Introduction
In 2012, 952,000 new cases of gastric cancer were
registered, making the disease the fourth most common cancer in the
world (1). Gastric cancer was the
third leading cause of mortality due to malignant neoplasms
(723,000 cases). The treatment results for this cancer remain
disappointing. The 5-year survival rate ranges from 10 to 30%
across Europe (2). Since the
publication of the results of the INT 0116 study, post-operative
chemoradiotherapy has become the standard of care in a number of
cancer centers around the world (3).
Ongoing studies are focused on improving the efficacy of the local
treatment of gastric cancer. One promising direction of this
research is the use of pre-operative radiotherapy or
chemoradiotherapy (4–10). Neoadjuvant therapy reduces the
incidence of unresectable cases, increases the proportion of R0
resections and reduces the risk of local recurrence (5,7,11).
Initially, radiation therapy was based on the schema
of two opposing fields, but treatment has gradually evolved towards
multi-field techniques (9).
Currently, radiotherapy offers the possibility of using radiation
in the treatment of gastric cancer through non-coplanar, dynamic or
rotating techniques, which make it possible to better protect
organs at risk and potentially reduce the risk of radiation-induced
reactions while retaining high conformity of the treatment plan
(12). Over the last few years, the
use of intensity-modulated radiation therapy (IMRT) has been
increasing rapidly. There have been few publications on the
technical aspects of pre-operative radiotherapy (13,14). At
the Institute of Oncology, Gliwice Branch (Gliwice, Poland),
pre-operative radiotherapy has been the subject of intense clinical
research over the past 10 years.
The aim of the present study was to compare the
plans created using the three-dimensional conformal radiation
therapy (3DCRT) and dynamic IMRT techniques to assess the
possibility of better protection of organs at risk and healthy
tissues in patients with gastric cancer treated with pre-operative
chemoradiotherapy.
Patients and methods
The present study received approval from the Ethics
Committee of the Maria Sklodowska-Curie Memorial Cancer Center and
Institute of Oncology, Gliwice Branch (KB/493-59/09). The study
group consisted of 25 patients (19 male, 6 female; average age, 69
years) with gastric cancer [adenocarcinoma T1-T4, N0-N3 and
GI-GIII, according to AJCC (15)],
who were treated at the Institute of Oncology, Gliwice Branch,
between January 2006 and December 2011. All patients were
administered neoadjuvant chemoradiotherapy. The total dose was 45
Gray (Gy) administered over five weeks (1.8 Gy per fraction).
During chemotherapy, 325 mg/m2 5-fluorouracil (days 1–5)
was applied.
Treatment and planning
Treatment planning was based on computed tomography
(CT) scanning in the therapeutic position (supine, with the hands
raised above the head) in a thermoplastic stabilizer (Somatom
Definition Edge, Siemens AG, Munich, Germany). CT scanning was
performed with contrast (uropolin) in 3-mm steps. Each patient
drank 500 ml of water to fill the stomach, thus enhancing tumor
visibility. Gross tumor volume (GTV) indicates a tumor that is
visible on the CT scans. Area of clinical target volume (CTV)
included a gastric tumor along with 5-cm margins (usually the
stomach) and the regional lymph nodes: Perigastric, celiac trunk,
splenic, pancreatic-duodenal, supra-pancreatic, portal vein and
para-aortic (16). Planning target
volume (PTV) was determined by adding a 1-cm margin around the CTV.
On each 3DCT, the following critical organs were traced: Liver,
left and right kidney, pancreas, spinal canal, intestine and
spleen. All patients were treated using IMRT plans, and the 3DCRT
plans have been added for comparison.
The planned total pre-operative radiotherapy dose in
the patients with gastric cancer was 45 Gy in 25 fractions.
The treatment plans for each patient were developed
on the Eclipse treatment planning system (version 10.0; Varian
Medical Systems UK Ltd., Crawley, UK). Plans were created using the
2-field technique, the multi-field (three- and four-field)
technique and the IMRT technique. Treatment plans met the criteria
recommended in Reports 50 and 62 by the International Commission on
Radiation Units and Measurements (ICRU; www.icru.org), determining the level of the minimum
dose to the PTV of 95% and a maximum dose not exceeding 107%.
Assumptions and parameters
Plans were compiled with the following assumptions
for the protection of the organs at risk: Less than 30% of the
liver volume received 30 Gy isodose (V30 of 30%); less
than 30% of the kidney volume received 20 Gy isodose
(V20 of 30%); and for the spinal canal, a maximum dose
of <50 Gy. A significant portion of the pancreas and spleen were
always within the area of the PTV.
The treatment plans were approved based on a
dose-volume histogram (DVH) analysis using the following determined
parameters: The minimum, mean, modal, median and maximum doses in
the GTV, CTV and PTV; the maximum, mean and median doses of the
spinal canal; the maximum, medium, modal and median doses of the
liver, the kidneys, the pancreas and the spleen; and the total
volume for the kidney.
In addition, the defined volumes of the
aforementioned organs were exposed to 10, 15, 20 and 30-Gy dose
ranges and were analyzed for each of the techniques.
Analysis
The V10 to V100 values for the
critical organs with respect to the planned radiation dose were
also analyzed. The established values for normal tissue dose were
based on the healthy tissue overdosage factor (HTOF) of Salt
(12,16–18). The
conformity index (CI) and the homogeneity index (HI) values for the
target volume were calculated according to the following formulae
(13,17,19–21): i)
CIRTOG = VRI / TV; where the volume of the
reference isodose (VRI) is the volume of the PTV
receiving a 95% reference/planned dose, and the target volume (TV)
is the volume of the PTV. ii) HI = Imax / RI; where
Imax is the maximum dose to the target, and RI is the
reference dose in the PTV. iii) HTOF = HTVRI / TV; where
healthy tissue volume covered by the reference isodose
(HTVRI) is the tissue/organ volume that received the
planned dose to the PTV.
The level of significance of the results for the
individual statistical analysis techniques were based on Friedman's
rank analysis of variance (P<0.001). All the statistical
computations were performed using Statistica software, version 10
(StatSoft, Inc., Tulsa, OK, USA).
Results
Target volumes
The average minimum dose in the PTV for each
technique was as follows: 42.71 Gy (2-field), 42.94 Gy (3-field),
43.33 Gy (4-field) and 42.45 Gy (IMRT). The detailed results are
shown in Table I. The average minimum
doses in the PTV were compared between each technique with the
following P-values: 2 vs. 3 fields, P=0.014; 2 vs. 4 fields,
P=0.001; 2 fields vs. IMRT, P=0.270; 3 vs. 4 fields, P=0.006; 3
fields vs. IMRT, P=0.058; and 4 fields vs. IMRT, P=0.001. Only the
4-field technique showed a significant difference in the minimum
dose in the PTV compared with the IMRT technique (P=0.001).
 | Table I.Parameters of the absorbed dose (Gy)
in the planning target volume for three-dimensional conformal
radiotherapy and IMRT. |
Table I.
Parameters of the absorbed dose (Gy)
in the planning target volume for three-dimensional conformal
radiotherapy and IMRT.
| Technique | Median Dmin
(range)a | Median Dmax
(range)b | Median Dmean
(range)c | Median Dmod
(range)d | Median Dmed
(range)e |
|---|
| 2-field | 42.7 (40.5–44) | 50.3 (46.6–53.9) | 46.8 (45.1–49.1) | 46.5 (45.2–48.2) | 46.8 (45.1–49) |
| 3-field | 42.9 (40.5–44.5) | 50.3 (46.1–55.9) | 46.9 (45.1–50) | 46.4 (45–49.2) | 46.8 (45.1–49.7) |
| 4-field | 43.3 (42.7–44.8) | 49.0 (46.2–50.7) | 46.2 (45–47.6) | 46.0 (44.2–47) | 46.1 (45.1–47.5) |
| IMRT | 42.5 (38.4–44.1) | 48.9 (47.3–52.4) | 45.9 (44.5–47.2) | 45.9 (44.1–47.3) | 45.9 (44.5–47.3) |
The average maximum dose values in the PTV for 2
fields, 3 fields, 4 fields and IMRT were 50.3, 50.3, 49.3 and 48.9
Gy, respectively. The location of the maximum dose (Dmax) was
tested and compared with the Dmax value for the PTV, external
contours and critical organs. The results are shown in Table II.
| Table II.Maximum dose (Gy) in the organs at
risk for three-dimensional conformal radiotherapy and IMRT. |
Table II.
Maximum dose (Gy) in the organs at
risk for three-dimensional conformal radiotherapy and IMRT.
| Technique | Spinal canal | Liver | Left kidney | Right kidney | Pancreas | Spleen | External |
|---|
| 2-field | 47.71 | 49.89 | 45.73 | 45.78 | 48.12 | 48.21 | 50.99 |
|
| (45.6–52) | (47.1–53.1) | (27.6–50.8) | (35.3–49) | (46–51.4) | (45.9–51.8) | (47.1–55.5) |
| 3-field | 43.82 | 49.46 | 45.52 | 44.82 | 48.44 | 49.99 | 50.64 |
|
| (14.7–48.6) | (46.4–53.6) | (24.8–50.3) | (29.9–48) | (45.7–54.6) | (46–58) | (46.4–58) |
| 4-field | 38.57 | 48.33 | 45.63 | 44.50 | 47.17 | 47.67 | 49.49 |
|
| (26.2–46.6) | (46.2–51.1) | (40.5–47.8) | (25.5–56.2) | (45.6–49.2) | (45.9–49.9) | (46.4–58) |
| IMRT | 41.26 | 47.68 | 42.42 | 40.56 | 47.63 | 48.10 | 49.99 |
|
| (34.5–50.3) | (45.2–50.7) | (22.5–49.1) | (28.3–47.4) | (44.8–49.9) | (45.9–51.7) | (47.1–571) |
In the 2-field techniques and IMRT, the maximum dose
to the PTV was comparable to the maximum dose over the entire
volume of the body. This indicates the location of the hot spots in
the PTV. However, in the case of the 2-field technique, the maximum
dose was reported in the critical organs, which was a vast area
that received a high dose.
Conformity and heterogeneity
index
The following results were obtained in the CI for
the PTV: 0.949 for the 2-field technique, 0.954 for the 3-field
technique, 0.962 for the 4-field technique and 0.943 for IMRT
(P<0.001). The CI for the CTV amounted to 0.957, 0.961, 0.969
and 0.955 (P<0.001), and the CI for the GTV amounted to 0.988,
0.992, 0.985 and 0. 983 (P<0.001).
In examining the ratio of HI for the PTV, the
following results were obtained: 1.118 for the 2-field technique,
1.117 for the 3-field technique, 1.089 for the 4-field technique
and 1.087 for IMRT (P<0.001). The CI for the CTV amounted to
1.115, 1.118, 1.088 and 1.082 (P<0.001), and the CI for the GTV
amounted to 1.085, 1.087, 1.066 and 1.063 (P<0.001).
Analogously, the average dose values for the CTV were determined
relative to the PTV volume. The results are shown in Table III.
| Table III.Average dose values (Gy) in the
clinical target volume. |
Table III.
Average dose values (Gy) in the
clinical target volume.
| Technique | Median Dmin
(range)a | Median Dmax
(range)b | Median Dmean
(range)c | Median Dmod
(range)d | Median Dmed
(range)e |
|---|
| 2-field | 43.0
(41.1–44.7) | 50.2
(46.5–53.8) | 46.8
(45.1–49.2) | 46.5
(45.2–48.2) | 46.0
(45.1–49.1) |
| 3-field | 43.3
(41.2–44.6) | 50.3
(46.1–55.9) | 46.9 (45–50.1) | 46.6 (45–50.1) | 46.9 (45–49.4) |
| 4-field | 43.6
(42.5–44.9) | 49.0
(46.1–50.5) | 46.2 (45–47.6) | 45.9 (44.2–47) | 46.1
(45.1–47.5) |
| IMRT | 43.0 (41–44.1) | 48.7
(46.3–52.4) | 46.0
(44.5–47.2) | 45.9
(44.2–47.3) | 46.0
(44.5–47.3) |
The CI indices for the studied techniques for the
average of the minimum dose in the GTV, CTV and PTV were
essentially ranked at the same level. The interpretation of the
minimum dose distribution in the target volume should be based on
all plans for a highly satisfactory result in the tested range.
Analysis of the coefficient of HI describing the dose homogeneity
indicates a clear difference in the assessment of the 3DCRT and
IMRT plans. While the best uniformity of the dose distribution was
observed with the dynamic techniques (1.08), the HI indices for the
two- and three-field techniques (1.12) were relatively high,
although they did not exceed the maximum dose of the tolerable
minimum dose level. The high toxicity of the combined treatment for
post-operative gastric cancer should be carefully considered; it
partially covered the PTV, but also affected healthy tissue and
critical organs. Minimizing the hot spots in the target areas and
hence producing better uniformity while reducing the total dose to
the critical organs should ensure less toxic radiation.
HTOF assumes values from 0 to 0.5. Values close to
0.5 indicate a high dose to the study volume, whereas values closer
to 0 indicate that the study volume is less vulnerable. Table IV show HTOF values for the organs at
risk.
| Table IV.Mean healthy tissue overdosage factor
values for the organs at risk for three-dimensional conformal
radiotherapy and IMRT. |
Table IV.
Mean healthy tissue overdosage factor
values for the organs at risk for three-dimensional conformal
radiotherapy and IMRT.
| Technique | Spinal canal | Liver | Pancreas | Spleen | Left kidney | Right kidney |
|---|
| 2-field | 0.27 | 0.13 | 0.46 | 0.41 | 0.22 | 0.10 |
| 3-field | 0.22 | 0.17 | 0.46 | 0.40 | 0.19 | 0.12 |
| 4-field | 0.18 | 0.23 | 0.45 | 0.39 | 0.18 | 0.09 |
| IMRT | 0.17 | 0.17 | 0.45 | 0.36 | 0.12 | 0.07 |
Spinal canal
The criterion for the maximum dose to the spinal
canal of <45 Gy was not fulfilled in the 2-field plans (47.7
Gy); in the other techniques, the average maximum dose was <44
Gy.
Liver
The criterion for the protection of the liver was a
V30 of 30%. This value was obtained for 64% of the plans
for the 2-field technique, 68% of the plans for the 3-field
technique, 52% of the plans for the 4-field technique and 80% of
the plans for IMRT. The average dose was fulfilled only for the
2-field and IMRT plans, reaching 27.1 Gy and 24.8 Gy, respectively.
In other multi-field techniques, a 30-Gy dose was administered to
higher than 30% of the liver volume (Table V).
| Table V.Liver volume (%) values in
association with dose (Gy) (P<0.001). |
Table V.
Liver volume (%) values in
association with dose (Gy) (P<0.001).
| Technique | 10 Gy | 15 Gy | 20 Gy | 30 Gy |
|---|
| 2-field | 39.2 (19–79) | 35.8 (17–69) | 32.2 (16–56) | 27.1 (13–49) |
| 3-field | 53.0 (20–90) | 39.8 (18–80) | 35.7 (17–76) | 31.0 (15–68) |
| 4-field | 82.0 (63–96) | 68.6 (20–95) | 58.7 (17–92) | 32.9 (16–61) |
| IMRT | 65.1 (22–90) | 53.8 (17–88) | 42.4 (14–81) | 24.8 (11–40) |
Pancreas and spleen
In the case of the spleen and pancreas, there are no
guidelines for their protection during radiotherapy for stomach
cancer (Tables VI and VII).
| Table VI.Association between irradiated volume
of the pancreas (%) and absorbed dose (Gy) for three-dimensional
conformal radiotherapy and IMRT (P<0.39–0.86). |
Table VI.
Association between irradiated volume
of the pancreas (%) and absorbed dose (Gy) for three-dimensional
conformal radiotherapy and IMRT (P<0.39–0.86).
| Technique | 10 Gy | 15 Gy | 20 Gy | 30 Gy |
|---|
| 2-field |
100.0 |
99.9 | 99.8 | 99.7 |
| 3-field | 99.9 |
99.8 | 99.8 | 99.7 |
| 4-field |
100.0 | 100.0 | 99.8 | 99.4 |
| IMRT |
100.0 |
99.9 | 99.9 | 99.6 |
| Table VII.Association between irradiated volume
of the spleen (%) and absorbed dose (Gy) for three-dimensional
conformal radiotherapy and IMRT (P=0.02). |
Table VII.
Association between irradiated volume
of the spleen (%) and absorbed dose (Gy) for three-dimensional
conformal radiotherapy and IMRT (P=0.02).
| Technique | 10 Gy | 15 Gy | 20 Gy | 30 Gy |
|---|
| 2-field | 96.6 (53–100) | 95.3 (48–100) | 93.8 (42–100) | 90.5 (34–100) |
| 3-field | 97.7 (67–100) | 96.4 (63–100) | 94.9 (58–100) | 90.5 (48–100) |
| 4-field | 97.7 (66–100) | 96.7 (60–100) | 94.8 (55–100) | 87.4 (39–100) |
| IMRT | 95.9 (48–100) | 93.9 (40–100) | 91.1 (32–100) | 83.0 (15–100) |
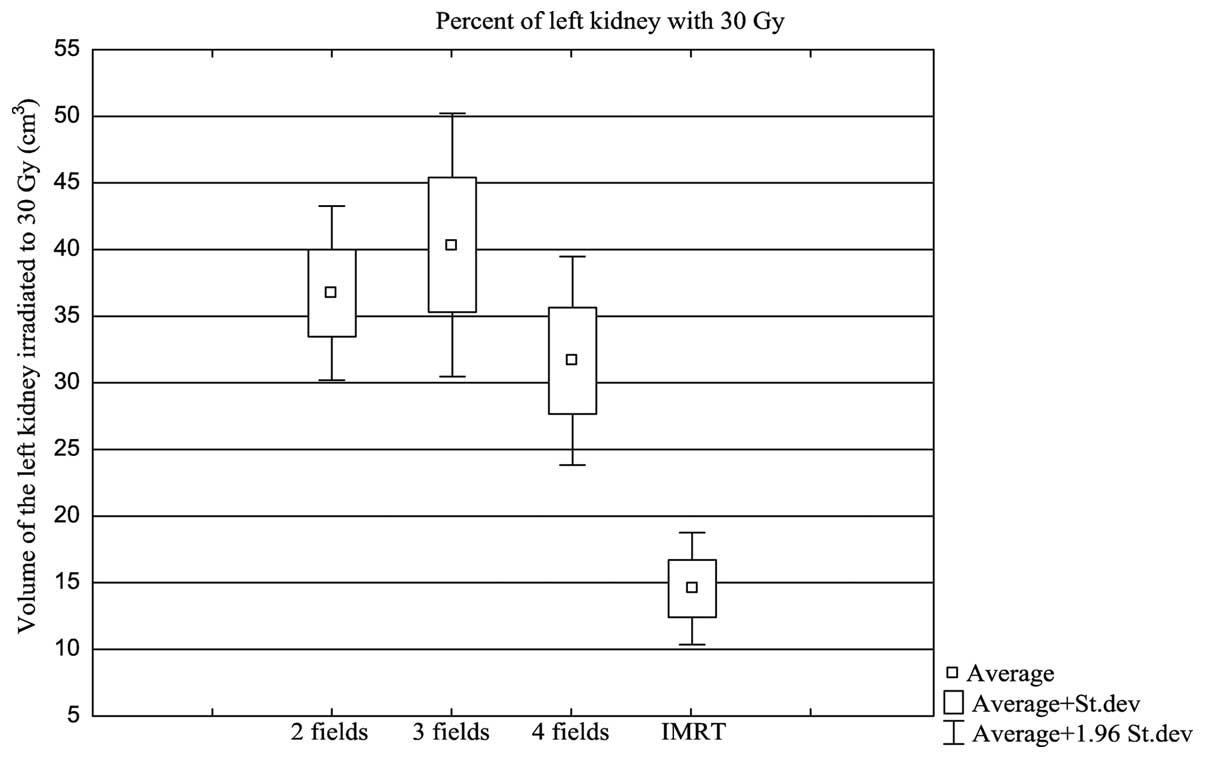
Right and left kidney
The criterion for the protection of the kidneys was
a V20 of 30%, and it was met in the case of the right
kidney. For the left kidney, only the IMRT plans allowed a dose of
<20 Gy in 30% of its volume to be obtained. For the left kidney,
this value was obtained for 24% of the plans for the 2-field
technique, 24% of the plans for the 3-field technique, 28% of the
plans for the 4-field technique and 64% of the plans for IMRT
(P=0.030). In the patients treated with the 3DCRT technique, in
which it was not possible to obtain a predetermined criterion
dose/volume for each kidney, the method of summing up the volume of
the two kidneys was used, and the DVH evaluation was performed for
the acceptance of the treatment plan in accordance with a
predetermined criterion. Table
VIII shows the association between the volumes of the right and
left kidneys and the dose levels of 10, 15, 20 and 30 Gy
(P<0.001).
| Table VIII.Asocation between irradiated volume
of the right and left kidney and absorbed dose for
three-dimensional conformal radiotherapy and IMRT. |
Table VIII.
Asocation between irradiated volume
of the right and left kidney and absorbed dose for
three-dimensional conformal radiotherapy and IMRT.
| Technique | 10 Gy | 15 Gy | 20 Gy | 30 Gy |
|---|
| Right kidney |
|
|
2-field | 33.8 (4–71) | 28.2 (3–65) | 24.0 (2–58) | 18.5 (0–49) |
|
3-field | 41.4 (4–90) | 30.5 (2–71) | 25.5 (1–69) | 18.6 (0–58) |
|
4-field | 36.1 (2–73) | 26.3 (1–53) | 21.0 (0–42) | 11.8 (0–31) |
|
IMRT | 27.5 (2–67) | 18.5 (1–53) | 11.9 (0–27) | 4.6
(0–17) |
| Left kidney |
|
|
2-field | 46.7 (7–90) | 43.3 (2–79) | 40.8 (1–75) | 36.5 (0–61) |
|
3-field | 56.7 (2–99) | 51.5 (1–100) | 47.6 (0–100) | 40.4 (0–100) |
|
4-field | 62.0 (15–100) | 54.7 (10–100) | 49.4 (1–100) | 31.6 (0–91) |
|
IMRT | 47.4 (3–100) | 36.4 (2–98) | 26.9 (0.5–85) | 14.5 (0–41) |
The most interesting result in the protection of
critical organs, was observed in the left kidney, which is an organ
that is located in the immediate vicinity of the PTV and was
exposed to a high dose of radiation during the radiotherapy for
stomach cancer (Fig. 1).
Discussion
Comparisons between conformal treatment planning and
IMRT are challenging due to different methods of prescription and
reporting of the absorbed doses. ICRU Report 50 used a
dose-at-a-point prescription for 3DCRT. By contrast, ICRU Report 83
did not favor a particular point, but favored the volume. This
method of treatment planning is based on a dose-volume
prescription. ICRU Report 83 changed the methods of dose reporting.
This report recommended the near-minimum (D98%) and near-maximum
(D2%) values instead of the previously recommended doses. In Report
50, the absorbed dose in the PTV, by definition, ranged from
95–107% of the prescribed absorbed dose. In the present study, a
local minimum is accepted, and in this way, an absorbed dose is not
dependent on a single computation point. D50% is considered to best
correspond to the previously defined dose at the ICRU reference
point. The new recommendations emphasize the value of homogeneity
and conformity indexes.
The CI for the studied techniques for the average of
the minimum dose was ranked practically at the same level for the
GTV, CTV and PTV structures. The interpretation of the minimum dose
distribution in the target should consider all plans for a highly
satisfactory result in the tested range. Analysis of the
coefficient of HI describing the dose homogeneity in the test
structure shows a clear difference in the assessment of the 3DCRT
and IMRT plans. While the best uniformity of the dose distribution
is observed with the dynamic techniques (1.08), the HI indices for
the 2- and 3-field techniques (1.17) showed a relatively high
maximum dose, although the minimum dose level was tolerable. There
is a relatively high toxicity of the combined treatment for gastric
cancer, where the healthy tissue and the critical organs are
covered by the PTV. Minimizing the maximum dose to the target
volumes, and, hence, achieving better uniformity should ensure less
radiation therapy toxicity.
The greatest differences were observed in the case
of the spinal canal and the two kidneys. Relatively low HTOF factor
values are associated with the dynamic techniques.
In addition, the occurrence of the largest dose
gradient over the external volume also refers to the IMRT
techniques. It appears that pre-operative/post-operative
radiotherapy should focus on techniques that are currently highly
specialized, such as the dynamic techniques, but also the rotary
techniques, for example, RapidArc.
A review of the available studies on 3DCRT for
gastric cancer published by Morganti et al (22) clearly indicated that conformal
techniques do not achieve optimal treatment plans (23). It is more appropriate to focus
attention on the possibilities offered by advanced dynamic or
rotating techniques. In 2004, Wieland et al described the
first attempts to assess the rotational techniques comparing the
coverage of large areas of PTV that were planned with IMRT and
RapidArc techniques (24). The first
report on the results of a comparison of the dynamic techniques
(IMRT) and conformal radiotherapy for post-operative gastric cancer
was published by Minn et al in 2010 (25). Over a 2-year period, the studied group
included 57 patients who were treated with combined
chemoradiotherapy. Site treatment success and treatment toxicity
were evaluated, and the study concluded that IMRT, in terms of
toxicity, is comparable to conformal techniques (61.2 vs. 61.5%).
The data regarding the critical organs, such as the liver and the
kidneys, were presented based on the dose averages. It was
concluded that the IMRT techniques better protect the liver and
kidneys. However, there is no indication of the maximum dose level
of radiation in the entire volume, which results in high doses to a
volume of the intestines and may increase the toxicity of
radiation, regardless of the type of radiation therapy used
(25). The most recent publication
that compared irradiation techniques in patients with gastric
cancer was that by Ma et al in 2013; the plans created for
15 patients involving 5- and 7-field IMRT and 3DCRT techniques were
evaluated (26). The study assessed
the volume of the PTV indices based on CI and HI analysis, as in
the present study. The results in terms of dose uniformity in the
target area indicated that IMRT was better than conformal
techniques. The number of fields ranged from 4 to 8, and the most
commonly used was the 5-field technique. The use of the 5-field
IMRT techniques did not improve the degradation in the kidney,
although at high doses for the liver and spinal canal, IMRT was
clearly shown to be a safer technique.
Overall, the use of conformity and homogeneity
indices for the evaluation of target volumes indicate that the
dynamic techniques provide good GTV, CTV and PTV coverage of high
and uniform dose areas during radiotherapy for gastric cancer.
Clearly improved protection of organs at risk is ensured with the
IMRT technique compared with the conformal techniques. Dynamic
techniques should replace the multi-field conformal techniques for
gastric cancer radiotherapy, mainly due to the far superior
protection of organs at risk. It is, however, also the amount and
location of the maximum dose of dynamic plans that should improve
treatment tolerance.
Acknowledgements
The original manuscript was edited by Managing
Editor-American Journal Experts (www.aje.com).
References
|
1
|
International Agency for Research on
Cancer, World Health Organization: Globocan 2012: Estimated cancer
incidence, mortality and prevalence worldwide in 2012. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspxAccessed.
August 09–2014
|
|
2
|
Sant M, Allemani C, Santaquilani M, Knijn
A, Marchesi F and Capocaccia R: EUROCARE Working Group: EUROCARE-4.
Survival of cancer patients diagnosed in 1995–1999. Reslts and
commentary. Eur J Cancer. 45:931–991. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Macdonald JS, Smalley SR, Benedetti J,
Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA,
Gunderson LL, Jessup JM and Martenson JA: Chemoradiotherapy after
surgery compared with surgery alone for adenocarcinoma of the
stomach or gastroesophageal junction. N Engl J Med. 345:725–730.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
NCCN: Practice Guidelines in Oncology
version 2. 2010.https://www.nccn.org/professionals/physician_gls/f_guidelines.aspAccessed.
December 11–2012
|
|
5
|
Zhang ZX, Gu XZ, Yin WB, Huang GJ, Zhang
DW and Zhang RG: Randomized clinical trial on the combination of
preoperative irradiation and surgery in the treatment of
adenocarcinoma of gastric cardia (ACG)-report on 370 patients. Int
J Radiat Oncol Biol Phys. 42:929–934. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sindelar WG and Kinsella TJ: Randomized
trial of resection and intraoperative radiotherapy in locally
advanced gastric cancer. Proc Ann Meet Am Soc Clin Oncol.
6:A3571987.
|
|
7
|
Ito H, Clancy TE, Osteen RT, Swanson RS,
Bueno R, Sugarbaker DJ, Ashley SW, Zinner MJ and Whang EE:
Adenocarcinoma of the gastric cardia: What is optimal surgical
approach? J Am Coll Surg. 199:880–886. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ajani JA, Mansfield PF, Janjan N, Morris
J, Pisters PW, Lynch PM, Feig B, Myerson R, Nivers R, Cohen DS and
Gunderson LL: Multi-institutional trial of preoperative
chemoradiotherapy in patients with potentially resectable gastric
carcinoma. J Clin Oncol. 22:2774–2780. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Allal AS, Zwahlen D, Bründler MA, de Peyer
R, Morel P, Huber O and Roth AD: Neoadjuvant radiochemotherapy for
locally advanced gastric cancer: Long-term results of a phase I
trial. Int J Radiat Oncol Biol Phys. 63:1286–1289. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wydmański J, Suwinski R, Poltorak S, Maka
B, Miszczyk L, Wolny E, Bielaczyc G and Zajusz A: The tolerance and
efficacy of preoperative chemoradiotherapy followed by gastrectomy
in operable gastric cancer, a phase II study. Radiother Oncol.
82:132–136. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hallissey MT, Dunn JA, Ward LC and Allum
WH: The second British stomach cancer group trial of adjuvant
radiotherapy or chemotherapy in respectable gastric cancer: Five
year follow-up. Lancet. 343:1309–1312. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Huchet A, Caudry M, Belkacémi Y, Trouette
R, Vendrely V, Causse N, Récaldini L, Atlan D and Maire JP:
Volume-effect and radiotherapy [II] part II: Volume-effect and
normal tissue. Cancer Radiother. 7:353–362. 2003.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Soyfer V, Corn BW, Melamud A, Alani S,
Tempelhof H, Agai R, Shmueli A, Figer A and Kovner F:
Three-Dimensional non-coplanar conformal radiotherapy yields better
results than traditional beam arrangements for adjuvant treatment
of gastric cancer. Int J Radiat Oncol Biol Phys. 69:364–369. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Matzinger O, Gerber E, Bernstein Z,
Maingon P, Haustermans K, Bosset JF, Gulyban A, Poortmans P,
Collette L and Kuten A: EORTC-ROG expert opinion: Radiotherapy
volume and treatment guidelines for neoadjuvant radiation of
adenocarcinomas of the gastroesophageal junction and the stomach.
Radiother Oncol. 92:164–175. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Edge BD, Compton CC, Fritz AG, Greene FL
and Trotti A: AJCC Cancer Staging Manual (7th). Springer-Verlag.
New York, NY: 2010.
|
|
16
|
Wydmański J and Mohanti BK: An appraisal
of radiation therapy techniques for adjuvant and neoadjuvant
therapy in gastric cancer. J Radiother Pract. 7:67–75. 2008.
View Article : Google Scholar
|
|
17
|
Feuvret L, Noël G, Mazeron JJ and Bey P:
Conformity index: A review. Int J Radiat Oncol Biol Phys.
64:333–342. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lomax NJ and Scheib SG: Quantifying the
degree of conformity in radiosurgery treatment planning. Int J
Radiat Oncol Biol Phys. 55:1409–1419. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lefkopoulos D, Dejean C, El-Balma H,
Platoni K, Grandjean P, Foulquier J and Schlienger M: Determination
of dose-volumes parameters to characterise the conformity of
stereotactic treatment plans. Proc. of the XIIIth Intern. Conf. on:
Computers in Radiation Therapy (XIIIth ICCR, Heidelberg, Germany).
356–358. 2000.
|
|
20
|
Shaw E, Scott C, Souhami L, Dinapoli R,
Kline R, Loeffler J and Farnan N: Single dose radiosurgical
treatment of recurrent previously irradiated primary brain tumors
and brain metastases: Final report of RTOG protocol 90–05. Int J
Radiat Oncol Biol Phys. 47:291–298. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Stanley J, Breitman K, Dunscombe P,
Spencer DP and Lau H: Evaluation of stereotactic radiosurgery
conformity indices for 170 target volumes in patients with brain
metastases. J Appl Clin Med Phys. 12:34492011.PubMed/NCBI
|
|
22
|
Morganti AG, Di Castelnuovo A, Massaccesi
M, Cellini F, Cilla S, Macchia G, Forte P, Buwenge M, Digesu C,
Ferro M, et al: Planning comparison between standart and conformal
3D techniques in post-operative radiotherapy of gastric cancer: A
systematic review. Br J Radiol. 86:201302742013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Leong T, Willis D, Joon DL, Condron S, Hui
A and Ngan SY: 3D conformal radiotherapy for gastric cancer-results
of a comparative planning study. Radiother Oncol. 74:301–306. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wieland P, Dobler B, Mai S, Hermann B,
Tiefenbacher U, Steil V, Wenz F and Lohr F: IMRT for postoperative
treatment of gastric cancer: Covering large target volumes in the
upper abdomen: A comparison of step-and-shoot and an arc therapy
approach. Int J Radiat Oncol Biol Phys. 59:1236–1244. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Minn AY, Hsu A, La T, Kunz P, Fisher GA,
Ford JM, Norton JA, Visser B, Goodman KA, Koong AC and Chang DT:
Comparison of intensity-modulated radiotherapy and 3-dimensional
conformal radiotherapy as adjuvant therapy for gastric cancer.
Cancer. 116:3943–3952. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ma H, Han J, Zhang T and Ke Y: Comparison
of dosiology between three dimensional conformal and
intensity-modulated radiotherapies (5 and 7 fields) in gastric
cancer post-surgery. J Huazhong Univ Sci Technolog Med Sci.
33:759–764. 2013. View Article : Google Scholar : PubMed/NCBI
|