Introduction
Bladder cancer, the most common malignancy of the
urinary tract, poses a threat to an increasing number of humans
(1). Progression of bladder tumors
greatly increases the risk of metastasis and subsequent mortality.
Consequently, early detection is crucial for improving patient
prognosis and long-term survival.
Currently, cystoscopy is considered the gold
standard for the detection of primary tumors and also the follow-up
of patients after transurethral resection of bladder tumors,
despite being an invasive approach (2). Urine cytology, another widely used
detection method, has been firmly established as a useful adjunct,
not only in the diagnosis, but also the follow-up of patients with
bladder cancer (3). However, it is
highly grade-dependent, and in low-grade cancers, it seems to not
be sensitive enough. In addition, urine cytology also suffers from
a high inter- and intra-observer variability, which limits its
validity in screening for bladder tumors (4,5).
With the aim of improving the lower sensitivity of
cytology and increasing the detection of low-grade tumors, the
uCyt+/ImmunoCyt test was developed by Fradet and Lockhard, it uses
three monoclonal antibodies to detect urothelial cells in voided
urine (6). A number of previous
studies demonstrated its high sensitivity, and some investigators
suggested that it also plays an important role in predicting
urothelial tumor recurrence (7–11). The
uCyt+/ImmunoCyt test has been in limited clinical and research use
for a decade, but its diagnostic accuracy has never been subjected
to a quantitative review. We therefore performed a systematic
review and meta-analysis of uCyt+/ImmunoCyt test to fully assess
its diagnostic accuracy in detecting bladder cancers and to guide
future implementation.
Materials and methods
Search methodology
We searched Medline and PubMed for articles that
reported on the diagnostic sensitivity and specificity of the
uCyt+/ImmunoCyt test for bladder cancers. The keywords used for the
search were: (uCyt+/ImmunoCyt OR ImmunoCyt), (bladder cancer or
urothelial tumor), sensitivity, specificity, and cytology. Only
data from original published papers were collected, with meeting or
conference abstracts being excluded. Primary sources from tracking
references were also obtained from manual searches in review papers
and original articles. Electronic databases were retrieved by two
independent investigators. If the assessments of the investigators
were not consistent, a discussion ensued whether to include the
data or not. The articles included contained studies of the
patients with bladder cancer diagnosed using the uCyt+/ImmunoCyt
and cytology tests. The effect sizes of the studies seen as odds
ratio (OR), sample size, gender, or range of age did not exclude
any articles. Studies that only described the uCyt+/ImmunoCyt test
or cytology data were excluded.
Data extraction
Test performance data were extracted as a 2×2 table
of true-positive (TP), false-positive (FP), false-negative (FN) and
true-negative (TN) values directly from tabulated results (Table I). If these were not directly
available, they were calculated from reported sensitivity,
specificity, positive predictive value (PPV) and/or negative PV
(NPV).
 | Table I.Characteristics of studies included in
the meta-analysis (n=7). |
Table I.
Characteristics of studies included in
the meta-analysis (n=7).
|
|
|
|
| uCyt+/ ImmunoCyt | Cytology | Combination of
both |
|---|
|
|
|
|
|
|
|
|
|---|
| Author (refs.) | Year | Sample size | STARD score | TP | FP | FN | TN | TP | FP | FN | TN | TP | FP | FN | TN |
|---|
| Yafi et al
(18) | 2014 | 109 | 18 | 52 |
5 | 31 | 21 | 36 |
4 | 47 | 22 | 54 |
6 | 29 | 20 |
| Soyuer et al
(19) | 2009 | 90 | 15 | 45 |
5 |
9 | 31 | 41 | 12 | 13 | 24 | 48 |
5 |
6 | 31 |
| Horstmann et
al (20) | 2009 | 221 | 16 | 82 | 30 | 31 | 78 | 95 | 41 | 18 | 67 | 105 | 47 |
8 | 61 |
| Têtu et al
(7) | 2005 | 870 | 19 | 100 | 281 | 36 | 453 | 39 | 17 | 97 | 717 | 114 | 284 | 22 | 450 |
| Toma et al
(21) | 2004 | 120 | 15 | 33 | 20 |
9 | 58 | 36 | 16 |
6 | 62 | 37 | 21 |
5 | 57 |
| Hautmann et
al (22) | 2004 | 94 | 14 | 19 | 16 | 11 | 48 | 22 | 13 |
8 | 51 | 25 |
9 |
5 | 55 |
| Sullivan et
al (11) | 2009 | 98 | 18 | 20 | 26 |
6 | 46 |
5 |
2 | 21 | 70 | 20 | 26 |
6 | 46 |
Data analysis
The estimates of sensitivity, specificity,
likelihood ratios (LRs), diagnostic odds ratio (DOR), and their 95%
confidence intervals (95% CIs) were pooled for each study. The
within- and between-study variation or heterogeneity were assessed
by testing Cochrans Q-statistic. Heterogeneity was calculated using
the formula I2 = 100% × (Q - df)/Q (12). A significant Q-statistic (P<0.10)
or I2-statistic (I2>50) indicated
heterogeneity across studies, and then the random effect model
(REM) was used; otherwise, the fixed effect model (FEM) was used.
The pooled estimate of ORs was obtained using the Mantel and
Haenszel method for FEM, the DerSimonian and Laird and DerSimonian
and Kacker method for REM (13–15).
The summary receiver operator characteristic (sROC)
curve was used to graphically determine performance following
testing for correlation between sensitivity and specificity [as the
logit TP rate (TPR) vs. the logit FP rate (FPR)] (16).
The area under the curve (AUC) and an index Q were
discussed as potentially useful summaries of the curve. An upper
bound was derived for the AUC based on an exact analytic expression
for the homogeneous situation, and a lower bound based on the limit
case Q, defined by the point where sensitivity equals specificity:
Q is invariant to heterogeneity (17).
Analyses were performed using the freeware Meta-Disc
version 1.4 (Universidad Complutense, Madrid, Spain) and STATA
package version 13.0 (Stata Corporation, College Station, TX, USA).
All P-values were two-sided. P<0.05 was considered to indicate a
statistically significant difference.
Results
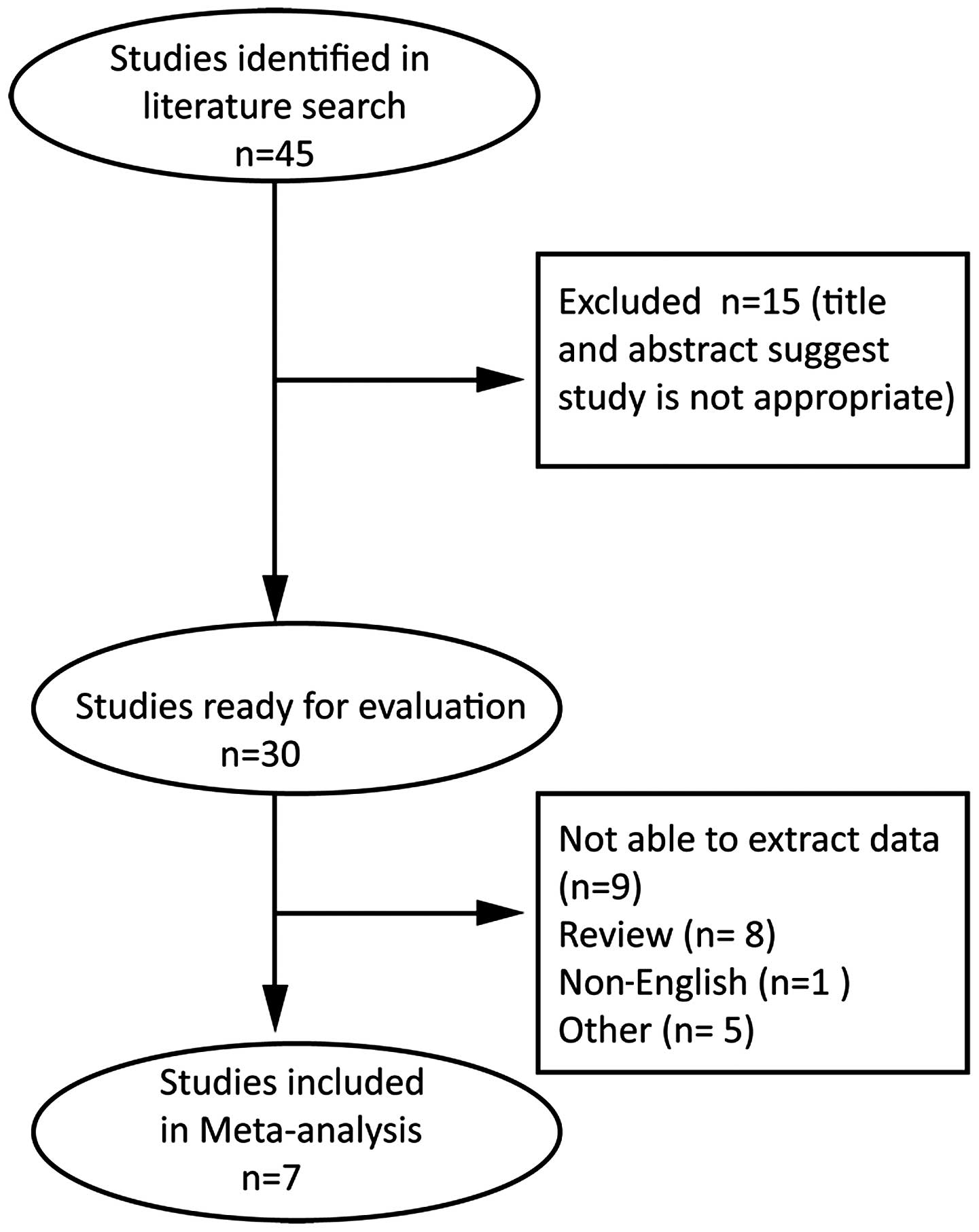
In total, 45 potentially relevant studies were
identified (Fig. 1). During the
abstract screening, 15 articles were excluded. Thirty studies were
considered for full publication review. Of these, 23 were excluded
(nine because there were no data available, eight because they were
reviews, one because it was a non-English article, five because
they only included cytology or ImmunoCyt data and no comparison).
Seven studies were eventually analyzed (Table I) (7,11,18–22). These
studies were published between 2004 and 2014, and included a total
of 1,602 patients with bladder cancer. Their sample size ranged
from 90 to 870. In these seven studies, a combination of cystoscopy
and biopsy was used as the gold standard of bladder cancer.
Assessment of study quality
Studies meeting the criteria were quality assessed
using positive scoring in a modified 23-point Standards for the
Reporting of Diagnostic Accuracy Studies (STARD) proforma (23,24). Two
readers (F.T. and M.M.) independently assessed the included studies
according to the prearranged proforma. An open discussion was
subsequently held in order to resolve any disagreement between the
readers. STARD scores for each study are provided in Table I.
Pooled sensitivity, specificity, LR+,
LR-, and DOR
We summarized the overall meta-analysis of bladder
cancer patients with the ImmunoCyt test, cytology test, and
combined method (Combination of ImmunoCyt and Cytology) (Table II). The REM or FEM was used to
combine the data of TP, FP, FN, and TN numbers.
| Table II.The indices of bladder cancer
diagnosed by ImmunoCyt test and cytology test. |
Table II.
The indices of bladder cancer
diagnosed by ImmunoCyt test and cytology test.
|
|
| Test of
association | Test of
heterogeneity |
| Egger's test for
publication bias |
|---|
|
|
|
|
|
|
|
|---|
| Diagnostic
methods | Parameter | Estimates | 95% CI | Q | P-value | I2
(%) | Model | t | P-value |
|---|
|
uCyt+/ImmunoCyt | Sensitivity | 0.725 | 0.683–0.765 | 9.66 | 0.140 | 37.9 | FEM | 2.56 | 0.051 |
|
| Specificity | 0.657 | 0.629–0.685 | 23.23 | 0.001 | 74.2 | REM |
|
|
|
| Positive LR | 2.578 | 2.003–3.318 | 17.56 | 0.007 | 65.8 | REM |
|
|
|
| Negative LR | 0.385 | 0.327–0.452 | 8.43 | 0.208 | 28.9 | FEM |
|
|
|
| DOR | 7.114 | 4.709–10.748 | 11.24 | 0.081 | 46.6 | REM |
|
|
| Cytology | Sensitivity | 0.566 | 0.521–0.611 | 132.48 | 0.000 | 95.5 | REM | −0.72 | 0.505 |
|
| Specificity | 0.906 | 0.887–0.923 | 161.32 | 0.000 | 96.3 | REM |
|
|
|
| Positive LR | 3.862 | 2.347–6.353 | 36.95 | 0.000 | 83.8 | REM |
|
|
|
| Negative LR | 0.459 | 0.320–0.658 | 66.46 | 0.000 | 91.0 | REM |
|
|
|
| DOR | 10.269 | 7.501–15.795 | 8.77 | 0.187 | 31.6 | FEM |
|
|
| Combination of
both | Sensitivity | 0.833 | 0.796–0.865 | 28.17 | 0.000 | 78.7 | REM | 1.80 | 0.132 |
|
| Specificity | 0.644 | 0.615–0.672 | 34.10 | 0.000 | 82.4 | REM |
|
|
|
| Positive LR | 2.804 | 2.163–3.636 | 23.59 | 0.001 | 74.6 | REM |
|
|
|
| Negative LR | 0.228 | 0.149–0.350 | 21.42 | 0.002 | 72.0 | REM |
|
|
|
| DOR | 13.50 | 7.847–23.238 | 14.56 | 0.024 | 58.8 | REM |
|
|
ImmunoCyt test
The pooled sensitivity of the ImmunoCyt test for all
seven studies included in the final meta-analysis was 72.5% (95%
CI, 68.3–76.5%), the pooled specificity 65.7% (95% CI, 62.9–68.5%),
the pooled positive LR was 2.578 (95% CI, 2.003–3.318), the pooled
negative LR was 0.385 (95% CI, 0.327–0.452), and the pooled DOR was
7.114 (95% CI, 4.709–10.748) (Table
II).
Cytology test
The pooled sensitivity of cytology test was 56.6%
(95% CI, 52.1–61.1%), the pooled specificity was 90.6% (95% CI,
88.7–92.3%), the pooled positive LR was 3.862 (95% CI,
2.347–6.353), the pooled negative LR was 0.459 (95% CI,
0.320–0.658), and the pooled DOR was 10.269 (95% CI, 7.501–15.795)
(Table II).
Combined method (ImmunoCyt and
cytology)
We also collected the pooled meta-analysis of
bladder cancer patients with the combined method. The pooled
sensitivity was 83.3% (95% CI, 79.6–86.5%), the pooled specificity
was 64.4% (95% CI, 61.5–67.2%), the pooled positive LR was 2.804
(95% CI, 2.163–3.636), the pooled negative LR was 0.228 (95% CI,
0.149–0.350), and the pooled DOR was 13.50 (95% CI, 7.847–23.238)
(Table II).
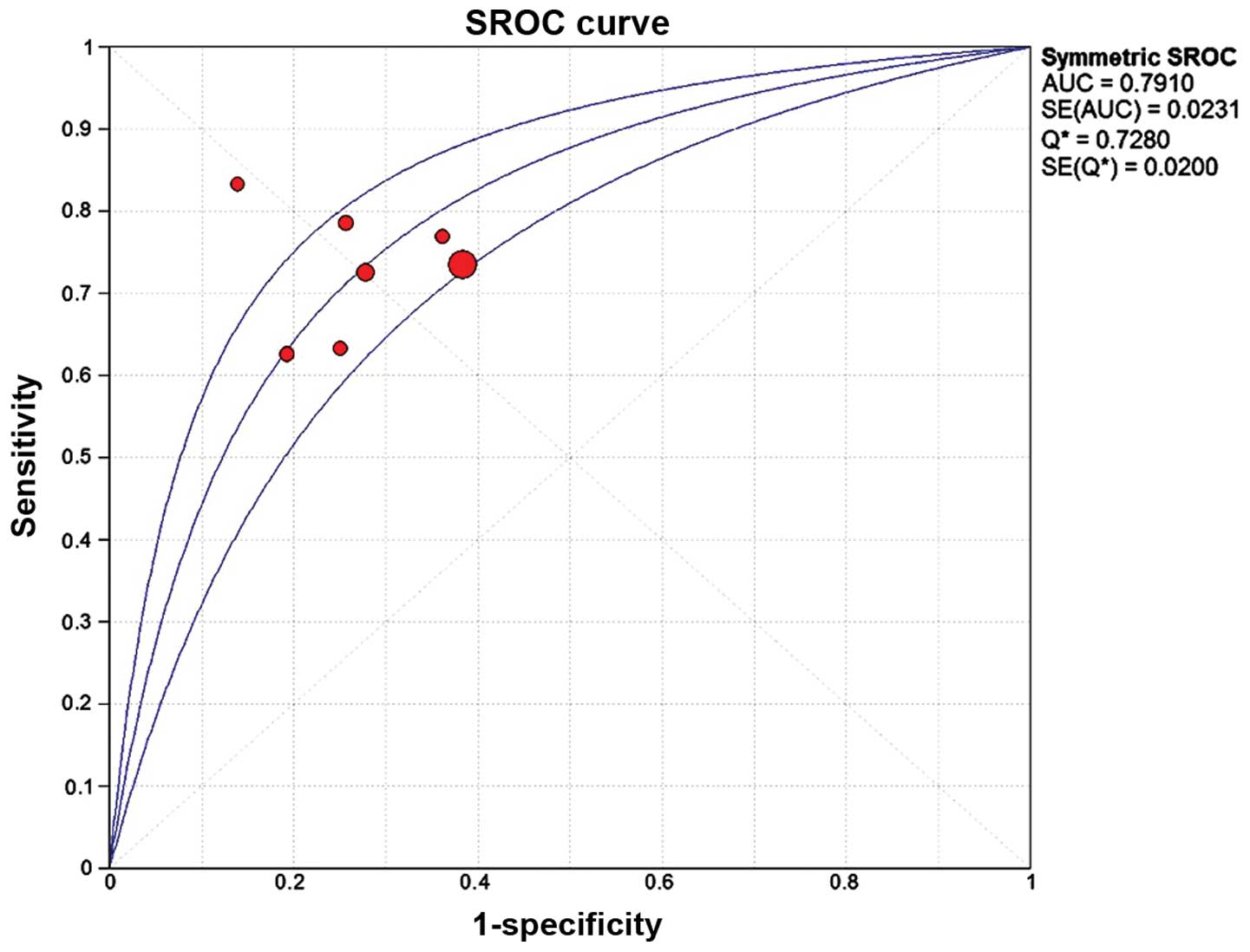
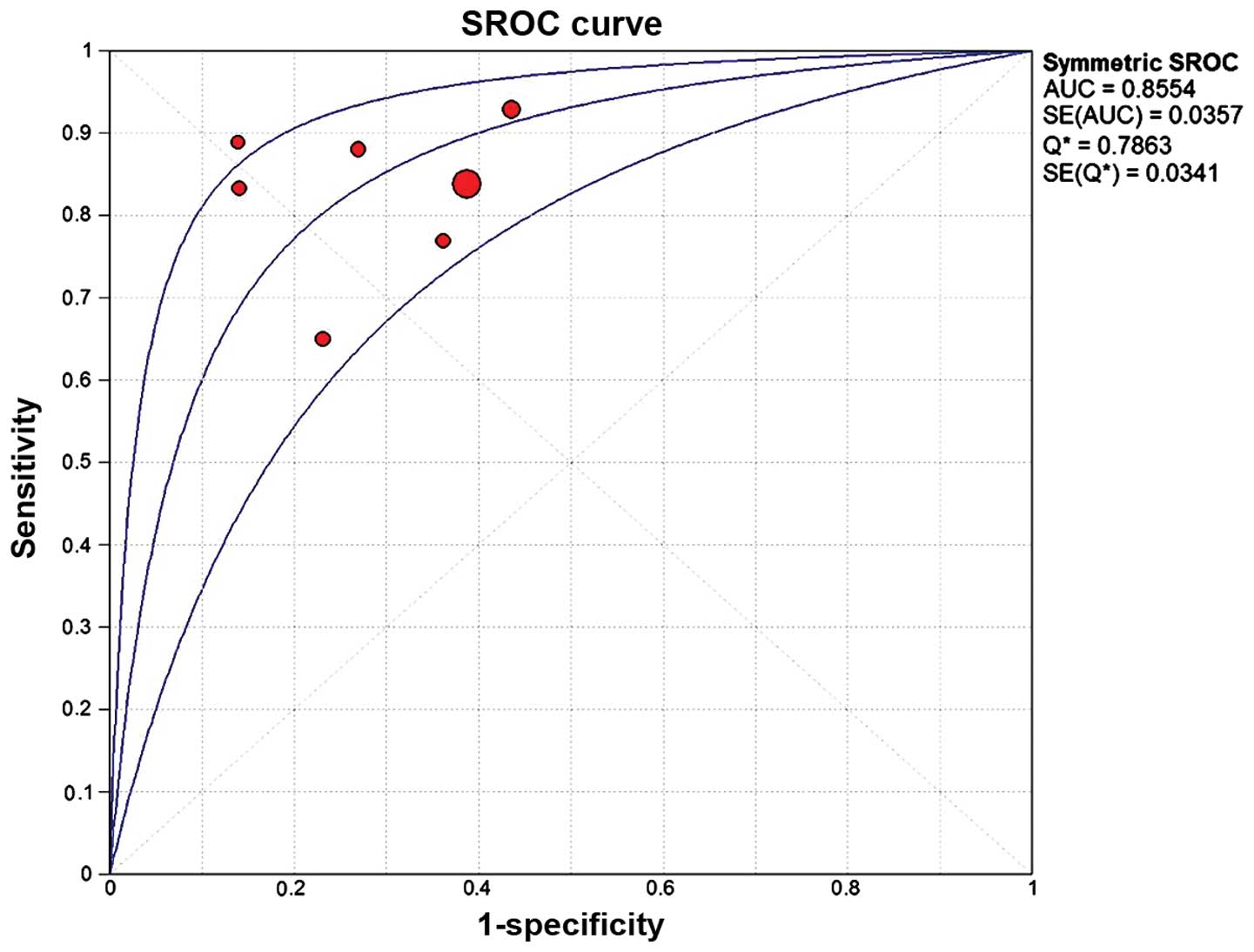
AUC and Q index in the three
tests
The AUC and Q index of ImmunoCyt test were 0.7910
and 0.7280, those of the cytology test 0.8239 and 0.7570, and those
of the combined method 0.8554 and 0.7863, respectively (Figs. 2–4).
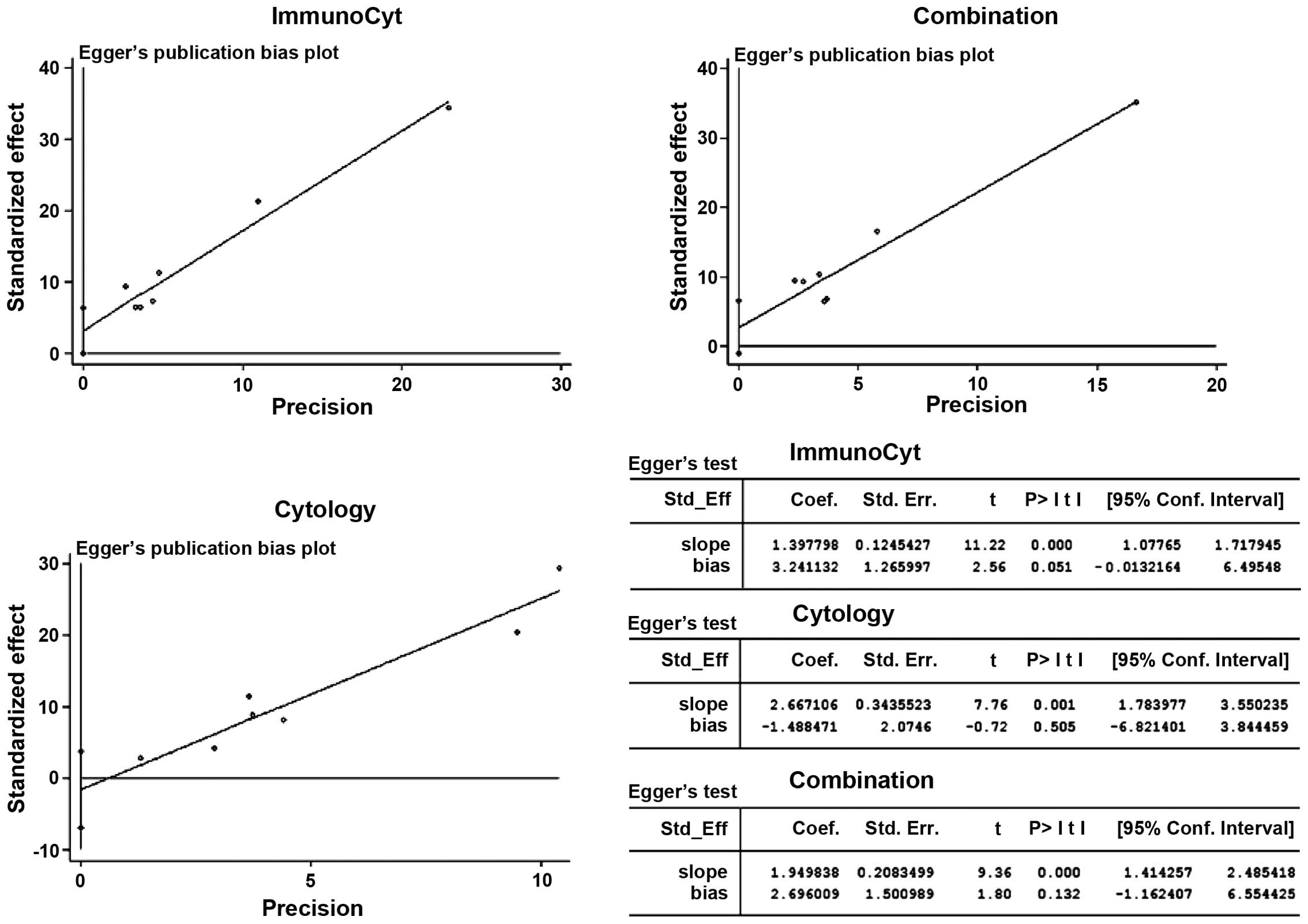
Publication bias
Eggers test was used to assess the publication bias.
For all samples, Eggers test provided no evidence of publication
bias for this meta-analysis. Detailed information is provided in
Fig. 5.
Discussion
As a useful adjunct for cystoscopy, cytology has
been used for more than 60 years for the diagnosis of urothelial
carcinoma (UC). The test suffers from low sensitivity (38–51%), but
boasts a high specificity (94–98%), particularly for high-grade
disease (25). The reliability of
cytology results depends on sample quality and cytopathologist
experience to some extent. Atypical results are often found in
urine cytology tests (6). Among these
atypical cytology results, biopsy reveals that malignancy underlies
23–68% of them. Investigators have also found that its sensitivity
is highly associated with tumor stage. For patients with
higher-grade bladder cancer, it appears to be more sensitive
(26–29).
With the aim of improving the low sensitivity of
cytology and the detection of low-risk UC, many voided urine
biomarker assays such as UroVysion, NMP22, BTA TRAK, and
ImmunoCyt/uCyt+ have been developed but have yet to gain widespread
clinical application. The ImmunoCyt test performance has been well
studied since its introduction by Fradet and Lockhard in 1997
(6,30). It is a triple immunofluorescent
monoclonal antibody assay associated with UC, approved by the US
Food and Drug Administration. A previous series reported a
sensitivity of 74–87% and specificity of 62–78%, with PPVs and NPVs
of 26–67% and 91–96%, respectively (6).
Additionally, the ImmunoCyt test can also provide
important information in evaluating hematuria, particularly in
patients with negative imaging and cystoscopy but atypical cytology
(31).
Many studies have reported on the diagnostic
accuracy of the ImmunoCyt and cytology tests in detecting bladder
cancer (29–32). The results of those studies, however,
have been met with skepticism due to their small sample sizes or
low statistical power. In the present meta-analysis, we combined
seven separate studies, consisting of 1,602 patients to compare the
diagnostic accuracy of the ImmunoCyt test with the urine cytology
test in detecting bladder cancer. We found that the ImmunoCyt test
had a higher sensitivity than the urine cytology test, but the
specificity, positive LR, negative LR, and DOR of the ImmunoCyt
test were lower compared with the urine cytology test. In addition,
the AUC and Q index of cytology were superior to those of the
ImmunoCyt test. Based on these comparisons, we can conclude that
the ImmunoCyt test would not replace the urine cytology test in
detecting bladder cancer.
We also collected data of a combined method
(combination of ImmunoCyt test and cytology). The pooled
sensitivity, specificity, positive LR, negative LR, DOR, AUC, and Q
index were 0.833, 0.644, 2.804, 0.228, 13.50, 0.8554 and 0.7863,
respectively. These data suggest that the ability of cytology to
detect malignancies of the bladder can be highly improved in
combination with ImmunoCyt. The results of the present study are in
agreement with previous findings of Mian et al regarding the
clinical usefulness of combining the two tests (32). Using the uCyt1/ImmunoCyt test in
combination with cytology to detect bladder cancer appeared to
improve the overall sensitivity for cytology alone. Furthermore,
the use of the two tests in combination constitute a potential
alternative option to limit the amount of cystoscopic evaluations
required for the follow-up of patients with low-risk bladder
cancer.
One limitation of our study is heterogeneity. The
considerable amount of heterogeneity detected between the studies
suggests a need for caution when pooling the diagnostic accuracy
measures together. Additionally, between-study heterogeneities may
distort the meta-analysis. The degree of heterogeneity is one of
the major concerns in a meta-analysis, as non-homogeneous data are
liable to result in misleading results (33). Different populations also contribute
to the heterogeneity. Therefore, the results of this meta-analysis
should be interpreted with caution. We minimized the likelihood of
bias by developing a detailed protocol prior to initiating the
study, by performing a rigorous search of published studies and by
using explicit methods for study selection, data extraction, and
data analysis.
Another limitation common to diagnostic
meta-analyses is the lack of clarity, quality, and standardization
in the methodology of diagnostic studies. Studies were assessed for
quality using STARD proforma to quantify the methodology of the
study design. Consequently, we excluded certain studies due to
ambiguity between the raw data and the diagnostic accuracy data in
the process of data extraction.
In conclusion, in this meta-analysis, we have
evaluated the pooled sensitivity, specificity, positive LR,
negative LR, DOR, AUC, and Q index of three tests (ImmunoCyt,
cytology, and combined test) from seven studies. We found that
ImmunoCyt was superior to cytology only in sensitivity, however,
inferior to cytology in specificity, positive LR, negative LR, DOR,
AUC, and Q index. In conclusion, cytology remains integral in the
detection of bladder cancer. Meta-analysis of the combined tests
suggests that the use of ImmunoCyt and cytology in combination
significantly improves the sensitivity for detecting bladder cancer
and promises to be an alternative option in the clinical
setting.
References
|
1
|
Ploeg M, Aben KK and Kiemeney LA: The
present and future burden of urinary bladder cancer in the world.
World J Urol. 27:289–293. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Garfield SS, Gavaghan MB, Armstrong SO and
Jones JS: The cost-effectiveness of blue light cystoscopy in
bladder cancer detection: United States projections based on
clinical data showing 4.5 years of follow up after a single
hexaminolevulinate hydrochloride instillation. Can J Urol.
20:6682–6689. 2013.PubMed/NCBI
|
|
3
|
Sullivan PS, Chan JB, Levin MR and Rao J:
Urine cytology and adjunct markers for detection and surveillance
of bladder cancer. Am J Transl Res. 2:412–440. 2010.PubMed/NCBI
|
|
4
|
Talwar R, Sinha T, Karan SC, Doddamani D,
Sandhu A, Sethi GS, Srivastava A, Narang V, Agarwal A and Adhlakha
N: Voided urinary cytology in bladder cancer: is it time to review
the indications? Urology. 70:267–271. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wiener HG: Cytology of the urinary tract.
A modern investigation method? Pathologe. 28:354–359. 2007.(In
German). PubMed/NCBI
|
|
6
|
Fradet Y and Lockhard C: Performance
characteristics of a new monoclonal antibody test for bladder
cancer: ImmunoCyt trade mark. Can J Urol. 4:400–405.
1997.PubMed/NCBI
|
|
7
|
Têtu B, Tiguert R, Harel F and Fradet Y:
ImmunoCyt/uCyt+ improves the sensitivity of urine cytology in
patients followed for urothelial carcinoma. Mod Pathol. 18:83–89.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Messing EM, Teot L, Korman H, Underhill E,
Barker E, Stork B, Qian J and Bostwick DG: Performance of urine
test in patients monitored for recurrence of bladder cancer: a
multicenter study in the United States. J Urol. 174:1238–1241.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mian C, Maier K, Comploj E, Lodde M,
Berner L, Lusuardi L, Palermo S, Vittadello F and Pycha A:
uCyt+/ImmunoCyt in the detection of recurrent urothelial carcinoma:
an update on 1991 analyses. Cancer. 108:60–65. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lodde M, Mian C, Comploj E, Palermo S,
Longhi E, Marberger M and Pycha A: uCyt+ test: alternative to
cystoscopy for less-invasive follow-up of patients with low risk of
urothelial carcinoma. Urology. 67:950–954. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sullivan PS, Nooraie F, Sanchez H,
Hirschowitz S, Levin M, Rao PN and Rao J: Comparison of ImmunoCyt,
UroVysion, and urine cytology in detection of recurrent urothelial
carcinoma: a ‘split-sample’ study. Cancer. 117:167–173.
2009.PubMed/NCBI
|
|
12
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mantel N and Haenszel W: Statistical
aspects of the analysis of data from retrospective studies of
disease. J Natl Cancer Inst. 22:719–748. 1959.PubMed/NCBI
|
|
14
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
DerSimonian R and Kacker R: Random-effects
model for meta-analysis of clinical trials: an update. Contemp Clin
Trials. 28:105–114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Walter SD: Properties of the summary
receiver operating characteristic (SROC) curve for diagnostic test
data. Stat Med. 21:1237–1256. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Altman DG and Bland JM: Diagnostic tests
3: receiver operating characteristic plots. BMJ. 309:1881994.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yafi FA, Brimo F, Steinberg J, Aprikian
AG, Tanguay S and Kassouf W: Prospective analysis of sensitivity
and specificity of urinary cytology and other urinary biomarkers
for bladder cancer. Urol Oncol. 33:66.e25–66.e31. 2015. View Article : Google Scholar
|
|
19
|
Soyuer I, Sofikerim M, Tokat F, Soyuer S
and Ozturk F: Which urine marker test provides more diagnostic
value in conjunction with standard cytology- ImmunoCyt/uCyt+ or
Cytokeratin 20 expression. Diagn Pathol. 4:202009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Horstmann M, Patschan O, Hennenlotter J,
Senger E, Feil G and Stenzl A: Combinations of urine-based tumour
markers in bladder cancer surveillance. Scand J Urol Nephrol.
43:461–466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Toma MI, Friedrich MG, Hautmann SH, Jäkel
KT, Erbersdobler A, Hellstern A and Huland H: Comparison of the
ImmunoCyt test and urinary cytology with other urine tests in the
detection and surveillance of bladder cancer. World J Urol.
22:145–149. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hautmann S, Toma M, Lorenzo Gomez MF,
Friedrich MG, Jaekel T, Michl U, Schroeder GL, Huland H, Juenemann
KP and Lokeshwar VB: Immunocyt and the HA-HAase urine tests for the
detection of bladder cancer: a side-by-side comparison. Eur Urol.
46:466–471. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis
CA, Glasziou PP, Irwig LM, Moher D, Rennie D, de Vet HC and Lijmer
JG: Standards for Reporting of Diagnostic Accuracy: The STARD
statement for reporting studies of diagnostic accuracy: explanation
and elaboration. Clin Chem. 49:7–18. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis
CA, Glasziou PP, Irwig LM, Lijmer JG, Moher D, Rennie D and de Vet
HC: STARD Group: Towards complete and accurate reporting of studies
of diagnostic accuracy: the STARD initiative. Fam Pract. 21:4–10.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Raab SS, Grzybicki DM, Vrbin CM and
Geisinger KR: Urine cytology discrepancies: frequency, causes, and
outcomes. Am J Clin Pathol. 127:946–953. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Deshpande V and McKee GT: Analysis of
atypical urine cytology in a tertiary care center. Cancer.
105:468–475. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mokhtar GA, Al-Dousari M and Al-Ghamedi D:
Diagnostic significance of atypical category in the voided urine
samples: a retrospective study in a tertiary care center. Urol Ann.
2:100–106. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kapur U, Venkataraman G and Wojcik EM:
Diagnostic significance of ‘atypia’ in instrumented versus voided
urine specimens. Cancer. 114:270–274. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Odisho AY, Berry AB, Ahmad AE, Cooperberg
MR, Carroll PR and Konety BR: Reflex ImmunoCyt testing for the
diagnosis of bladder cancer in patients with atypical urine
cytology. Eur Urol. 63:936–940. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Vriesema JL, Atsma F, Kiemeney LA, Peelen
WP, Witjes JA and Schalken JA: Diagnostic efficacy of the ImmunoCyt
test to detect superficial bladder cancer recurrence. Urology.
58:367–371. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Schmitz-Dräger BJ, Beiche B, Tirsar LA,
Schmitz-Dräger C, Bismarck E and Ebert T: Immunocytology in the
assessment of patients with asymptomatic microhaematuria. Eur Urol.
51:1582–1588. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Mian C, Lodde M, Comploj E, Palermo S,
Mian M, Maier K and Pycha A: The value of the ImmunoCyt/uCyt+ test
in the detection and follow-up of carcinoma in situ of the urinary
bladder. Anticancer Res. 25:3641–3644. 2005.PubMed/NCBI
|
|
33
|
Moreno SG, Sutton AJ, Thompson JR, Ades
AE, Abrams KR and Cooper NJ: A generalized weighting
regression-derived meta-analysis estimator robust to small-study
effects and heterogeneity. Stat Med. 31:1407–1417. 2012. View Article : Google Scholar : PubMed/NCBI
|