Introduction
Common sites for synchronous metastases from
colorectal cancer include the liver, lung, peritoneum, bone and
brain (1). The frequency of ovarian
metastasis from colorectal cancer is 1.6–6.4%, however, this type
of metastasis is difficult to distinguish from primary ovarian
neoplasms (2–5). Furthermore, synchronous ovarian
metastasis from colorectal cancer is generally poor, and the
optimal first-line treatment strategy is debatable (6,7). The
present study reports two cases of synchronous ovarian metastasis
from colorectal cancer that were managed by cytoreductive
surgery.
Case report
Case one
A 60-year-old female patient presented to Katsuta
Hospital (Katsuta, Japan) in June 2014 with progressive abdominal
distension and lower abdominal pain. The following day the patient
was referred to Ibaraki Medical Center, Tokyo Medical University
(Ami, Japan) with a suspected diagnosis of pelvic tumor. The
patient's medical history was otherwise unremarkable. Physical
examination revealed lower abdominal tenderness with a palpable
mass. Laboratory data revealed slight hypoalbuminemia (albumin, 3.5
g/dl; normal range, >4.0 g/dl), and carcinoembryonic antigen
(CEA; 11.1 ng/ml; normal range, <5.0 ng/ml) and carbohydrate
antigen (CA) 125 (743.7 U/ml; normal range, <37.0 U/ml) levels
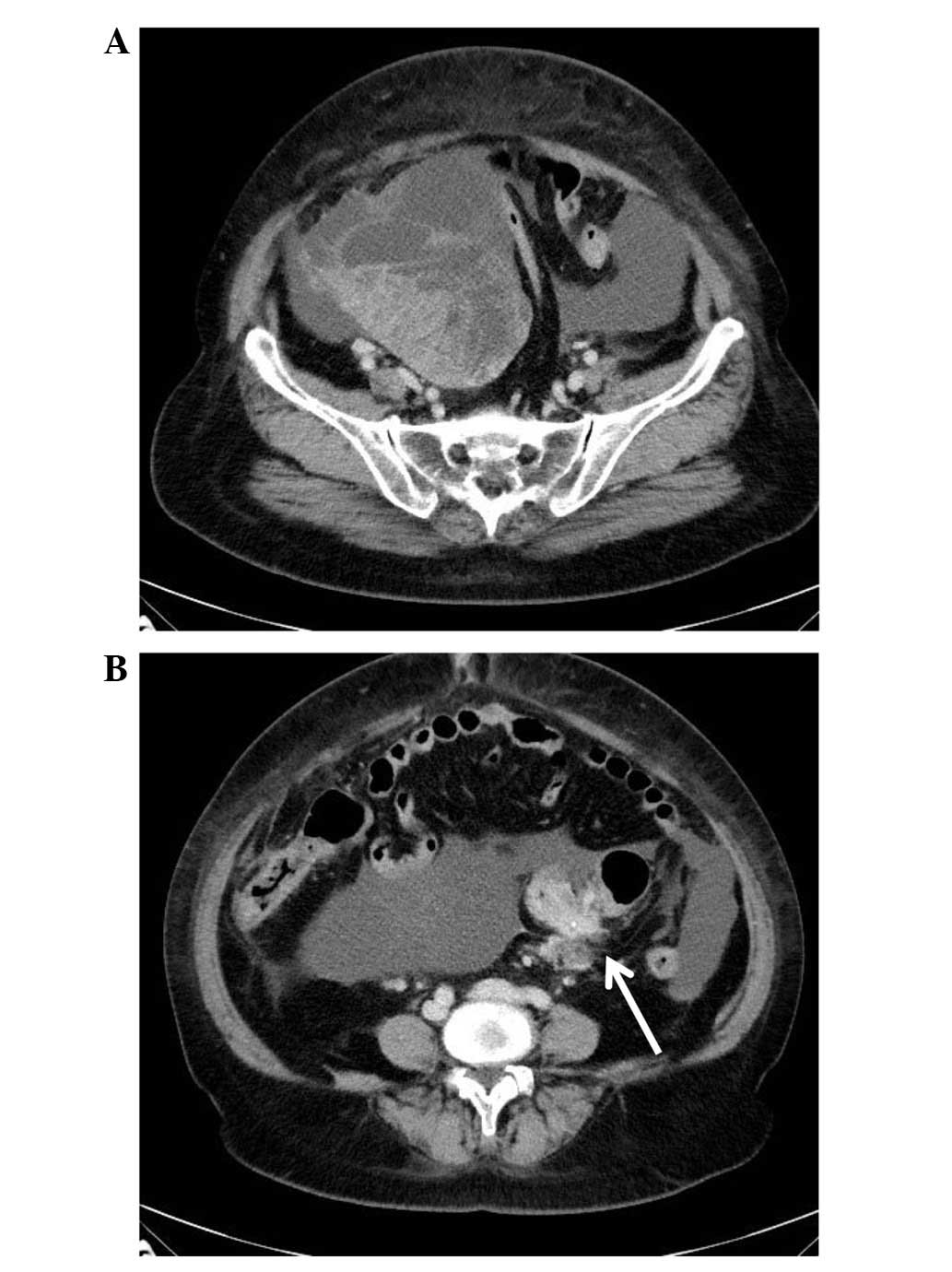
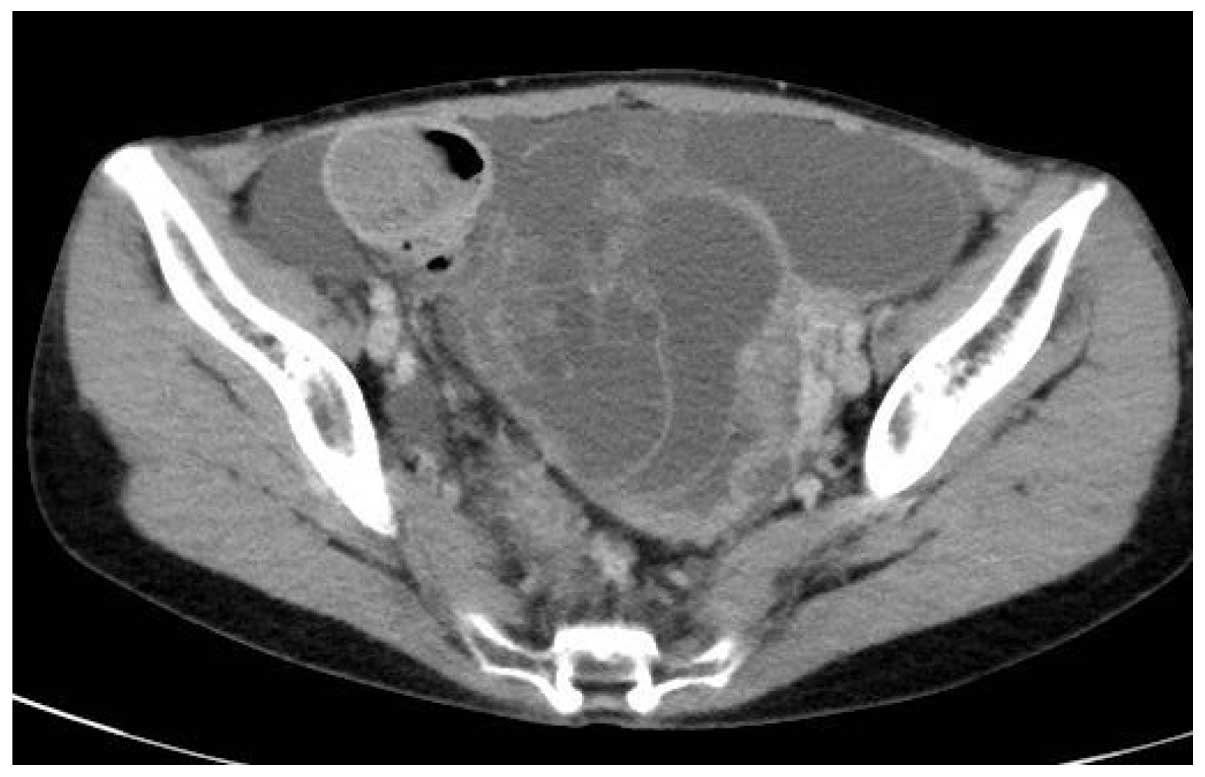
were increased. Abdominal computed tomography (CT; Somatom
Sensation Cardiac; Siemens, AG, Munich, Germany) revealed a
multilocular cystic pelvic mass with a solid component measuring 17
cm in diameter and an irregular mass located in the sigmoid colon
(Fig. 1). Extensive ascites were also
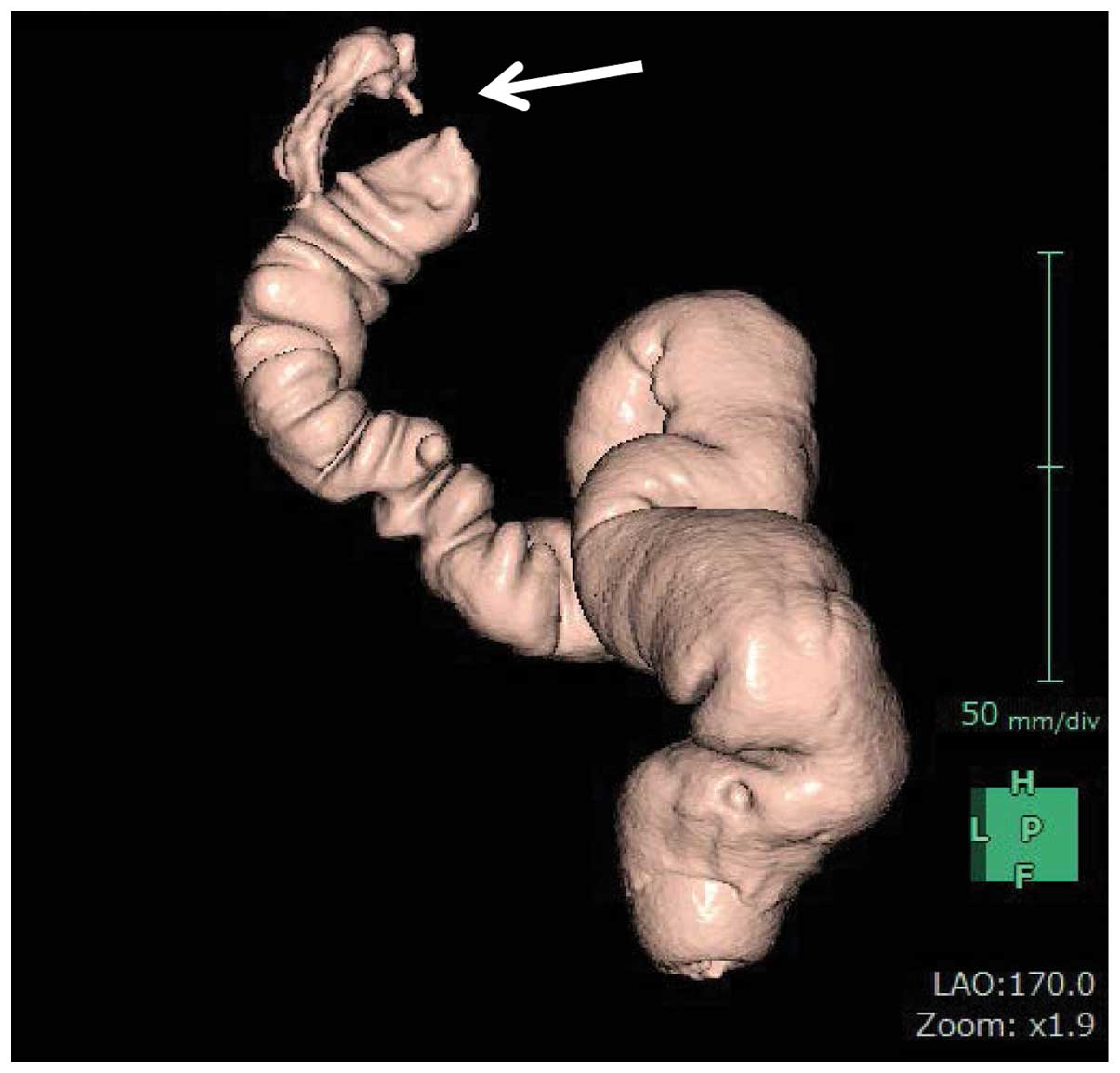
present. Virtual colonoscopy (Synapse VINCENT; Fujifilm Corporatio,
Tokyo, Japan) revealed stenosis with a mass in the sigmoid colon
(Fig. 2), which was confirmed by
traditional colonoscopy. However, no tumor cells were identified in
the biopsy specimen (which was obtained during colonoscopy) on
hematoxylin and eosin histological examination. Ovarian metastasis
from sigmoid colon cancer was suspected, therefore, adnexectomy was
performed in July 2014. Intraoperatively, a disseminated tumor in
the pelvic cavity was identified and cytology of the ascites using
Papanicolaou staining revealed clusters of atypical cells
exhibiting anisokaryosis, hyperchromasia and enlarged nuclei,
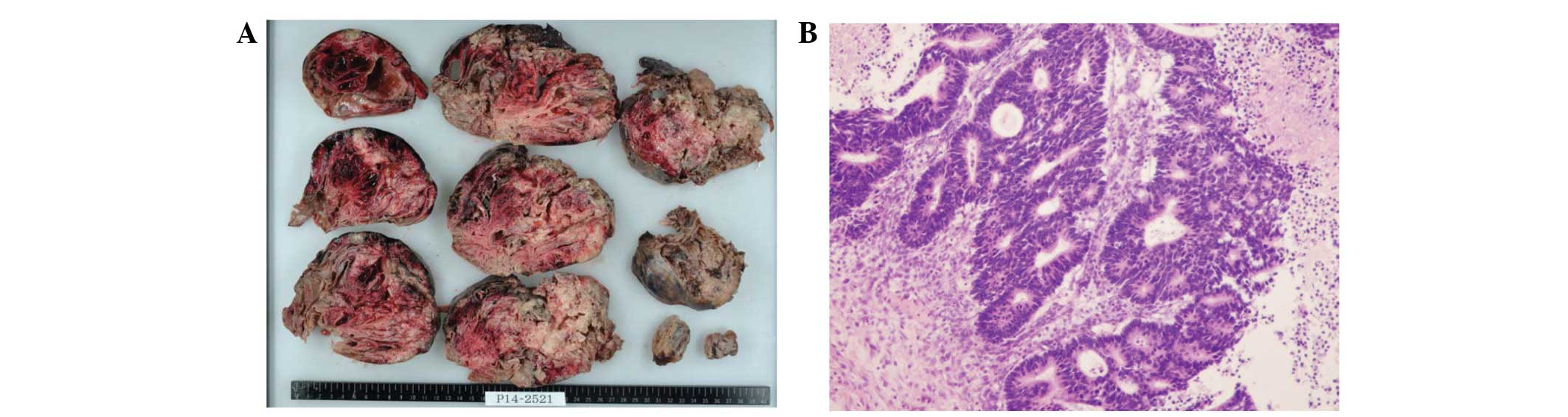
yielding a diagnosis of adenocarcinoma. The resected tumor measured
17×14×8 cm, and macroscopic examination revealed multicystic walls
and septa composed of solid and necrotic components (Fig. 3A). Hematoxylin and eosin histological
examination of the formalin-fixed and paraffin-embedded excised
tumor revealed moderately-differentiated adenocarcinoma forming in
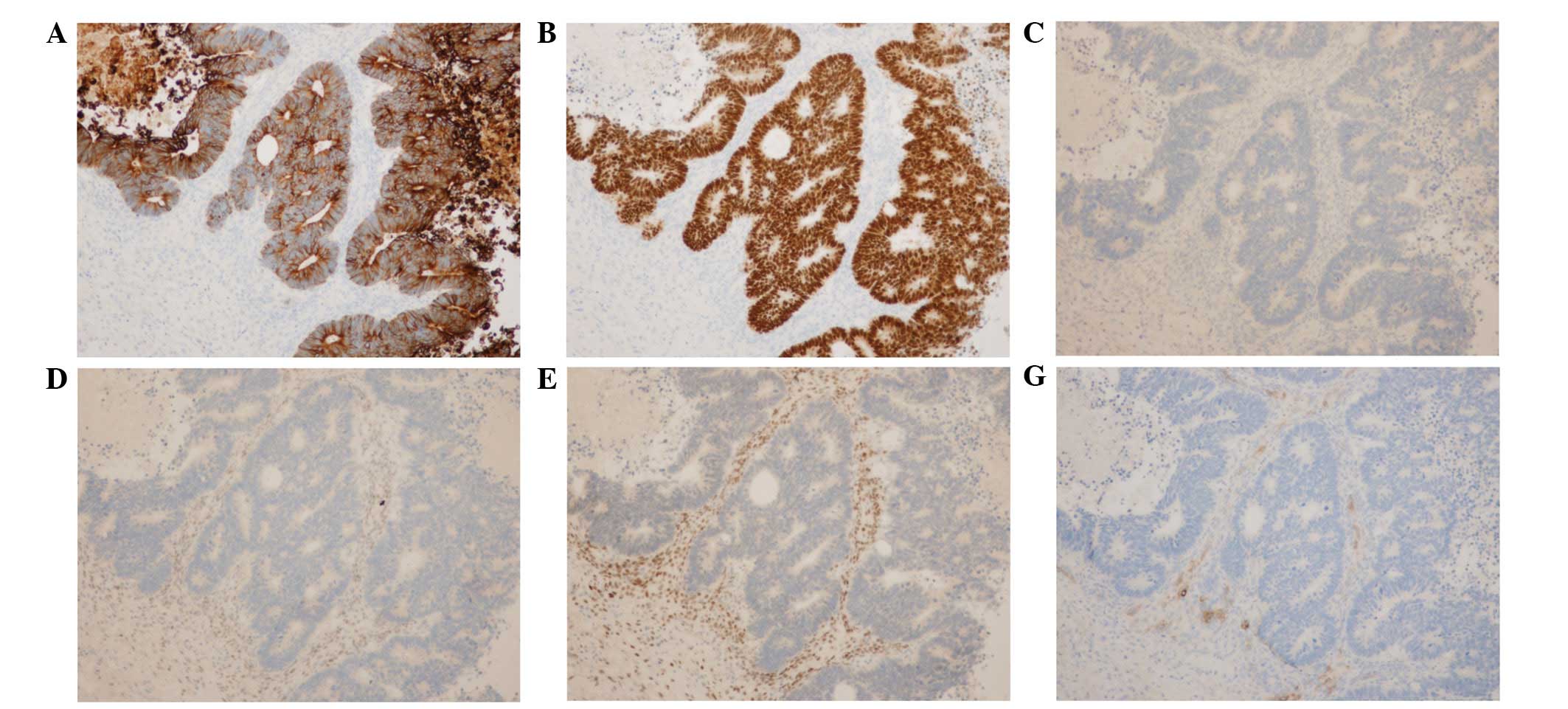
the septa with infiltration of the cystic wall (Fig. 3B). Immunohistochemical analysis of the
tumor revealed positive staining for cytokeratin (CK)20 (mouse
monoclonal; dilution 1:50; M7019; Dako, Glostrup Denmark) and
caudal-type homeobox 2 (CDX2; rabbit monoclonal; dilution 1:1;
418011; Nichirei Biosciences, Inc., Tokyo, Japan), and negative
staining for CK7 (mouse monoclonal; dilution 1:100; M7018; Dako),
estrogen receptor (rabbit monoclonal; dilution 1:1; 107925; Roche
Diagnostics, Basel, Switzerland), progesterone receptor (rabbit
monoclonal; dilution 1:1; 109431; Roche Diagnostics) and inhibin
(mouse monoclonal; dilution 1:50; M3609; Dako) (Fig. 4). These immunohistological results
supported the diagnosis of ovarian metastasis originating from
colon cancer of the sigmoid. Recovery was uneventful and the
patient was discharged 12 days after surgery. From October 2014,
the patient was administered modified FOLFOX6 [oxaliplatin (85
mg/m2), leucovorin (400 mg/m2) and
fluorouracil (5-FU; 400 mg/m2) intravenous infusion on
day 1, followed by 2,400 mg/m2 intravenous infusion of
5-FU over 46 h every 2 weeks] plus anti-vascular endothelial growth
factor monoclonal antibody (bevacizumab; 5 mg/kg every 2 weeks) for
primary sigmoid colon cancer with peritoneal dissemination. At
present, the patient is regularly followed up every 2 weeks at the
outpatient clinic of Ibaraki Medical Center, Tokyo Medical
University, and her condition remains stable at the time of writing
the present manuscript, in April 2016.
Case two
A 56-year-old female patient presented to Ryugasaki
Saiseikai Hospital (Ryugasaki, Japan) in September 2014 with
progressive abdominal distension. The following day the patient was
referred to Ibaraki Medical Center, Tokyo Medical University, with
a suspected ovarian tumor. The patient's medical history was
otherwise unremarkable. Physical examination revealed abdominal
distention with fluctuation, indicating abundant ascites.
Laboratory data revealed increased lactate dehydrogenase (2,473
IU/l, normal range, 120–240 IU/l), CEA (93.9 ng/ml) and CA 125
(274.4 U/ml) levels. Abdominal CT (Somatom Sensation Cardiac)
revealed a multilocular cystic pelvic mass with a solid component,
measuring 12 cm in diameter, and ascites (Fig. 5). Cytology of abdominocentesis fluid
using Papanicolau staining revealed clusters of atypical cells
exhibiting anisokaryosis, hyperchromasia and enlarged nuclei, thus
confirming adenocarcinoma, while colonoscopy revealed an elevated
tumor with a central depression in the rectum, which did not
involve the tumor. Biopsy of the tumor specimen indicated
moderately-differentiated adenocarcinoma. A diagnosis of ovarian
metastasis from rectal carcinoma with peritoneal dissemination was
established; therefore, left ovariectomy and transverse colostomy
were performed in November 2014. The resected tumor measured
12×11×8 cm, and macroscopic examination revealed multicystic walls
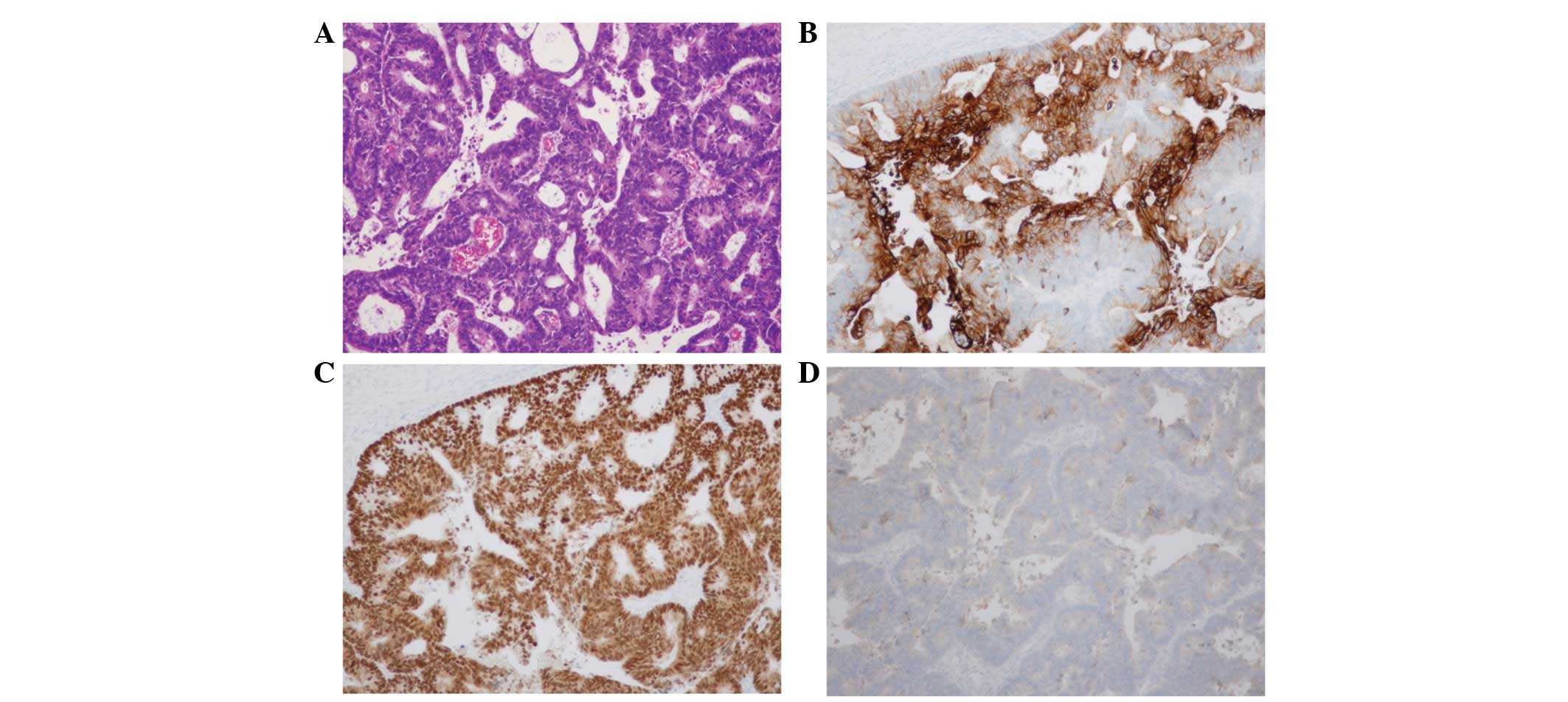
and septa composed of a solid component with hemorrhage (Fig. 6). Hematoxylin and eosin histological
examination of the formalin-fixed and paraffin-embedded excised
tumor revealed moderately-differentiated adenocarcinoma (Fig. 7A), and immunohistochemical analysis
identified positive staining for CK20 and CDX2, and negative
staining for CK7 (Fig. 7B–D). These
immunohistological results confirmed the diagnosis of ovarian
metastasis from rectal cancer. Recovery was uneventful and the
patient was discharged 13 days postoperatively. From December 2014,
the patient was administered modified FOLFOX plus bevacizumab for
primary rectal cancer with peritoneal dissemination. At present,
the patient is undergoing regular follow-up examinations every 2
weeks at the outpatient clinic of Ibaraki Medical Center, Tokyo
Medical University, and her condition was stable at the time of
writing.
Discussion
Metastatic ovarian tumors account for ~21.5% of all
malignant ovarian tumors and 3.7–7.4% of the cases metastasize from
colorectal cancer (8–10). However, the process by which
colorectal cancer metastasizes to the ovary remains unclear.
Graffner et al (9) and
Birnkrant et al (11) have
postulated that, as there is no lymph flow between the colon and
the ovaries, both hematogenous and disseminated peritoneal
metastasis present possible metastatic pathways. In the two present
cases, peritoneal dissemination was confirmed intraoperatively.
Clinically, it is difficult to distinguish between primary and
metastatic cancer of the ovary, which results in diagnostic
problems for clinicians, radiologists and pathologists. Regarding
radiological examination, Cho and Gold (12) reported that a mixed cystic and solid
ovarian mass observed by CT scan must be regarded as a metastatic
tumor in patients with a history of colonic or gastric carcinoma.
In the present cases, the ovarian tumor presented as a multilocular
cystic pelvic mass with a solid component. In addition, the patient
in case two was preoperatively diagnosed with advanced rectal
carcinoma with peritoneal dissemination. Regarding histological
examination, Lee and Young (2)
reported that bilaterality, microscopic surface involvement of
epithelial cells and an infiltrative pattern of stromal invasion
were strong indicators of metastatic ovarian carcinoma. In case
one, histological examination of the sigmoid colon tumor did not
reveal carcinoma cells, although virtual colonoscopy identified
stenosis with a mass. However, resection of the ovarian tumor
revealed moderately-differentiated adenocarcinoma, and
immunohistochemical analysis of the tumor cells revealed positive
staining for CK20 and CDX2, and negative staining for CK7, estrogen
receptor, progesterone receptor and inhibin. In the majority of
cases, primary ovarian neoplasms exhibit positive staining for CK7
and negative staining for CK20. By contrast, colorectal carcinomas
most frequently exhibit negative staining for CK7 and positive
staining for CK20 (13,14). CDX2 is a homeobox gene encoding
the CDX2 protein, which serves as a transcription factor that is
expressed in the nuclei of intestinal epithelial cells (15). CDX2 is a useful marker for
adenocarcinoma of the gastrointestinal tract, and for
distinguishing between primary and metastatic carcinomas of the
ovary (16–18). According to immunohistological
examination, the results of case one support the diagnosis of
metastatic ovarian carcinoma from sigmoid colon carcinoma.
The optimal first-line treatment strategy for
synchronous ovarian metastasis from colorectal cancer remains
controversial. The Japanese guidelines for colorectal cancer
treatment recommend surgery for metastatic lesions if the primary
colorectal and metastatic lesions are completely resectable, and if
the patient is able to tolerate resection of the metastatic lesions
(1). In the present two cases, tumor
dissemination was intraoperatively detected in the pelvic cavity,
however, complete resection was not possible for all lesions. Only
excision of ovarian metastases was performed for the following
reasons: i) Patients presented with progressive abdominal
distension and excision of ovarian metastasis may have alleviated
the symptoms (19); ii) it is
difficult to distinguish between primary and metastatic cancer of
the ovary by diagnostic imaging alone, thus, a definitive
histological diagnosis was required to identify appropriate
treatment, particularly in case one (preoperative histological
examination of the sigmoid colon tumor did not lead to a
diagnosis); and iii) cytoreductive surgery is associated with
improvement of overall survival in patients with widespread
metastases of colorectal cancer (20). A number of cases of synchronous
ovarian metastasis from colorectal cancer also exhibit distant
metastasis and/or peritoneal dissemination (6,7),
therefore, the prognosis is generally poor. Jiang et al
(21) reported that the median
survival in patients with residual disease after metastasectomy is
10 months. However, as a result of marked improvement in systemic
chemotherapy treatment for advanced colorectal cancer, it has been
estimated that the median survival time of the patients may improve
to >20 months following the administration of FOLFOX or 5-FU,
leucovorin and irinotecan combination chemotherapy plus bevacizumab
or anti-epidermal growth factor receptor monoclonal antibody
(22–25).
In conclusion, ovarian metastases from primary
colorectal cancer may present as pelvic tumors, thus, preoperative
examination of the gastrointestinal tract and excision of the
ovarian tumor are required to establish a histological diagnosis
for the selection of appropriate treatment strategies.
Acknowledgements
The authors would like to thank Enago (www.enago.jp) for reviewing the English language of
the present study.
References
|
1
|
Watanabe T, Itabashi M, Shimada Y, Tanaka
S, Ito Y, Ajioka Y, Hamaguchi T, Hyodo I, Igarashi M, Ishida H, et
al: Japanese Society for Cancer of the Colon and Rectum: Japanese
Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010
for the treatment of colorectal cancer. Int J Clin Oncol. 17:1–29.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lee KR and Young RH: The distinction
between primary and metastatic mucinous carcinomas of the ovary:
Gross and histologic findings in 50 cases. Am J Surg Pathol.
27:281–292. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shiono S, Saito T, Fujii H, Arakawa A,
Nakamura T and Yao T: A case of Krukenberg carcinoma metastasized
from colon cancer resembling mucinous cystadenocarcinoma of the
ovary. Int J Clin Exp Pathol. 7:394–401. 2013.PubMed/NCBI
|
|
4
|
Aiyer R, Sweetman K, Larsen-Disney P and
Fish A: A colorectal carcinoma imitating a primary ovarian
carcinoma in a postpartum woman. BMJ Case Rep. 2013:pii:
bcr2013201055. 2013.PubMed/NCBI
|
|
5
|
Hata T, Yoshioka S, Asukai K, Mizumoto S,
Nakanishi M, Hamano R, Maekawa T, Hama N, Kashiwazaki M, Taniguchi
M, et al: Two cases of ovarian metastasis of colon cancer. Gan To
Kagaku Ryoho. 38:2286–2288. 2011.(In Japanese). PubMed/NCBI
|
|
6
|
Chung TS, Chang HJ, Jung KH, Park SY, Lim
SB, Choi HS and Jeong SY: Role of surgery in the treatment of
ovarian metastases from colorectal cancer. J Surg Oncol.
100:570–574. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rayson D, Bouttell E, Whiston F and Stitt
L: Outcome after ovarian/adnexal metastectomy in metastatic
colorectal carcinoma. J Surg Oncol. 75:186–192. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ayhan A, Tuncer ZS and Bükülmez O:
Malignant tumors metastatic to the ovaries. J Surg Oncol.
60:268–276. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Graffner HO, Alm PO and Oscarson JE:
Prophylactic oophorectomy in colorectal carcinoma. Am J Surg.
146:233–235. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
MacKeigan JM and Ferguson JA: Prophylactic
oophorectomy and colorectal cancer in premenopausal patients. Dis
Colon Rectum. 22:401–405. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Birnkrant A, Sampson J and Sugarbaker PH:
Ovarian metastasis from colorectal cancer. Dis Colon Rectum.
29:767–771. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cho KC and Gold BM: Computed tomography of
Krukenberg tumors. AJR Am J Roentgenol. 145:285–288. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wauters CC, Smedts F, Gerrits LG, Bosman
FT and Ramaekers FC: Keratins 7 and 20 as diagnostic markers of
carcinomas metastatic to the ovary. Hum Pathol. 26:852–855. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Berezowski K, Stastny JF and Kornstein MJ:
Cytokeratins 7 and 20 and carcinoembryonic antigen in ovarian and
colonic carcinoma. Mod Pathol. 9:426–429. 1996.PubMed/NCBI
|
|
15
|
German MS, Wang J, Fernald AA, Espinosa R
III, Le Beau MM and Bell GI: Localization of the genes encoding two
transcription factors, LMX1 and CDX3, regulating insulin gene
expression to human chromosomes 1 and 13. Genomics. 24:403–404.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mutoh H, Sakurai S, Satoh K, Tamada K,
Kita H, Osawa H, Tomiyama T, Sato Y, Yamamoto H, Isoda N, et al:
Development of gastric carcinoma from intestinal metaplasia in
Cdx2-trasgenic mice. Cancer Res. 64:7740–7747. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li MK and Folpe AL: CDX-2, a new marker
for adenocarcinoma of gastrointestinal origin. Adv Anat Pathol.
11:101–105. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Guo RJ, Suh ER and Lynch JP: The role of
Cdx proteins in intestinal development and cancer. Cancer Biol
Ther. 3:593–601. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kato R, Murata K, Okamura S, Wada Y,
Makino S, Nishigaki T, Owada Y, Murakami M, Okada K, Ebisui C, et
al: Resection of ovarian metastasis of colon cancer to improve
quality of life. Gan To Kagaku Ryoho. 39:2278–2279. 2012.(In
Japanese). PubMed/NCBI
|
|
20
|
McCormick CC, Giuntoli RL II, Gardner GJ,
Schulick RD, Judson K, Ronnett BM, Vang R and Bristow RE: The role
of cytoreductive surgery for colon cancer metastatic to the ovary.
Gynecol Oncol. 105:791–795. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jiang R, Tang J, Cheng X and Zang RY:
Surgical treatment for patients with different origins of
Krukenberg tumors: Outcomes and prognostic factors. Eur J Surg
Oncol. 35:92–97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Saltz LB, Clarke S, Díaz-Rubio E,
Scheithauer W, Figer A, Wong R, Koski S, Lichinitser M, Yang TS,
Rivera F, et al: Bevacizumab in combination with oxaliplatin-based
chemotherapy as first-line therapy in metastatic colorectal cancer:
A randomized phase III study. J Clin Oncol. 26:2013–2019. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fuchs CS, Marshall J and Barrueco J:
Randomized, controlled trial of irinotecan plus infusional, bolus,
or oral fluoropyrimidines in first-line treatment of metastatic
colorectal cancer: Updated results from the BICC-C study. J Clin
Oncol. 26:689–690. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Douillard JY, Siena S, Cassidy J,
Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham
D, Jassem J, et al: Randomized, phase III trial of panitumumab with
infusional fluorouracil, leucovorin and oxaliplatin (FOLFOX4)
versus FOLFOX4 alone as first-line treatment in patients with
previously untreated metastatic colorectal cancer: The PRIME study.
J Clin Oncol. 28:4697–4705. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Köhne CH, Hofheinz R, Mineur L, Letocha H,
Greil R, Thaler J, Fernebro E, Gamelin E, Decosta L and Karthaus M:
First-line panitumumab plus irinotecan/5-fluorouracil/leucovorin
treatment in patients with metastatic colorectal cancer. J Cancer
Res Clin Oncol. 138:65–72. 2012. View Article : Google Scholar : PubMed/NCBI
|