Introduction
Gastrointestinal stromal tumors (GISTs) are the most
common gastrointestinal tract tumors of mesenchymal origin. Those
occurring outside of the gastrointestinal tract comprise a specific
type of GIST, known as extra-gastrointestinal stromal tumors
(EGISTs) (1). EGISTs share similar
biological and histological characteristics with GISTs, and
predominantly occur in the omentum, retroperitoneum or mesentery
(2–5),
and less often in the abdominal wall (6), pleura (7),
pancreas (8), liver (9), adrenal glands (10), bladder (11) and prostate (12). The incidence of EGISTs is low,
accounting of ~5–7% of all GISTs (13). GIST metastasis to the liver is
considered common, whereas primary EGIST of the liver is
considerably rare. According to a study by Li et al
(14), only 6 cases worldwide of
primary hepatic EGIST were reported between 2003 and 2012. The
present study reports a case of primary EGIST located in the
caudate lobe of the liver in a 61-year-old Chinese man.
Case report
A 61-year-old Chinese man was admitted to The First
Hospital of Jilin University (Changchun, China) on February 11,
2014, for the treatment of an abdominal mass detected by abdominal
ultrasonography during a health examination. The abdominal
ultrasound identified a 3×7-cm mass in the caudate lobe of the
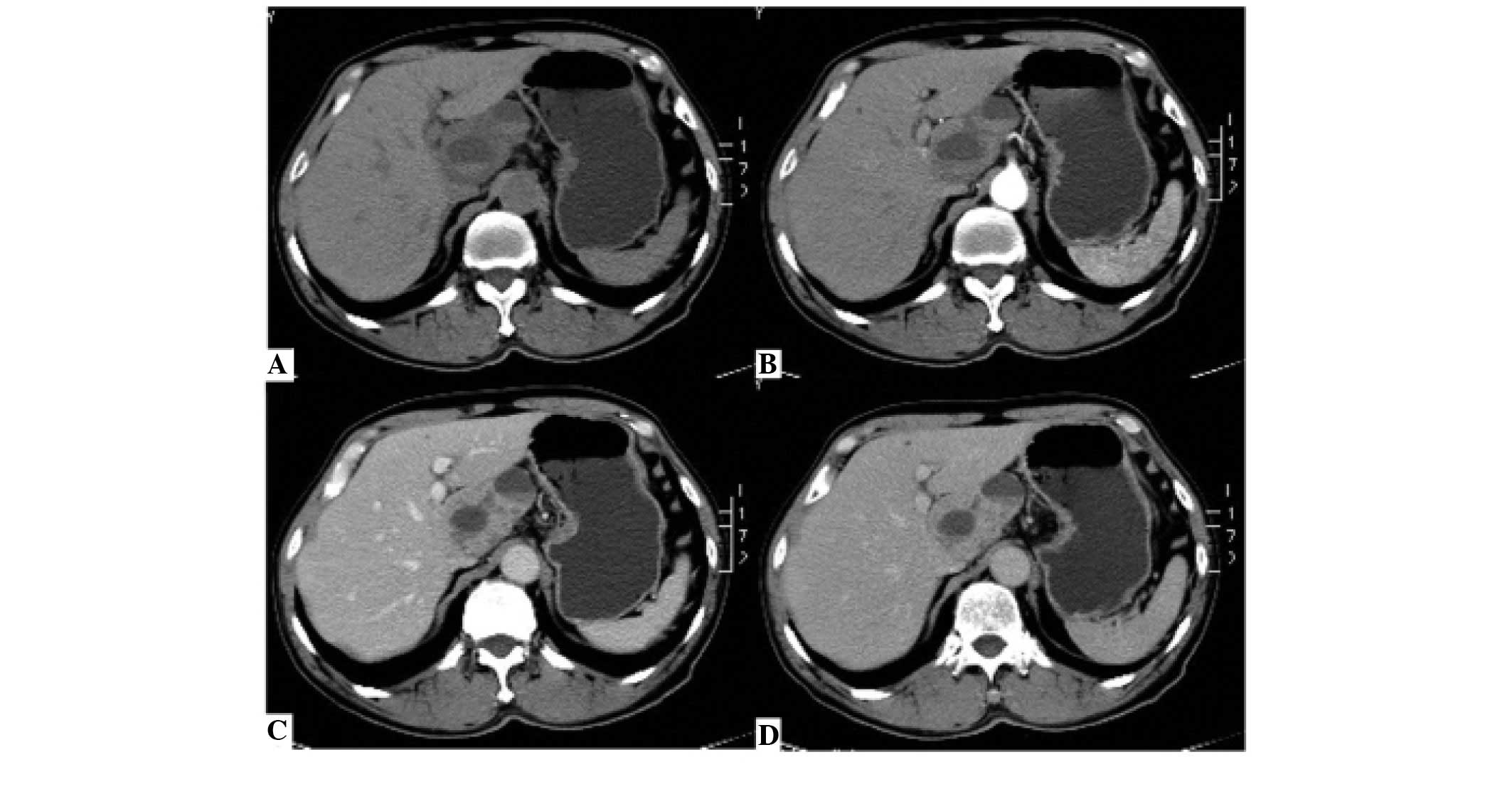
liver. Following admission, a contrast-enhanced computed tomography
(CECT) scan revealed a 7.3×5.1-cm mass with solid and cystic
components in the caudate lobe of the liver. The mass displayed
post-contrast heterogeneous enhancement (Fig. 1), therefore, the mass was considered
to be malignant. The possibility of a neurogenic tumor was also
considered. The findings of physical and laboratory tests for
hepatitis B and C virus, liver function and tumor markers, such as
α-fetoprotein and carcinoembryonic antigen, were all within the
normal limits. Therefore, the patient underwent an exploratory
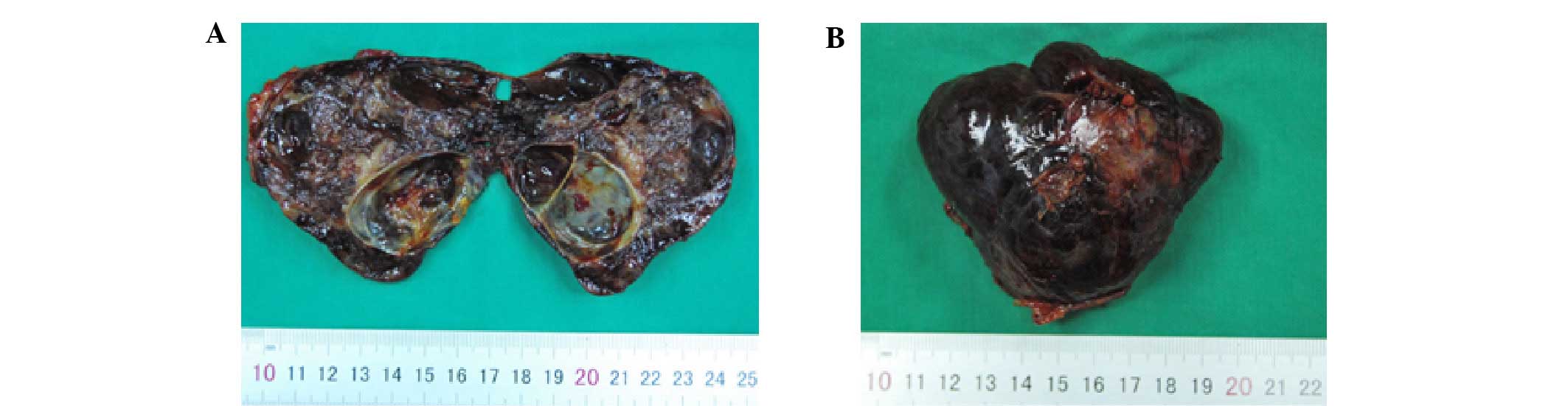
laparotomy on February 17, 2014. Intraoperatively, the mass was
hard with an uneven surface, measured 7×5 cm and was located in the
caudate lobe of the liver (Fig. 2).
No abnormal lesions were identified in the stomach, duodenum, small
intestine, colon, pancreas, peritoneum, omentum or any other organs
in the abdominal cavity. The patient underwent caudate lobe
resection, in particular Spiegel lobe resection. Sectioning of the
resected tumor revealed that inside of the mass was divided by
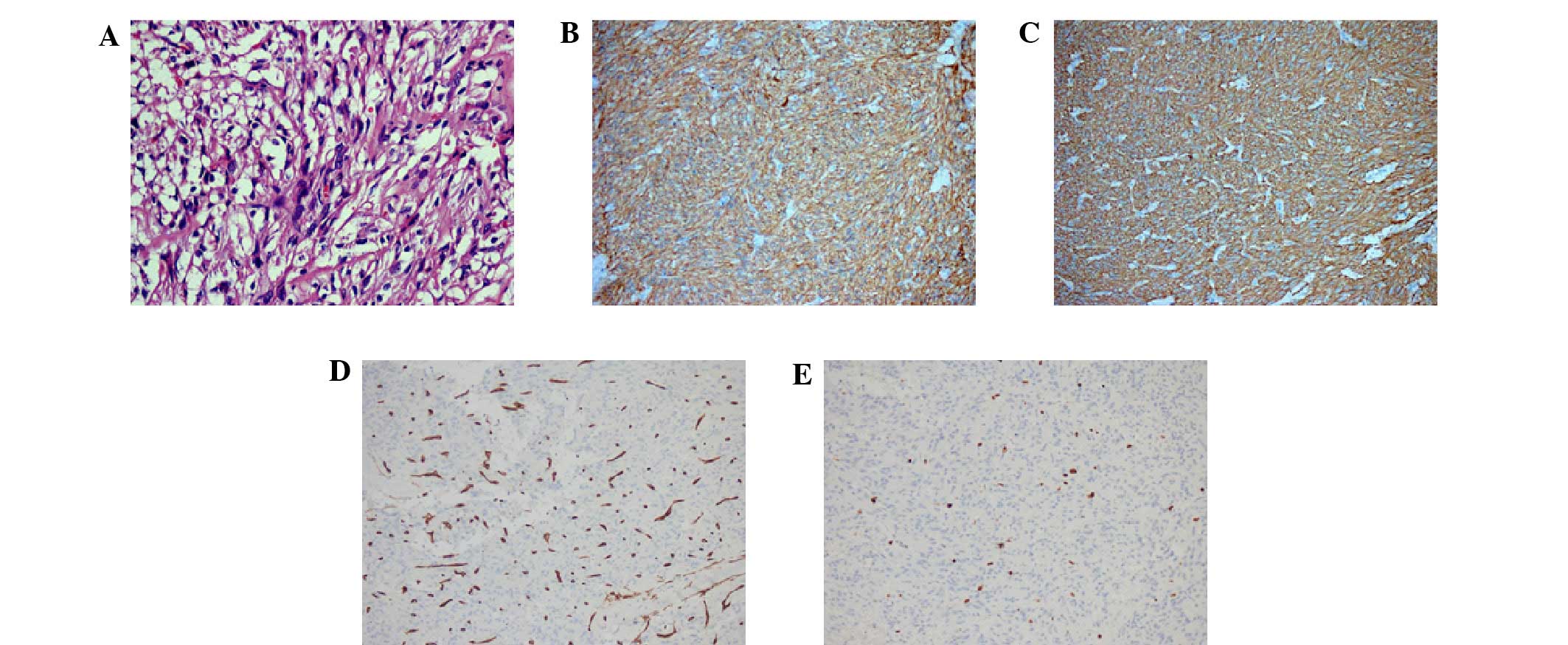
numerous fibers and filled with necrotic tissue (Fig. 2). Immunohistochemistry of the resected
tissue showed a strong positivity for cluster of differentiation
(CD)117, discovered on GIST-1 (DOG1) and CD34. The Ki-67 labeling
index was found to be ~2%. Hematoxylin and eosin staining
demonstrated the tumor was composed of spindle cells (Fig. 3). These histological and
immunohistochemical features led to a final diagnosis of high-grade
primary hepatic EGIST. The present study was approved by the ethics
committee of the first hospital of Jilin University, Changchun,
China.
The patient was discharged from the hospital in the
absence of any clinically significant events, and follow up was at
3-month intervals during the first year and at 6-month intervals
thereafter. Follow-up tests included routine CBC, liver function
test as well as abdominal CT scan. The patient was asymptomatic
without any sign of recurrence during the follow-up period. Lab
tests were in normal range, and no mass was found in CT scan.
Discussion
EGISTs predominantly occur in male adults aged
>50 years (15,16) and the tumor size is typically >5
cm. The phenotypic characteristics of GISTs include elevated
expression of CD117, a receptor tyrosine kinase protein that is
encoded by the c-Kit gene in humans. Generally, EGISTs exhibit a
c-Kit expression similar to that of GISTs. Gain-of-function
mutations in the c-Kit and platelet-derived growth factor
receptor-α (PDGFR-α) genes have been previously reported in GISTs,
and are considered to constitute an important mechanism for their
development (17). Yamamoto et
al (18) identified that the
c-Kit and PDGFR-α mutation pattern in EGISTs was similar to that in
GISTs, indicating the potential role of c-Kit and PDGFR-α mutations
in the tumorigenesis of EGISTs as well.
Several hypotheses have been proposed regarding the
tumorigenesis of EGISTs. A previous study has suggested that GISTs
may originate from interstitial cells of Cajal (ICCs), due to the
striking morphological and immunophenotypic similarities between
GISTs and ICCs (19). From a
molecular genetic perspective, EGISTs comprise a specific type of
GIST, therefore, theoretically, they could be share the same
mesenchymal origin; however, ICCs form a network surrounding the
gastrointestinal plexus, which cannot explain the occurrence of
EGISTs. Agaimy et al (20)
proposed that EGISTs are extremely rare, and that various reported
EGISTs may have actually been GISTs that arose from the outermost
muscle layer of the gastrointestinal tract but were detached from
the original site during their growth. For example, mesenteric and
omental EGISTs may derive from GISTs of the small intestine and
stomach, respectively. An alternative explanation is that EGISTs
originate from multipotent mesenchymal stem cells located outside
of the gastrointestinal tract.
Thus far, no common symptoms specific to EGISTs have
been identified. The majority of cases are initially detected by
the presence of a mass upon physical examination. In the current
case, the patient was found to have a hepatic lesion during a
health examination. CECT further confirmed a 7.3×5.1-cm
heterogeneously enhanced mass with solid and cystic components in
the caudate lobe of the liver. The mass was filled with necrotic
tissue and fed by numerous blood vessels. The lesion exhibited an
uneven enhancement in the arterial phase of scanning, presenting as
a large, well-circumscribed low-density mass with a partial
high-density area. In the venous and delayed phases, enhancement
was progressively strengthened (Fig.
1).
In the majority of cases of EGISTs, preoperative
diagnosis is not possible, therefore, patients may be easily
misdiagnosed with different types of cancer, such as lymphoma,
neurogenic tumors and malignant fibrous histiocytoma. In the
present case, the mass was diagnosed as a malignant lesion of the
liver prior to surgical intervention, however, the nature of the
tumor could not be determined preoperatively. Occasionally,
preoperative ultrasound-guided fine needle aspiration cytology can
assist the diagnosis of EGISTs. The final diagnosis, however, is
generally based on histological, immunohistochemical and molecular
findings. In 95% of EGIST cases, the CD117 protein exhibits a
strong, diffuse positive immunohistochemical reaction, and 60–70%
of EGISTs are CD34-positive (21). In
the present case, immunohistochemical examination of the tumor
tissue revealed strong positivity for CD117, DOG1 and CD34. The
final diagnosis of primary hepatic EGIST was based on the fact that
no abnormal lesions were identified in any other organs in the
abdominal cavity except the liver.
The standard treatment for both GISTs and primary
non-metastatic EGISTs is complete surgical resection with a
microscopic negative margin, which was the case for the patient in
the present report. During the surgical resection of the tumor,
clinicians should be careful not to cause implantation metastasis.
In addition, large tumors should not be removed via laparoscopic
resection (22). Imatinib, a tyrosine
kinase inhibitor of c-Kit, has also been used for the treatment of
GISTs and EGISTs. Imatinib can improve overall recurrence-free
survival, even in patients with advanced GISTs (23,24);
however, certain studies have indicated that adjuvant therapy with
tyrosine kinase inhibitors appears to be unnecessary in cases when
a negative microscopic margin (R0 resection) is achieved (24). EGISTs are commonly accompanied by
certain adverse prognostic factors, such as large primary tumors
and distant or lymph node metastases. As a result, EGISTs have a
worse prognosis than GISTs (7).
In conclusion, primary hepatic EGISTs are extremely
rare. Histological and immunohistochemical features, including
positive staining for CD117 and CD34, can aid in obtaining an
accurate diagnosis. Complete tumor resection with a microscopic
negative margin is considered the optimal treatment option.
Acknowledgements
The authors would like to thank the staff of the
Pathological Department of The First Hospital of Jilin University
(Changchun, China) for their the assistance.
References
|
1
|
Emory TS, Sobin LH, Lukes L, Lee DH and
O'Leary TJ: Prognosis of gastrointestinal smooth-muscle (stromal)
tumors: Dependence on anatomic site. Am J Surg Pathol. 23:82–7.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fukuda H, Suwa T, Kimura F, Sugiura T,
Shinoda T and Kaneko K: Gastrointestinal stromal tumor of the
lesser omentum: Report of a case. Surg Today. 31:715–718. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nakaya I, Iwata Y, Abe T, Yokoyama H, Oda
Y and Nomura G: Malignant gastrointestinal stromal tumor
originating in the lesser omentum, complicated by rapidly
progressive glomerulonephritis and gastric carcinoma. Intern Med.
43:102–105. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Takao H, Yamahira K, Doi I and Watanabe T:
Gastrointestinal stromal tumor of the retroperitoneum: CT and MR
findings. Eur Radiol. 14:1926–1929. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Llenas-Garcia J, Guerra-Vales JM, Moreno
A, Ibarrola C, Castelbon FJ, Fernández-Ruiz M, Meneu JC, Ballestin
C and Moreno E: Primary extragastrointestinal stromal tumors in the
omentum and mesentery: A clinicopathological and
immunohistochemical study. Hepatogastroenterology. 55:1002–1005.
2008.PubMed/NCBI
|
|
6
|
Kumar AS, Padmini R, Veena G and Murugesan
N: Extragastrointestinal stromal tumour of the abdominal wall-a
case report. J Clin Diagn Res. 7:2970–2972. 2013.PubMed/NCBI
|
|
7
|
Yi JH, Sim J, Park BB, Lee YY, Jung WS,
Jang HJ, Ha TK and Paik SS: The primary extra-gastrointestinal
stromal tumor of pleura: A case report and a literature review. Jpn
J Clin Oncol. 43:1269–1272. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yamaura K, Kato K, Miyazawa M, Haba Y, et
al: Stromal tumor of the pancreas with expression of c-kit protein:
Report of a case. J Gastroenterol Hepatol. 19:467–470. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chen J, Du YJ, Song JTELN and Liu BR:
Primary malignant liver mesenchymal tumor: A case report. World J
Gastroenterol. 16:5263–5266. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sereg M, Buzogány I, Gonda G, Sápi Z,
Csöregh E, Jakab Z, Rácz K and Tóth M: Gastrointestinal stromal
tumor presenting as a hormonally inactive adrenal mass. Endocrine.
39:1–5. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mekni A, Chelly I, Azzouz H, Ben Ghorbel
I, Bellil S, Haouet S, Kchir N, Zitouna M and Bellil K:
Extragastrointestinal stromal tumor of the urinary wall bladder:
Case report and review of the literature. Pathologica. 100:173–175.
2008.PubMed/NCBI
|
|
12
|
Zhou J and Teng X: Primary
extragastrointestinal stromal tumor of the prostate: A case report.
Anal Quant Cytopathol Histpathol. 36:55–60. 2014.PubMed/NCBI
|
|
13
|
Emory TS, Sobin LH, Lukes L, Lee DH and
O'Leary TJ: Prognosis of gastrointestinal smooth-muscle (stromal)
tumors: Dependence on anatomic site. Am J Surg Pathol. 23:82–87.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li ZY, Liang QL, Chen GQ, Zhou Y and Liu
QL: Extra-gastrointestinal stromal tumor of the liver diagnosed by
ultrasound-guided fine needle aspiration cytology: A case report
and review of the literature. Arch Med Sci. 8:392–397. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fagkrezos D, Touloumis Z, Giannila M,
Penlidis C, et al: Extra-gastrointestinal stromal tumor of the
omentum: A rare case report and review of the literature. Rare
Tumors. 4:e442012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Goh BK, Chow PK, et al: A
single-institution experience with eight CD117-positive primary
extragastrointestinal stromal tumors: Critical appraisal and a
comparison with their gastrointestinal counterparts. J Gastrointest
Surg. 13:1094–1098. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Isozaki K and Hirota S: Gain-of-Function
mutations of receptor tyrosine kinases in gastrointestinal stromal
tumors. Curr Genomics. 7:469–475. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yamamoto H, Oda Y, Kawaguchi K, Nakamura
N, Takahira T, Tamiya S, Saito T, Oshiro Y, Ohta M, Yao T and
Tsuneyoshi M: c-kit and PDGFRA mutations in extragastrointestinal
stromal tumor (gastrointestinal stromal tumor of the soft tissue).
Am J Surg Pathol. 28:479–488. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kindblom LG, Remotti HE, Aldenborg F and
Meis-Kindblom JM: Gastrointestinal pacemaker cell tumor (GIPACT):
Gastrointestinal stromal tumors show phenotypic characteristics of
the interstitial cells of Cajal. Am J Pathol. 152:1259–1269.
1998.PubMed/NCBI
|
|
20
|
Agaimy A and Wünsch PH: Gastrointestinal
stromal tumours: A regular origin in the muscularis propria, but an
extremely diverse gross presentation. A review of 200 cases to
critically re-evaluate the concept of so-called
extra-gastrointestinal stromal tumours. Langenbecks Arch Surg.
391:322–329. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tian YT, Liu H, Shi SS, Xie YB, Xu Q,
Zhang JW, Zhao DB, Wang CF and Chen YT: Malignant
extra-gastrointestinal stromal tumor of the pancreas: Report of two
cases and review of the literature. World J Gastroenterol.
20:863–868. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Casali PG and Blay JY:
ESMO/CONTICANET/EUROBONET Consensus Panel of Experts:
Gastrointestinal stromal tumours: ESMO clinical practice guidelines
for diagnosis, treatment and follow-up. Ann Oncol. 21(Suppl 5):
v98–v102. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Blanke CD, Demetri GD, von Mehren M,
Heinrich MC, Eisenberg B, Fletcher JA, Corless CL, Fletcher CD,
Roberts PJ, Heinz D, et al: Long-term results from a randomized
phase II trial of standard- versus higher-dose imatinib mesylate
for patients with unresectable or metastatic gastrointestinal
stromal tumors expressing KIT. J Clin Oncol. 26:620–625. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li J, Gong JF, Wu AW and Shen L:
Post-operative imatinib in patients with intermediate or high risk
gastrointestinal stromal tumor. Eur J Surg Oncol. 37:319–324. 2011.
View Article : Google Scholar : PubMed/NCBI
|