P, Johansson B and Fioretos T:
Fusion gene-mediated truncation of RUNX1 as a potential mechanism
underlying disease progression in the 8p11 myeloproliferative
syndrome. Genes Chromosomes Cancer. 46:635–643. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Richebourg S, Theisen O, Plantier I, Parry
A, Soenen-Cornu V, Lepelley P, Preudhomme C, Renneville A, Laï JL
and Roche-Lestienne C: Chronic myeloproliferative disorder with
t(8;22)(p11;q11) can mime clonal cytogenetic evolution of authentic
chronic myelogeneous leukemia. Genes Chromosomes Cancer.
47:915–918. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Patnaik MM, Gangat N, Knudson RA, Keefe
JG, Hanson CA, Pardanani A, Ketterling RP and Tefferi A: Chromosome
8p11.2 translocations: Prevalence, FISH analysis for FGFR1 and
MYST3 and clinicopathologic correlates in a consecutive cohort of
13 cases from a single institution. Am J Hematol. 85:238–242. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Dolan M, Cioc A, Cross NC, Neglia JP and
Tolar J: Favorable outcome of allogeneic hematopoietic cell
transplantation for 8p11 myeloproliferative syndrome associated
with BCR-FGFR1 gene fusion. Pediatr Blood Cancer. 59:194–196. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Baldazzi C, Iacobucci I, Luatti S,
Ottaviani E, Marzocchi G, Paolini S, Stacchini M, Papayannidis C,
Gamberini C, Martinelli G, et al: B-cell acute lymphoblastic
leukemia as evolution of a 8p11 myeloproliferative syndrome with
t(8;22)(p11;q11) and BCRFGFR1 fusion gene. Leuk Res. 34:e282–e285.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Wakim JJ, Tirado CA, Chen W and Collins R:
t(8;22)/BCR-FGFR1 myeloproliferative disorder presenting as B acute
lymphoblastic leukemia: Report of a case treated with sorafenib and
review of the literature. Leuk Res. 35:e151–e153. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Haslam K, Langabeer SE, Kelly J, Coen N,
O'Connell NM and Conneally E: Allogeneic hematopoietic stem cell
transplantation for a BCR-FGFR1 myeloproliferative neoplasm
presenting as acute lymphoblastic leukemia. Case Rep Hematol.
2012:6209672012.PubMed/NCBI
|
|
13.
|
Lee SG, Park TS, Lee ST, Lee KA, Song J,
Kim J, Suh B, Choi JR and Park R: Rare translocations involving
chromosome band 8p11 in myeloid neoplasms. Cancer Genet Cytogenet.
186:127–129. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Kim SY, Oh B, She CJ, Kim HK, Jeon YK,
Shin MG, Yoon SS and Lee DS: 8p11 myeloproliferative syndrome with
BCR-FGFR1 rearrangement resenting with T-lymphoblastic lymphoma and
bone marrow stromal cell proliferation: A case report and review of
the literature. Leuk Res. 35:e30–e34. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Morishige S, Oku E, Takata Y, Kimura Y,
Arakawa F, Seki R, Imamura R, Osaki K, Hashiguchi M, Yakushiji K,
et al: A Case of 8p11 myeloproliferative syndrome with BCR-FGFR1
gene fusion presenting with trilineage acute leukemia/lymphoma,
successfully treated by cord blood transplantation. Acta Haematol.
129:83–89. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Shimanuki M, Sonoki T, Hosoi H, Watanuki
J, Murata S, Mushino T, Kuriyama K, Tamura S, Hatanaka K, Hanaoka N
and Nakakuma H: Acute leukemia showing t(8;22)(p11;q11),
myelodysplasia, CD13/CD33/CD19 expression and immunoglobulin heavy
chain gene rearrangement. Acta Haematol. 129:238–242. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Matikas A, Tzannou I, Oikonomopoulou D and
Bakiri M: A case of acute myelogenous leukaemia characterised by
the BCR-FGFR1 translocation. BMJ Case Rep.
2013:bcr20130088342013.PubMed/NCBI
|
|
18.
|
Roumiantsev S, Krause DS, Neumann CA,
Dimitri CA, Asiedu F, Cross NC and Van Etten RA: Distinct stem cell
myeloproliferative/T lymphoma syndromes induced by ZNF198-FGFR1 and
BCR-FGFR1 fusion genes from 8p11 translocations. Cancer Cell.
5:287–298. 2004. View Article : Google Scholar : PubMed/NCBI
|