Introduction
α-fetoprotein (AFP) is a protein that is mainly
formed by the liver and yolk sac during fetal development, and to a
lesser extent, in the fetal gastrointestinal tract (1,2). AFP is
detected in fetal serum and the highest serum levels appear between
12 and 15 weeks of gestation, decreasing to normal levels ~1 year
later (3,4). High AFP expression detected in the serum
of adults is always associated with liver disease and yolk sac
tumors (2–6). AFP-secreting carcinoma is an
increasingly recognized tumor, and has been reported in the
Japanese literature. Increased AFP expression was detected in
malignant tumors of various organs, such as the stomach, lung,
pancreas, colon bladder and ovary (7–13). The
stomach is one of the most common locations of these tumors
(10), whereas AFP-producing
esophageal cancer (AFP-EC) is rare (14–17).
AFP-producing tumors are usually diagnosed at an advanced stage and
have a poor prognosis (18–20).
There are extremely few case reports of
AFP-producing esophageal cancers (14–17).
Wahren et al (21) reported
that 18 patients (33%) had elevated serum AFP levels out of 55
patients with esophageal carcinoma, and 5 patients with esophageal
carcinoma had an AFP level of 320 ng/ml. The serum AFP levels in
patients with adenocarcinoma were evidently increased compared with
the levels in patients with squamous cell carcinoma. The serum AFP
level can be measured, which may be a useful index for monitoring
clinical status, evaluating cure, recurrence or metastases. The
serum AFP levels in the patient reported by Kobayashi et al
(17) decreased to within normal
limits following surgery. This indicates that surgery and
chemotherapy are useful therapeutic methods for patients with
esophageal carcinoma. It was reported by Wahren et al
(21) that there are no significant
changes in serum AFP levels subsequent to radiation therapy.
AFP-producing upper gastrointestinal tumors are considered to be
resistant to chemotherapy (22). The
clinical course of numerous patients with AFP-producing esophageal
carcinomas is notable for the development of hematogenous
metastases to the liver, lung, spleen and brain. The prognosis of
these patients is extremely poor. Shimakawa et al (23) and Sawada et al (24) each reported cases of patients that
succumbed after 1 year and 4 months, respectively. A case was also
reported by Kobayashi et al (17) in which the patient had a satisfactory
clinical course for >3 years, without further elevation of AFP
levels or evidence of metastases on imaging studies.
Due to the poor prognosis of AFP-producing tumors,
it is important to make an accurate diagnosis in clinical
treatment. In the present study, a case of squamous cell carcinoma
that was misdiagnosed as an AFP-producing esophageal carcinoma is
reported.
Case report
A 50-year-old woman presented to a local doctor in
August 2014 with a 20-day history of progressive dysphagia. A
radiographic examination of the upper gastrointestinal tract
revealed an esophageal mass that was clinically similar to
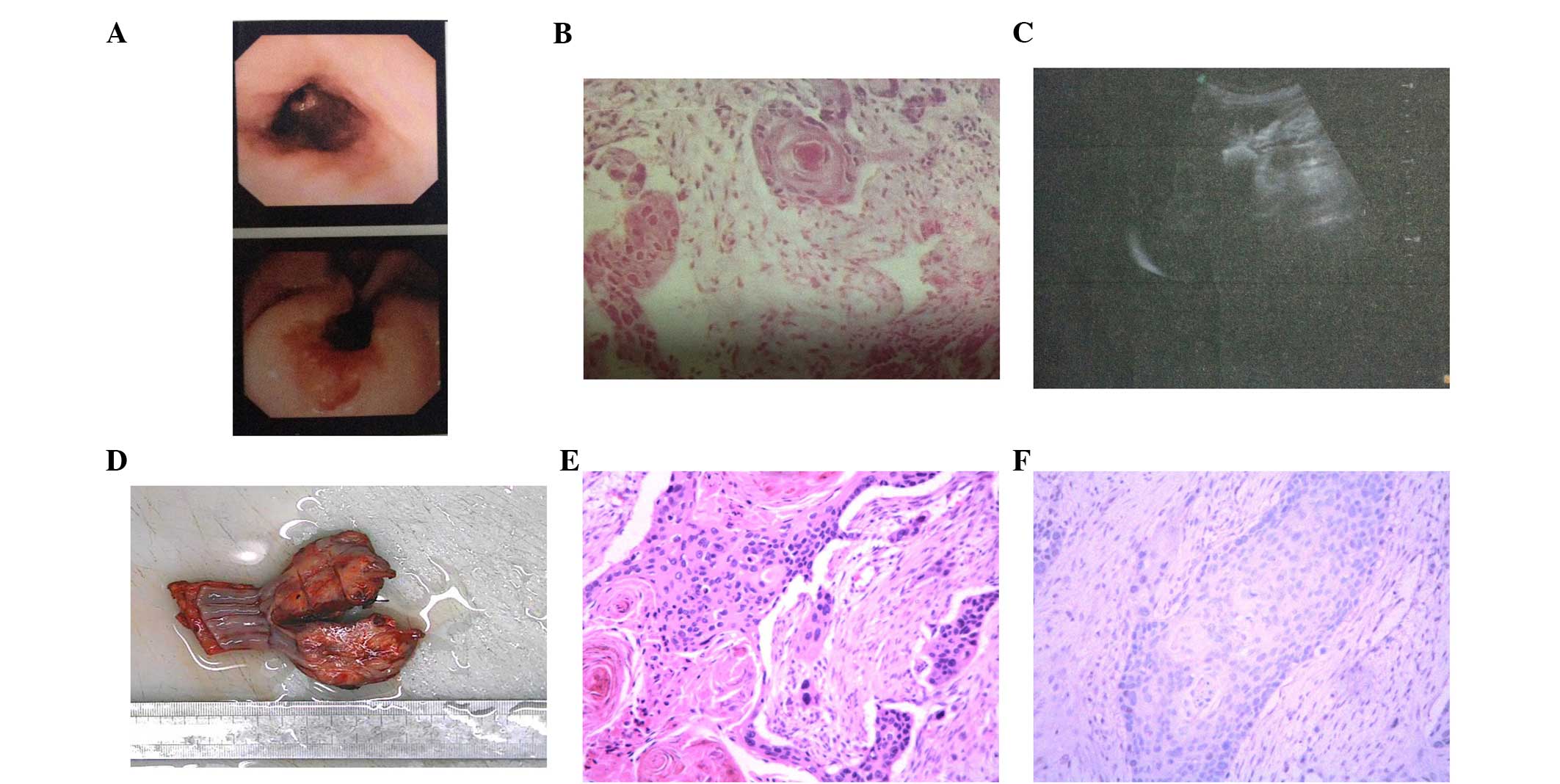
esophageal cancer. An endoscopy revealed an elevated tumor in the
middle and lower segment of esophagus (Fig. 1A). Biopsies taken from the area 3 days
subsequent to presentation revealed a squamous cell carcinoma
(Fig. 1B). The patient received one
cycle of chemotherapy with oxaliplatin (140 mg; day 1),
fluorouracil (1.0 g; days 2–6) and calcium folinate (0.3 g; days
2–6). However, the progressive dysphagia symptom had worsened due
to disease progression. For additional examination and treatment,
the patient was referred to Qianfoshan Hospital Affiliated to
Shandong University (Jinan, Shandong, China) in November 2014. A
chest computed tomography (CT) scan showed thickening of the wall
of the esophagus, corresponding regions of luminal stenosis and
massive lymph node swelling around the lesser curvature of the
esophagus. No primary or metastatic tumors were observed. An
abdominal ultrasound was performed and cystic low density measuring
5×4 mm was identified, and no metastases in the liver were
identified (Fig. 1C). The boundary of
the focal low density was clear, which indicated a clinical
diagnosis of liver cyst. A laboratory investigation showed that the
serum AFP levels of the patient were elevated to 18.97 ng/ml
(normal range, <12 ng/ml), the serum carcinoembryonic antigen
level was 1.62 ng/ml (normal range, <5.0 ng/ml), and squamous
cell carcinoma (SCC) antigen level was 12.30 ng/ml (normal range,
1.5 ng/ml). Results of other laboratory tests, including and liver
function tests, were all within normal limits. These laboratory
investigation findings combined with the aforementioned
pathological diagnosis supported a diagnosis of AFP-producing
squamous cell carcinoma of the esophagus.
A radical esophagectomy was performed on December 5,
2014. The surgically resected specimen showed an elevated tumor
(5.0 cm at the maximal diameter) in the middle and lower segment of
the esophagus (Fig. 1D).
Microscopically, the tumor was a moderately differentiated squamous
cell carcinoma invading the area of serous layer, with no hepatoid
features (Fig. 1E).
Immunohistochemistry showed that the cells were diffusely negative
for AFP (Fig. 1F). One lymph node
beside the esophagus showed massive swelling. The tumor was
diagnosed as stage IIIA (T3N1M0), according to the American Joint
Committee on Cancer guidelines (25).
Postoperatively, the patient was treated with four
cycles of nedaplatin (200 mg; day 1, repeated on day 21) plus
gemcitabine (1,500 mg; days 1 and 8, repeated on day 21), and has
been free of recurrence for 4 months. However, the serum AFP levels
had increased between 13.39 and 17.39 ng/ml, and had not decreased
to the normal range. These findings show that the increase in AFP
levels was not associated with esophageal cancer.
Written informed consent was obtained from the
patient for publication of the present study and any accompanying
images.
Discussion
AFP is a type of protein that is mainly formed by
the liver and yolk sac during fetal development, and to a lesser
extent, in the fetal gastrointestinal tract (1,2). AFP is
detected in the fetal serum and the highest serum levels majority
of appear between 12 and 15 weeks of pregnancy and ~1 year later
the levels decrease to the normal range (3,4). High AFP
levels are detected in the serum with liver disease and yolk sac
tumors (2–6). AFP-secreting carcinoma is an
increasingly recognized tumor, and the main part in reported in the
Japanese literature. AFP rising was detected in malignant tumors of
different organs, for example, the stomach, lung, pancreas, colon
bladder, and ovary (7–13). The stomach is one of the most common
locations of such tumors (10),
whereas AFP-EC is rare.
In tumors, the molecular mechanism associated with
AFP expression is poorly understood. In upper gastrointestinal
tumors, it proposed that the increase in AFP levels is due to an
absence of AT motif binding factor I, which is a transcription
factor that binds to the AFP-regulatory element and downregulates
the AFP gene (26). In AFP-producing
tumors, human albumin mRNA in situ hybridization showed
cytoplasmic positivity and is considered to be additional evidence
of hepatocellular differentiation of these tumors (27). Previously, certain factors associated
with mitosis, cell movement, proliferative activity and tumor
progression, such as hepatocyte growth factor (HGF), Ki-67 and its
receptor, vascular endothelial growth factor (VEGF), and c-Met and
its isoform VEGF-C, were found to be highly expressed in
AFP-producing tumors, and these factors may be associated with the
poor prognosis of this tumor (28–30).
Furthermore, AFP-producing upper gastrointestinal tumors are
considered to be resistant to chemotherapy (22).
P-glycoprotein (PGP), which is associated with the
phenotypic expression of multidrug resistance in cancerous tissue,
was found to be overexpressed in AFP-producing tumors. Therefore,
the observed drug resistance and frequent recurrence may be
explained by the presence of PGP (31). Chang et al (22) proposed that even if no metastasis is
present preoperatively, liver metastasis frequently occur within a
year of surgery. In addition, AFP-producing tumors were found to
have an increased likelihood of expression of
chemoresistance-associated proteins. However, chemotherapy has been
reported to be effective in several patients (18–20,32). Due
to the poor prognosis of this type of tumor, accurate diagnosis is
necessary, and clinicians should consider more effective treatments
of this particular type of AFP-producing tumor in patients with
good performance status, and recommend for curative resection and
further chemotherapy.
Glossary
Abbreviations
Abbreviations:
|
AFP
|
α-fetoprotein
|
|
AFP-EC
|
AFP-producing esophageal cancer
|
|
CT
|
computed tomography
|
|
VEGF
|
vascular endothelial growth factor
|
|
PGP
|
P-glycoprotein
|
References
|
1
|
Gitlin D, Pericelli A and Gitlin GM:
Synthesis of -fetoprotein by liver, yolk, sac and gastrointestinal
tract of the human conceptus. Cancer Res. 32:979–982.
1972.PubMed/NCBI
|
|
2
|
Babali A, Cakal E, Purnak T, Bıyıkoğlu I,
Cakal B, Yüksel O and Köklü S: Serum α-fetoprotein levels in liver
steatosis. Hepatol Int. 3:551–555. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mizejewski GJ: Levels of alpha-fetoprotein
during pregnancy and early infancy in normal and disease states.
Obstet Gynecol Surv. 58:804–826. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Breborowicz J, Mackiewicz A and
Breborowicz D: Microheterogeneity of alpha-fetoprotein in patient
serum as demonstrated by lectin affino-electrophoresis. Scand J
Immunol. 14:15–20. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ezaki T, Yukaya H, Ogawa Y, Chang YC and
Nagasue N: Evaluation of alpha-fetoprotein level without evidence
of recurrence after hepatectomy for hepatocellular carcinoma.
Cancer. 61:1880–1883. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ganjei P, Nadji M, Albores-Saavedra J and
Morales AR: Histologic markers in primary and metastatic tumors of
the liver. Cancer. 62:1994–1998. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yamagata T, Yamagata Y, Nakanishi M,
Matsunaga K, Minakata Y and Ichinose M: A case of primary lung
cancer producing alpha-fetoprotein. Can Respir J. 11:504–506. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hamanaka W, Yoneda S, Shirakusa T,
Shirahama H, Tashiro Y, Iwasaki A, Shiraishi T and Tsuru H:
Alpha-fetoprotein (AFP)-producing adrenocortical carcinoma-long
survival with various therapeutic strategies including a lung
resection: Report of a case. Surg Today. 38:275–278. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Matsueda K, Yamamoto H, Yoshida Y and
Notohara K: Hepatoid carcinoma of the pancreas producing protein
induced by vitamin K absence or antagonist II (PIVKA-II) and
alpha-fetoprotein (AFP). J Gastroenterol. 41:1011–1019. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kinjo T, Taniguchi H, Kushima R, Sekine S,
Oda I, Saka M, Gotoda T, Kinjo F, Fujita J and Shimoda T:
Histologic and immunohistochemical analyses of
α-fetoprotein-producing cancer of the stomach. Am J Surg Pathol.
36:56–65. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cappetta A, Bergamo F, Mescoli C, Lonardi
S, Rugge M and Zagonel V: Hepatoid adenocarcinoma of the colon:
What should we target? Pathol Oncol Res. 18:93–96. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kawamura N, Hatano K, Kakuta Y, Takada T,
Hara T and Yamaguchi S: A case of hepatoid adenocarcinoma of the
urinary bladder. Hinyokika Kiyo. 55:619–622. 2009.PubMed/NCBI
|
|
13
|
Isonishi S, Ogura A, Kiyokawa T, Suzuki M,
Kunito S, Hirama M, Tachibana T, Ochiai K and Tanaka T:
Alpha-fetoprotein (AFP)-producing ovarian tumor in an elderly
woman. Int J Clin Oncol. 14:70–73. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen YY, Hsu WH, Hu HM, Wu DC and Lin WY:
A case of alpha-fetoprotein-producing esophageal adenocarcinoma.
Kaohsiung J Med Sci. 29:106–110. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kripp M, Ströbel P, Dinter D, Lukan N,
Hochhaus A and Hofheinz RD: Alpha-fetoprotein expressing
metastastic adenocarcinoma of the esophago-gastric junction
responding favorably to capecitabine and oxaliplatin. Anticancer
Drugs. 20:75–78. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kawai H, Sekine S, Sanada T, Andoh T,
Takechi Y and Okada S: Alpha-fetoprotein-producing esophageal
carcinoma: A case report. Anticancer Res. 23:3837–3840.
2003.PubMed/NCBI
|
|
17
|
Kobayashi N, Ohbu M, Kuroyama S, Kikuchi
S, Shimao H, Mitomi H and Kakita A: Alpha-Fetoprotein-producing
esophageal adenocarcinoma: Report of a case. Surg Today.
31:915–919. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Takeuchi M, Yamaoka S, Matsumura K, et al:
An alpha-fetoprotein producing gastric carcinoma with hepatoid
features. A case report of hepatoid adenocarcinoma of the stomach.
Gastroenterol Endosc. 31:442–448. 1989.(In Japanese).
|
|
19
|
Nemoto A, Goshima H, Tanigawa K, et al: A
case of AFP-producing gastric cancer with multiple liver
metastasisn showing marked improvement by hepatoarterial infusion
with cisplatin. Mie Igaku. 42:84–94. 1998.(In Japanese).
|
|
20
|
Suzuki Y, Watanabe M, Nonaka H, Kase H,
Tokura N, Kikuchi M, Matsumoto H, Kobayashi K, Akima M and Yoshio
T: A case of advanced gastric carcinoma producing alpha-fetoprotein
with multiple liver metastasis in which intrahepatic chemotheraphy
was effective postgastrectomy. Jpn J Gastroenterol Surg.
32:2365–2369. 1999.(In Japanese). View Article : Google Scholar
|
|
21
|
Wahren B, Harmenberg J, Edsmyr F,
Jakobsson P and Ingimarsson S: Possible tumour markers in patients
with oesophagus cancer. Scand J Gastroenterol. 14:361–365. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chang YC, Nagasue N, Kohono H, Ohiwa K,
Yamanoi A and Nakamura T: Xenotransplantation of
alpha-fetoprotein-producing gastric cancers into nude mice:
Characteristics and responses to chemotherapy. Cancer. 69:872–877.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shimakawa T, Ogawa K, Naritaka Y,
Wagatsuma Y, Katsube T, Hamaguchi K, Konno S, Aiba M and Kajiwara
T: Alpha-fetoprotein producing Barrett's esophageal adenocarcinoma:
A case report. Anticancer Res. 19:4369–4373. 1999.PubMed/NCBI
|
|
24
|
Sawada H, Watanabe A, Yamada Y, Yano T,
Nakano H and Konishi Y: Alpha-fetoprotein producing esophageal
adenocarcinoma: Report of a case. Surg Today. 23:1103–1107. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sobin LH, Gospodarowicz M and Wittekind C:
Oesophagus including oesophagogastric junction. TNM Classification
of Malignant Tumours (7th). Wiley-Blackwell. (Oxford). 66–72.
2009.
|
|
26
|
Kataoka H, Miura Y, Joh T, Seno K, Tada T,
Tamaoki T, Nakabayashi H, Kawaguchi M, Asai K, Kato T and Itoh M:
Alpha-fetoprotein producing gastric cancer lacks
transcriptionalfactor ATBF1. Oncogene. 20:869–873. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Foschini MP, Baccarini P, Dal Monte PR,
Sinard J, Eusebi V and Rosai J: Albumin gene expression in
adenocarcinomas with hepatoid differentiation. Virchows Arch.
433:537–541. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Koide N, Nishio A, Igarashi J, Kajikawa S,
Adachi W and Amano J: Alpha-fetoprotein-producing gastric cancer:
Histochemical analysis of cell proliferation, apoptosis, and
angiogenesis. Am J Gastroenterol. 94:1658–1663. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Amemiya H, Kono K, Mori Y, Takahashi A,
Ichihara F, Iizuka H, Sekikawa T and Matsumoto Y: High frequency of
c-Met expression in gastric cancers producing alpha-fetoprotein.
Oncology. 59:145–151. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kamei S, Kono K, Amemiya H, Takahashi A,
Sugai H, Ichihara F, Fujii H and Matsumoto Y: Evaluation of VEGF
and VEGF-C expression in gastric cancer cells producing
alpha-fetoprotein. J Gastroenterol. 38:540–547. 2003.PubMed/NCBI
|
|
31
|
Dhar DK, Nagasue N, Yoshimura H, Tachibana
M, Tahara H, Matsuura H, Abe S, Chang YC and Nakamura T:
Overexpression of P-glycoprotein in untreated AFP-producing gastric
carcinoma. J Surg Oncol. 60:50–54. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ohashi N, Goshima H, Yamazaki H, et al: A
case report of so-called hepatoid adenocarcinoma of the stomach
without liver metastasis. Ringe (J Clin Surg). 43:1537–1541.
1988.(In Japanese).
|