Introduction
Squamous cell carcinoma (SCC) represents the vast
majority (90%) of malignant oral neoplasms (1). Recent figures on SCCs emphasise the
growing incidence rate and the limited and often unsatisfying
treatment options (2,3). Treatments are known to be unsatisfactory
in terms of survival rates, as local and regional metastases occur
frequently even in small tumors (4).
The harm caused by agents, such as alcohol or tobacco, is important
in cancerization, and may be responsible for the formation of
secondary tumors and disease recurrence (5,6). A
detailed knowledge concerning the molecular mechanisms in the
pathogenesis and progression of SCCs, and its precursor lesions, is
required to aid in the improvement of therapeutics and incidence
rates.
Cytokeratins (CKs) are major intermediate filaments
in squamous epithelium and are critical in cell stabilization,
shape, intracellular signalling and transport (7,8). CK
expression is a hallmark of tumor progression. Previous studies
demonstrated that the expression of high-molecular weight CK8 and
18 was associated with dysplasia grades of tumor precursor lesions
and an unfavorable prognosis for patients with SCCs (9,10). Other
studies had similar observations (11,12). Loss
of CK8 phosphorylation initiates an increased cell migration and
tumor spread in SCCs, whereas loss of CK8 and 18 led to alterations
in α6β4-integrin mediated signalling and decreased neoplastic
progression (11,13,14). In
addition, an increased expression of low-molecular weight CK19 was
associated with high-grade dysplasia and squamous intraepithelial
neoplasia and a decreased survival rate of patients with SCCs
(9,15). CK19 expression is not observed in
benign or hyperplastic regions of keratinized oral epithelium
(10,15). Additionally, the expression of CKs
interferes with a multitude of other intracellular regulation
pathways, including numerous kinases, receptors and apoptotic
proteins (16); therefore, the
effects of CKs are highly complex.
The present study demonstrates the frequencies of
low and high molecular weight CKs in SCCs of the oral cavity with
respect to their anatomical sublocalization, and evaluates the
coexpression of a multitude of proteins involved in various
cellular regulatory pathways. The aim of the present study was to
elucidate the complex interaction between CK expression patterns
and alterations in other cellular pathways. The present results
revealed the existence of two pathogenetic pathways in the
evolution of oral SCC, which are associated with the preferential
expression of low- and high-molecular weight CKs.
Patients and methods
Patients
All patients eligible for the current study
presented with histologically confirmed oral SCC, and underwent
surgery at the University Hospital Muenster (Münster, Germany)
between January 1988 and December 2000. Data collection and
evaluation was conducted in compliance with the current version of
the Declaration of Helsinki and the International Conference for
Harmonization of Good Clinical Practice (17,18). All
data and specimens were evaluated after obtaining written informed
consent from the patient and ethical approval from the Ethical
Commission of the Medical Association Westfalen-Lippe and the
Faculty of Medicine of the Westphalian Wilhelms-University
Muenster. The tumor samples were formalin-fixed, archival
paraffin-embedded tissues from 193 patients (154 men; 39 women)
with primary oral SCC. The patients' mean age was 59 years (range,
31–90 years) (Table I). Information
regarding clinicopathological details and treatment modalities of
this tumor series is described in previous studies (9,10,19–21).
According to the Union for International Cancer Control guidelines
(22), all the SCCs were classified
post-surgery by the tumor-node-metastasis system (T1=96, T2=82,
T3-4=15; N0=136, N>0=57). All patients attended a follow-up
program with clinical evaluation for 4–181 months. As described in
previous studies (9,10,19–21), the
time of survival was defined as the time between the date of
surgery and the date of histopathologically proven tumor
recurrence, metastatic disease, death associated with the disease
or a tumor-free follow-up period of 60 months. Patients who missed
regular attendance at follow-up were excluded from the present
study.
 | Table I.Clinicopathological characteristics
of 193 patients with oral squamous cell carcinoma. |
Table I.
Clinicopathological characteristics
of 193 patients with oral squamous cell carcinoma.
| Characteristic | Value |
|---|
| Age at diagnosis,
years |
|
|
Mean | 59 |
|
Range | 31–90 |
| Gender |
|
|
Female | 39 |
|
Male | 154 |
| Tumor stage |
|
| T1 | 96 |
| T2 | 82 |
|
T3-T4 | 15 |
| Lymph node |
|
|
Negative | 136 |
|
Positive | 57 |
| Tumor grade |
|
| G1 | 44 |
| G2 | 126 |
| G3 | 23 |
| Disease
recurrence |
|
|
Positive | 66 |
|
Negative | 127 |
| Localization |
|
| Floor
of mouth | 76 |
|
Tongue | 49 |
|
Other | 68 |
Immunohistochemistry
To provide equal assessment conditions, all tumor
samples were analyzed by tissue microarray (TMA) and
immunohistochemistry. As previously described (23), all TMAs were used according to a
standard procedure. For the TMA block construction, two punch
biopsies (diameter, 0.6 mm) were extracted from formalin-fixed,
paraffin-embedded tumor tissue (thickness, 4 µm) using a tissue
microarray instrument (Beecher Instruments, Inc., Sun Prairie, WI,
USA) and inserted into a novel acceptor block. The acceptor block
underwent deparaffinization, using various concentrations of
ethanol (70, 95 and 100%; Walter-CMP GmbH & Co. KG, Kiel,
Germany) and rehydration. Endogenous peroxidase activity was
blocked using methanol (with 0.3% hydrogen peroxide) (Walter-CMP
GmbH & Co. KG) for 30 min. Antigen retrieval was preceded by a
cooling time of 20 min at room temperature and incubation with
primary antibodies for 30 min at room temperature (Table II). Catalyzed Signal Amplification
System (Dako, Glostrup, Denmark) was used for CK1, 5/6, 8/18, 10,
14 and 19 immunohistochemistry, according to the manufacturer's
protocol. The staining procedures for p53, p21, p27, p16, cyclin
D1, epidermal growth factor receptor, mast/stem cell growth factor
receptor (c-kit), B-cell lymphoma 6, α/β/γ-catenin, hypoxia
inducible factor-1α (HIF-1α), glucose transporter 1 (GLUT1),
carbonic anhydrase 9 (CAIX), caspase-3, heat shock protein (hsp) 70
and X-linked inhibitor of apoptosis protein (XIAP) were performed
as previously described (24,25). Antigen detection was performed by a
standardised avidin-biotin complex method using anti-rabbit and
anti-mouse biotinylated antibodies [Dako REAL Detection Systems
(LSAB+); catalog no. K5003; Dako] and a Biotin-Blocking System
(Ready-to-Use, catalog no. X0590; Dako). Diaminobenzidine (included
in the p16 and EGFR kits; Table II)
or LSAB 2 System-AP (Dako) was used for visualization, along with
counterstaining with hematoxylin for 45 sec, followed by
dehydration in alcohol and xylene (Walter-CMP GmbH & Co. KG).
During TMA analysis and immunohistochemistry, negative (omission of
the primary antibody) and positive controls were performed.
| Table II.Primary antibodies used for
immunohistochemistry in the present study. |
Table II.
Primary antibodies used for
immunohistochemistry in the present study.
| Antibody | Supplier | Catalog no. | Clone |
Mono/polyclonal | Species | Dilution | Antigen
retrieval |
|---|
| p21 | Merck
Millipore | 05–655 | CP74 | Mono | Mouse | 1:500 | Citrate buffer
(pH6) |
| p27 | BD TL | 610241 | 57/Kip1/p27 | Mono | Mouse | 1:1,000 | Citrate buffer
(pH6) |
| p53 | Dako | M7001 | DO-7 | Mono | Mouse | 1:100 | EDTA (pH8) |
| HIF-1α | BD TL | 610958 | 54/HIF-1α | Mono | Mouse | 1:50 | EDTA (pH8) |
| GLUT1 | Dako | M7211 | Clone A 35 | Mono | Mouse | 1:40 | EDTA (pH8) |
| CAIX | Abcam | ab128883 | – | Poly | Rabbit | 1:1,000 | Citrate buffer
(pH6) |
| XIAP | BD TL | 610716 | 28/hILP/XIAP | Mono | Mouse | 1:50 | Citrate buffer
(pH6) |
| Hsp 70 | Invitrogen | 33–3800 | MB-H1 | Mono | Mouse | 1:40 | Citrate buffer
(pH6) |
| α-catenin | BD TL | 610194 | 5/a-catenin | Mono | Mouse | 1:250 | EDTA (pH8) |
| β-catenin | BD TL | 610153 |
14/beta-Catenin | Mono | Mouse | 1:1,000 | EDTA (pH8) |
| γ-catenin | BD TL | 610253 | 15/γ-catenin | Mono | Mouse | 1:1,500 | EDTA (pH8) |
| BCL-6 | Dako | M7211 | PG-B6p | Mono | Mouse | 1:50 | Citrate buffer
(pH6) |
| Caspase-3 | Invitrogen | 35–1600Z | 43191 | Mono | Mouse | 1:100 | Citrate buffer
(pH6) |
| C-kit | Dako | A4502 | – | Poly | Rabbit | 1:200 | Citrate buffer
(pH6) |
| CK1 | Novocastra | NCL-Ck1 | 34βB4 | Mono | Mouse | 1:150 | Citrate buffer
(pH6) |
| CK5/6 | Dako | M7237 | D5/16 B4 | Mono | Mouse | 1:80 | Autoclave (10
min) |
| CK10 | Dako | M7002 | DE-K10 | Mono | Mouse | 1:400 | Citrate buffer
(pH6) |
| CK14 | Dianova GmbH | DLN-06600 | LL002 | Mono | Mouse | 1:50 | Citrate buffer
(pH6) |
| CK8/18 | Dianova GmbH | DLN-08110 | K8.8/DC10 | Mono | Mouse | 1:40 | Autoclave (10 min),
citrate buffer (pH) |
| CK19 | Dianova GmbH | DLN-08330 | KS19.1 | Mono | Mouse | 1:80 | Citrate buffer
(pH6) |
| Cyclin D1 | Novocastra | NCL-L-cyclin
D1-GM | P2D11F11 | Mono | Mouse | 1:20 | EDTA (pH8) |
| EGFR | Dako | K1492 | pharmDX kit | Mono | Mouse | – | – |
| p16 | CINtec | 9517 | E6H4 | Mono | Mouse |
| Citrate buffer
(pH6) |
Scoring of staining
Expression of CK1, 5/6, 8/18, 10, 14 and 19 was
evaluated by the rate of positively stained cells in each core. The
expression levels (%) were classified into three groups for CK19
(0%, no expression; 1–50%, moderate expression; >50%, high
expression) and into two groups for CK5/6, 8/18, 1, 10 and 14 (0%,
no expression; ≥1%, positive expression). The mean percentage value
of two cores from one tumor was calculated. Cytoplasmic expression
of hsp70, caspase-3 and XIAP was graded as negative or positive
(intermediate to strong expression), irrespective of the relative
number of stained tumor cells. The remaning molcecules were
assessed as follows: CAIX and p21/27/16 (<1%, no expression;
≥1%, positive expression); HIF-1α and GLUT1 (<1%, no expression;
≥1–4%, low expression; ≥5%, high expression); BCL-6, α-catenin,
cyclin D1, c-kit and EGFR (0–15%, no expression; 16–50%, low
expression; 85–100%, positive expression); β/γ-catenin (0–15%, no
expression; 16–50%, low expression; 51–100%, high expression); p53
(<5%, no expression; ≥5–50%, low expression; ≥50%, high
expression). Moderate, intermediate, strong and high expressions
were rendered as positive expression.
Statistical analysis
Statistical analysis was performed using
χ2 analysis. Biomathematical analysis of
immunohistochemical data was evaluated using permutation analysis,
which analyses information from protein-expression patterns of TMA
data and identifies synergistic or antagonistic effects amongst all
evaluated proteins (26). Botstein
et al (27) describe this
method as preserving the original physiological information of the
tumor tissue and revealing the different compounds of the tumor
samples to the smallest detail (28,29). This
combinatorial analysis calculates the ideal precedence of
protein-expression coherence; therefore allowing the generation of
an overview of differential regulation patterns in different tumor
subgroups. A detailed description of this approach and its use in a
clinical setting, using TMA data, have been previously described
(24,29). Statistical analysis was performed on R
version 3.1.3 software (www.r-project.org/), Fortran 95-based program
‘TMAinspiration’ (complex-systems.uni-muenster.de/tma_inspiration.html)
and SPSS version 21.0 software (IBM SPSS, Armonk, NY, USA)
Results
CK expression patterns and tumor
localization
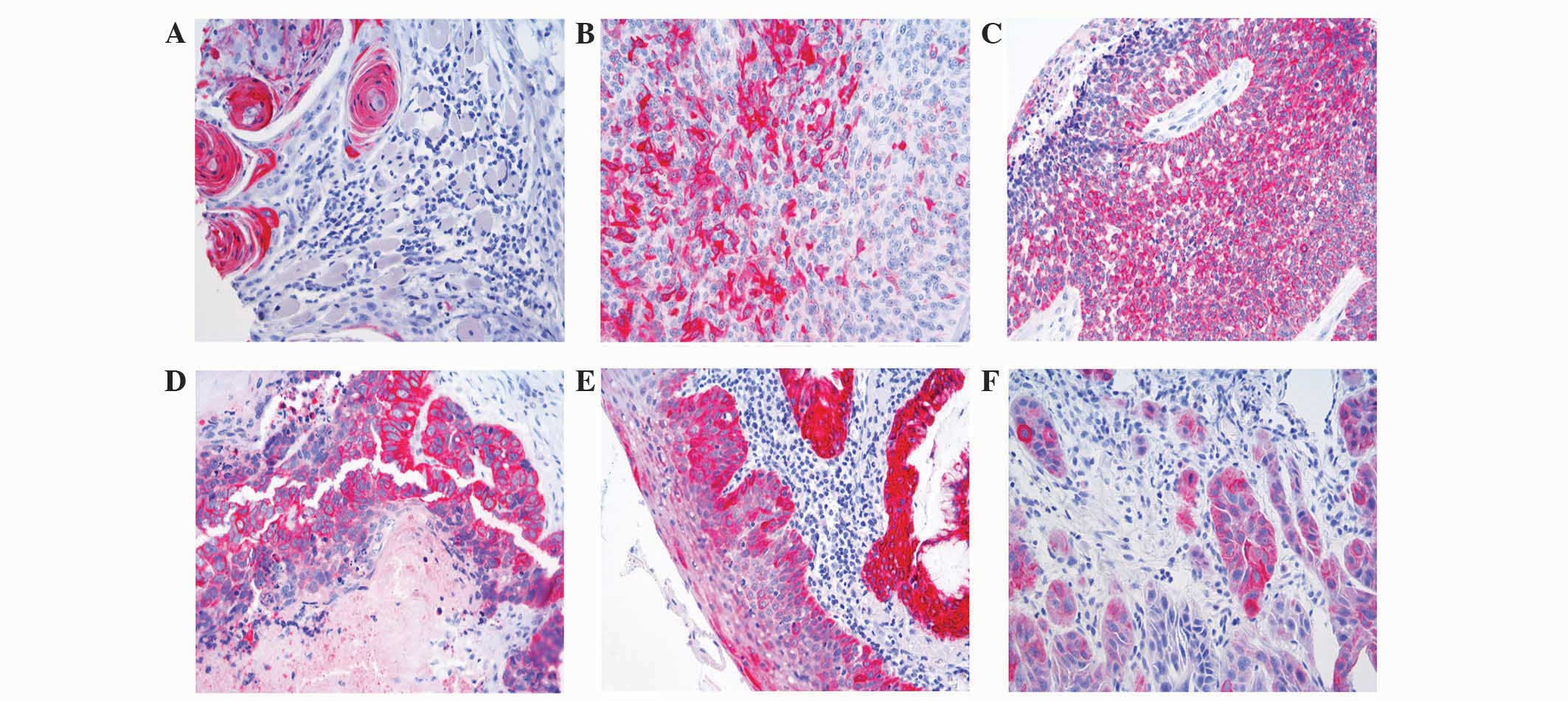
The expression (%) of the 6 CKs and other biomarkers
in the SCC tumors are presented in Table III. Representative images of
immunohistochemical staining are presented in Fig. 1.
| Table III.Expression of CKs and other
biomarkers in 193 samples of oral squamous cell carcinoma. |
Table III.
Expression of CKs and other
biomarkers in 193 samples of oral squamous cell carcinoma.
|
| Expression, % of
tumors |
|---|
|
|
|
|---|
| Protein | Negative | Positive |
|---|
| CK1 | 53.9 |
0.5 |
| CK5/6 |
1.7 |
98.3 |
| CK8/18 | 33.3 |
66.7 |
| CK10 | 62.8 |
37.2 |
| CK14 |
2.6 |
97.4 |
| CK19 | 59.9 |
40.1 |
| α-catenin | 34.6 |
65.4 |
| β-catenin | 15.8 |
84.2 |
| γ-catenin | 35.0 |
65.0 |
| GLUT1 |
8.5 |
91.5 |
| Caspase-3 | 74.2 |
25.8 |
| XIAP | 80.5 |
19.5 |
| CAIX | 73.4 |
26.6 |
| Hsp 70 | 89.3 |
10.7 |
| C-kit | 86.4 |
13.6 |
| p16 | 79.4 |
20.6 |
| p21 | 28.8 |
71.2 |
| p27 | 79.8 |
20.2 |
| p53 |
0.0 | 100.0 |
| BCL-6 | 78.7 |
21.3 |
| EGFR | 24.9 |
75.1 |
| Cyclin D1 | 50.6 |
49.4 |
| HIF-1α | 42.2 |
57.8 |
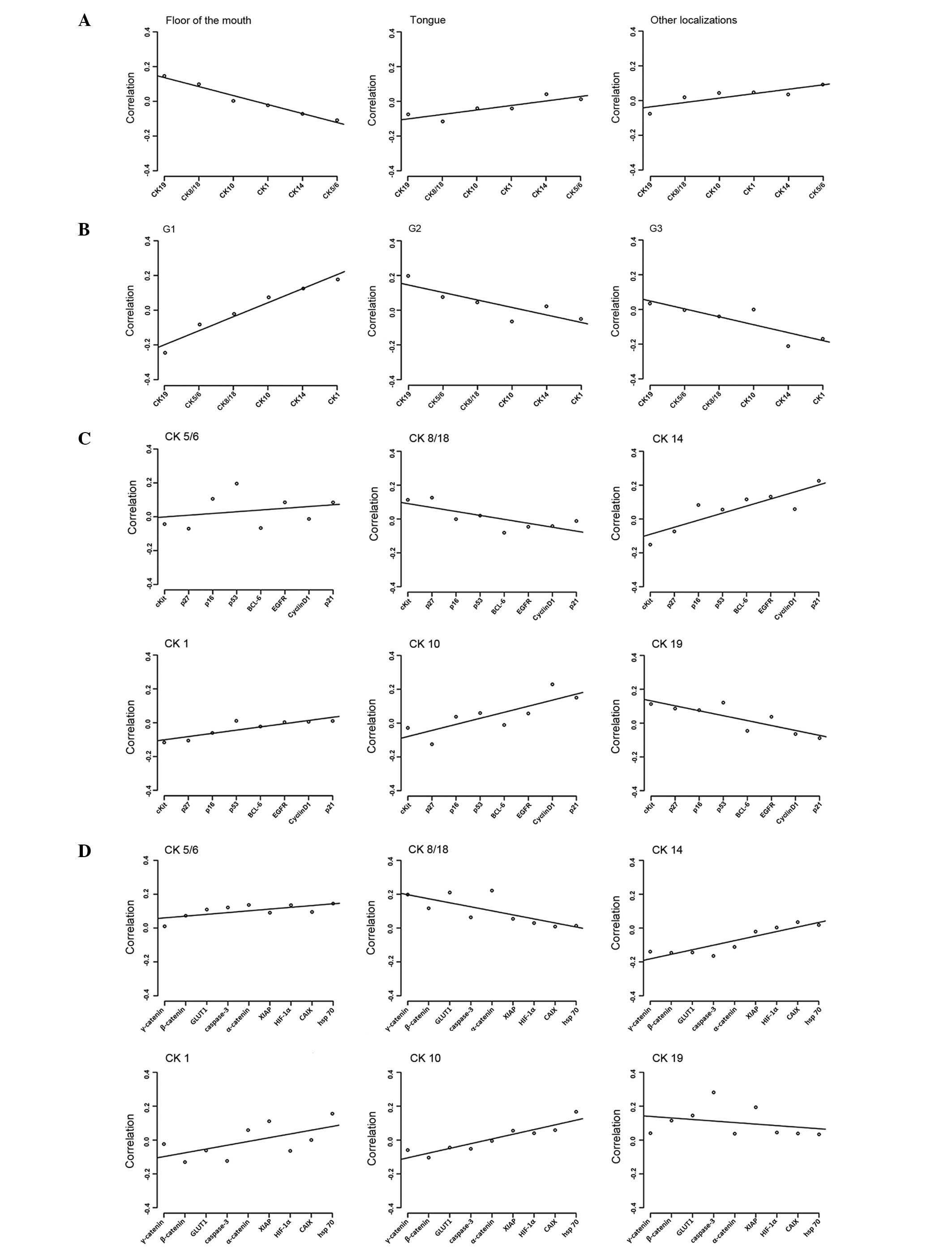
Global, but not individual, CK expression in oral
SCCs was significantly different between the anatomical
localization of the tumor in the floor of the mouth and other
localizations (floor of mouth vs. tongue, P=1.6×10−4;
floor of mouth vs. other localizations, P=1.3×10−4;
Fig. 2A). SCCs located on the floor
of the mouth revealed inverse regression lines in contrast to SCCs
of other tumor subsites within the oral cavity, including the
maxilla, tonsils and buccal region. Expression of CK8/18 and 19 was
associated with SCCs of the floor of the mouth, whereas CK1, 10,
8/18 and 19 were equally expressed in all other subsites (Fig. 2A).
CK expression patterns and tumor
grade
Significant differences could be observed in global
CK expression patterns in association with tumor grade. Regression
lines for grade 2 (G2) and 3 (G3) SCCs were similar, but regression
lines for grade 1 (G1) SCCs exhibited an inverse behavior compared
to G2 and G3 (Fig. 2B).
G1 carcinomas revealed a statistically significant
inverse association with G2 and G3 carcinomas concerning the
expression of CK19 (P=4.1×10−5 and
P=6.9×10−5, respectively). Expression of CK14 and 1 was
predominantly observed in G3 SCCs (P=5.1×10−3 and
P=0.03, respectively).
CK expression patterns and cell cycle
proteins and growth factors
Two patterns of cell cycle proteins expression were
observed in association with CK expression. High-molecular weight
CK14, 5/6, 1 and 10 exhibited similar regression lines compared
with the regression lines exhibited by low-molecular weight CK8/18
and 19. In this molecular pattern p21, due to its extreme position
in the regression approach, has the strongest impact in
discriminating between the 6 CKs (Fig.
2C). By contrast, EGFR does not play a major regulative
role.
CK expression patterns and factors
involved in cell motility, apoptosis and cellular stress
responses
Similar findings were observed in a second approach
for factors involved in cell motility, apoptosis and cellular
stress responses. As demonstrated in Fig.
2C, CK14, 5/6, 1 and 10 revealed a contrasting expression
compared with CK8/18 and 19. Comparable results were observed for
c-kit, α/β/γ-catenin, HIF-1α, GLUT1, CAIX, caspase-3, hsp 70 and
XIAP (Fig. 2D). In this second
pattern, the discriminating role was primarily performed by
γ-catenin and hsp 70.
Discussion
SCC of the oral cavity is associated with a variety
of risk factors, including smoking, alcohol abuse, tobacco chewing,
oral hygiene and human papilloma virus (HPV) infection (30–34). The
current treatment protocols are based on a combination of surgery
and radio/chemotherapy (35,36). Despite these complex,
multidisciplinary treatment regimens, the long term results are
unsatisfactory (1,37), the reasons for which are unclear. The
underlying biology of SCCs remains poorly understood, and
discerning the distinct molecular mechanisms underlying SCC may
lead to improvements in treatment strategies.
CKs are the major intermediate filaments of squamous
epithelium (38,39), and in different organ systems it has
been demonstrated that alterations in CK expression patterns leads
to the altered expression of numerous genes and proteins (9–11,40).
The present study demonstrates that previously
described (9,10) prognostically relevant cytokeratin
expression patterns are associated with different expression
patterns of crucial cellular proteins. Low-molecular weight CK8/18
and 19 expression had opposing patterns to high-molecular weight
CK1, 5/6, 10 and 14 with biomarkers involving cell cycle regulation
(p21), hypoxic stress (HIF-1α and CAIX) or cellular adhesion
(α/γ-catenin). This indicates that CK8/18 and 19 are expressed in
poorly-differentiated hypoxic SCC with a higher degree of cell
cycle deregulation, whereas CK1, 5/6, 10 and 14 appear to be
expressed in well-differentiated cancers with lower hypoxia and
cell cycle deregulation. These results are similar to the general
observation that low-molecular weight CK8/18 and 19 cytokeratins,
whose expression is a hallmark of glandular tissues, are not
physiologically expressed in normal squamous epithelium, but may be
expressed during carcinogenesis (11,12,41).
These results are similar to previous studies
regarding the prognostic significance of these proteins (9,10,19,21).
However, the interpretation of these findings is challenging, since
it cannot be excluded that these alterations in expression of CKs
and the chosen biomarkers are a reflection of tumor progression. By
contrast, the present results may allow an alternative
interpretation; in invasive breast cancer it was previously
demonstrated that the expression of distinct high-molecular weight
CKs defines a subgroup of poorly-differentiated breast cancer,
representing a unique, independent pathway associated with poor
prognosis, which has different responses to various treatment
modalities (42,43). Therefore, the present results may be
as a result of the existence of different pathways in the
pathogenesis of oral SCCs. At present, two pathways characterized
by the differential expression of CKs may be distinguished in the
present study. In various other tumor entities, such parallel,
independent pathogenetic pathways have been reported for colorectal
cancer, ovarian cancer and SCCs of the female genital tract,
including the vulva and cervix (24,44–46).
In addition, the present authors consider that the
results support the hypothesis that SCCs of the oral cavity may not
be regarded as a homogeneous entity. In the present study, global
expression patterns of high- and low-molecular weight CKs exhibit
clear differences between G1 and G2/3 SCCs. It may be argued that
the alteration in CK expression has been interpreted as a result of
tumor dedifferentiation. However, the present authors hypothesize
that this may not be true for several reasons. The expression of
CK8/18 and 19 has been described in epithelial precursor lesions of
oral SCC (10), and therefore does
not support the hypothesis that CK8/18 and 19 expression is a late
phenomena in carcinogenesis after invasion has occurred. It is also
widely accepted that CK expression patterns appear to be highly
conserved during tumor progression (8). As a consequence, the existence of CK8/18
and/or 19-positive oral SCC raises fundamental controversies
concerning their formal pathogenesis (9,10,12,41). These
carcinomas appear to represent an independent pathway rather than
being the endstage of a stepwise dedifferentiation of CK8/18/19
negative SCCs. Therefore, it may be postulated that there is a low-
and high-grade pathway. A similar concept has also been proposed
for squamous intraepithelial neoplasms in the cervix and the vulva
(47,48), which is associated with various HPV
subtypes (44).
The oral cavity is a highly complex anatomical
region, emerging from various branchial arches that are associated
with an aggregation of mesenchyme, ectoderm and endoderm (49–51);
however, to what extent tumor localization has an effect on tumor
biology and prognosis remains to be demonstrated. The present
results reveal that differences appear to exist between SCCs on the
floor of the mouth and SCCs of other anatomical subsites within the
oral cavity, as observed by previous studies (5,21,52,53). In
the present study, SCCs of the floor of the mouth had an increased
expressed of CK8/18 and 19. The number of tumors investigated in
the present study was too small to allow for a definite conclusion;
however the present results reveal that complex interactions appear
to exist between the expression of CKs and other major cellular
proteins, as well as tumor grade and anatomical sublocalization of
SCCs of the oral cavity.
In summary, the present study analyzed low- and
high-molecular weight CK expression in association with the
expression of various other major cellular proteins using a
sophisticated biomathematical algorithm in a series of 193 SCCs of
the oral cavity. The present study provided evidence of the
existence of two pathogenetic pathways characterized by the
expression of low- and high-molecular weight CKs in oral SCC. These
results provide evidence for additional investigation concerning
the pathways identified and provide improved understanding of oral
tumor biology.
References
|
1
|
Scully C and Bagan J: Oral squamous cell
carcinoma overview. Oral Oncol. 45:301–308. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
American Cancer Society: Cancer Facts
& Figures 2015. American Cancer Society. Altanta, GA: 2015.
|
|
3
|
Cancer Research UK: Oral cancer incidence
statistics. http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/oral-cancer/incidence.s
|
|
4
|
D'Cruz AK, Vaish R, Kapre N, Dandekar M,
Gupta S, Hawaldar R, Agarwal JP, Pantvaidya G, Chaukar D, Deshmukh
A, et al: Head and Neck Disease Management Group: Elective versus
therapeutic neck dissection in node-negative oral cancer. N Engl J
Med. 373:521–529. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yamauchi K, Fujioka Y, Kogashiwa Y and
Kohno N: Quantitative expression study of four cytokeratins and p63
in squamous cell carcinoma of the tongue: Suitability for sentinel
node navigation surgery using one-step nucleic acid amplification.
J Clin Pathol. 64:875–879. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Slaughter DP, Southwick HW and Smejkal W:
Field cancerization in oral stratified squamous epithelium;
clinical implications of multicentric origin. Cancer. 6:963–968.
1953. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chu PG and Weiss LM: Keratin expression in
human tissues and neoplasms. Histopathology. 40:403–439. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moll R, Franke WW, Schiller DL, Geiger B
and Krepler R: The catalog of human cytokeratins: Patterns of
expression in normal epithelia, tumors and cultured cells. Cell.
31:11–24. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fillies T, Werkmeister R, Packeisen J,
Brandt B, Morin P, Weingart D, Joos U and Buerger H: Cytokeratin
8/18 expression indicates a poor prognosis in squamous cell
carcinomas of the oral cavity. BMC Cancer. 6:102006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fillies T, Jogschies M, Kleinheinz J,
Brandt B, Joos U and Buerger H: Cytokeratin alteration in oral
leukoplakia and oral squamous cell carcinoma. Oncol Rep.
18:639–643. 2007.PubMed/NCBI
|
|
11
|
Alam H, Gangadaran P, Bhate AV, Chaukar
DA, Sawant SS, Tiwari R, Bobade J, Kannan S, D'Cruz AK, Kane S and
Vaidya MM: Loss of keratin 8 phosphorylation leads to increased
tumor progression and correlates with clinico-pathological
parameters of OSCC patients. PLoS One. 6:e277672011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gires O, Mack B, Rauch J and Matthias C:
CK8 correlates with malignancy in leukoplakia and carcinomas of the
head and neck. Biochem Biophys Res Commun. 343:252–259. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Raul U, Sawant S, Dange P, Kalraiya R,
Ingle A and Vaidya M: Implications of cytokeratin 8/18 filament
formation in stratified epithelial cells: Induction of transformed
phenotype. Int J Cancer. 111:662–668. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Alam H, Kundu ST, Dalal SN and Vaidya MM:
Loss of keratins 8 and 18 leads to alterations in
α6β4-integrin-mediated signalling and decreased neoplastic
progression in an oral-tumour-derived cell line. J Cell Sci.
124:2096–2106. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lindberg K and Rheinwald JG: Suprabasal 40
kd keratin (K19) expression as an immunohistologic marker of
premalignancy in oral epithelium. Am J Pathol. 134:89–98.
1989.PubMed/NCBI
|
|
16
|
Paramio JM and Jorcano JL: Beyond
structure: Do intermediate filaments modulate cell signalling?
Bioessays. 24:836–844. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
World Medical Association: World Medical
Association Declaration of Helsinki. Ethical principles for medical
research involving human subjects. Bull World Health Organ.
79:373–374. 2001.PubMed/NCBI
|
|
18
|
Barton A: Handbook for good clinical
research practice (GCP): Guidance forsimplementation. J Epidemiol
Community Health. 61:5592007. View Article : Google Scholar
|
|
19
|
Fillies T, Woltering M, Brandt B, Van
Diest JP, Werkmeister R, Joos U and Buerger H: Cell cycle
regulating proteins p21 and p27 in prognosis of oral squamous cell
carcinomas. Oncol Rep. 17:355–359. 2007.PubMed/NCBI
|
|
20
|
Fillies T, Werkmeister R, van Diest PJ,
Brandt B, Joos U and Buerger H: HIF1-alpha overexpression indicates
a good prognosis in early stage squamous cell carcinomas of the
oral floor. BMC Cancer. 5:842005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fillies T, Buerger H, Gaertner C, August
C, Brandt B, Joos U and Werkmeister R: Catenin expression in T1/2
carcinomas of the floor of the mouth. Int J Oral Maxillofac Surg.
34:907–911. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sobin LH, Gospodarowicz MK and Wittekind
C: UICC TNM Classification of Malignant Tumours (7th).
Wiley-Blackwell. Hoboken, NJ: 2009.
|
|
23
|
Packeisen J, Buerger H, Krech R and
Boecker W: Tissue microarrays: A new approach for quality control
in immunohistochemistry. J Clin Pathol. 55:613–615. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schymik B, Buerger H, Krämer A, Voss U,
van der Groep P, Meinerz W, van Diest PJ and Korsching E: Is there
‘progression through grade’ in ductal invasive breast cancer?
Breast Cancer Res Treat. 135:693–703. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Helms MW, Packeisen J, August C, Schittek
B, Boecker W, Brandt BH and Buerger H: First evidence supporting a
potential role for the BMP/SMAD pathway in the progression of
oestrogen receptor-positive breast cancer. J Pathol. 206:366–376.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Packeisen J, Korsching E, Herbst H,
Boecker W and Buerger H: Demystified…tissue microarray technology.
Mol Pathol. 56:198–204. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Botstein D and Fink GR: Yeast: An
experimental organism for 21st Century biology. Genetics.
189:695–704. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Vidal M, Cusick ME and Barabási AL:
Interactome networks and human disease. Cell. 144:986–998. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Buerger H, Boecker F, Packeisen J,
Agelopoulos K, Poos K, Nadler W and Korsching E: Analyzing the
basic principles of tissue microarray data measuring the
cooperative phenomena of marker proteins in invasive breast cancer.
Open Access Bioinformatics. 5:1–21. 2013.
|
|
30
|
Warnakulasuriya S: Global epidemiology of
oral and oropharyngeal cancer. Oral Oncol. 45:309–316. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Petti S: Lifestyle risk factors for oral
cancer. Oral Oncol. 45:340–350. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Moergel M, Kammerer P, Kasaj A, Armouti E,
Alshihri A, Weyer V and Al-Nawas B: Chronic periodontitis and its
possible association with oral squamous cell carcinoma - a
retrospective case control study. Head Face Med. 9:392013.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Feller L, Wood NH, Khammissa RA and Lemmer
J: Human papillomavirus-mediated carcinogenesis and HPV-associated
oral and oropharyngeal squamous cell carcinoma. Part 1: Human
papillomavirus-mediated carcinogenesis. Head Face Med. 6:142010.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Feller L, Wood NH, Khammissa RA and Lemmer
J: Human papillomavirus-mediated carcinogenesis and HPV-associated
oral and oropharyngeal squamous cell carcinoma. Part 2: Human
papillomavirus associated oral and oropharyngeal squamous cell
carcinoma. Head Face Med. 6:152010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
AWMF and GAOOAM: Surgery Guidelines for
Oncology, S3: Guideline for diagnostics and treatment of oral
cancer. AWMF-Register-Number (007–100O, 2012L). 119:2012.(In
German).
|
|
36
|
Frerich B: Standard therapy of oral
squamous epithelial carcinoma. Onkologe. 16:527–536. 2010.(In
German). View Article : Google Scholar
|
|
37
|
Institut RK and GEKID: Cancer in Germany
2007/2008. Journal. 137:2012.(In German).
|
|
38
|
Steinert PM, Idler WW and Zimmerman SB:
Self-assembly of bovine epidermal keratin filaments in vitro. J Mol
Biol. 108:547–567. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Romano V, Bosco P, Rocchi M, Costa G,
Leube RE, Franke WW and Romeo G: Chromosomal assignments of human
type I and type II cytokeratin genes to different chromosomes.
Cytogenet Cell Genet. 48:148–151. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Thiel UJ, Feltens R, Adryan B, Gieringer
R, Brochhausen C, Schuon R, Fillies T, Grus F, Mann WJ and Brieger
J: Analysis of differentially expressed proteins in oral squamous
cell carcinoma by MALDI-TOF MS. J Oral Pathol Med. 40:369–379.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhong LP, Chen WT, Zhang CP and Zhang ZY:
Increased CK19 expression correlated with pathologic
differentiation grade and prognosis in oral squamous cell carcinoma
patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
104:377–384. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Korsching E, Packeisen J, Agelopoulos K,
Eisenacher M, Voss R, Isola J, van Diest PJ, Brandt B, Boecker W
and Buerger H: Cytogenetic alterations and cytokeratin expression
patterns in breast cancer: Integrating a new model of breast
differentiation into cytogenetic pathways of breast carcinogenesis.
Lab Invest. 82:1525–1533. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Korsching E, Jeffrey SS, Meinerz W, Decker
T, Boecker W and Buerger H: Basal carcinoma of the breast
revisited: An old entity with new interpretations. J Clin Pathol.
61:553–560. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Schiffman M, Castle PE, Jeronimo J,
Rodriguez AC and Wacholder S: Human papillomavirus and cervical
cancer. Lancet. 370:890–907. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kurman RJ and Shih Ie M: Molecular
pathogenesis and extraovarian origin of epithelial ovarian
cancer-shifting the paradigm. Hum Pathol. 42:918–931. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Rajagopalan H, Nowak MA, Vogelstein B and
Lengauer C: The significance of unstable chromosomes in colorectal
cancer. Nat Rev Cancer. 3:695–701. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Lee BH, Roh S, Kim YI, Lee A and Kim SY:
Difference of genome-wide copy number alterations between
high-grade squamous intraepithelial lesions and squamous cell
carcinomas of the uterine cervix. Korean J Pathol. 46:123–130.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Tornesello ML, Buonaguro L, Giorgi-Rossi P
and Buonaguro FM: Viral and cellular biomarkers in the diagnosis of
cervical intraepithelial neoplasia and cancer. Biomed Res Int.
2013:5196192013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Helms JA, Cordero D and Tapadia MD: New
insights into craniofacial morphogenesis. Development. 132:851–861.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Diewert VM: Development of human
craniofacial morphology during the late embryonic and early fetal
periods. Am J Orthod. 88:64–76. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Moore KL and Persuad TVN: The Developing
Human: Clinicall Oriented Embryology (8th). Saunders/Elsevier.
Philadelphia, PA: 2007.
|
|
52
|
Löfdahl HE, Du J, Näsman A, Andersson E,
Rubio CA, Lu Y, Ramqvist T, Dalianis T, Lagergren J and Dahlstrand
H: Prevalence of human papillomavirus (HPV) in oesophageal squamous
cell carcinoma in relation to anatomical site of the tumour. PLoS
One. 7:e465382012. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Li R, Koch WM, Fakhry C and Gourin CG:
Distinct epidemiologic characteristics of oral tongue cancer
patients. Otolaryngol Head Neck Surg. 148:792–796. 2013. View Article : Google Scholar : PubMed/NCBI
|