Introduction
Colorectal cancer (CRC) is a leading cause of
morbidity and mortality worldwide, with >600,000 associated
mortalities annually (1). Of all CRC
cases, 75–80% occur sporadically as the result of complex
interactions between susceptibility genes and environmental factors
(2). Despite the recent and
continuous improvements in diagnosis and treatments, >50% of
colon and rectal tumors metastasize to liver, lung and lymph nodes,
and the 5-year survival rate remains low (~10%) for patients with
metastatic CRC (mCRC) (3). There is,
therefore, an urgent requirement for non-invasive, novel molecular
biomarkers that could be useful in diagnosis and could also improve
prognosis and treatment prediction. The accumulation of in
vitro and in vivo evidence suggests that epigenetics
exerts a fundamental role in CRC pathogenesis (4). The best known and more frequent
epigenetic alteration is DNA methylation, which affects tumor
suppressor genes that may be involved in cell cycle control, DNA
repair, metabolism of carcinogens, cell-cell interaction, apoptosis
and angiogenesis (5).
Hypermethylation of CpG islands in the promoter region of tumor
suppressor genes leads to their inappropriate silencing, which may
trigger cancer initiation and progression (6). The technical advantage of studying DNA
methylation is its chemical stability, thus enabling its detection
with very high sensitivity (≤1:1,000 molecules) (7). Numerous studies have demonstrated that
cancer-specific, methylated DNA may be present in body fluids,
suggesting that it could be used as a non-invasive marker (8,9). Blood,
plasma or serum constitute the most easy-to-handle samples, and are
also a great source of cell-free circulating tumor DNA (10). The mechanism surrounding the origin of
tumoral DNA that is released into the circulation is poorly
understood, but it is assumed that DNA is released during necrosis
and/or apoptosis of tumor cells (11). These circulatory DNA molecules are
easily isolated, and may serve for the detection of the methylation
status of certain genes (12,13). Several genes with altered levels of
methylation have been investigated in respect to their involvement
in CRC initiation or progression. A number of those, including
human mutL homolog 1, O(6)-methylguanine-DNA methyltransferase (MGMT)
and thrombospondin 1, exhibited an increase in methylation during
all the stages of the disease, while other genes such as Ras
association domain family 1 isoform A (RASSF1A) or tissue
inhibitor of metalloproteinase 3 have been reported to be
methylated in later disease stage or in metastases (14).
RASSF members belong to a family of putative tumor
suppressor RAS effectors, for which epigenetic silencing by
promoter methylation has been reported to occur throughout the
progression of several types of cancer, including CRC (15,16). Since
its identification in 2000, the tumor suppressor RASSF1A
gene has been extensively investigated (17). Transcriptional silencing of
RASSF1A by inappropriate promoter methylation has been
frequently observed in various types of human cancer, including
lung, breast, colorectal, gastric and cervical cancer (18). RASSF1A methylation has been
reported to range from 12 to 81% in CRC (19,20). In
colon primary tumors, Yoon et al (19) detected methylation in the CpG island
of the RASSF1A gene in 3 out of 26 (12%) tumor tissues,
while none of the available normal tissues were methylated.
Mutations in the human tumor suppressor gene
adenomatous polyposis coli (APC) are frequent in both
sporadic and familial CRC (21).
Wild-type APC protein contributes to the destabilization and
degradation of β-catenin, which is a central effector molecule in
the Wnt/β-catenin signaling pathway (22). Loss of APC function results in
nuclear accumulation of β-catenin, which leads to the
transcriptional activation (via the β-catenin/T-cell factor
complex) of target genes that may contribute to colorectal
tumorigenesis (23,24). The rate of APC promoter
methylation in CRC and normal colorectal mucosa has been reported
to range from 11 to 62% in different populations, and has been
suggested to moderate the Wnt signaling pathway (25–29).
Furthermore, hypermethylation of the APC promoter has been
demonstrated to be relatively common in other gastrointestinal
neoplasms, including those of the stomach, liver, pancreas and
oesophagus (30).
In the present study, the methylation status of
APC and RASSF1A were investigated in cell-free
circulating DNA of patients with operable CRC (oCRC) and mCRC. The
aim of the present study was to primarily assess the methylation
status of the above genes and to explore their possible prognostic
significance in early and advanced disease.
Materials and methods
Study design
The study material consisted of 155 blood samples
obtained from patients with CRC between March 2010 and May 2014.
Patients were suffering from either early operable (88/155, 56.8%)
or metastatic disease (67/155, 43.2%). The clinicopathological data
for all patients are presented in Table
I. All patients had a performance status (PS) of 0–1 [World
Health Organization scale (31)] and
provided informed consent. Additionally, 20 blood samples obtained
from healthy individuals [friends and non-blood related family
members of patients treated at the Department of Medical Oncology
of the University Hospital of Alexandroupolis (Alexandroupolis,
Greece)] were used as a control group. The majority of controls
were men, all age-matched with the patient population, who had no
received medical care at the time of sample collection. All
patients included in the study had signed an informed consent form
along with an agreement to use biological material for experimental
purposes.
 | Table I.Patients' characteristics in early
(n=88) and advanced (n=67) disease. |
Table I.
Patients' characteristics in early
(n=88) and advanced (n=67) disease.
| Patients'
characteristics | All patients, no.
(%) | Patients with oCRC,
no. (%) | Patients with mCRC,
no. (%) |
|---|
| No. of
patients | 155 | 88 | 67 |
| Gender |
|
|
|
|
Males | 89 (57.4) | 51 (58.0) | 38 (56.7) |
|
Females | 66 (42.6) | 37 (42.0) | 29 (43.3) |
| Age, years |
|
|
|
|
≤70 | 83 (53.5) | 41 (46.6) | 42 (62.7) |
|
>70 | 72 (46.5) | 47 (53.4) | 25 (37.3) |
| Dukes' stage |
|
|
|
|
A+B | 58 (37.4) | 58 (65.9) | – |
| C | 30 (19.4) | 30 (34.1) | – |
| D | 67 (43.2) | – | 67 (100.0) |
|
Differentiation |
|
|
|
|
Well | 48 (31.0) | 30 (34.1) | 18 (26.9) |
|
Moderate | 79 (51.0) | 43 (48.9) | 36 (53.7) |
|
Poor | 28 (18.0) | 15 (17.0) | 13 (19.4) |
| Presence of
metastases |
|
|
|
| No | 88 (56.8) | – | – |
|
Yes | 67 (43.2) | – | – |
| Tumor location,
colon side |
|
|
|
|
Right | 74 (47.7) | 43 (48.9) | 31 (46.3) |
|
Left | 81 (52.3) | 45 (51.1) | 36 (53.7) |
| CEA levels, ng/ml
(n=138) |
|
|
|
|
≤10 | 57 (41.3) | 40 (48.8) | 17 (30.4) |
|
>10 | 81 (58.7) | 42 (51.2) | 39 (69.6) |
| CA 19.9 levels,
U/ml (n=137) |
|
|
|
| <37
(low) | 95 (69.3) | 67 (81.7) | 28 (50.9) |
| >37
(high) | 42 (30.7) | 15 (18.3) | 27 (49.1) |
Sample collection and isolation of
cell-free DNA
Whole blood was extracted from patients
pre-operatively. Blood was collected in serum clot activator tubes.
Serum was obtained immediately through centrifugation at 3,000 × g
for 10 min and stored at −80°C until DNA extraction. Cell-free DNA
from serum samples was isolated using the High Pure Viral Nucleic
Acid kit (Roche Diagnostics GmbH, Mannheim, Germany). A total of
300 µl serum were mixed with 300 µl working solution and 60 µl
proteinase K (18 mg/ml), and incubated for 10 min at 72°C; DNA
isolation was then processed as described in the manufacturer's
protocol. DNA concentration was determined with an ND-100
spectrophotometer (NanoDrop Technologies; Thermo Fisher Scientific,
Inc., Wilmington, DE, USA).
Carcinoembryonic antigen (CEA) and
carbohydrate antigen 19-9 (CA 19-9) measurements
CEA and CA 19-9 levels were measured using the
Elecsys® CEA kit (Roche Diagnostics GmbH). The cut-offs
used were 10 ng/ml for CEA and 37 U/ml for CA 19-9.
Sodium bisulfite conversion
Sodium bisulfite conversion of ≤200 ng cell-free DNA
was performed using the EZ DNA Methylation-Gold™ kit (Zymo Research
Corporation, Irvine, CA, USA), according to the manufacturer's
protocol. The converted DNA was stored at −80°C until used.
Methylation-specific polymerase chain
reaction (MSP)
The methylation status of APC and
RASSF1A in cell-free circulating serum DNA samples was
detected by MSP using specific primer pairs for both the methylated
and unmethylated promoter sequences. Each MSP reaction was
performed in a total volume of 25 µl. Sodium bisulfite-converted
DNA (1 µl) was added into a 24-µl reaction mixture that contained
0.1 µl Taq DNA polymerase (5 U/µl; GoTaq® Hot Start Polymerase;
Promega Corporation, Madison, WI, USA), 5 µl 10X buffer, 2.0 µl
MgCl2 (50 mmol/l), 0.5 µl deoxynucleotides triphosphate (10 mmol/l;
Fermentas; Thermo Fisher Scientific, Inc., Pittsburgh, PA, USA) and
1 µl each of the corresponding forward and reverse primers (10
µmol/l); lastly, distilled H2O was added to a final volume of 25
µl. Sodium bisulfite-treated DNA was amplified in two separate MSP
reactions, one with a set of primers specific for methylated DNA,
and one for unmethylated promoter sequences. The primer pairs used
in this study are as follows: RASSF1A unmethylated, forward
GGTTGTATTTGGTTGGAGTG and reverse CTACAAACCTTTACACACAACA; RASSF1A
methylated, forward GTTGGTATTCGTTGGGCGC and reverse
GCACCACGTATACGTAACG; APC unmethylated, forward
GTGTTTTATTGTGGAGTGTGGGTT and reverse CCAATCAACAAACTCCCAACAA; APC
methylated, forward TATTGCGGAGTGCGGGTC and reverse
TCGACGAACTCCCGACGA. Human placental genomic DNA (gDNA;
Sigma-Aldrich, St. Louis, MO, USA) methylated in vitro with
M.SssI methylase (New England BioLabs, Inc., Ipswich, MA, USA) was
used, following sodium bisulfite conversion, as a fully methylated
(100%) MSP positive control. The same unmethylated placental gDNA
was used, following sodium bisulfite conversion, as a negative MSP
control. The thermocycling conditions used were as follows: i)
APC, 1 cycle at 95°C for 5 min, followed by 39 cycles of
95°C for 45 sec, 63°C for 60 sec and 72°C for 60 sec, with a final
extension cycle of 72°C for 10 min; and ii) RASSF1A, 1 cycle
at 95°C for 5 min, followed by 39 cycles of 95°C for 30 sec, 58°C
for 45 sec and 72°C for 45 sec, with a final extension cycle of
72°C for 5 min. MSP products for methylated and unmethylated
promoters were fractionated on 2% agarose gels containing 40 mM
Tris-acetate/1.0 mM ethylenediaminetetraacetic acid (pH 8.0) and
visualized by ethidium bromide staining.
Statistical analysis
Statistical analysis of the data was performed using
SPSS version 19.0 (IBM SPSS, Armonk, NY, USA). The methylation
status of APC and RASSF1A and all other qualitative
variables were expressed as frequencies and percentages. The χ2
test was used to evaluate any potential association of APC
and RASSF1A status with patients' demographic and
clinicopathological characteristics. Odds ratios (ORs) and their
95% confidence intervals (CIs) were estimated as a measure of the
association between APC and RASSF1A status and
patients' characteristics. Survival rates were calculated with the
Kaplan-Meier method, and the statistical difference between the
survival curves was determined with the log-rank test. Multivariate
Cox proportional hazards regression (HR) analysis, using a backward
selection approach, were performed to explore the independent
effect of APC and RASSF1A status on overall survival.
Patients' gender, age, clinical stage, tumor differentiation, lymph
node status, CEA and CA 19.9 levels were also included in the
multivariate model as potential confounders. All tests were two
tailed, and P<0.05 was considered to indicate a statistical
significant difference.
Results
Characteristics of the study
population
The study population consisted of 155 patients with
CRC with a median age of 70 years (range, 44–76 years; mean age ±
standard deviation, 68.35±9.20 years), 57.4% of whom were males.
The patient's clinicopathological characteristics are indicated in
Table I. In total, 48 tumors (31.0%)
were well differentiated, 79 (51.0%) were moderately differentiated
and 28 (18.1%) were poorly differentiated carcinomas. The Dukes'
system (32) was used for the
classification of patients into different stages. Almost half of
the cases (67 patients, 43.2%) were at stage D, 30 (19.3%) cases
were at stage C and 58 (37.4%) were at stage A or B. APC and
RASSF1A promoters were observed to be methylated in 65
(41.9%) and 52 (33.5%) of the 155 colon cancer samples examined,
but in none of the normal control samples (both P<0.001). The
association of the patients' demographic and clinicopathological
features with APC and RASSF1A methylation status is
presented in Tables II and III.
| Table II.Association of APC and
RASSF1A methylation status with demographic and
clinicopathological characteristics of patients with operable
disease. |
Table II.
Association of APC and
RASSF1A methylation status with demographic and
clinicopathological characteristics of patients with operable
disease.
| Patients'
characteristics | APC
methylation | P-value | RASSF1A
methylation | P-value |
|---|
| Gender |
| 0.711 |
| 0.170 |
|
Males | 16 (31.4) |
| 10 (19.6) |
|
|
Females | 13 (35.1) |
| 12 (32.4) |
|
| Age, years |
| 0.012 |
| 0.267 |
|
≤70 | 8 (19.5) |
| 8 (19.5) |
|
|
>70 | 21 (44.7) |
| 14 (29.8) |
|
| Dukes' stage |
| 0.014 |
| 0.021 |
|
A+B | 14 (24.1) |
| 8 (14.3) |
|
| C | 15 (50.0) |
| 14 (34.1) |
|
|
Differentiation |
| 0.403 |
| 0.670 |
|
Well | 8 (26.7) |
| 9 (30.0) |
|
|
Moderate | 14 (32.6) |
| 9 (20.9) |
|
|
Poor | 7 (46.7) |
| 4 (26.7) |
|
| Tumor location,
colon side |
| 0.407 |
| 0.538 |
|
Right | 16 (37.2) |
| 12 (27.9) |
|
|
Left | 13 (28.9) |
| 10 (22.2) |
|
| CEA levels, ng/ml
(n=82) |
| 0.088 |
| 0.697 |
| ≤5 | 10 (25.0) |
| 9 (22.5) |
|
|
>5 | 18 (42.9) |
| 11 (26.2) |
|
| CA 19.9 levels,
U/ml (n=82) |
| 0.083 |
| 0.372 |
| <37
(low) | 20 (29.9) |
| 15 (22.4) |
|
| >37
(high) | 8 (53.3) |
| 5 (33.3) |
|
| APC
status |
| – |
| 0.050 |
|
Unmethylated | – |
| 11 (18.6) |
|
|
Methylated | – |
| 11 (37.9) |
|
| RASSF1A
status |
| 0.050 |
| – |
|
Unmethylated | 18 (27.3) |
| – |
|
|
Methylated | 11 (50.0) |
| – |
|
| Table III.Association of APC and
RASSF1A methylation status with demographic and
clinicopathological characteristics of patients with metastatic
disease. |
Table III.
Association of APC and
RASSF1A methylation status with demographic and
clinicopathological characteristics of patients with metastatic
disease.
|
| |
| |
|
|---|
| Patients'
characteristics | APC
methylation | P-value | RASSF1A
methylation | P-value |
|---|
| Gender |
| 0.076 |
| 0.994 |
|
Males | 24 (63.2) |
| 17 (44.7) |
|
|
Females | 12 (41.4) |
| 13 (44.8) |
|
| Age, years |
| 0.427 |
| 0.921 |
|
≤70 | 21 (50.0) |
| 19 (45.2) |
|
|
>70 | 15 (60.0) |
| 11 (44.0) |
|
| Dukes' stage |
| – |
| – |
|
A+B | – |
| – |
|
| C | – |
| – |
|
| D | 36 (53.7) |
| 30 (44.8) |
|
|
Differentiation |
| 0.388 |
| 0.032 |
|
Well | 10 (55.6) |
| 12 (66.7) |
|
|
Moderate | 17 (47.2) |
| 11 (30.6) |
|
|
Poor | 9 (69.2) |
| 7 (53.8) |
|
| Tumor location,
colon side |
| 0.100 |
| 0.581 |
|
Right | 20 (64.5) |
| 15 (48.4) |
|
|
Left | 16 (44.4) |
| 15 (41.7) |
|
| CEA levels, ng/ml
(n=56) |
| 0.159 |
| 0.023 |
| ≤5 | 7 (41.2) |
| 4 (23.5) |
|
|
>5 | 24 (61.5) |
| 22 (56.4) |
|
| CA 19.9 levels,
U/ml (n=55) |
| 0.883 |
| 0.898 |
| <37
(low) | 15 (53.6) |
| 13 (46.4) |
|
| >37
(high) | 15 (55.6) |
| 13 (48.1) |
|
| APC
status |
| – |
| 0.016 |
|
Unmethylated | – |
| 9 (29.0) |
|
|
Methylated | – |
| 21 (58.3) |
|
| RASSF1A
status |
| 0.016 |
| – |
|
Unmethylated | 15 (40.5) |
| – |
|
|
Methylated | 21 (70.0) |
| – |
|
Correlation between APC methylation
status and different tumor parameters
Patients with early oCRC
APC was methylated in 29 of 88 patients with
early oCRC (33.0%). χ2 analysis revealed that methylated APC
promoter status was associated with age >70 years (OR=3.33, 95%
CI=1.27–8.73, P=0.012), higher stage (OR=3.14, 95% CI=1.23–8.00,
P=0.014) and methylated RASSF1A status (OR=2.67, 95%
CI=1.00–7.22, P=0.050), while a tendency was noticed with high CEA
levels (OR=2.25, 95% CI=0.88–5.77, P=0.088) and high CA 19.9 levels
(OR=2.69, 95% CI=0.86–8.41, P=0.083) (Table II).
Patients with metastatic disease
APC was methylated in 36 of 67 patients with
mCRC (53.7%). Methylated APC promoter status was associated
with methylated RASSF1A status (OR=3.42, 95% CI=1.23–9.49,
P=0.016) and marginally with male gender (OR=2.43, 95%
CI=0.90–6.54, P=0.076). No other significant associations between
APC methylation status and other tumor parameters were
observed in patients with mCRC (Table
III).
Correlation between RASSF1A
methylation status and different tumor parameters
Patients with early oCRC
RASSF1A was methylated in 22 of 88 patients
with early oCRC (25.0%). Methylated RASSF1A promoter status
was significantly associated with higher disease stage (OR=3.11,
95% CI=1.16–8.36, P=0.021). No other significant associations were
observed (Table II).
Patients with metastatic disease
RASSF1A was methylated in 30 of 67 patients
with mCRC (44.8%). Methylated RASSF1A promoter status was
significantly associated with moderate differentiation (OR=3.60,
95% CI=1.31–9.91, P=0.012), high CEA levels (OR=4.21, 95%
CI=1.16–15.23, P=0.023) and methylated APC status (OR=3.42,
95% CI=1.23–9.49, P=0.016) (Table
III).
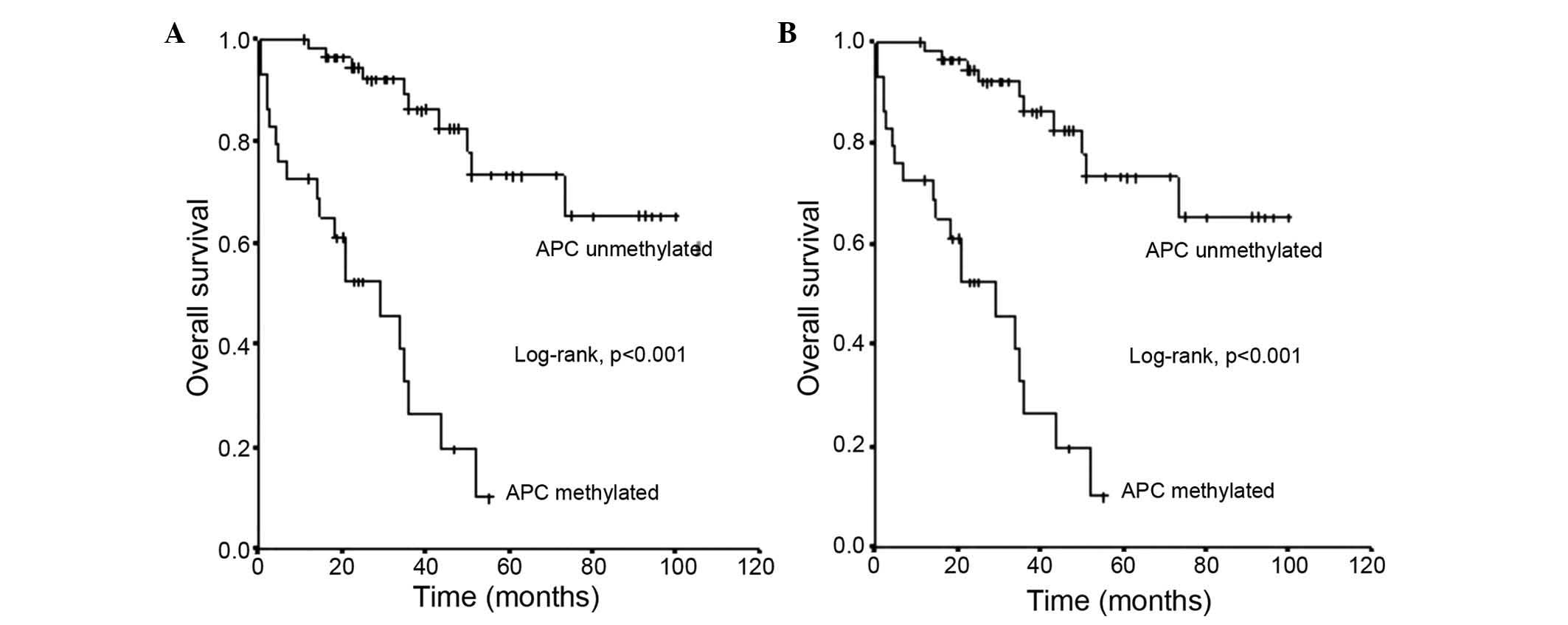
APC methylation status and survival in patients
with early oCRC
The mean survival time ± standard error (SE) of
patients with oCRC and an unmethylated APC promoter status
was 81±5 months (95% CI=71–91), which was significantly longer than
the mean survival ± SE of 27±4 months (95% CI=19–34) observed for
those with a methylated APC promoter status (log-rank test,
P<0.001) (Fig. 1A).
APC methylation status and survival in patients
with mCRC
The mean survival time ± SE of patients with mCRC
and an unmethylated APC promoter status was 37±7 months (95%
CI=23–50), which was substantially longer than the mean survival ±
SE of 15±3 months (95% CI=9–20) observed in those with a methylated
APC promoter status (log-rank test, P<0.001) (Fig. 1B).
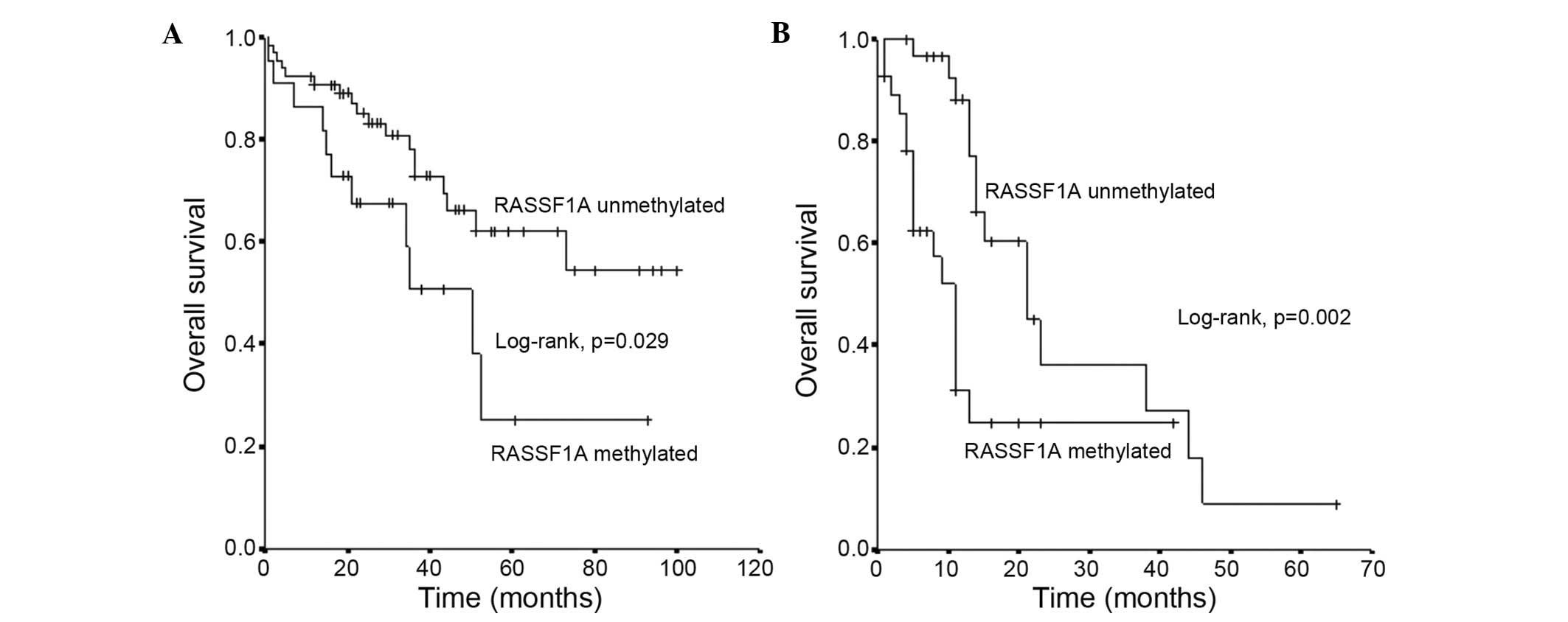
RASSF1A methylation status and survival in
patients with early oCRC
The mean survival time ± SE of patients with oCRC
and an unmethylated RASSF1A promoter status was 71±6 months
(95% CI=60–81), which was substantially longer than the mean
survival ± SE of 46±8 months (95% CI=29–62) observed in those with
a methylated RASSF1A promoter status (log-rank test,
P<0.001) (Fig. 2A).
RASSF1A methylation status and survival in
patients with mCRC
The mean survival time ± SE of patients with mCRC
and an unmethylated RASSF1A promoter status was 28±4 months
(95% CI=19–36) months, which was substantially longer than the mean
survival ± SE of 16±3 months (95% CI=9–22) months observed in
patients with a methylated RASSF1A promoter status (log-rank
test, P<0.001) (Fig. 2B).
Multivariate Cox proportional HR analysis
Upon stratification of the analysis according to the
presence or absence of metastases, the negative impact of
methylated APC promoter status on patients' survival was
more pronounced in patients without metastases [adjusted HR
(aHR)=7.88, 95% CI=2.73–22.73, P<0.001] than in patients with
metastases (aHR=3.47, 95% CI=1.35–8.92, P=0.017), while the
negative impact of methylated RASSF1A promoter status on
patients' survival was more pronounced in patients with metastases
(aHR=5.76, 95% CI=2.44–14.82, P=0.001) than among patients without
metastases (aHR=3.06, 95% CI=1.25–7.50, P=0.038).
Discussion
CRC remains a global burden on world health and
economy, despite having a 90% 5-year survival rate when detected
and treated early (1,33). Traditional methods cannot sufficiently
predict the prognosis of single cancer cases, and clinicians may be
not able to accurately decide which patients will be at high risk
of recurrence and benefit from chemotherapy. Therefore, it is
essential to identify novel biomarkers for improved prognosis,
which would aid clinicians to decide which patients should receive
adjuvant treatment. The questions of which patients should be
treated and why certain patients respond better to chemotherapy
than others must be solved, as adjuvant cancer therapy imposes
unnecessary toxicity and a huge financial burden on patients. In
the present study, the promoter methylation status of the
APC and RASSF1A genes in cell-free DNA from patients
with CRC was explored, and their incidence and potential
correlations with different tumor parameters and survival were
examined.
RASSF1A protein is actively involved in microtubule
regulation, genomic stability maintenance, cell-cycle regulation,
apoptosis modulation, cell motility and invasion control (34–36). A
number of studies have identified a high percentage of
RASSF1A methylation in CRC samples. Wagner et al
(37) observed RASSF1A
promoter methylation in 45% (13/29) of the primary CRC and in 80%
(4/5) of the CRC cell lines analyzed. Contrarily, in a study with
222 sporadic CRC samples, van Engeland et al (38) detected RASSF1A methylation in
20% (45/222) of the samples, and a mutually exclusive association
with the presence of Kirsten rat sarcoma viral oncogene homolog
(KRAS) mutations was suggested. Several other studies reported
RASSF1A methylation in 17% (8/47), 36% (26/73) and 47%
(17/36) of the CRC samples examined (39–41).
Notably, the above different studies reporting RASSF1A
methylation at different stages, as well as in the corresponding
normal mucosa adjacent to the tumor, point to a role of the tumor
suppressor gene RASSF1A early in the development of
colorectal carcinogenesis. It may mean that methylation possibly
occurs in proximal sites of cancer cells due to field effect
phenomena; however, the mechanism remains to be determined. The
present results are in accordance with the aforementioned reports,
as 25% hypermethylated RASSF1A promoter was detected in
patients with early oCRC, and 44.8% hypermethylated RASSF1A
promoter was detected in patients with mCRC, suggesting that
RASSF1A methylation is a frequent event in CRC, although
more pronounced at later disease stages. This higher incidence of
RASSF1A methylation in metastatic disease may be indicative
of a more aggressive tumor behavior, which may explain the
association with poorer prognosis observed in the present study. In
our previous study, we performed a similar analysis of
RASSF1A methylation status in patients with operable gastric
cancer (42). In that study, a
methylation rate of 68.5% was detected, which underlines the
difference in the biological behavior of gastric cancer in
comparison with CRC. Which of the multiple roles of RASSF1A
is played at different disease stages according to its methylation
status is unclear.
Wagner et al (37) investigated whether RASSF1A
methylation correlated with tumor-node-metastasis status, but did
not detect any significant associations. Similarly, in the study by
Van England et al (38),
RASSF1A methylation was not associated with gender, Duke's stage or
location of the tumor. The only exception was the age at diagnosis,
which was slightly higher in RASSF1A methylated CRC cases compared
to non-methylated ones.
In a previous study with 36 CRC samples, a
significant correlation was observed between RASSF1A
methylation and gender, with RASSF1A being more frequently
methylated in females (41) In the
present study, methylated RASSF1A was associated with higher
stages in patients with early oCRC, while in patients with
metastatic disease, methylated RASSF1A was significantly
associated with moderate differentiations, high CEA levels and
APC hypermethylated promoter status. Notably, in other
studies, RASSF1A methylation levels were significantly
higher in distal CRC, compared with proximal CRC (43,44), as
well as in normal mucosae (44). The
present data did not support a difference in the profile of
methylation between right and left colon. Additionally, a
significant difference was observed in the survival of patients
with unmethylated RASSF1A promoter status, compared with
those with methylated RASSF1A, in patients with and without
metastases. Furthermore, the negative impact of methylated
RASSF1A promoter status on patients' survival was more
pronounced in patients with metastases. Additional studies are
required for a better characterization of the subsets of patients
with RASSF1A promoter methylation and a better understanding
of the role of RASSF1A in CRC development.
Germline mutations in the tumor suppressor
APC gene cause familial adenomatous polyposis, and somatic
mutations are common in sporadic CRC (45). Hypermethylation of the APC
promoter has been reported in early steps of carcinogenesis in
several tumors (46). A previous
study reported that the frequencies of aberrant promoter
methylation were 16% for cadherin 1, 2% for p16, 4% for MGMT and
24% for APC (47). An aberrant
methylation of ≥1 of these genes was identified in 45 of 51 (88%)
primary tumors (48). In the present
cohort, APC was methylated in 33% of patients with early
oCRC and in 53.7% of patients with mCRC. In patients with early
oCRC, methylated APC promoter status was associated with
ages older than 70 years and methylated RASSF1A status,
while a tendency was observed with high CEA and CA 19.9 levels. In
patients with metastatic disease, APC methylation was
associated with methylated RASSF1A status and male gender.
Patients with an unmethylated APC promoter status had a
substantially longer mean survival than those with a methylated
APC promoter status, both in early and metastatic disease. A
significant and unexpected finding of the present study was that
the negative impact of methylated APC promoter status on
patients' survival was more pronounced in patients without
metastases than in patients with metastases. The present authors do
not have a clear explanation for this observation. It appears that,
although APC methylation is most frequently observed at
later stages, when present at earlier stages it is indicative of an
aggressive tumor phenotype associated with shorter survival. The
present findings are in agreement with the proposed roles of
APC and RASSF1A as tumor suppressor genes. Their
silencing as a result of their methylation is indicative of a more
aggressive tumor phenotype with shorter survival. This is also
supported by the observed correlations with bad prognostic
features, such as higher disease stages and older age for
APC, and higher stages, moderate differentiation and high
CEA levels for RASSF1A.
In conclusion, the present study demonstrated that
serum RASSF1A and APC promoter hypermethylation is a
frequent epigenetic event in patients with colon cancer, in both
early and metastatic disease, which is indicative of a crucial role
for both proteins in colorectal carcinogenesis. In addition, a
significant correlation was observed between APC and
RASSF1A promoter methylation status and survival. The high
percentage of methylation of both proteins in the early and
metastatic setting indicates that methylation represents a common
event, and when present, it is possibly associated with a more
aggressive tumor phenotype. Additional studies in a larger cohort
of patients are required to further explore whether these findings
could establish the methylation status of APC and
RASSF1A as potential biomarkers for early detection and
prognosis in CRC.
Glossary
Abbreviations
Abbreviations:
|
MSP
|
methylation-specific polymerase chain
reaction
|
|
OS
|
overall survival
|
|
PS
|
performance status
|
|
CRC
|
colorectal cancer
|
|
oCRC
|
operable colorectal cancer
|
|
mCRC
|
metastatic colorectal cancer
|
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Migliore L, Migheli F, Spisni R and
Coppedè F: Genetics, cytogenetics, and epigenetics of colorectal
cancer. J Biomed Biotechnol. 2011:7923622011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Segal NH and Saltz LB: Evolving treatment
of advanced colon cancer. Annu Rev Med. 60:207–219. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bardhan K and Liu K: Epigenetics and
colorectal cancer pathogenesis. Cancers (Basel). 5:676–713. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kulis M and Esteller M: DNA methylation
and cancer. Adv Genet. 70:27–56. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Baylin SB: DNA methylation and gene
silencing in cancer. Nat Clin Pract Oncol. 2(Suppl 1): S4–S11.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nakajima T, Enomoto S and Uschijima T: DNA
methylation: A marker for carcinogen exposure and cancer risk.
Environ Health Prev Med. 13:8–15. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ye T, Chen Y and Fang J: DNA methylation
biomarkers in serum for gastric cancer screening. Mini Rev Med
Chem. 10:1034–1038. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shivapurkar N and Gazdar AF: DNA
methylation based biomarkers in non-invasive cancer screening. Curr
Mol Med. 10:123–132. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Aarthy R, Mani S, Velusami S, Sundarsingh
S and Rajkumar T: Role of circulating cell-free DNA in cancers. Mol
Diagn Ther. 19:339–350. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jahr S, Hentze H, English S, Hardt D,
Fackelmayer FO, Hesch RD and Knippers R: DNA fragments in the blood
plasma of cancer patients: Quantitations and evidence for their
origin from apoptotic and necrotic cells. Cancer Res. 61:1659–1665.
2001.PubMed/NCBI
|
|
12
|
Gormally E, Caboux E, Vineis P and Hainaut
P: Circulating free DNA in plasma or serum as a biomarker of
carcinogenesis: Practical aspects and biological significance.
Mutat Res. 635:105–117. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jung K, Fleischhacker M and Rabien A:
Cell-free DNA in the blood as a solid tumor biomarker-a critical
appraisal of the literature. Clin Chim Acta. 411:1611–1624. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bardhan K and Liu K: Epigenetics and
colorectal cancer pathogenesis. Cancer (Basel). 5:676–713. 2013.
View Article : Google Scholar
|
|
15
|
Richter AM, Pfeifer GP and Dammann RH: The
RASSF proteins in cancer; From epigenetic silencing to functional
characterization. Biochim Biophys Acta. 1796:114–128.
2009.PubMed/NCBI
|
|
16
|
Oliveira C, Velho S, Domingo E, Preto A,
Hofstra RM, Hamelin R, Yamamoto H, Seruca R and Schwartz S Jr:
Concomitant RASSF1A hypermethylation and KRAS/BRAF mutations
occur preferentially in MSI sporadic colorectal cancer. Oncogene.
24:7630–7634. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dammann R, Li C, Yoon JH, Chin PL, Bates S
and Pfeifer GP: Epigenetic inactivation of a RAS association domain
family protein from lung tumour suppressor locus 3p21.3. Nat Genet.
25:315–319. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Donninger H, Vos MD and Clark GJ: The
RASSF1A tumor suppressor. J Cell Sci. 120:3163–3172. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yoon JH, Dammann R and Pfeifer GP:
Hypermethylation of the CpG island of the RASSF1A gene in
ovarian and renal cell carcinomas. Int J Cancer. 94:212–217. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sakamoto N, Terai T, Ajioka Y, Abe S,
Kobayasi O, Hirai S, Hino O, Watanabe H, Sato N, Shimoda T and
Fujii H: Frequent hypermethylation of RASSF1A in early
flat-type colorectal tumors. Oncogene. 23:8900–8907. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Miyoshi Y, Nagase H, Ando H, Horii A,
Ichii S, Nakatsuru S, Aoki T, Miki Y, Mori T and Nakamura Y:
Somatic mutations of the APC gene in colorectal tumors:
Mutation cluster region in the APC gene. Hum Mol Genet.
1:229–233. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rosin-Arbesfeld R, Townsley F and Bienz M:
The APC tumour suppressor has a nuclear export function. Nature.
406:1009–1012. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Morin PJ, Sparks AB, Korinek V, Barker N,
Clevers H, Vogelstein B and Kinzler KW: Activation of
beta-catenin-Tcf signaling in colon cancer by mutations in
beta-catenin or APC. Science. 275:1787–1790. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schneikert J and Behrens J: The canonical
Wnt signaling pathway and its APC partner in colon cancer
development. Gut. 56:417–425. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Naghibalhossaini F, Zamani M, Mokarram P,
Khalili I, Rasti M and Mostafavi-Pour Z: Epigenetic and genetic
analysis of WNT signaling pathway in sporadic colorectal cancer
patients from Iran. Mol Biol Rep. 39:6171–6178. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Esteller M, Sparks A, Toyota M,
Sanchez-Cespedes M, Capella G, Peinado MA, Gonzales S, Tarafa G,
Sidransky D, Meltzer SJ, et al: Analysis of adenomatous polyposis
coli promoter hypermethylation in human cancer. Cancer Res.
60:4366–4371. 2000.PubMed/NCBI
|
|
27
|
Lee S, Hwang KS, Lee HJ, Kim JS and Kang
GH: Aberrant CpG island hypermethylation of multiple genes in
colorectal neoplasia. Lab Invest. 84:884–893. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lee BB, Lee EJ, Jung EH, Chun HK, Chang
DK, Song SY, Park J and Kim DK: Aberrant methylation of APC,
MGMT, RASSF2A, and Wif-1 genes in plasma as a biomarker for early
detection of colorectal cancer. Clin Cancer Res. 15:6185–6191.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chen SP, Chiu SC, Wu CC, Lin SZ, Kang JC,
Chen YL, Lin PC, Pang CY and Harn HJ: The association of
methylation in the promoter of APC and MGMT and the
prognosis of Taiwanese CRC patients. Genet Test Mol Biomarkers.
13:67–71. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Clément G, Bosman FT, Fontolliet C and
Benhattar J: Monoallelic methylation of the APC promoter is
altered in normal gastric mucosa associated with neoplastic
lesions. Cancer Res. 64:6867–6873. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Edge S, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual (7th). Springer.
New York: 2010.
|
|
33
|
Choong MK and Tsafnat G: Genetic and
epigenetic biomarkers of colorectal cancer. Clin Gastroenterol
Hepatol. 10:9–15. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ghazaleh HA, Chow RS, Choo SL, Pham D,
Olessen JD, Wang RX, Onyskiw C and Baksh S: 14-3-3 mediated
regulation of the tumor suppressor protein, RASSF1A.
Apoptosis. 15:117–127. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Shivakumar L, Minna J, Sakamaki T, Pestell
R and White MA: The RASSF1A tumor suppressor blocks cell
cycle progression and inhibits cyclin D1 accumulation. Mol Cell
Biol. 22:4309–4318. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dallol A, Agathanggelou A, Fenton SL,
Ahmed-Choudhury J, Hesson L, Vos MD, Clark GJ, Downward J, Maher ER
and Latif F: RASSF1A interacts with microtubule-associated
proteins and modulates microtubule dynamics. Cancer Res.
64:4112–4116. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wagner KJ, Cooper WN, Grundy RG, Caldwell
G, Jones C, Wadey RB, Morton D, Schofield PN, Reik W, Latif F and
Maher ER: Frequent RASSF1A tumor suppressor gene promoter
methylation in Wilms' tumor and colorectal cancer. Oncogene.
21:7277–7282. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
van Engeland M, Roemen GM, Brink M, Pachen
MM, Weijenberg MP, de Bruïne AP, Arends JW, van den Brandt PA, de
Goeij AF and Herman JG: K-ras mutations and RASSF1A promoter
methylation in colorectal cancer. Oncogene. 21:3792–3795. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Gonzalo V, Lozano JJ, Muñoz J, Balaguer F,
Pellisé M, de Rodríguez Miguel C, Andreu M, Jover R, Llor X,
Giráldez MD, et al: Aberrant gene promoter methylation associated
with sporadic multiple colorectal cancer. PLoS One. 5:e87772010.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Miladi-Abdennadher I, Abdelmaksoud-Damak
R, Ayadi L, Khabir A, Frikha F, Kallel L, Amouri A, Frikha M,
Sellami-Boudawara T, Gargouri A and Mokdad-Gargouri R:
Hypermethylation of RARβ2 correlates with high COX-2 expression and
poor prognosis in patients with colorectal carcinoma. Tumor Biol.
31:503–511. 2010. View Article : Google Scholar
|
|
41
|
Abouzeid HE, Kassem AM, Wahab Abdel AH,
El-mezayen HA, Sharad H and Abdel Rahman S: Promoter
hypermethylation of RASSF1A, MGMT, and HIC-1 genes in benign
and malignant colorectal tumors. Tumor Biol. 32:845–852. 2011.
View Article : Google Scholar
|
|
42
|
Balgkouranidou I, Matthaios D,
Karayiannakis A, Bolanaki H, Michailidis P, Xenidis N, Amarantidis
K, Chelis L, Trypsianis G, Chatzaki E, et al: Prognostic role of
APC and RASSF1A promoter methylation status in cell free
circulating DNA of operable gastric cancer patients. Mutat Res.
778:46–51. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ahlquist T, Bottillo I, Danielsen SA,
Meling GI, Rognum TO, Lind GE, Dallapiccola B and Lothe RA: RAS
signaling in colorectal carcinomas through alteration of RAS, RAF,
NF1, and/or RASSF1A. Neoplasia. 10:680–686. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
An B, Kondo Y, Okamoto Y, Shinjo K,
Kanemitsu Y, Komori K, Hirai T, Sawaki A, Tajika M, Nakamura T, et
al: Characteristic methylation profile in CpG island methylator
phenotype-negative distal colorectal cancers. Int J Cancer.
127:2095–2105. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Huang J, Zheng S, Jin SH and Zhang SZ:
Somatic mutations of APC gene in carcinomas from hereditary
non-polyposis colorectal cancer patients. World J Gastroenterol.
10:834–836. 2010.
|
|
46
|
Kim MS, Lee J and Sidransky D: DNA
methylation markers in colorectal cancer. Cancer Metastasis Rev.
29:181–206. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Kamiyama H, Noda H, Takata O, Suzuki K,
Kawamura Y and Konishi F: Promoter hypermethylation of
tumor-related genes in peritoneal lavage and the prognosis of
patients with colorectal cancer. J Surg Oncol. 100:69–74. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Kamiyama H, Noda H, Takata O, Suzuki K,
Kawamura Y and Konishi F: Promoter hypermethylation of
tumor-related genes in peritoneal lavage and the prognosis of
patients with colorectal cancer. J Surg Oncol. 100:69–74. 2009.
View Article : Google Scholar : PubMed/NCBI
|