Introduction
Isolated double pituitary adenomas are considerably
rare. Between 1978 and 2014, only 115 cases of double or multiple
pituitary adenomas, including clearly separated and contiguous
adenomas, were reported in the literature (1–7).
Furthermore, the diagnostic criteria for double or multiple
pituitary adenomas vary between pathologists and clinical doctors.
Certain cases have been diagnosed on the basis of the expression of
≥2 types of hormones and immunohistochemical staining results by
pathologists (5). The combined
expression of adrenocorticotropic hormone (ACTH) and prolactin
(PRL) is the most common characteristic of double or multiple
pituitary adenomas (5); however,
immunohistochemical studies on the diagnosis of double or multiple
pituitary adenomas have not been fully trusted by clinical doctors
when there is cross-reactivity of antisera and an insufficient
specimen (8). The doctor making the
diagnosis of double or multiple pituitary adenomas should correlate
the patient's symptoms with the type of hormone produced by the
tumor, since, in the majority of cases, the diagnosis of double or
multiple pituitary adenomas is made only on the basis of
immunohistochemical staining results. Only a few, clear cases of
multiple adenomas have been confirmed by pre- and intraoperative
evaluations (6,9–12). If
clinicians considered the presence of ≥2 separated tumors in the
same pituitary gland or the patient's clinical characteristics pre-
and intraoperatively, surgical failure could be prevented to a
greater extent.
The present study reports a case of clearly
separated adenomas, diagnosed based on preoperative
contrast-enhanced magnetic resonance imaging (MRI) findings and
surgical exploration. Written informed consent was obtained from
the patient.
Case report
Preoperative findings
A 50-year-old Chinese woman with a history of
diabetes mellitus and hypertension presented to The First
Affiliated Hospital of Chongqing Medical University (Chongqing,
China) with clinical symptoms of Cushing's disease, such as oily
skin, moon face, buffalo hump, facial plethora, typical cushingoid
central fat distribution and slight purple striae on the abdomen,
which had lasted for >10 years. Prior to admission on October
24, 2013, endocrine tests revealed that the patient's serum ACTH
level was 55.0 pg/ml and the cortisol (COR) level was 688.9 nmol/l;
therefore, the dexamethasone suppression test was performed, and
the diurnal variations of ACTH and COR were evaluated. The diurnal
variation of both the hormones spontaneously disappeared. The
patient's plasma COR and ACTH diurnal variations were as follows:
COR, 688.9 nmol/l and ACTH, 55 pg/ml at 8:00 a.m.; COR, 500.6
nmol/l and ACTH, 50.45 pg/ml at 4:00 p.m.; and COR, 614.8 nmol/l
and ACTH, 41.23 pg/ml at 12:00 a.m. The overnight low-dose
dexamethasone suppression test (1 mg dexamethasone administered
orally at 12:00 a.m.) revealed that low-dose dexamethasone could
not suppress the secretion of ACTH and COR, but high-dose
dexamethasone (8 mg orally) suppressed >50% of the initial
production of COR. The patient was hospitalized due to the highly
increased COR and ACTH levels (Table
I).
 | Table I.Dexamethasone suppression test. |
Table I.
Dexamethasone suppression test.
| A, Low-dose
overnight dexamethasone suppression test (1 mg orally at 12:00
a.m.) |
|---|
|
|---|
| Time of day | ACTH, pg/ml | COR, nmol/l |
|---|
| 8:00 am | 55.00 | 29.06 |
| 8:00 am (after 1
day) | 688.9 | 950.8 |
|
| B, High-dose
dexamethasone suppression test (8 mg orally) |
|
| Time of day | ACTH, pg/ml | COR, nmol/l |
|
| 8:00 am | 57.06 | 16.43 |
| 8:00 am (after 2
days) | 353.18 | 84.77 |
Following admission, the chief complaint of the
patient was rapid body-weight gain subsequent to surgery for an
ectopic pregnancy in 2000. The patient's body mass index was 39.56
kg/m2, and no family history of a pituitary tumor was
recorded. Blood biochemical assay results demonstrated blood lipid
metabolic disorders: The total cholesterol level was 6.8 mmol/l
(normal range, 2.8–5.2 mmol/l), triglyceride levels were 4.55
mmol/l (normal range, 0.35–1.7 mmol/l), high-density lipoprotein
level was 1.08 mmol/l (normal range, 0.9–1.8 mmol/l) and
low-density lipoprotein level was 4.05 mmol/l (normal range,
2.07–3.1 mmol/l). An endocrine examination revealed that all
hormone levels, except for ACTH (53 pg/ml; normal range, 7.20–63.30
pg/ml) and COR (829.07 nmol/l; normal range, 2.74–19.64 nmol/l),
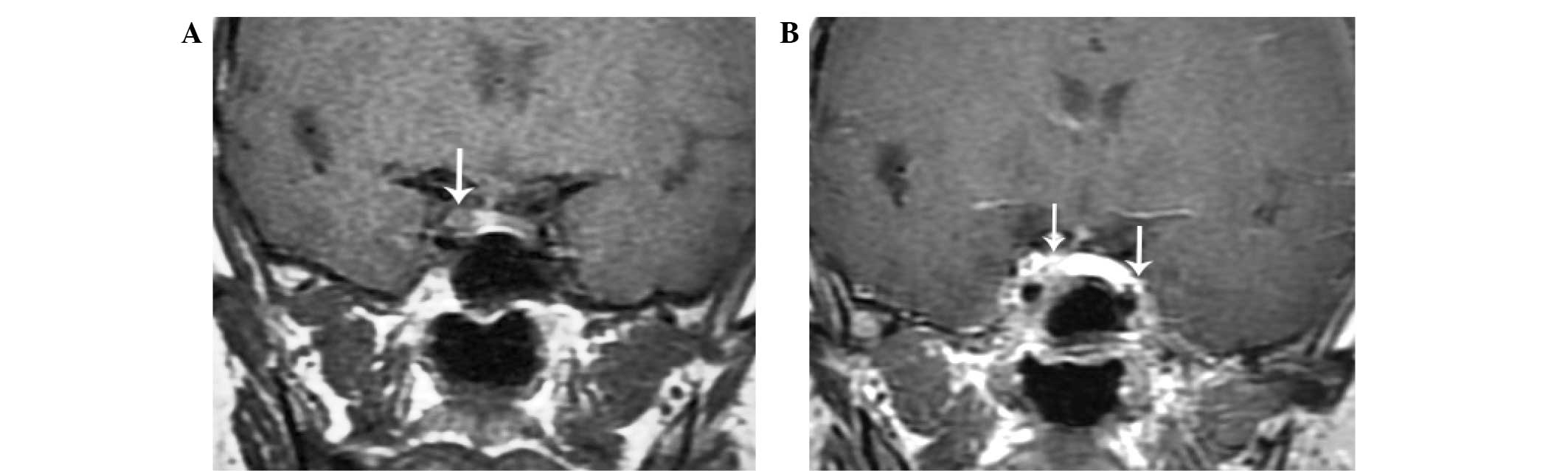
were normal (Table II). A
preoperative MRI scan detected a 5-mm tumor located on the right
side of the pituitary gland (Fig.
1A). Electrocardiography revealed sinus rhythm, and abdominal
ultrasonography demonstrated that the adrenal gland was normal.
Based on the patient's medical history and radiologic and
laboratory findings, an ACTH-secreting pituitary adenoma was
diagnosed, and neuroendoscopic surgery was performed. Preoperative
preparation included the control of the patient's glycemic and
blood pressure and improvement of her nutritional status.
| Table II.Preoperative and postoperative
hormonal tests. |
Table II.
Preoperative and postoperative
hormonal tests.
|
|
|
| Postoperative
values |
|---|
|
|
|
|
|
|---|
| Hormones | Reference
values | Preoperative
values | Day 1 | Day 7 | Month 3 |
|---|
| GH, ng/ml | 0.00–5.00 | 0.29 | 0.43 | 0.16 | 0.28 |
| ACTH, pg/ml | 7.20–63.30 | 53 | 1 | 1 | 1 |
| PRL, ng/ml | 2.74–19.64 | 12.81 | 5.30 | 7.83 | 30.75 |
| COR, nmol/l | 118.64–618.02 | 829.07 | 38.47 | 33.01 | 64.35 |
| TSH, uIU/ml | 0.35–3.50 | 0.45 | 1.03 | 1.01 | 2.88 |
| FT4, ng/ml | 0.61–1.12 | 0.74 | 0.94 | 0.94 | 1.27 |
| FT, pg/ml | 2.19–3.90 | 2.67 | 2.74 | 3.39 | 3.86 |
| LH, mIU/ml | 1.20–12.86 | 45.44 | 31.72 | 10.96 | 17.11 |
| FSH, mIU/ml | 1.79–5.12 | 86.20 | 58.52 | 30.62 | 34.14 |
| Estradiol,
ng/ml | 49–291 | 21 | 36 | 30 | 28 |
| Progesterone,
pg/ml | 0.00–0.78 | 0.94 | 0.21 | 0.32 | 0.22 |
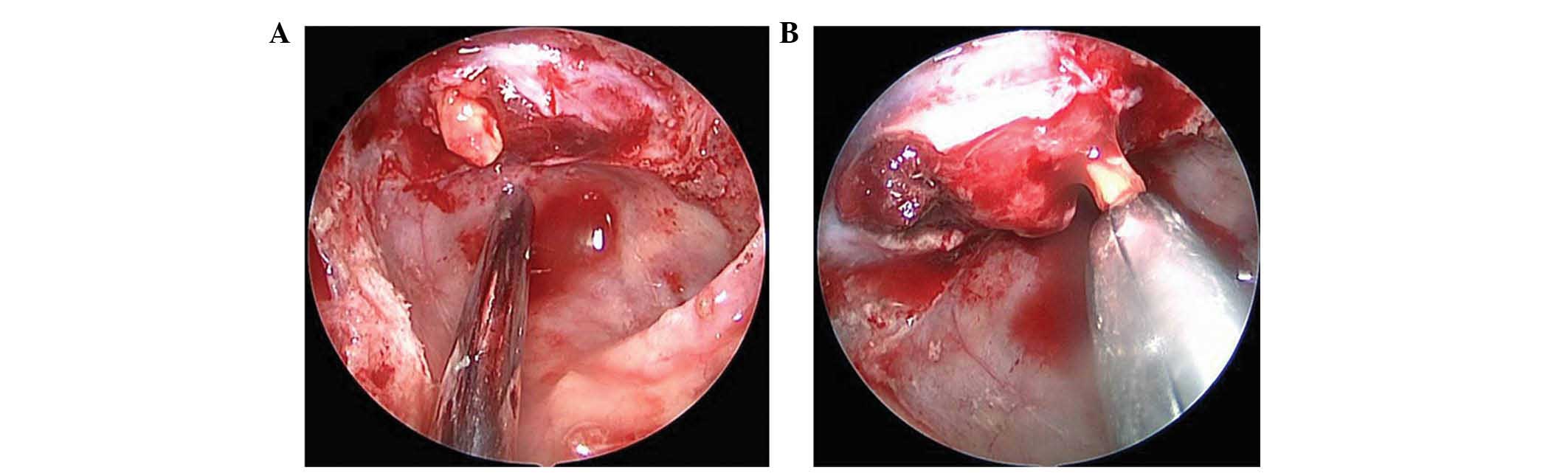
Intraoperative findings
A 5-mm white pituitary microadenoma was visualized
on the right side of the pituitary gland. Subsequently, another
3–5-mm white pituitary microadenoma was observed on the left side
of the pituitary gland during neuroendoscopic exploration. Based on
the findings of the preoperative contrast-enhanced MRI scan
(Fig. 1B) and surgical exploration
via neuroendoscopy (Fig. 2), the
lesions were confirmed as isolated double ACTH-secreting pituitary
adenomas, and were completely resected (Fig. 2).
Postoperative findings
The two pituitary tumors obtained during primary
surgical resection in October 2013 were analyzed. Pituitary adenoma
blocks (5 mm) were established using formalin-fixed,
paraffin-embedded tumor samples. Hematoxylin and eosin staining,
which was visualized using an optical microscope (Olympus
Corporation, Tokoyo, Japan), revealed that both specimens were
adenomas. Subsequently, each pathological section was subjected to
immunohistochemical staining with an avidin biotin-peroxidase
complex system. Briefly, following deparaffinization and
rehydration, epitope retrieval was performed using 10 mmol/l
citrate buffer (pH 6.0) for 15 min. The activity of endogenous
peroxidases was blocked with 3% hydrogen peroxide for 10 min at
room temperature. The sections were then incubated with primary
rabbit polyclonal ACTH (dilution, 1:200; cat no. ab74976; Abcam),
mouse monoclonal growth hormone (GH; dilution, 1:200; cat no.
ab7905; Abcam, Cambridge, UK), mouse monoclonal thyroid-stimulating
hormone (TSH; dilution, 1:200; cat no. ab27974; Abcam) and mouse
monoclonal PRL (dilution, 1:200; cat no. ab47150; Abcam) antibodies
at 4°C overnight in a humidified chamber. Negative controls were
obtained by the omission of primary antibodies, followed by
incubation with polyclonal horseradish peroxidase-conjugated goat
anti-rabbit (1:300; cat. no. ab6112; Abcam) and anti-mouse (1:200;
cat. no. ab5879; Abcam) IgG secondary antibodies for 30 min at room
temperature. Slides were stained with 3,3′-diaminobenzidine as the
chromogenic substrate for 10 min in the dark. The slides were then
visualized using an optical microscope (Olympus Corporation).
Immunohistochemical staining demonstrated that the two adenomas
were mainly positive for ACTH and focally positive for TSH, GH and
PRL (Fig. 3). The serum hormone
levels were measured on postoperative days 1 and 7. Compared with
preoperative levels, the expression of ACTH and COR in the two
tumors had markedly decreased following surgery (postoperative day
1, 1 pg/ml ACTH and 38.47 nmol/l COR; postoperative day 7, 1 pg/ml
ACTH and 33.01 nmol/l COR) (Table
II). The patient presented with secondary hypoadrenalism and
received hydrocortisone replacement treatment.
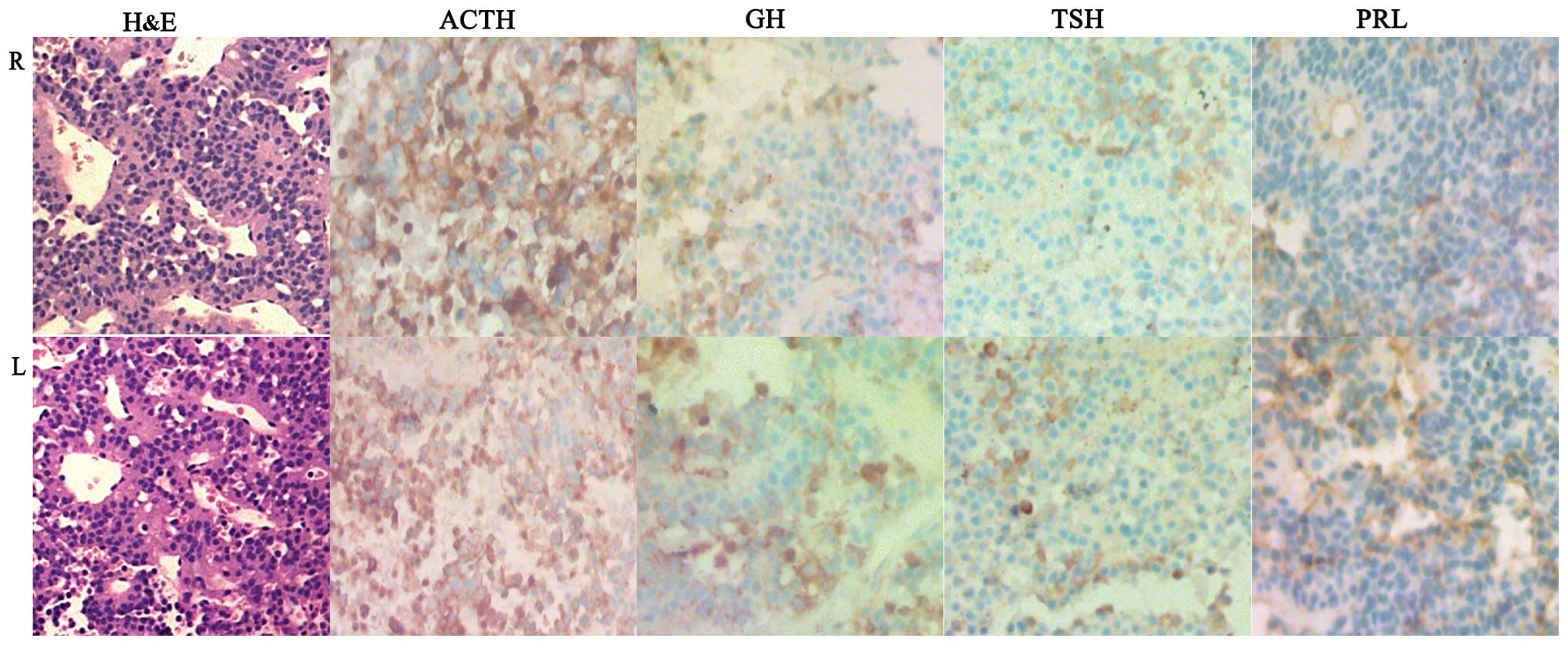 | Figure 3.Pathological and immunohistochemical
staining findings of the two tumors. Hematoxylin and eosin staining
of the two tumors suggested adenomas. The cells of both tumors were
oval, basophilic cells with clear nucleoli, without signs of focal
necrosis, active mitosis or atypical nuclei. Immunohistochemical
staining of the two tumors revealed that the cells were mainly
positive for adrenocorticotropic hormone and focally positive for
thyroid-stimulating, growth and prolactin hormones (magnification,
×400). R, right; L, left; H&E, hematoxylin and eosin; GH,
growth hormone; ACTH, adrenocorticotropic hormone; PRL, prolactin;
TSH, thyroid-stimulating hormone. |
Three months after surgery, the patient's hormone
levels were re-evaluated. Oral glucose tolerance test results
revealed impaired glucose tolerance, suggesting that the patient's
glycometabolism disorders were recovering slowly following the
resection of the pituitary tumors. Dyslipidemia had also improved.
The patient had no obvious discomfort.
Discussion
The incidence rates of clearly separated adenomas
are unknown. Magri et al (9)
reported that the incidence of double pituitary adenomas in
patients who chose not to undergo surgery was 2.6%. Double or
multiple pituitary adenomas, and clearly separated adenomas
confirmed by preoperative imaging or intraoperative exploration in
particular, are considerably rare. Kim et al (10) identified 4 cases (0.67%) of multiple
adenomas among 600 surgical cases that were suspected to be
multiple adenomas based on preoperative MRI scan. Ratliff and
Oldfield (11) also reported 13
patients (1.82%) with multiple adenomas that were detected
intraoperatively, and 1 patient (0.15%) that was diagnosed with
multiple adenomas on the basis of preoperative MRI findings.
Following a review of the literature, 115 cases of
double or multiple pituitary adenomas were identified (1–7). Based on
the classification of double or multiple pituitary adenomas
established by Ratliff and Oldfield (11), Andrioli et al (13) and Kontogeorgos et al (14), 37 patients were diagnosed with
unclassified multiple pituitary adenomas on autopsy (15,16). The
types of adenomas of the remaining 78 patients are listed in
Table III. Patients were divided
into two groups: Those with clearly separated adenomas and those
with a contiguous pituitary tumor diagnosed by pathology.
| Table III.Cases of multiple pituitary
adenomas. |
Table III.
Cases of multiple pituitary
adenomas.
|
| Clearly separated
pituitary adenomas (n=42)a | Contiguous
pituitary adenomas (n=36)b |
|---|
|
|
|
|
|---|
| Variable | N | % | N | % |
|---|
| Gender |
|
|
|
|
|
Female | 29 |
69.0 | 16 | 55.6 |
|
Male | 13 |
31.0 | 20 | 44.4 |
| Preoperative
imaging |
|
|
|
|
|
Magnetic resonance
imaging | 22 |
52.4 | 0 |
0.0 |
|
Computed tomography | 2 |
4.8 | 0 |
0.0 |
| Intraoperative
diagnosis (neurosurgery) | 18 |
42.9 | 0 |
0.0 |
| Postoperative
diagnosis (pathology) | 42 | 100.0 | 36 | 100.0 |
The youngest reported patient was a 15-year-old
girl, whose condition was diagnosed on the basis of MRI findings,
according to Goldberg et al (2). The oldest reported patient was 80 years
old (8). The majority of patients
were aged 41.5–45.5 years. On the basis of preoperative,
intraoperative and postoperative evaluations, 42 patients were
diagnosed with clearly separated double pituitary adenomas
(1–4,8,10–14,17–25),
36 patients with contiguous pituitary adenomas (6–9,11,12,14,26–29),
and 3 patients with 3 pituitary adenomas (11,22,23).
The majority of double or multiple pituitary
adenomas are mainly detected by one of the following methods:
Imaging examination, surgical exploration or autopsy (9–11,14,16,22,23);
however, the adenomas nature and type of hormones expressed are
confirmed by pathology and immunohistochemistry, respectively
(11). At present, in clinical
practice, a useful detection method is essential to evaluate the
presence of double or multiple pituitary adenomas (9). The coexistence of multiple pituitary
tumors often accounts for surgical failure (22). Numerous examination types, including
MRI and computed tomography (CT) scans, as well as intraoperative
ultrasonography, are able to detect double or multiple pituitary
adenomas. MRI was the first reported modality to diagnose multiple
pituitary adenomas (22).
Preoperative MRI, particularly thin-slice, dynamic
and contrast-enhanced MRI (2,10,13,17), is an
effective and sensitive method of determining the presence of
multiple adenomas (10–12,14,21,22,29).
Among 42 patients (Table III), 22
(52.4%) were diagnosed on the basis of preoperative MRI findings,
and 2 (4.8%) on the basis of CT findings (24). The remaining 18 patients were
diagnosed during surgery. Preoperative MRI is more important than
CT in the diagnosis of multiple adenomas. As indicated in the
present case and previous literature reports, contrast-enhanced MRI
is able to confirm separated double or multiple pituitary adenomas
(1,3,9,13,17,28).
Intraoperative evaluation, including MRI and
ultrasonography, as well as surgical exploration, may assist the
diagnosis of double or multiple pituitary adenomas (11,14,18,20,25,30,31).
A total of 18 cases (42.9%) of double pituitary adenomas from the
literature were diagnosed during surgery (11,14,18,20,25,30),
with the majority of them being clearly visible to the surgeon by
the microscopic approach (11).
Endoscopic transsphenoidal surgery is used more often than the
microscopic approach, particularly in cases of pituitary lesions
(32). In the present case, the
patient underwent neuroendoscopic transsphenoidal surgery, which
allowed for better visualization and enabled the detection of
another microadenoma. This prevented the requirement for a second
surgery (Fig. 2). Oyama et al
(18) reported that 1 patient had to
undergo two surgeries to resect two pituitary adenomas; the disease
manifestation and hormone levels following the first surgery
revealed that the tumors were not in remission, and indicated the
presence of another microadenoma. Kontogeorgos et al
(14) and McKelvie and McNeill
(20) have reported similar cases.
Thus, according to Liu et al (33), establishing the difference between a
normal pituitary gland and a pituitary adenoma is crucial during
surgery.
There are numerous different theories on the
pathogenesis of pituitary tumors, including genetic mutations,
autocrine/paracrine interactions, altered hypothalamic function,
abnormal extrapituitary regulatory mechanisms, epigenetic
modification, and microRNAs and large non-coding RNAs such as
maternally expressed 3 (8,10,34,35). Kim
et al (10) reported 2
patients with a family history of pituitary adenomas, suggesting
that genetic abnormalities may be associated with the pathogenesis
of double or multiple pituitary tumors. Kumar and Prusty (4) were the first to report a case of a
macroprolactinoma that evolved from two separate microadenomas. It
was suggested that a polyclonal origin of the prolactinoma was
responsible for the pathogenesis of multiple pituitary adenomas,
but there were no definite histopathological results to demonstrate
that the original lesion consisted of two prolactinomas. In the
present case, the histopathological results demonstrated a
pituitary adenoma, and immunohistochemical staining revealed that
the tumor cells were positive for ACTH, TSH, GH and PRL (Fig. 3). These findings may explain Kumar and
Prusty's conclusions (4).
In summary, progress has been made in determining
the roles that tumor suppressors, oncogenes and cycle abnormalities
perform during the onset of pituitary adenoma; however, due to the
limitations in the use of human pituitary adenoma cell lines and
animal models, the acute pathogenesis of multiple pituitary
adenomas remains to be fully elucidated (1,3,4,34,36).
References
|
1
|
Kobayashi Y, Takei M, Ohkubo Y, Kakizawa
Y, Matoba H, Kumagai M, Takeda T, Suzuki S and Komatsu M: A
somatotropin-producing pituitary adenoma with an isolated
adrenocorticotropin-producing pituitary adenoma in a female patient
with acromegaly, subclinical Cushing's disease and a left adrenal
tumor. Endocr J. 61:589–595. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Goldberg AS, Stein R, Merritt NH, Inculet
R and Van Uum S: A pediatric patient with Cushing syndrome caused
by ectopic ACTH syndrome and concomitant pituitary incidentalomas.
J Pediatr Endocrinol Metab. 27:123–128. 2013.
|
|
3
|
Zielinski G, Maksymowicz M, Podgorski J
and Olszewski WT: Double, synchronous pituitary adenomas causing
acromegaly and Cushing's disease. A case report and review of
literature. Endocr Pathol. 24:92–99. 2014. View Article : Google Scholar
|
|
4
|
Kumar KV and Prusty P: Resistant
prolactinoma: Is it monoclonal or polyclonal? Indian J Endocrinol
Metab. 17:2013. View Article : Google Scholar
|
|
5
|
Iacovazzo D, Bianchi A, Lugli F, Milardi
D, Giampietro A, Lucci-Cordisco E, Doglietto F, Lauriola L and De
Marinis L: Double pituitary adenomas. Endocrine. 43:452–457. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Koutourousiou M, Kontogeorgos G, Wesseling
P, Grotenhuis AJ and Seretis A: Collision sellar lesions:
Experience with eight cases and review of the literature.
Pituitary. 13:8–17. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Al Brahim NY, Rambaldini G, Ezzat S and
Asa SL: Complex endocrinopathies in MEN-1: Diagnostic dilemmas in
endocrine oncology. Endocr Pathol. 18:37–41. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jastania RA, Alsaad KO, Al-Shraim M,
Kovacs K and Asa SL: Double adenomas of the pituitary:
Transcription factors Pit-1, T-pit and SF-1 identify cytogenesis
and differentiation. Endocr Pathol. 16:187–194. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Magri F, Villa C, Locatelli D, Scagnelli
P, Lagonigro MS, Morbini P, Castellano M, Gabellieri E, Rotondi M,
Solcia E, et al: Prevalence of double pituitary adenomas in a
surgical series: Clinical, histological and genetic features. J
Endocrinol Invest. 33:325–331. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim K, Yamada S, Usui M and Sano T:
Preoperative identification of clearly separated double pituitary
adenomas. Clin Endocrinol (Oxf). 61:26–30. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ratliff JK and Oldfield EH: Multiple
pituitary adenomas in Cushing's disease. J Neurosurg. 93:753–761.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sano T, Horiguchi H, Xu B, Li C, Hino A,
Sakaki M, Kannuki S and Yamada S: Double pituitary adenomas: Six
surgical cases. Pituitary. 1:243–250. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Andrioli M, Giraldi Pecori F, Losa M,
Terreni M, Invitti C and Cavagnini F: Cushing's disease due to
double pituitary ACTH-secreting adenomas: The first case report.
Endocr J. 57:833–837. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kontogeorgos G, Scheithauer BW, Horvath E,
Kovacs K, Lloyd RV, Smyth HS and Rologis D: Double adenomas of the
pituitary: A clinicopathological study of 11 tumors. Neurosurgery.
31:840–849. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Buurman H and Saeger W: Subclinical
adenomas in postmortem pituitaries: Classification and correlations
to clinical data. Eur J Endocrinol. 154:753–758. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kontogeorgos G, Kovacs K, Horvath E and
Scheithauer BW: Multiple adenomas of the human pituitary. A
retrospective autopsy study with clinical implications. J
Neurosurg. 74:243–247. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
de Oliveira Andrade LJ, Santos França L,
Santos França L and de Cordeiro Almeida MA: Double pituitary
prolactinoma. J Clin Endocrinol Metab. 95:4848–4849. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oyama K, Yamada S, Hukuhara N, Hiramatsu
R, Taguchi M, Yazawa M, Matsuda A, Ohmura E and Imai Y:
FSH-producing macroadenoma associated in a patient with Cushing's
disease. Neuro Endocrinol Lett. 27:733–736. 2006.PubMed/NCBI
|
|
19
|
Shimizu C, Koike T and Sawamura Y: Double
pituitary adenomas with distinct histological features and
immunophenotypes. J Neurol Neurosurg Psychiatry.
75:1402004.PubMed/NCBI
|
|
20
|
McKelvie PA and McNeill P: Double
pituitary adenomas: A series of three patients. Pathology.
34:57–60. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tosaka M, Kohga H, Kobayashi S, Zama A,
Tamura M, Murakami M and Sasaki T: Double pituitary adenomas
detected on preoperative magnetic resonance images. Case
illustration. J Neurosurg. 92:3612000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cannavò S, Curtò L, Lania A, Saccomanno K,
Salpietro FM and Trimarchi F: Unusual MRI finding of multiple
adenomas in the pituitary gland: A case report and review of the
literature. Magn Reson Imaging. 17:633–636. 1999.PubMed/NCBI
|
|
23
|
Pantelia E, Kontogeorgos G, Piaditis G and
Rologis D: Triple pituitary adenoma in Cushing's disease: Case
report. Acta Neurochir (Wien). 140:190–193. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hashimoto N, Handa H, Yamagami T, Kojima
M, Aoki M, Okamoto S, Kato Y and Imura H: Acromegaly with multiple
secreting pituitary adenomas. Surg Neurol. 22:556–558. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Woosley RE: Multiple secreting
microadenomas as a possible cause of selective transsphenoidal
adenomectomy failure. Case report. J Neurosurg. 58:267–269. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rotondo F, Khatun N, Scheithauer BW,
Horvath E, Marotta TR, Cusimano M and Kovacs K: Unusual double
pituitary adenoma: A case report. Pathol Int. 61:42–46. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mohammed S, Cusimano MD, Scheithauer BW,
Rotondo F, Horvath E and Kovacs K: O-methylguanine-DNA
methyltransferase immunoexpression in a double pituitary adenoma:
Case report. Neurosurgery. 66:E421–E422. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Coiré CI, Smyth HS, Rosso D, Horvath E and
Kovacs K: A double pituitary adenoma presenting as a
prolactin-secreting tumor with partial response to medical therapy.
Case report. Endocr Pathol. 21:135–138. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Meij BP, Lopes MB, Vance ML, Thorner MO
and Laws ER Jr: Double pituitary lesions in three patients with
Cushing's disease. Pituitary. 3:159–168. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tolis G, Bertrand G, Carpenter S and
McKenzie JM: Acromegaly and galactorrhea-amenorrhea with two
pituitary adenomas secreting growth hormone or prolactin. A case
report. Ann Intern Med. 89:345–348. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Laws ER: Multiple pituitary adenomas.
Journal of neurosurgery. 93:2000.
|
|
32
|
Yadav Y, Sachdev S, Parihar V, Namdev H
and Bhatele P: Endoscopic endonasal trans-sphenoid surgery of
pituitary adenoma. J Neurosci Rural Pract. 3:328–337. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Liu JF, Ke CS, Chen X, Xu Y, Zhang HQ,
Chen J, Gan C, Li CX and Lei T: Identification and management of
intra-operative suspicious tissues in 20 transsphenoidal surgery
cases. Sichuan Da Xue Xue Bao Yi Xue Ban. 44:441–443. 2013.(In
Chinese). PubMed/NCBI
|
|
34
|
Jiang X and Zhang X: The molecular
pathogenesis of pituitary adenomas: An update. Endocrinol Metab
(Seoul). 28:245–254. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Melmed S: Pathogenesis of pituitary
tumors. Nat Rev Endocrinol. 7:257–266. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Curtò L and Trimarchi F: Comment on:
Double, synchronous pituitary adenomas causing acromegaly and
Cushing's disease. A case report and review of literature. Endocr
Pathol 2013;24:92-99. Endocr Pathol. 25:439–440. 2014. View Article : Google Scholar : PubMed/NCBI
|