Introduction
Acute leukemia (AL) is a clonal disease that
progressively produces novel sub-clones, which exhibit altered
phenotypic and cytogenetic traits. AL is divided into acute
lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML). AML
is the most common type of leukemia in adults. Acute promyelocytic
leukemia (APL) is a distinct subtype of AML characterized by
coagulopathy and signs of disseminated intravascular coagulation
(1,2).
It is not known whether coagulation results are associated with AL
except in APL. Therefore, the comparison of certain clinical
parameters of AL patients, including activated partial
thromboplastin time (aPTT), prothrombin time (PT), D-dimer and
fibrinogen (FIB) should be eliminated due to interference from the
APL cohort. Despite high sensitivity to standard chemotherapy,
which leads to increased rate of complete remission (CR) in the two
subtypes of AL, ~1/3 of AL patients subsequently relapse (3–6). AL
relapse following standard chemotherapy remains a significant
therapeutic challenge (7–10). AL continues to have a low survival
rate compared to other cancers (11).
Disease-free survival rates are 5–15% in older adults and 25–40% in
younger patients (12).
Metabolic changes occur as part of oncogenesis and
tumor progression. A better understanding of AL relapse and the
careful monitoring of clinical parameters following chemotherapy
may aid clinicians in determining the best treatment options on an
individual patient basis. As a result of local activation of
intravascular coagulation at the onset of some forms of malignancy
(13,14), the fibrinolytic marker D-dimer
increases and accumulates (14). LDH
exists in numerous cell systems and, subsequent to tissue or cell
damage, serum LDH levels may increase (15). Although it is generally understood
that there is a poor outcome for adults with AL that develop bone
marrow relapse (16) and various risk
factors predicting outcome are continuously analyzed, there are few
studies concerning LDH and D-dimer in these types of patients. The
present study was performed to determine whether D-dimer and LDH
levels during treatment are associated with relapse in patients
with AL.
Materials and methods
Patients
The present study evaluated data from 204 patients
that were newly diagnosed with AL at the The First Affiliated
Hospital of Wenzhou Medical University (Wenzhou, China) between
February 2010 and October 2014, several of whom relapsed. At the
initial onset, 204 patients were treated uniformly for AML or ALL.
AL was classified according to the FAB criteria (17). In total there were 40 ALL patients and
164 AML patients (M1, 44; M2, 26; M3, 32; M4, 36; M5, 20; M6, 6).
AML patients only were treated with daunorubicin (45
mg/m2 per day on days 1–3) and cytarabine (150
mg/m2 per day for 7 days) according to the 3 plus 7
regimen. APL patients were treated based on an all-trans retinoic
acid (20 mg/m2 per day on days 1–15) plus anthracycline
(idarubicin; 8 mg/m2 per day on days 1–3) protocol. The
induction chemotherapy in ALL patients included vincristine (2 mg
per day on days 1, 8, 15 and 22) and daunorubicin (40
mg/m2 per day on days 1–3), prednisone]1 mg/kg per day
on days 1–14 and 15–28 (2/3 dose)] and L-asparaginase (6,000
IU/m2 per day on days 11, 14, 17, 20, 23 and 26). The AL
patients were free from any systemic, cardiovascular or
inflammatory illnesses. The Ethics Committee at The First
Affiliated Hospital of Wenzhou Medical University approved the
present study. Written informed consent was obtained from the
patients.
Blood collection
Blood samples were taken from the antecubual vein
and placed in plastic tubes containing 3.8% trisodium citrate (9
volumes of blood and 1 volume of 0.1 M trisodium citrate) or
ethylenediaminetetraacetic acid (EDTA)·K2 anticoagulant.
For plasma separation, blood was centrifuged at 2,500 × g for 15
min at 4°C; blood samples were obtained prior to the initiation of
any treatment for AL. The present study adhered to the tenets of
the Declaration of Helsinki.
Data collection
Blood counts were performed using an XE 2100 Sysmex™
automated hematology analyzer (Sysmex, Kobe, Japan). aPTT, PT,
D-dimer and FIB were measured using a STAGO Coagulation analyzer
(Diagnostica Stago, Asnières, France). The
STA®-Liatest® D-Di kit (Diagnostica Stago) is
intended for use with analyzers of the STA® line
suitable with these reagents for the quantitative determination of
D-dimer in plasma by immuno-turbidimetric method. The
STA®-fibrinogen kit (Diagnostica Stago) is intended for
use with STA-R® analyzers for the quantitative
determination of FIB levels in plasma using the clotting method of
Clauss. The STA®-néoplastine Cl Plus and
STA®-APTT kits (Diagnostica Stago) are intended for use
with STA-R® analyzers for the determination of PT and
aPTT in plasma by the clotting method, respectively. Lactate
dehydrogenase (LDH) plasma levels were measured using the LDH
substrates method (Beckman Coulter Experiment System Co., Ltd.,
Suzhou, China). Markers were compared against normal ranges, which
were as follows: White blood cell (WBC) count,
3.5–9.5×109/l; platelet (PLT) count,
125.0–350.0×109/l; hemoglobin (Hb), 115.0–175.0 g/l; PT,
11.6–14.9 sec; aPTT, 29.0–43.0 sec; FIB, 2.0–4.0 g/l; D-dimer,
0.0–0.5 mg/l; and LDH, 0.0–247.0 units (U)/l. The laboratory data
were collected promptly at the initial onset of AL, CR and in
patients with relapsed AL.
Response evaluation
The diagnostics were comprised of cytomorphology,
cytochemistry, cytogenetics, molecular genetics and
immunophenotyping of bone marrow or peripheral blood. Bone marrow
aspirate smears were applied to assess the therapeutic effect of
AL. The morphological diagnosis and classification were performed
according to the WHO 2008 diagnostic criteria (18).
Statistical analysis
The results were graphed using line charts depicting
medians and range. The data were analyzed using the Wilcoxon
matched pairs test. Spearman's rank correlation coefficient was
used to analyze correlations between serum D-dimer or LDH level and
selected blood routine parameters. P-values of <0.05 were
considered to indicate a statistically significant difference. Data
were analyzed using SPSS version 13.0 for Windows (SPSS, Chicago,
IL, USA).
Results
Clinical parameters of AL patients at
various stages of disease
Laboratory data in patients with initial onset, CR
and relapsed AL are shown in Table I.
The WBC count was significantly different at the initial onset of
AL (P=0.002) and during relapsed AL, compared with patients in the
CR group (P=0.009). Hb levels (P<0.001 and P=0.003) and PLT
counts (P=0.001 and P<0.001) were significantly reduced in the
initial onset and relapsed AL groups. compared with the CR group.
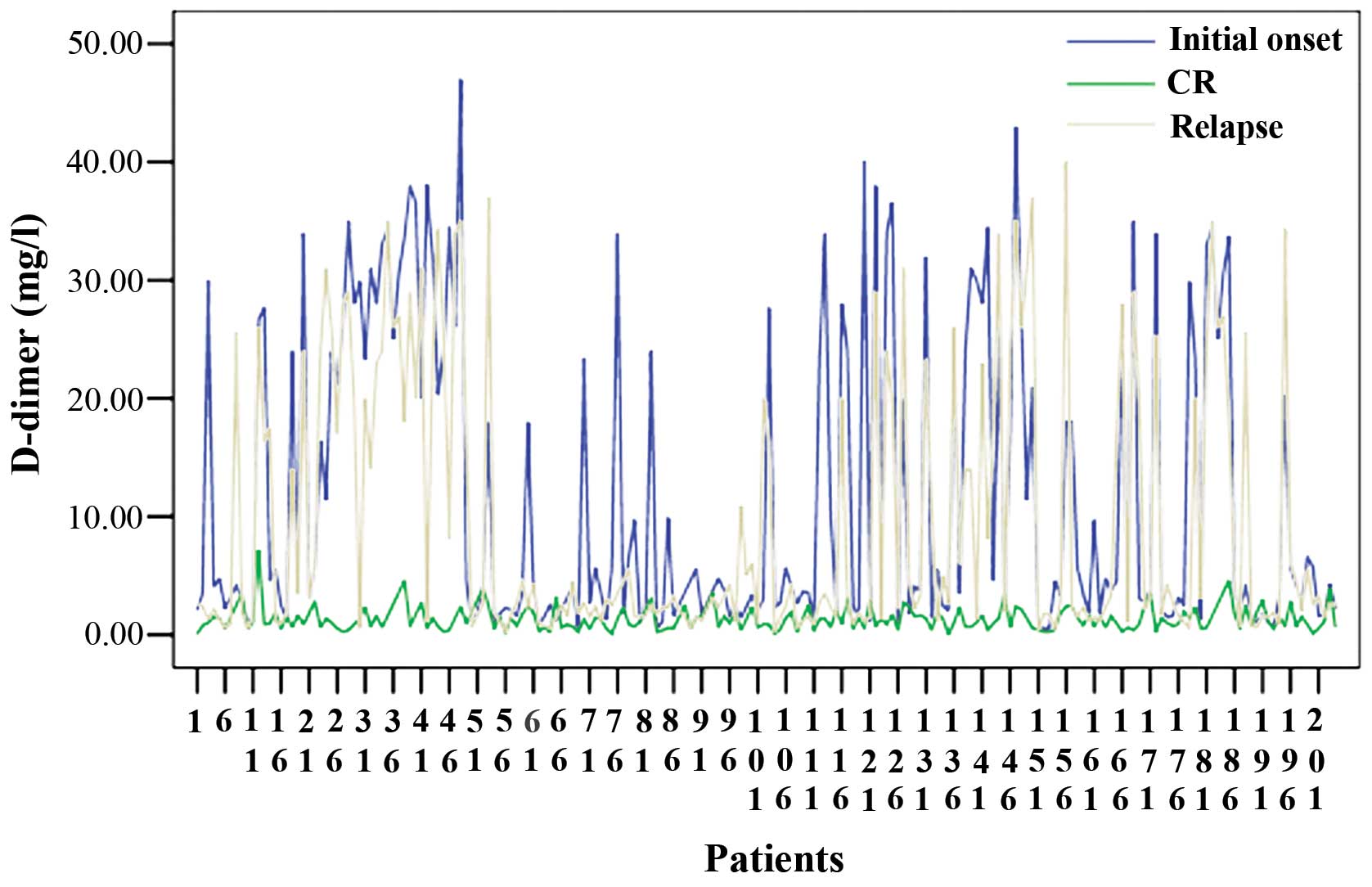
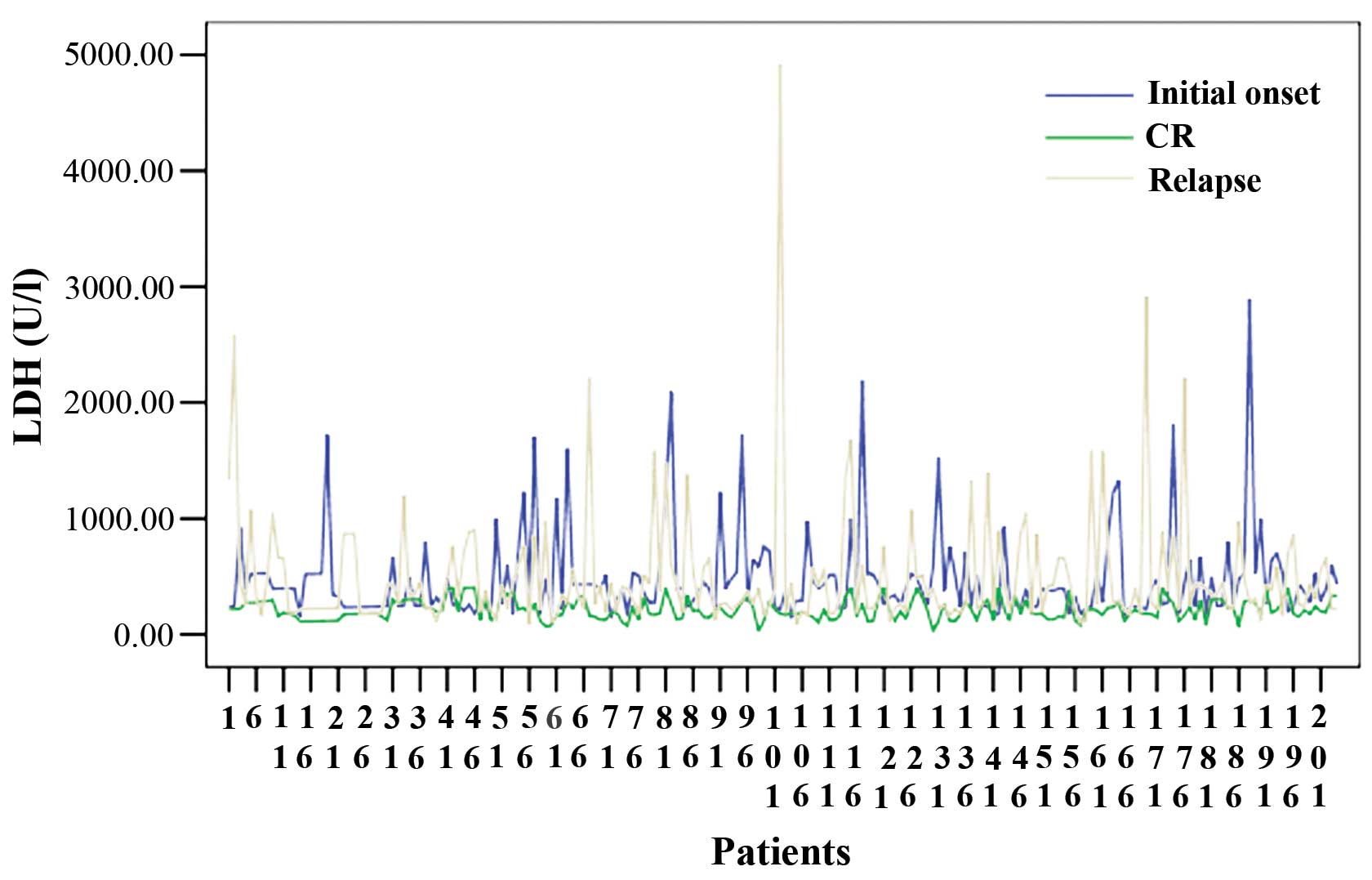
D-dimer (P=0.005 and P=0.007) and LDH levels (P=0.007 and P=0.008)
were also significantly increased in the two groups compared with
the CR group (Figs. 1 and 2). In addition, these levels were
significantly different across the two groups compared with AL in
CR, regardless of whether APL patients were included. Plasma PT and
FIB levels were significantly (P=0.020) increased in the initial
onset and relapsed AL groups compared with patients achieving CR.
Plasma FIB levels were significantly decreased in the initial onset
(P=0.008) and relapsed AL groups (P=0.009) compared with patients
achieving CR. Plasma aPTT levels were not significantly different
between patients with initial onset or relapsed AL and AL in CR.
When coagulation data results were eliminated in patients with APL,
plasma levels of aPTT were elevated, but plasma PT, aPTT and FIB
levels were not significantly different between patients with
relapsed AL and AL in CR.
 | Table I.Blood routine and coagulation
measurements in patients at various stages of AL. |
Table I.
Blood routine and coagulation
measurements in patients at various stages of AL.
|
| AL disease
including APL, median (range) | AL disease except
for APL, median (range) |
|---|
|
|
|
|
|---|
|
Characteristics | Initial onset | CR | Relapse | Initial onset | CR | Relapse |
|---|
| WBC,
×109/l | 11.6 | 4.8 | 5.8 | 21.9 | 4.2 | 10.6 |
|
|
(0.1–658.4)a | (2.1–13.2) |
(0.1–328.0)c |
(1.1–200.0)a | (2.4–10.3) |
(0.1–254.4)c |
| Hb, g/l | 79.0 | 105.0 | 92.0 | 80.0 | 101.0 | 90.0 |
|
|
(34.0–149.0)a | (64.0–155.0) |
(45.0–148.0)c |
(34.0–148.0)a | (64.0–140.0) |
(45.0–145.0)c |
| PLT,
×109/l | 30.0 | 180.0 | 32.0 | 41.0 | 143.0 | 32.0 |
|
|
(5.0–235.0)a | (6.0–460.0) |
(4.0–167.0)c |
(6.0–235.0)a | (21.0–462.0) |
(6.0–167.0)c |
| PT, sec | 15.6 | 13.7 | 14.6 | 14.2 | 13.3 | 14.1 |
|
|
(12.5–33.6)b | (11.7–18.1) |
(11.9–22.8)d | (12.5–21.6) | (11.7–18.1) | (12.1–21.4) |
| aPTT, sec | 38.8 | 38.8 | 39.8 | 38.1 | 38.4 | 39.3 |
|
| (26.6–75.5) | (29.1–58.8) |
(25.9–59.6) | (30.0–75.5) | (29.4–57.8) | (25.9–55.5) |
| FIB, g/l | 3.5 | 3.7 | 2.9 | 3.77 | 3.4 | 3.3 |
|
|
(0.2–9.1)a | (0.6–8.5) |
(0.8–8.4)c |
(0.8–8.5) | (0.6–8.5) | (1.26–7.39) |
| D-dimer, mg/l | 4.2 | 1.2 | 2.7 | 2.2 | 0.6 | 1.6 |
|
|
(0.5–47.0)a | (0.1–7.2) |
(0.3–40.0)c |
(0.5–10.4)a | (0.1–1.6) |
(0.3–17.4)c |
| LDH, units/l | 385.0 | 198.0 | 335.0 | 395.0 | 173.0 | 376.0 |
|
|
(140.0–2,894.0)a | (29.0–405.0) |
(88.0–4,919.0)c |
(156.0–2,405.0)a | (69.0–293.0) |
(88.0–4,919.0)c |
Plasma levels of D-dimer and LDH
levels in all subtypes of AL at various stages of disease
In the AML-M1 group (Table II), LDH (P=0.030) and D-dimer
(P=0.020) plasma levels were significantly increased at the initial
onset of AL compared with during CR. The plasma levels of D-dimer
and LDH were significantly increased in the relapsed group compared
with the CR group (P=0.010 and P=0.020, respectively), which were
higher during relapse compared with at initial onset of AL. In the
AML-M2 group, LDH (P=0.008 and P=0.010) and D-dimer (P=0.008 and
P=0.007) plasma levels were significantly increased in the initial
onset and relapsed groups compared with CR; LDH plasma levels were
increased in patients with initial onset of M2 compared with
relapsed patients. The highest values of D-dimer were observed in
AML-M3 patients. D-dimer plasma levels were significantly increased
at initial onset of APL compared with during CR, and significantly
increased during relapse compared with CR. Plasma LDH levels were
significantly greater in patients at the initial onset and in
patients with relapsed AL compared with patients achieving CR
(P=0.009 and P=0.007, respectively). In the AML-M4 patients group,
D-dimer plasma levels were significantly increased in patients with
initial onset and patients with relapsed AL (P=0.010 and P=0.030,
respectively), but not with CR. LDH levels in AML-M4 patients were
significantly increased at initial onset and in relapsed AL
compared with at CR. In the AML-M5 patients group, D-dimer (P=0.030
and P=0.040) and LDH (P=0.020 and P=0.040) plasma levels
significantly increased in the relapsed group and initial onset of
disease compared with the CR group. In the AML-M6 patient group,
D-dimer plasma levels increased during relapsed AL (P=0.030), but
not at initial onset of AL compared with patients with CR. Plasma
LDH levels were significantly greater in patients with initial
onset and relapsed AL compared with CR (P=0.030 and P=0.020,
respectively). In the ALL patient group, D-dimer plasma levels were
significantly increased in the initial onset and relapsed groups
compared with the CR group, but were higher at the initial onset of
ALL compared with during relapse. LDH plasma levels significantly
increased at initial onset and during relapse compared with
patients achieving CR (P=0.005 and P=0.002, respectively).
| Table II.Clinical parameters of patients with
various stages of AL subtypes. |
Table II.
Clinical parameters of patients with
various stages of AL subtypes.
|
|
| D-dimer (median,
range) | LDH (median,
range) |
|---|
|
|
|
|
|
|---|
| Subtype | No. of cases | Initial onset | CR | Relapse | Initial onset | CR | Relapse |
|---|
| M1 | 44 | 1.8 | 1.0 | 1.9 | 359.0 | 166.0 | 424.0 |
|
|
|
(0.7–18.0)b | (0.2–3.0) |
(0.9–40.0)d |
(156.0–704.0)b | (77.0–400.0) |
(100.0–588.0)d |
| M2 | 26 | 2.6 | 1.8 | 3.2 | 432.0 | 176.0 | 260.0 |
|
|
|
(0.9–4.2)a | (0.3–3.6) |
(0.9–6.0)c |
(217.0–760.0)a | (69.0–334.0) |
(163.0–984.0)d |
| M3 | 32 | 29.0 | 1.0 | 24 | 253.0 | 200.0 | 297.0 |
|
|
|
(1.3–47.0)a | (0.3–7.2) |
(0.5–37.0)c |
(180.0–929.0)a | (140.0–405.0) |
(110.0–1,200.0)c |
| M4 | 36 | 3.3 | 1.4 | 2.4 | 484.0 | 192.0 | 363.0 |
|
|
|
(1.2–34.0)b | (0.1–5.3) |
(1.0–13.5)d |
(140.0–2,405.0)b |
(29.0–334.0) |
(167.0–2,584.0)c |
| M5 | 20 | 2.3 | 0.6 | 1.7 | 419.0 | 154.0 | 263.0 |
|
|
|
(1.0–3.7)b | (0.1–1.9) |
(0.3–3.4)d |
(162.0–1,725.0)b | (76.0–287.0) |
(88.0–569.0)d |
| M6 | 6 | 0.5 | 0.4 | 1.6 | 379.0 | 148.0 | 409.0 |
|
|
| (0.5–1.0) | (0.2–1.1) |
(1.5–1.8)d |
(240.0–644.0)b | (128.0–187.0) |
(376.0–424.0)d |
| ALL | 40 | 4.1 | 1.2 | 2.1 | 496.0 | 255.0 | 630.0 |
|
|
|
(0.7–24.0)a | (0.1–3.5) |
(0.5–25.6)d |
(214.0–2,894.0)a | (114.0–400.0) |
(119.0–4,919.0)c |
Serum LDH levels were elevated in the majority of AL
patients following initial diagnosis and in relapsed patients;
however, there does not appear to be a correlation between
increased LDH levels and blood routine parameters in AL patients.
Increased D-dimer concentrations demonstrated no correlation with
any blood routine parameters in AL patients.
Discussion
Despite the outstanding advances made over the past
decade regarding our knowledge of AL, AL relapse following routine
conventional-dose chemotherapy remains to be associated with a
dismal prognosis (3–6,8,10). D-dimers are a sensitive measure of
endogenous fibrinolysis and are used to screen for deep vein
thrombosis (19–24). Elevated LDH levels have frequently
been observed in animal and human malignancies (15,25,26); in
addition, there appears to be a strong correlation between disease
activity and tumor mass (27). The
association, pathogenesis and significance of D-dimers and LDH
levels with relapse within the subtypes of AML and ALL are
currently unknown. A clear understanding of the associations
between these parameters and relapsed AL patients requires
additional research.
Coagulation disorders are frequently observed in APL
and can also occur in other AL subtypes (28–30). The
pathogenic mechanism underlying the blood coagulation disorder in
these patients is complex. The levels of D-dimer complex generally
reflect the functional state of the clotting and fibrinolysis
systems and support the existence of a hypercoagulable state
(19,20,31,32).
In the present study, during the initiation of AL,
PT was found to be significantly prolonged (P=0.020), plasma levels
of FIB were significantly decreased (P=0.009), the levels of
D-dimer were elevated in all subtypes of AML and ALL, and the
highest levels of D-dimer were found in AML-M3 (Tables I and II); however, there was no significant
difference in aPTT between patients with initial onset and those
with CR, or between relapse and CR. When coagulation data results
were eliminated in patients with APL, plasma PT, aPTT and FIB
levels were not significantly increased at the initial onset of AL
or during AL relapse compared to patients with CR. The results of
the present study indicate that the determination of D-dimer levels
may be useful for predicting the probability of relapse during
chemotherapy, as the PT, aPTT and FIB tests were not reliable
markers of AL relapse.
Increased D-dimer levels at initial onset, which
further increased during relapse, strongly suggest a
hypercoagulable state, with secondary activation of fibrinolysis in
the majority of patients (33,34).
Activation of coagulation and secondary activation of fibrinolysis
are likely to occur continuously and simultaneously throughout
circulation (20,24,34). The
activation of coagulation is most likely associated with the
leukemic cells circulating in the blood, which may contain
procoagulants, and the content of these substances depends on the
leukemia subtype (35,36). These substances may be released into
the blood from disintegrating cells during relapse.
Tanaka et al (35) confirmed that the development of
disseminated intravascular coagulation in patients with AL prior to
chemotherapy is associated with the presence of tissue factor (TF)
on the surface of the leukemic cells. TF is a major procoagulant
that initiates blood coagulation in vivo and is the membrane
protein receptor for factor VII. The resulting factor VIIa
activates factors IX and X, leading to thrombin generation and
fibrin formation (35,37,38). The
TF gene is expressed in cells from patients with AL.
In the present study, cells from AML patients
expressed particularly high VII activity; these levels become
essentially undetectable when patients are in CR. Other
procoagulant mediators, including tumor necrosis factor α (39,40),
cysteine proteinase (41),
interferon-γ (40), asinterleukin-1
(42) and vascular permeability
factor (43), are regarded as
indirect procoagulants as they initiate coagulation by inducing TF
in endothelial cells and monocytes (44). In addition, natural apoptosis may
contribute to thrombogenesis in AL via the release of
microparticles from the damaged leukemic cells (35). Coagulation disorders may also occur
due to leukemia-associated complications, including infection or
organic impairment (45).
Notably, for patients that achieved CR following the
induction of chemotherapy, D-dimer levels did not return to a
normal value. The increased D-dimer levels during CR following
chemotherapy treatment suggest a hypercoagulable state with
secondary activation of fibrinolysis. Velasco et al
(46). Observed an increase in the
D-dimer level during treatment in patients with AML. In the present
study, the results showed that the LDH levels were moderately
elevated in the majority of AL patients with the exception of the
CR phase, irrespective of cell type. Significantly elevated levels
were recorded in the majority of patients with ALL but there was no
significant difference in serum LDH levels between AML and ALL
patients during relapse; in addition, no significant difference was
found at initial onset of AL and during relapse.
In patients with increased levels of LDH at
diagnosis, AL relapse was not found to lead to significant
elevation. LDH activity reflects increased glycolysis in the
cytoplasm of malignant cells accompanied by a high metabolic rate
(15,25). The increase of serum LDH activity may
be due to thrombotic microangiopathy, intravascular hemolysis or
tumor lysis (25,26). Certain values from the ALL patients
were remarkably high (Table II), and
the majority of these patients had a high WBC counts during
relapse. This phenomenon is likely due to the correlation between
LDH levels and the number of circulating ALL blasts during relapse
(47). Cumulative evidence indicates
that serum LDH levels can be a good and reliable prognostic marker
of ALL patients (48–50), suggesting an association between LDH
levels and relapse.
Although D-dimer and LDH levels have been shown to
be elevated in all subtypes of AML and ALL, none of these
parameters provide diagnostic specificity. In the present study, a
significant change in routine hematological parameters was
indicated in patients with relapsed AL, which is consistent with
previous findings (51,52). The most important and most common
associated risk factors for the hematological relapse of AL are
thrombocytopenia, leukocyte count and lower hemoglobin, which is
associated with the proliferating leukemic clone (53,54).
Ambulatory monitoring of D-dimer, LDH, and routine hematological
parameters are recommended for the assessment of relapse in AL
patients.
In conclusion, the present study demonstrated that
D-dimer and LDH plasma levels were significantly increased at
initial onset and during relapse in AL patients compared to those
with CR. D-dimer and LDH levels may be useful for predicting AL
relapse; therefore, the present study recommends that monitoring
D-dimer and LDH for the assessment of AL relapse.
Acknowledgements
The authors gratefully acknowledge the patients for
participating in the present study, and thank Dr Xiao Bo Nie for
the critical reading of this manuscript.
References
|
1
|
Deschler B and Lübbert M: Acute myeloid
leukemia: Epidemiology and etiology. Cancer. 107:2099–2107. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lo-Coco F, Ammatuna E, Montesinos P and
Sanz MA: Acute promyelocytic leukemia: Recent advances in diagnosis
and management. Semin Oncol. 35:401–409. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Inagaki J, Fukano R, Noguchi M, Kurauchi
K, Tanioka S and Okamura J: Hematopoietic stem cell transplantation
following unsuccessful salvage treatment for relapsed acute
lymphoblastic leukemia in children. Pediatr Blood Cancer.
62:674–679. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cui L, Gao C, Zhang RD, Jiao Y, Li WJ,
Zhao XX, Liu SG, Yue ZX, Zheng HY, Deng GR, et al: Low expressions
of ARS2 and CASP8AP2 predict relapse and poor prognosis in
pediatric acute lymphoblastic leukemia patients treated on China
CCLG-ALL 2008 protocol. Leuk Res. 39:115–123. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Arakawa Y, Koh K, Aoki T, Kubota Y, Oyama
R, Mori M, Hayashi M and Hanada R: Clofarabine-based combination
chemotherapy for relapse and refractory childhood acute
lymphoblastic leukemia. Rinsho Ketsueki. 55:2316–2319.
2014.PubMed/NCBI
|
|
6
|
Bruedigam C, Bagger FO, Heidel FH, Kuhn
Paine C, Guignes S, Song A, Austin R, Vu T, Lee E, Riyat S, et al:
Telomerase inhibition effectively targets mouse and human AML stem
cells and delays relapse following chemotherapy. Cell Stem Cell.
15:775–790. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ilyas AM, Ahmad S, Faheem M, Naseer MI,
Kumosani TA, Al-Qahtani MH, Gari M and Ahmed F: Next generation
sequencing of acute myeloid leukemia: Influencing prognosis. BMC
Genomics. 16(Suppl 1): S52015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Itzykson R, Thépot S, Berthon C, Delaunay
J, Bouscary D, Cluzeau T, Turlure P, Prébet T, Dartigeas C,
Marolleau JP, et al: Azacitidine for the treatment of relapsed and
refractory AML in older patients. Leuk Res. 39:124–130. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rashidi A and Cashen AF: A cytogenetic
model predicts relapse risk and survival in patients with acute
myeloid leukemia undergoing hematopoietic stem cell transplantation
in morphologic complete remission. Leuk Res. 39:77–81. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Martelli MF, Di Ianni M, Ruggeri L,
Falzetti F, Carotti A, Terenzi A, Pierini A, Massei MS, Amico L,
Urbani E, et al: HLA-haploidentical transplantation with regulatory
and conventional T-cell adoptive immunotherapy prevents acute
leukemia relapse. Blood. 124:638–644. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Byrd JC, Mrozek K, Dodge RK, Carroll AJ,
Edwards CG, Arthur DC, Pettenati MJ, Patil SR, Rao KW, Watson MS,
et al: Cancer and Leukemia Group B (CALGB 8461): Pretreatment
cytogenetic abnormalities are predictive of induction success,
cumulative incidence of relapse, and overall survival in adult
patients with de novo acute myeloid leukemia: Results from Cancer
and Leukemia Group B (CALGB 8461). Blood. 100:4325–4336. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thakkar SG, Fu AZ, Sweetenham JW, McIver
ZA, Mohan SR, Ramsingh G, Advani AS, Sobecks R, Rybicki L, Kalaycio
M and Sekeres MA: Survival and predictors of outcome in patients
with acute leukemia admitted to the intensive care unit. Cancer.
112:2233–2240. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Benyo M, Flasko T, Molnar Z, Kerenyi A,
Batta Z, Jozsa T and Harsfalvi J: Follow-up of thrombin generation
after prostate cancer surgery: Global test for increased
hypercoagulability. PLoS One. 7:e512992012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Diao D, Zhu K, Wang Z, Cheng Y, Li K, Pei
L and Dang C: Prognostic value of the D-dimer test in oesophageal
cancer during the perioperative period. J Surg Oncol. 108:34–41.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kachel P, Trojanowicz B, Sekulla C,
Prenzel H, Dralle H and Hoang-Vu C: Phosphorylation of pyruvate
kinase M2 and lactate dehydrogenase A by fibroblast growth factor
receptor 1 in benign and malignant thyroid tissue. BMC Cancer.
15:1402015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Park HY, Suh GY, Jeon K, Koh WJ, Chung MP,
Kim H, Kwon OJ, Kim K, Jang JH, Jung CW, et al: Outcome and
prognostic factors of patients with acute leukemia admitted to the
intensive care unit for septic shock. Leuk Lymphoma. 49:1929–1934.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bennett JM, Catovsky D, Daniel MT,
Flandrin G, Galton DA, Gralnick HR and Sultan C: Criteria for the
diagnosis of acute leukemia of megakaryocyte lineage (M7). A report
of the French-American-British Cooperative Group. Ann Int Med.
103:460–462. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vardiman JW, Thiele J, Arber DA, Brunning
RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM,
Hellström-Lindberg E, Tefferi A and Bloomfield CD: The 2008
revision of the World Health Organization (WHO) classification of
myeloid neoplasms and acute leukemia: Rationale and important
changes. Blood. 114:937–951. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Danese E, Montagnana M, Cervellin G and
Lippi G: Hypercoagulability, D-dimer and atrial fibrillation: An
overview of biological and clinical evidence. Ann Med. 46:364–371.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee K, Kim JE, Kwon J, Kim I, Yoon SS,
Park S, Han KS and Kim HK: Poor prognosis of hypocoagulability
assessed by thrombin generation assay in disseminated intravascular
coagulation. Blood Coagul Fibrinolysis. 25:241–247. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sartori M, Migliaccio L, Favaretto E, Cini
M, Legnani C, Palareti G and Cosmi B: D-dimer for the diagnosis of
upper extremity deep and superficial venous thrombosis. Thromb Res.
135:673–678. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
van der Hulle T, Tan M, den Exter PL, Mol
GC, del Iglesias Sol A, van de Ree MA, Huisman MV and Klok FA:
Selective D-dimer testing for the diagnosis of acute deep vein
thrombosis: A validation study. J Thromb Haemost. 11:2184–2186.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yoon CW, Kim SJ, Bang OY, Chung CS, Lee KH
and Kim GM: Premorbid warfarin use and lower D-dimer levels are
associated with a spontaneous early improvement in an atrial
fibrillation-related stroke. J Thromb Haemost. 10:2394–2396. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sartori M, Cosmi B, Legnani C, Favaretto
E, Valdré L, Guazzaloca G, Rodorigo G, Cini M and Palareti G: The
Wells rule and D-dimer for the diagnosis of isolated distal deep
vein thrombosis. J Thromb Haemost. 10:2264–2269. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Han X, Sheng X, Jones HM, Jackson AL,
Kilgore J, Stine JE, Schointuch MN, Zhou C and Bae-Jump VL:
Evaluation of the anti-tumor effects of lactate dehydrogenase
inhibitor galloflavin in endometrial cancer cells. J Hematol Oncol.
8:22015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Augoff K, Hryniewicz-Jankowska A and
Tabola R: Lactate dehydrogenase 5: An old friend and a new hope in
the war on cancer. Cancer Lett. 358:1–7. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Dowling P, Pollard D, Larkin A, Henry M,
Meleady P, Gately K, O'Byrne K, Barr MP, Lynch V, Ballot J, et al:
Abnormal levels of heterogeneous nuclear ribonucleoprotein A2B1
(hnRNPA2B1) in tumour tissue and blood samples from patients
diagnosed with lung cancer. Mol Biosyst. 11:743–752. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Choudhry A and DeLoughery TG: Bleeding and
thrombosis in acute promyelocytic leukemia. Am J Hematol.
87:596–603. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chang H, Kuo MC, Shih LY, Dunn P, Wang PN,
Wu JH, Lin TL, Hung YS and Tang TC: Clinical bleeding events and
laboratory coagulation profiles in acute promyelocytic leukemia.
Eur J Haematol. 88:321–328. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Asakura H, Takahashi H, Tsuji H,
Matsushita T, Ninomiya H, Honda G, Mimuro J, Eguchi Y, Kitajima I
and Sakata Y: Post-marketing surveillance of thrombomodulin alfa, a
novel treatment of disseminated intravascular coagulation-safety
and efficacy in 1,032 patients with hematologic malignancy. Thromb
Res. 133:364–370. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Mego M, Zuo Z, Gao H, Cohen EN, Giordano
A, Tin S, Anfossi S, Jackson S, Woodward W, Ueno NT, et al:
Circulating tumour cells are linked to plasma D-dimer levels in
patients with metastatic breast cancer. Thromb Haemost.
113:593–598. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Gomes M and Khorana AA: Risk assessment
for thrombosis in cancer. Semin Thromb Hemost. 40:319–324. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yanada M, Matsushita T, Suzuki M, Kiyoi H,
Yamamoto K, Kinoshita T, Kojima T, Saito H and Naoe T: Disseminated
intravascular coagulation in acute leukemia: Clinical and
laboratory features at presentation. Eur J Haematol. 77:282–287.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hess EP and Sztajnkrycer MD: Images in
emergency medicine. Acute leukemia with blast crisis, disseminated
intravascular coagulation, and intraparenchymal hemorrhage. Ann
Emerg Med. 46:314–322. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tanaka M and Yamanishi H: The expression
of tissue factor antigen and activity on the surface of leukemic
cells. Leuk Res. 17:103–111. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jácomo RH, Santana-Lemos BA, Lima AS,
Assis PA, Lange AP, Figueiredo-Pontes LL, Oliveira LO, Bassi SC,
Benício MT, Baggio MS, et al: Methionine-induced
hyperhomocysteinemia reverts fibrinolytic pathway activation in a
murine model of acute promyelocytic leukemia. Blood. 120:207–213.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Marchetti M, Russo L, Balducci D and
Falanga A: All trans-retinoic acid modulates the procoagulant
activity of human breast cancer cells. Thromb Res. 128:368–374.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Marchetti M, Diani E, ten Cate H and
Falanga A: Characterization of the thrombin generation potential of
leukemic and solid tumor cells by calibrated automated
thrombography. Haematologica. 97:1173–1180. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ohkawara H, Ishibashi T, Sugimoto K, Ikeda
K, Ogawa K and Takeishi Y: Membrane type 1-matrix
metalloproteinase/Akt signaling axis modulates TNF-α-induced
procoagulant activity and apoptosis in endothelial cells. PLoS One.
9:e1056972014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Poovassery JS, Sarr D, Smith G, Nagy T and
Moore JM: Malaria-induced murine pregnancy failure: Distinct roles
for IFN-gamma and TNF. J Immunol. 183:5342–5349. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
de Menezes YA, Félix-Silva J, da
Silva-Júnior AA, Rebecchi IM, de Oliveira AS, Uchoa AF and
Fernandes-Pedrosa Mde F: Protein-rich fraction of Cnidoscolus urens
(L.) Arthur leaves: Enzymatic characterization and procoagulant and
fibrinogenolytic activities. Molecules. 19:3552–3569. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Gansler J, Preissner KT and Fischer S:
Influence of proinflammatory stimuli on the expression of vascular
ribonuclease 1 in endothelial cells. FASEB J. 28:752–760. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zucker S, Mirza H, Conner CE, Lorenz AF,
Drews MH, Bahou WF and Jesty J: Vascular endothelial growth factor
induces tissue factor and matrix metalloproteinase production in
endothelial cells: Conversion of prothrombin to thrombin results in
progelatinase A activation and cell proliferation. Int J Cancer.
75:780–786. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hawiger J, Veach RA, Liu XY, Timmons S and
Ballard DW: IkappaB kinase complex is an intracellular target for
endotoxic lipopolysaccharide in human monocytic cells. Blood.
94:1711–1716. 1999.PubMed/NCBI
|
|
45
|
Ma J, Duffy MR, Deng L, Dakin RS, Uil T,
Custers J, Kelly SM, McVey JH, Nicklin SA and Baker AH:
Manipulating adenovirus hexon hypervariable loops dictates immune
neutralisation and coagulation factor X-dependent cell interaction
in vitro and in vivo. PLoS Pathog. 11:e10046732015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Velasco F, Torres A, Rojas R, Alvarez MA,
Gomez P and Castillo D: Increase in the D-dimer levels during
treatment in patients with acute myelogenous leukemia. Haemostasis.
22:117–123. 1992.PubMed/NCBI
|
|
47
|
Cortelazzo S, Ponzoni M, Ferreri AJ and
Hoelzer D: Lymphoblastic lymphoma. Crit Rev Oncol Hematol.
79:330–343. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Rao D, Ghalaut VS, Ghalaut PS and Rao S:
Case series: CSF LDH, proteins and electrolyte levels in patients
of acute lymphocytic leukemia. Clin Chim Acta. 413:1045–1048. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Thomas X, Danaïla C, Le QH, Sebban C,
Troncy J, Charrin C, Lhéritier V, Michallet M, Magaud JP and Fiere
D: Long-term follow-up of patients with newly diagnosed adult acute
lymphoblastic leukemia: A single institution experience of 378
consecutive patients over a 21-year period. Leukemia. 15:1811–1822.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yeh CH, Tseng R, Hannah A, Estrov Z, Estey
E, Kantarjian H and Albitar M: Clinical correlation of circulating
heat shock protein 70 in acute leukemia. Leuk Res. 34:605–609.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Suvajdžić N, Cvetković Z, Dorđević V,
Kraguljac-Kurtović N, Stanisavljević D, Bogdanović A, Djunić I,
Colović N, Vidović A, Elezović I and Tomin D: Prognostic factors
for therapy-related acute myeloid leukaemia (t-AML)-a single centre
experience. Biomed Pharmacother. 66:285–292. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Litzow MR, Othus M, Cripe LD, Gore SD,
Lazarus HM, Lee SJ, Bennett JM, Paietta EM, Dewald GW, Rowe JM, et
al: Failure of three novel regimens to improve outcome for patients
with relapsed or refractory acute myeloid leukaemia: A report from
the Eastern Cooperative Oncology Group. Br J Haematol. 148:217–225.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Shiozawa Y, Takita J, Kato M, Sotomatsu M,
Koh K, Ida K and Hayashi Y: Prognostic significance of leukopenia
in childhood acute lymphoblastic leukemia. Oncol Lett. 7:1169–1174.
2014.PubMed/NCBI
|
|
54
|
Hossain MJ, Xie L and Caywood EH:
Prognostic factors of childhood and adolescent acute myeloid
leukemia (AML) survival: Evidence from four decades of US
population data. Cancer Epidemiol. 39:720–726. 2015. View Article : Google Scholar : PubMed/NCBI
|