Introduction
Ovarian cancer patients demonstrate poor survival;
the five-year survival rate for patients with advanced stage [FIGO
stage III–IV (1)] disease is just
30.6% (2,3). Despite a high initial response rate to
primary treatments, 75% of patients eventually relapse and succumb
to the disease (2,4). Responses to second-line chemotherapy for
recurrence occur in ≥60% of platinum-sensitive patients, with ~25%
of these patients achieving complete responses (5,6). Although
there is much published data on the survival outcomes of various
third-line chemotherapy options, limited information is available
specifically regarding the response to chemotherapy. Generally,
chemotherapy is considered the best initial treatment option for
patients with incurable cancer (7–9). The
challenge for the physician is to continuously balance the pros and
cons in each individual patient, so as to optimize tumor response
while minimizing adverse effects. Decisions about chemotherapy
should consider various clinical factors, including the performance
status (PS) of the patient and the likely tumor response and
patient survival time. In particular, the prediction of the
survival time is important. Evidence of deterioration and adverse
effects should be monitored closely to avoid overtreatment
(8).
In addition to clinical predictors of the survival
duration, such as PS, possible prognostic biomarkers associated
with the systemic inflammatory processes have been examined in
various types of cancer, as inflammation in tumors has previously
been identified to enable various cancer characteristics and to be
important in determining the prognosis (10). Changes in the proportions of the
subtypes of white blood cells have been the most frequently
evaluated of these biomarkers, as they are easily assessable and
economically feasible potential markers of cancer prognosis
(11,12). The neutrophil to lymphocyte ratio
(NLR) and the platelet to lymphocyte ratio (PLR) have attracted the
interest of studies as systemic inflammatory markers of prognosis
(13,14). Several studies have reported that
peripheral blood NLR and PLR measured during the pre-operative or
pre-treatment phase are independent predictors of poor prognosis in
various cancers, including pancreatic, breast, colon, lung and
gastric cancer (15–19). However, associations between the NLR
and PLR and the tumor responses and survival of patients receiving
chemotherapy have not been examined.
Therefore, in the present study, the association
between the NLR and PLR and the PS, tumor response and survival
time were investigated in patients with recurrent epithelial
ovarian cancer subsequent to the administration of chemotherapy, in
which the response to chemotherapy had been monitored by serial
cancer antigen 125 (CA125) concentrations (20).
Patients and methods
Patients
The present study was a retrospective analysis of 30
ovarian cancer patients with recurrence that had been treated in
the Department of Obstetrics and Gynecology of Okayama University
Hospital (Okayama, Okayama, Japan) between April 2005 and April
2013. The primary treatment received by these patients was complete
cytoreductive surgery and adjuvant and/or neo-adjuvant chemotherapy
with conventional taxotere and cyclophosphamide (TC) [180
mg/m2 paclitaxel infused over 3 h; carboplatin, dosage
calculated for an area under the curve (AUC) of 5 infused over 1 h;
Bristol-Myers Squibb, New York, NY, USA]. Following primary
treatment, the patients underwent follow-up examinations every 1–2
months for the first 6 months, every 3 months for the next 2 years,
and every 6 months thereafter. The present protocol was approved by
the Institutional Review Board of Okayama University Hospital.
Informed consent was obtained from all patients.
Chemotherapy
The policy of the Department of Obstetrics and
Gynecology of Okayama University Hospital required an Eastern
Cooperative Oncology Group PS of ≤2 (21) prior to initiating chemotherapy. In the
present study, no patients showed clinical or radiographic evidence
of relapse within 6 months subsequent to completing adjuvant and/or
neo-adjuvant chemotherapy with conventional TC. Conventional TC was
also administered as second-line chemotherapy to patients that
developed evidence of clinical or radiographic relapse within the 6
months subsequent to completing adjuvant and/or neo-adjuvant
chemotherapy. Chemotherapy for the treatment of recurrent disease
was continued until complete response (CR) or progressive disease
(PD) was identified. Patients with PD received regimens of
chemotherapy that were different from the adjuvant and second-line
combinations. The second line chemotherapy consisted of weekly TC
(paclitaxel, 80 mg/m2; carboplatin, AUC of 2.0). Third,
fourth and fifth-line chemotherapy was either single agent
irinotecan (CPT-11; 70 mg/m2 weekly for 3 weeks followed
by 1 week off; Yakult, Tokyo, Japan), pegylated liposomal
doxorubicin (Doxil; 40 mg/m2 once every four weeks;
Janssen, Tokyo, Japan), or gemcitabine (700 mg/m2 weekly
for 3 weeks followed by 1 week off; Eli Lilly and Company,
Indianapolis, IN, USA). The objective responses of the patients
were principally evaluated using the Response Evaluation Criteria
in Solid Tumors guidelines (version 1.1) (22). Patients with recurrence that occurred
in a single site, and therefore underwent secondary surgical
cytoreduction, and those in whom granulocyte colony stimulating
factor was used were excluded from the present study.
NLR, PLR and CA125
All subjects underwent complete blood and
differential white blood cell counts prior to commencing
chemotherapy. The NLR was defined as the absolute neutrophil count
divided by the absolute lymphocyte count, and the PLR was defined
as the absolute platelet count divided by the lymphocyte count
(Bayer HealthCare, Tarrytown, NY, USA). Serum CA125 concentrations
were measured using an electrochemiluminescence immunoassay using
Hitachi Modular Analytics E170 (Roche Diagnostics, Tokyo, Japan).
Additionally, NLR, PLR and CA125 concentrations were measured prior
to commencing treatment for recurrent ovarian cancer. Since
objectively measurable criteria for assessing the response to
chemotherapy were considered important, changes in the NLR and PLR
values and CA125 concentrations were evaluated as single prognostic
criteria and in combination with other clinical response
criteria.
Statistical analysis
Statistical analyses were performed using the
Mann-Whitney U-test for comparisons with controls and one-way
analysis of variance followed by Fisher's protected least
significant difference test for all pairwise comparisons. Receiver
operating characteristic (ROC) curves were generated for
pre-treatment NLR, PLR and CA125 concentrations prior to final line
chemotherapy to determine the cut-off values for predicting
survival for >100 days that yielded optimal sensitivity and
specificity. The patients were then allocated to groups based on
the cut-off values. Univariate and multivariate analyses using
Cox's proportional hazards model were performed to determine the
biomarkers that predicted survival subsequent to adjusting for the
effects of known prognostic factors. Analyses were performed using
SPSS software version 20.0 (IBM, Armonk, NY, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
Patient characteristics
The histological types of ovarian cancer included in
the present study and the duration of recurrence-free survival are
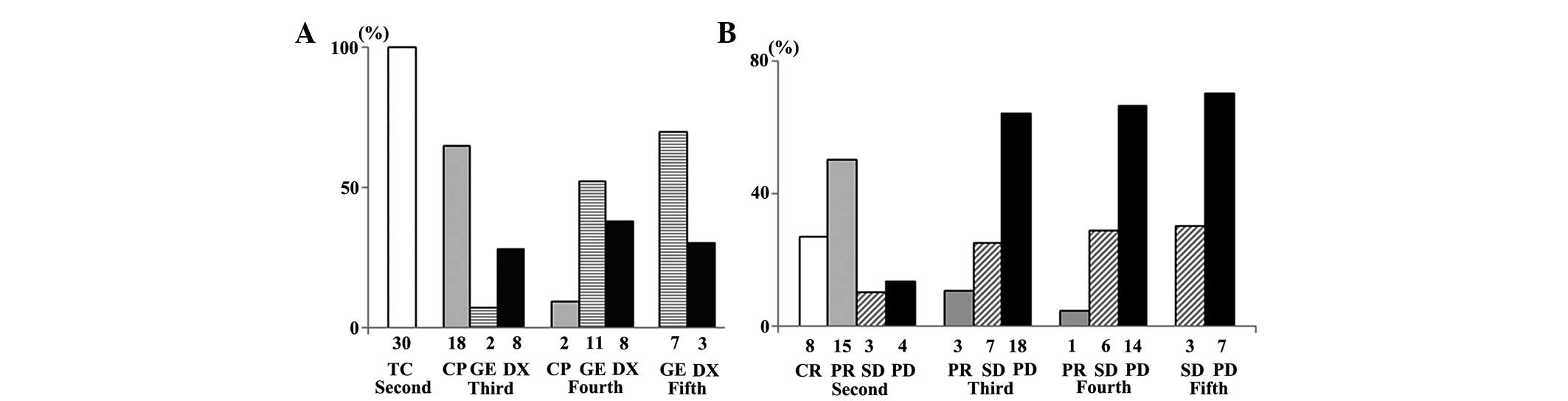
listed in Table I. Following disease
recurrence, 30 (100%), 28 (93.3%), 21 (70.0%) and 10 (33.3%)
patients received second, third, fourth and fifth-line
chemotherapy, respectively (Fig. 1A).
The tumor responses of patients that received second to fifth-line
chemotherapy are exhibited in Fig.
1B. The tumor response and disease control rates were 76.7 and
86.7%, respectively, for second-line chemotherapy, 10.7 and 35.7%,
respectively, for third-line chemotherapy, 4.3 and 33.3%,
respectively, for fourth-line chemotherapy, and 0.0 and 30.0%,
respectively, for fifth-line chemotherapy. The median number of
cycles of second, third, fourth and fifth-line chemotherapy
received were 16 (range, 5–27), 7 (range, 2–27), 6 (range, 2–20),
and 5 (range, 2–18), respectively.
 | Table I.Characteristics of patients with
ovarian cancer. |
Table I.
Characteristics of patients with
ovarian cancer.
| Baseline
characteristics | Patients, n (%) |
|---|
| Age at diagnosis,
mean years (range) | 54.9 (33–78) |
| Histology |
|
| High
grade serous adenocarcinoma | 30 (100.0) |
| RFS time |
|
| 7–12
months | 23 (76.7) |
| 13–24
months | 5
(16.6) |
| >25
months | 2 (6.7) |
Association between chemotherapy line
and the NLR, PLR and CA125 concentration of patients
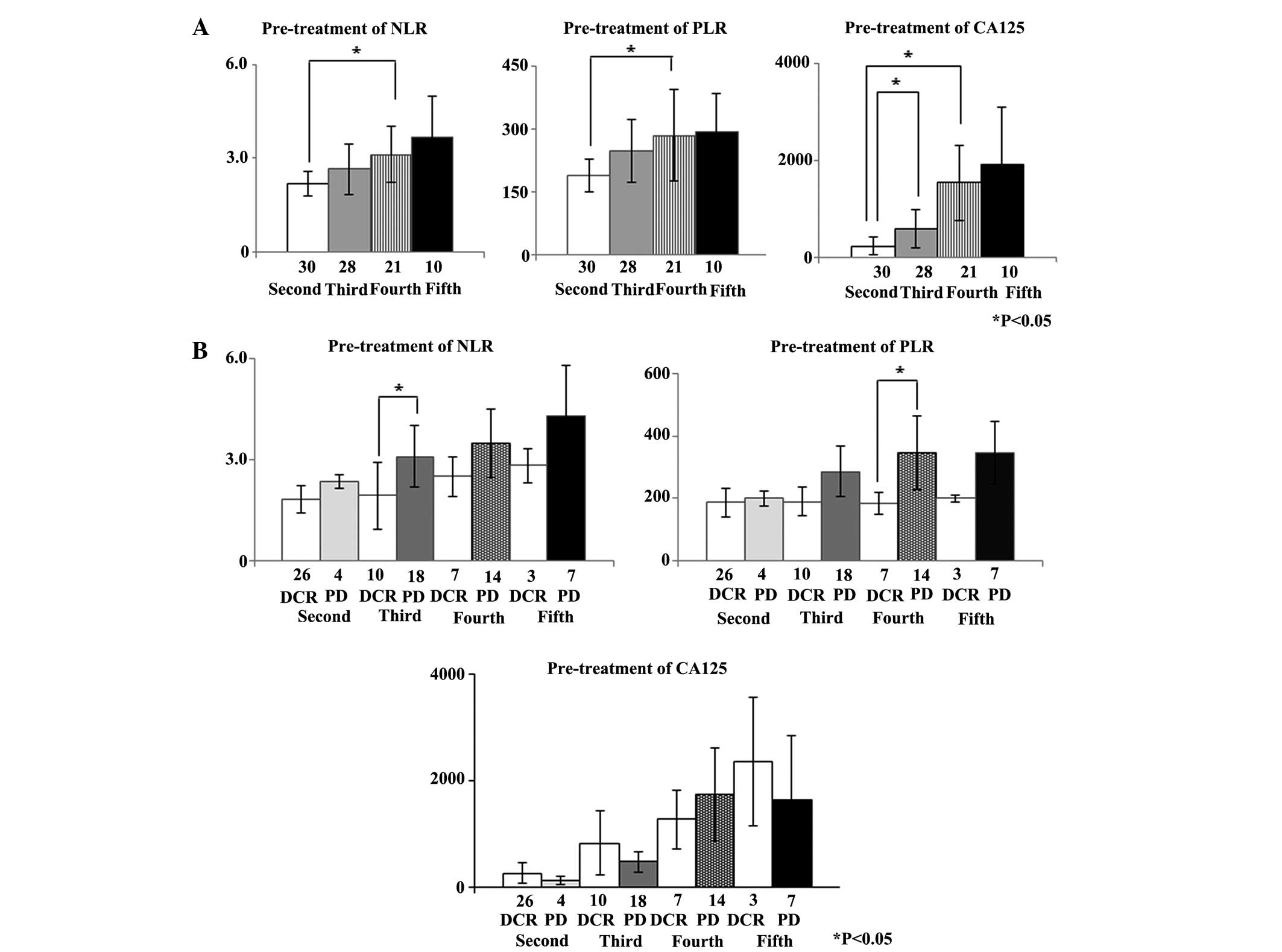
The pre-treatment NLR, PLR and CA125 concentrations
were calculated for second to fifth-line chemotherapy. The mean
pre-treatment NLR (±2 SD) for second, third, fourth and fifth-line
chemotherapy was 2.24±0.74, 2.64±1.56, 3.12±1.72 and 3.66±2.70,
respectively. The mean pre-treatment PLR (±2 SD) for second, third,
fourth and fifth-line chemotherapy was 188.6±87.5, 246.8±152.2,
284.2±210.8 and 293.2±182.5, respectively. The mean pre-treatment
CA125 concentration (±2 SD) for second, third, fourth and
fifth-line chemotherapy was 238.1±385.6, 597.0±808.0,
1539.2±1568.6, and 1919.0±2462.0 U/ml, respectively. The
pre-treatment NLR and PLR for fourth-line chemotherapy were
significantly increased compared with those for second-line
chemotherapy (P=0.029 and 0.049, respectively). The mean
pre-treatment CA125 concentrations for third and fourth-line
chemotherapy were significantly increased compared with the mean
pre-treatment CA125 concentrations for second-line chemotherapy
(P=0.039 and 0.001, respectively) (Fig.
2A).
Whether the pre-treatment NLR, PLR and CA125
concentrations for second to fifth-line chemotherapy were
associated with the disease control rate (DCR), including CR,
partial response (PR), and stable disease (SD) was assessed. For
third-line chemotherapy, the mean pre-treatment NLR of patients
with subsequent PD was increased compared with the mean
pre-treatment NLR for patients that achieved CR, PR, and SD
(P=0.022). Similarly, the mean pre-treatment PLR for patients with
subsequent PD was significantly increased compared with the mean
pre-treatment PLR for patients that achieved CR, PR, and SD with
fourth-line chemotherapy (P=0.032). However, there was no
association between the CA125 concentration and tumor response for
any line of chemotherapy (Fig.
2B).
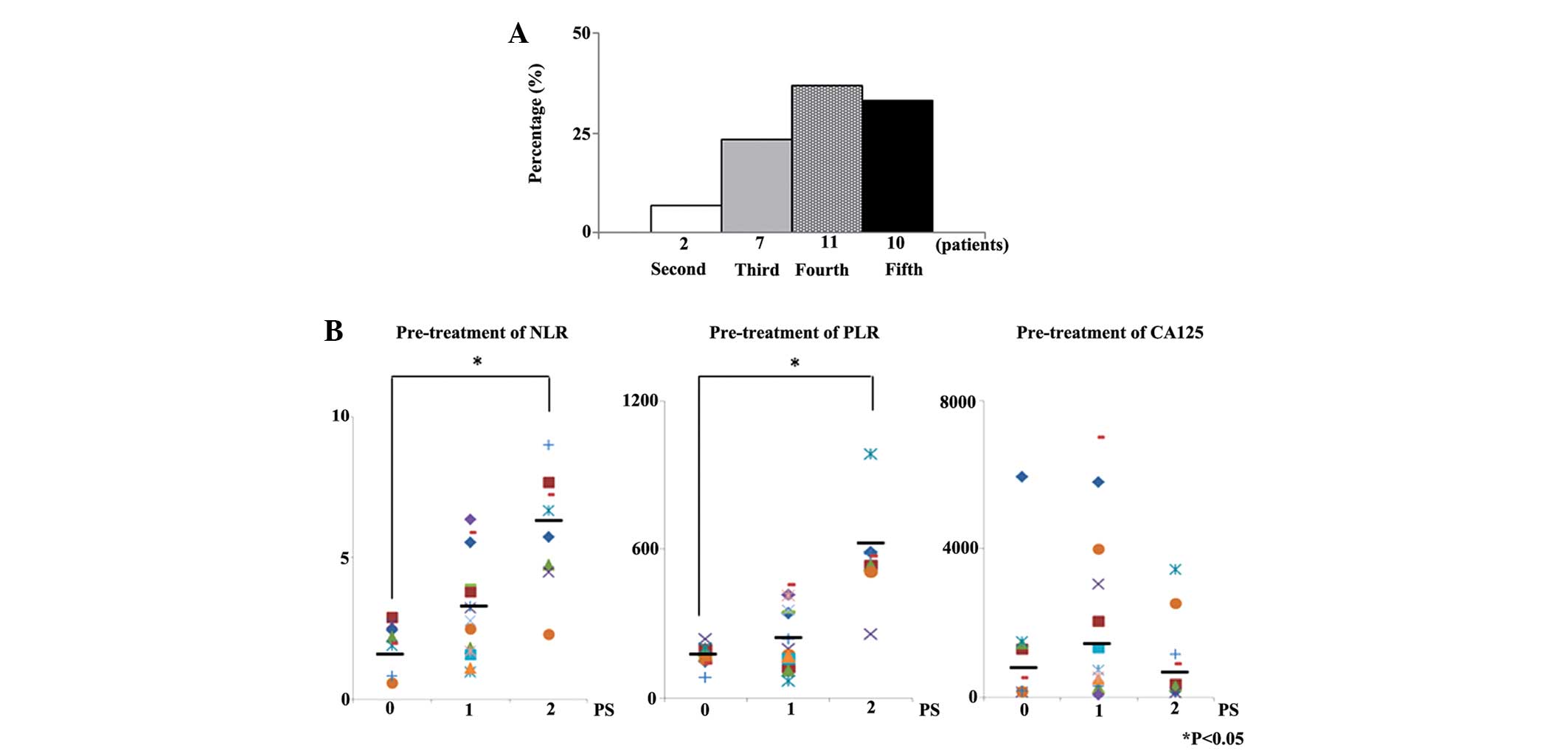
Of the 30 patients that succumbed, 2 (6.7%) had
received second-line chemotherapy, 7 (23.3%) third-line
chemotherapy, 11 (36.7%) fourth-line chemotherapy, and 10 (33.3%)
fifth-line chemotherapy as their last line of chemotherapy
(Fig. 3A).
Whether the pre-treatment NLR, PLR, CA125
concentration and PS were associated with final-line chemotherapy
was also examined in the present study. Pre-treatment NLR and PLR
of patients with PS of 2 were significantly higher than those of
patients with a PS of 0 prior to final line chemotherapy
(P<0.001 and P<0.001). However, CA125 concentration prior to
final line chemotherapy was not associated with PS (Fig. 3B).
The time between final line chemotherapy and
mortality was ≤100 days in 11 patients (36.7%), 101–200 days in 8
(26.7%), 201–300 days in 5 (16.6%), 301–400 days in 4 (13.3%), and
≥401 days in 2 (6.7%) (Fig. 4A).
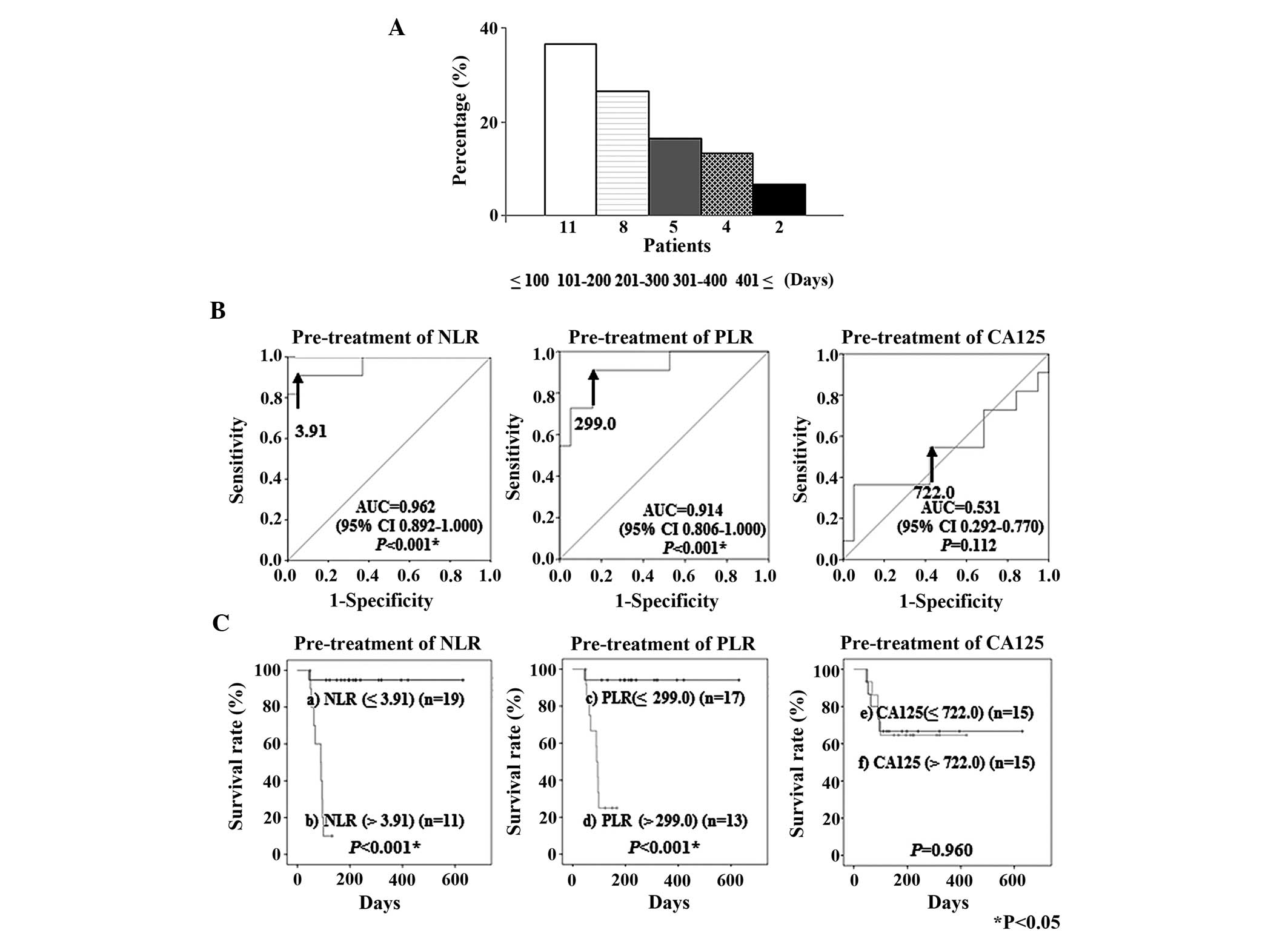 | Figure 4.(A) Time between final-line
chemotherapy and mortality in patients with recurrent ovarian
cancer. (B) Receiver operating characteristic curves for the
ability of pre-treatment NLR, PLR and CA125 concentrations to
predict mortality within 100 days of final-line chemotherapy. The
optimal cut-off value for pre-treatment NLR was 3.91 (AUC, 0.962;
95% CI, 0.892–1.000; P<0.001), for PLR it was 299.0 (AUC, 0.914;
95% CI, 0.806–1.000; P<0.001), and for CA125 concentrations it
was 722.0 U/ml (AUC, 0.531; 95% CI, 0.292–0.770; P=0.112). (C)
Kaplan-Meier plots for the survival rates of 30 patients with
recurrent ovarian cancer, based on the pre-treatment NLR, PLR and
serum CA125 values. a), NLR ≤3.91 (n=19); b), NLR >3.91 (n=11);
c), PLR ≤299.0 (n=17); d), PLR >299.0 (n=13), e) serum CA125
concentrations ≤722.0 U/ml (n=15); and f), serum CA125
concentrations >722.0 U/ml (n=15). NLR, neutrophil to lymphocyte
ratio; PLR, platelet to lymphocyte ratio; CA125, cancer antigen
125; AUC, area under the curve; U/ml, units/ml. |
ROC curve analysis
ROC curve analyses were performed to determine the
cut-off values for the pre-treatment NLR, PLR and CA125
concentrations that predicted mortality within 100 days of the
failure of final line chemotherapy. These analyses identified a
cut-off value for a pre-treatment NLR of 3.91 (AUC, 0.962;
sensitivity, 90.9%; specificity, 94.7%), for a pre-treatment PLR of
299.0 (AUC, 0.914; sensitivity, 90.9%; specificity, 84.2%) and for
a pre-treatment CA125 concentration of 722.0 (units/ml) (AUC,
0.531; sensitivity, 54.5%; specificity, 52.6%) (Fig. 4B). When patients were classified into
the regions above and below each cut-off value for survival,
Kaplan-Meyer curves of survival demonstrated that patients with a
high NLR and PLR had significantly shorter survival times than
patients with a low NLR and PLR (P<0.001 and P<0.001,
respectively) (Fig. 4C).
Association between clinical factors
and mortality
The association between clinical factors and
mortality within 100 days of the failure of final-line chemotherapy
was assessed by univariate and multivariate analyses. According to
the univariate analyses, pre-treatment NLR >3.91, pre-treatment
PLR >299.0 and PS 2 were significantly associated with mortality
within 100 days of the failure of final-line chemotherapy (P=0.001,
0.005 and 0.021, respectively). Furthermore, multivariate analyses
demonstrated that patients with high pre-treatment NLR had a
significantly increased hazard ratio (14.128) for mortality within
100 days subsequent to failure of final line chemotherapy compared
with patients without this risk factor (P=0.035) (Table II).
| Table II.Prognostic factors for mortality
within 100 days of the failure of final-line chemotherapy. |
Table II.
Prognostic factors for mortality
within 100 days of the failure of final-line chemotherapy.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | Hazard ratio | 95% CI | P-value | Hazard ratio | 95% CI | P-value |
|---|
| Years (>60
years) |
1.202 | 0.339–4.264 | 0.776 |
|
|
|
| RFS (≤12
months) |
3.339 | 0.423–26.376 | 0.253 |
|
|
|
| Over fourth line
chemotherapy |
0.905 | 0.234–3.509 | 0.886 |
|
|
|
| Pre-treatment NLR
(>3.91) | 31.667 | 3.887–257.963 |
0.001* | 14.128 | 1.207–165.400 |
0.035* |
| Pre-treatment PLR
(>299.0) | 19.173 | 2.396–153.423 |
0.005* |
4.628 | 0.432–49.567 | 0.205 |
| CA125
(>722.0) |
1.032 | 0.299–3.568 | 0.960 |
|
|
|
| PS (2) |
4.362 | 1.248–15.240 |
0.021* |
0.974 | 0.258–3.667 | 0.969 |
Discussion
Predictors of the outcome of multiple metastases in
cancer patients with recurrence include factors associated with the
response to chemotherapy (23). The
decision to administer chemotherapy should consider various
clinical factors, including PS, likely tumor response and survival.
In particular, the prediction of the survival time is important.
Evidence of the deterioration and adverse effects associated with
chemotherapy should be monitored closely to avoid over-treatment
(8).
In addition to the clinical predictors of the
duration of survival, including the PS, factors associated with
systemic inflammatory processes have been examined for possible
roles as biomarkers of prognosis in various types of cancer
(24). Neutrophils and T and
B-lymphocytes have been suggested as prominent in inflammatory and
immunological responses to tumors (25,26).
Inflammatory responses to tumors are mediated by the release from
neutrophils of inflammatory cytokines, leukocytic and other
phagocytic mediators that induce damage to cellular DNA, inhibit
apoptosis and promote cancer-associated angiogenesis (11,27,28).
Platelets may be important for releasing potent mitogens or
glycoproteins, such as platelet-derived growth factor, platelet
factor 4, transforming growth factor β, vascular endothelial growth
factor and thrombospondin, which adhere to various cell types,
including ovarian surface epithelium (29–33).
Various ratios of neutrophil, platelet and lymphocyte counts,
notably the NLR and PLR, have attracted the interest of
investigators as possible markers of systemic inflammation, and
therefore of prognosis (15–19). High pre-treatment NLR and PLR have
reportedly been significantly associated with mortality in various
types of cancer (12–16). High NLR is an independent indicator of
poor prognosis in patients with epithelial ovarian cancer (34) and PLR is a better predictor of
survival of these patients (35).
However, no studies have reported correlations between the
pre-treatment NLR and PLR, tumor response or pre-treatment CA125
concentrations and the survival of patients with recurrent ovarian
cancer following chemotherapy. Therefore, in the present study,
these associations were assessed.
The pre-treatment NLR, PLR and CA125 concentrations
for patients that received second to fifth-line chemotherapy were
calculated. The NLR and PLR prior to fourth-line chemotherapy were
significantly greater than prior to second-line chemotherapy.
Pre-treatment CA125 concentrations for patients that received third
and fourth-line chemotherapy were significantly greater than for
patients that received second-line chemotherapy. In addition,
associations between pre-treatment NLR and PLR and DCR for each
line of chemotherapy were assessed. Prior to third-line
chemotherapy, patients that later developed PD had significantly
greater pre-treatment NLR compared with those that achieved CR, PR
and SD. Prior to fourth-line chemotherapy, patients that went on to
develop PD had significantly greater PLR compared with patients
that achieved CR, PR and SD.
The less sensitive a cancer is to chemotherapy, the
more consideration treatment decisions require (19). The duration of survival is challenging
to predict; however, poor PS is one of the strongest predictors of
a short survival time (8,24). In the present study, whether NLR, PLR
and CA125 concentrations prior to final line chemotherapy were
associated with PS was examined. PS was identified to be
significantly correlated with the pre-treatment NLR and PLR.
Furthermore, prior to final-line chemotherapy, patients with a
worse PS (PS 2) had significantly greater NLR and PLR than patients
with a better PS (PS 0).
In the present study, 36.7% of patients with
recurrent epithelial ovarian cancer subsequent to chemotherapy
received final line chemotherapy within 100 days prior to
mortality. This is consistent with other studies, such as one study
in which 30% of patients received final-line chemotherapy in the
final month of life (36) and another
in which 50% of patients received treatment in the final two months
of life (37). One of the aims of the
present study was to determine whether the NLR and PLR values and
CA125 concentration prior to final-line chemotherapy may predict
mortality within 100 days. ROC curve analyses were used to
determine the optimal cut-off values for predicting mortality
within 100 days of final line chemotherapy. The cut-off values for
the pre-treatment NLR and PLR values and CA125 concentration were
3.91, 299.00 and 722 units (U)/ml, respectively, for survival for
<100 days subsequent to final-line chemotherapy. According to
univariate analyses using the determined cut-off values,
pre-treatment NLR >3.91, PLR >299.0 and PS 2 were
significantly associated with the outcomes of patients following
failure of final-line chemotherapy. Multivariate analysis
demonstrated that pre-treatment NLR (>3.91) was an independent
negative indicator of the duration of survival time following the
failure of final-line chemotherapy.
The limitations of the present study have been
acknowledged. First, the number of patients was relatively small.
Second, the duration of the follow-up was relatively short.
Additional prospective studies with larger patient numbers and
longer follow-up periods may provide more definitive data to
clarify the significance of the findings.
In summary, the findings of the present study
suggest that the pre-treatment NLR is an important predictor of the
outcome of patients with recurrent ovarian cancer following
chemotherapy.
References
|
1.
|
Prat J: FIGO Committee on Gynecologic
Oncology: Staging classification for cancer of the ovary, fallopian
tube, and peritoneum. Int J Gynaecol Obstet. 124:1–5. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Cannistra SA: Cancer of the ovary. N Engl
J Med. 351:2519–2529. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Clarke-Pearson DL: Clinical practice.
Screening for ovarian cancer. N Engl J Med. 361:170–177. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Covens A, Carey M, Bryson P, Verma S, Fung
Kee, Fung M and Johnston M: Systematic review of first-line
chemotherapy for newly diagnosed postoperative patients with stage
II, III, or IV epithelial ovarian cancer. Gynecol Oncol. 85:71–80.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Parmar MK, Ledermann JA, Colombo N, du
Bois A, Delaloye JF, Kristensen GB, Wheeler S, Swart AM, Qian W,
Torri V, et al: ICON and AGO Collaborators: Paclitaxel plus
platinum-based chemotherapy versus conventional platinum-based
chemotherapy in women with relapsed ovarian cancer: The
ICON4/AGO-OVAR-2.2 trial. Lancet. 361:2099–2106. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Alberts DS, Liu PY, Wilczynski SP, Clouser
MC, Lopez AM, Michelin DP, Lanzotti VJ and Markman M: Southwest
Oncology Group: Randomized trial of pegylated liposomal doxorubicin
(PLD) plus carboplatin versus carboplatin in platinum-sensitive
(PS) patients with recurrent epithelial ovarian or peritoneal
carcinoma after failure of initial platinum-based chemotherapy
(Southwest Oncology Group Protocol S0200). Gynecol Oncol.
108:90–94. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
O'Brien ME, Yau T, Coward J, Hughes S,
Papadopoulos P, Popat S, Norton A and Ashley S: Time and
chemotherapy treatment trends in the treatment of elderly patients
(age>or=70 years) with non-small cell lung cancer. Clin Oncol (R
Coll Radiol). 20:142–147. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Kim A, Fall P and Wang D: Palliative care:
Optimizing quality of life. J Am Osteopath Assoc. 105(Suppl 5):
S9–S14. 2005.PubMed/NCBI
|
|
9.
|
Renouf D, Kennecke H and Gill S: Trends in
chemotherapy utilization for colorectal cancer. Clin Colorectal
Cancer. 7:386–389. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Lee Y, Kim SH, Han JY, Kim HT, Yun T and
Lee JS: Early neutrophil-to-lymphocyte ratio reduction as a
surrogate marker of prognosis in never smokers with advanced lung
adenocarcinoma receiving gefitinib or standard chemotherapy as
first-line therapy. J Cancer Res Clin Oncol. 138:2009–2016. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Balkwill F and Mantovani A: Inflammation
and cancer: Back to Virchow? Lancet. 357:539–545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Templeton AJ, McNamara MG, Šeruga B,
Vera-Badillo FE, Aneja P, Ocaña A, Leibowitz-Amit R, Sonpavde G,
Knox JJ, Tran B, et al: Prognostic role of neutrophil-to-lymphocyte
ratio in solid tumors: A systematic review and meta-analysis. J
Natl Cancer Inst. 106:dju1242014. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Templeton AJ, Ace O, McNamara MG,
Al-Mubarak M, Vera-Badillo FE, Hermanns T, Seruga B, Ocaña A,
Tannock IF and Amir E: Prognostic role of platelet to lymphocyte
ratio in solid tumors: A systematic review and meta-analysis.
Cancer Epidemiol Biomarkers Prev. 23:1204–1212. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Aliustaoglu M, Bilici A, Seker M, Dane F,
Gocun M, Konya V, Ustaalioglu BB and Gumus M: The association of
pre-treatment peripheral blood markers with survival in patients
with pancreatic cancer. Hepatogastroenterology. 57:640–645.
2010.PubMed/NCBI
|
|
16.
|
Azab B, Bhatt VR, Phookan J, Murukutla S,
Kohn N, Terjanian T and Widmann WD: Usefulness of the
neutrophil-to-lymphocyte ratio in predicting short- and long-term
mortality in breast cancer patients. Ann Surg Oncol. 19:217–224.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Kishi Y, Kopetz S, Chun YS, Palavecino M,
Abdalla EK and Vauthey JN: Blood neutrophil-to-lymphocyte ratio
predicts survival in patients with colorectal liver metastases
treated with systemic chemotherapy. Ann Surg Oncol. 16:614–622.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Sarraf KM, Belcher E, Raevsky E, Nicholson
AG, Goldstraw P and Lim E: Neutrophil/lymphocyte ratio and its
association with survival after complete resection in non-small
cell lung cancer. J Thorac Cardiovasc Surg. 137:425–428. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Yamanaka T, Matsumoto S, Teramukai S,
Ishiwata R, Nagai Y and Fukushima M: The baseline ratio of
neutrophils to lymphocytes is associated with patient prognosis in
advanced gastric cancer. Oncology. 73:215–220. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Bast RC Jr, Klug TL, St John E, Jenison E,
Niloff JM, Lazarus H, Berkowitz RS, Leavitt T, Griffiths CT, Parker
L, et al: A radioimmunoassay using a monoclonal antibody to monitor
the course of epithelial ovarian cancer. N Engl J Med. 309:883–887.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Prommer E: Guidelines for the use of
palliative chemotherapy. AAHPM Bulletin. 5:2–13. 2004.
|
|
24.
|
McIllmurray M: Symptom management. Oxford
Textbook of Palliative Medicine. Doyle D, Hanks G, Cherny NI and
Calman K: (3rd). (New York, NY). Oxford University Press. 229–239.
2004.
|
|
25.
|
Lin X, Li W, Lai J, Okazaki M, Sugimoto S,
Yamamoto S, Wang X, Gelman AE, Kreisel D and Krupnick AS: Five-year
update on the mouse model of orthotopic lung transplantation:
Scientific uses, tricks of the trade, and tips for success. J
Thorac Dis. 4:247–258. 2012.PubMed/NCBI
|
|
26.
|
Schreiber RD, Old LJ and Smyth MJ: Cancer
immunoediting: Integrating immunity's roles in cancer suppression
and promotion. Science. 331:1565–1570. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Jackson JR, Seed MP, Kircher CH,
Willoughby DA and Winkler JD: The codependence of angiogenesis and
chronic inflammation. FASEB J. 11:457–465. 1997.PubMed/NCBI
|
|
28.
|
McMillan DC, Canna K and McArdle CS:
Systemic inflammatory response predicts survival following curative
resection of colorectal cancer. Br J Surg. 90:215–219. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Assoian RK and Sporn MB: Type beta
transforming growth factor in human platetlets: Release during
platelet degranulation and action on vascular smooth muscle cells.
J Cell Biol. 102:1217–1223. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Dubernard V, Arbeille BB, Lemesle MB and
Legrand C: Evidence for an alpha-granular pool the cytoskeletal
protein alpha-actinin in human platelets that redistributes with
the adhesive glycoprotein thrombospondin-1 during the exocytotic
process. Arterioscler Thromb Vasc Biol. 17:2293–2305. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Kaplan KL, Broekman MJ, Chernoff A,
Lesznik GR and Drillings M: Platelet alpha-granule proteins:
Studies on release and subcellular localization. Blood. 53:604–618.
1979.PubMed/NCBI
|
|
32.
|
Qian X and Tuszynski GP: Expression of
thrombospondin-1 in cancer: A role in tumor progression. Proc Soc
Exp Biol Med. 212:199–207. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Dabrow MB, Francesco MR, McBrearty FX and
Caradonna S: The effects of platelet-derived growth factor and
receptor on normal and neoplastic human ovarian surface epithelium.
Gynecol Oncol. 71:29–37. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Cho H, Hur HW, Kim SW, Kim SH, Kim JH, Kim
YT and Lee K: Pre-treatment neutrophil to lymphocyte ratio is
elevated in epithelial ovarian cancer and predicts survival after
treatment. Cancer Immunol Immunother. 58:15–23. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Asher V, Lee J, Innamaa A and Bali A:
Preoperative platelet lymphocyte ratio as an independent prognostic
marker in ovarian cancer. Clin Transl Oncol. 13:499–503. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
36.
|
Matsuyama R, Reddy S and Smith TJ: Why do
patients choose chemotherapy near the end of life? A review of the
prospective of those facing death from cancer. J Clin Oncol.
24:3490–3496. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37.
|
Keam B, Oh DY, Lee SH, Kim DW, Kim MR, Im
SA, Kim TY, Bang YJ and Heo DS: Aggressiveness of cancer-care near
the end-of-life in Korea. Jpn J Clin Oncol. 38:381–386. 2008.
View Article : Google Scholar : PubMed/NCBI
|