Introduction
Metastatic brain tumor is the most common type of
intracranial neoplasm in adults (1),
with a reported survival rate of 3–6 months (2). Patients with lung cancer have been shown
to develop brain metastasis at an early stage, usually within the
first 2 years following the diagnosis of the primary tumor
(3,4).
It has been reported that 25–40% of patients with non-small cell
lung cancer (NSCLC) develop brain metastasis during the course of
their disease (5). The majority of
recurrent tumors are distant, and >80% of them occur within the
first 2 years subsequent to NSCLC resection (6–9). A
previous study has reported that the 1- and 2-year post-recurrence
survival rates are 69.8 and 44.4%, respectively (10). Recurrence after >2 years is
considered late recurrence, although isolated solitary brain
metastasis as a late postoperative recurrence of NSCLC is rare
(11). The present study describes
the case of a 64-year-old male patient with NSCLC who presented
with an isolated solitary brain metastasis 28 months following the
complete resection of the primary tumor.
Case report
A 64-year-old male patient was admitted to the
Tongji University Affiliated Shanghai Pulmonary Hospital (Shanghai,
China) in March 2011 for examination of a chest mass in the left
lower lobe of the lung. The patient was asymptomatic. Upon
admission, a laboratory examination was performed, which revealed a
lactate dehydrogenase level of 159 IU/l (normal range, 94–250
IU/l). The serum level of carcinoembryonic antigen (CEA) was 48.77
µg/ml (normal range, 0–10 µg/ml). Computed tomography scan
(Brilliance 16; Philips Healthcare, Amsterdam, The Netherlands) and
chest X-ray (DigitalDiagnost DR; Philips Healthcare) revealed a
poorly defined mass located in the lower lobe of the left lung,
with ipsilateral mediastinal lymph node swelling. No malignant
cells were observed following transbronchial and percutaneous
aspiration lung biopsy. As no metastatic lesions were identified,
surgery was selected as the appropriate treatment option, and the
lower lobe of the lung was removed on April 1, 2011. The
pathological diagnosis was adenocarcinoma and stage IB (T2N0M0)
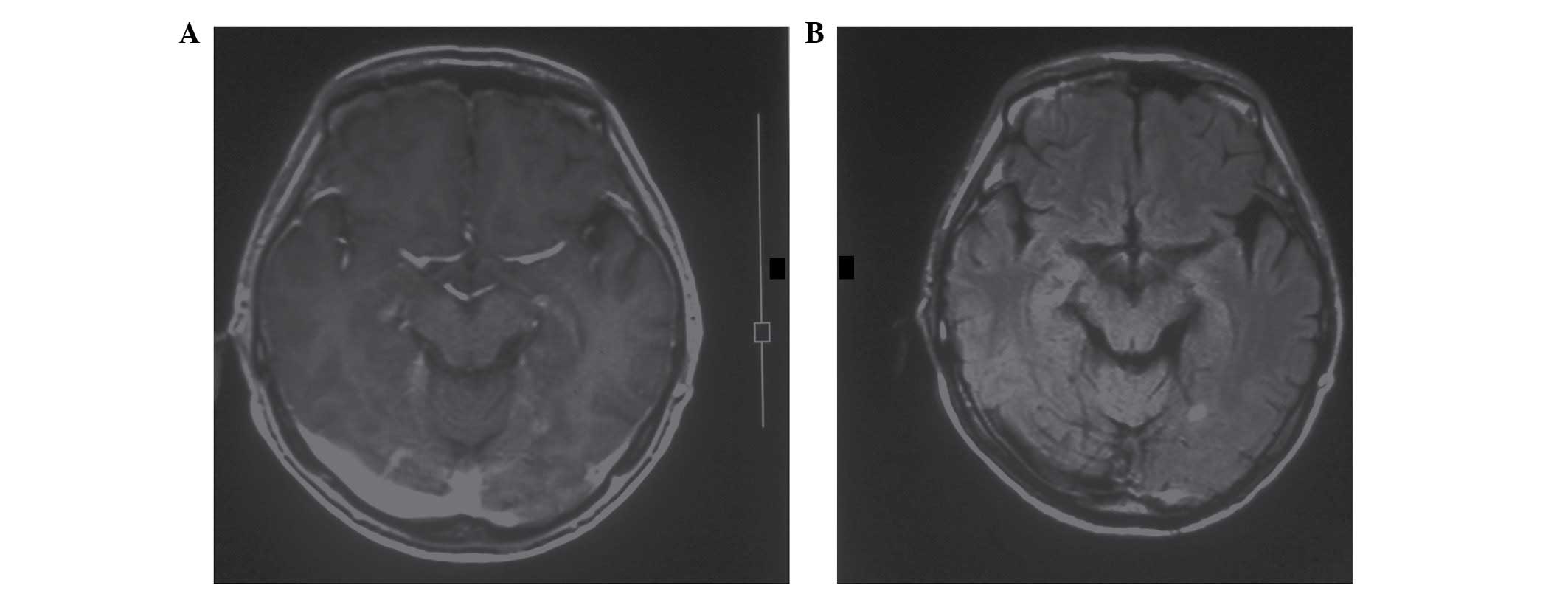
NSCLC. The patient refused postoperative adjuvant chemotherapy. A
follow-up magnetic resonance imaging (MRI) scan (Intera 1.5T;
Philips Healthcare) conducted 28 months following the initial
diagnosis of NSCLC detected a metastatic lesion in the left
occipital lobe of the cerebral hemisphere (Fig. 1). In addition, the patient's CEA level
had risen to 80.19 µg/ml. Systemic imaging evaluation identified no
tumor recurrence at the primary site and no other distant
metastases. The patient was then administered a 30 Gy dose of whole
brain radiation therapy (WBRT; Lightspeed RT; GE Healthcare, Little
Chalfont, UK). No chemotherapy was prescribed. At the time of
writing the patient remained healthy 1 year following the
successful treatment of the metastatic tumor.
The present case report conformed to the Ethical
Guidelines for Clinical Studies issued by the Ministry of Health,
Labor and Welfare of China (12), and
written informed consent was obtained from the patient.
Discussion
Brain metastasis in NSCLC is the most common type of
intracranial metastasis, and 10% of NSCLC patients are diagnosed
with brain metastasis at the initial stage of NSCLC, while 30–50%
of patients are diagnosed at later stages (13). The majority of chemotherapy drugs fail
to treat brain metastasis; despite the fact that the blood brain
barrier around the brain tumor is damaged, the concentration of the
chemotherapy drugs in the brain remains low, possibly due to efflux
pump-mediated resistance (14). These
patients usually have a poor prognosis, being the median survival
time of 4–6 months in treated patients, compared with 1 month in
untreated patients (15,16). WBRT is the most common treatment
modality for brain metastasis in NSCLC, since it has an effect on
palliation and stabilization of cranial progression and has been
shown to prolong survival in all patients with brain tumors
(17).
The prognosis of patients with recurrence following
complete surgical resection of NSCLC is considered to be a
multifactorial process, which depends on clinicopathological,
biological and treatment characteristics (18). The reported recurrence rates following
complete NSCLC resection are 30–75% (6,7,8,9,19,20), and
~15% for pathological stage I cases (21,22). The
late recurrence of lung cancer has become an increasing subject of
research, due to the high level of curability and the likelihood of
long-survival (23). The development
of isolated solitary brain metastasis is not a common occurrence
for patients with lung adenocarcinomas, and a proportion of those
patients has a favorable prognosis (24–26).
The present study describes a case of isolated
solitary brain metastasis as a late recurrence of completely
resected NSCLC. To the best of our knowledge, no similar reports of
late isolated solitary brain metastasis as a postoperative
recurrence of NSCLC have been previously described in the
literature. The patient of the present study was a long-term
survivor who was treated with WBRT alone. The brain metastasis was
not confirmed by histology; it was detected by brain MRI scan
without any presenting symptoms. At the time of writing, the
patient was healthy 1 year following the successful treatment of
the metastatic tumor using WBRT. Therefore, clinicians should
consider whether chemotherapy is required in cases of isolated
solitary brain metastasis as a late recurrence of completely
resected NSCLC.
Acknowledgements
The present study was financially supported by the
National Natural Science Foundation of China (Beijing, China;
grant. no. 81207106), the Traditional Chinese Medicine Research
Fund of Shanghai Municipal Health Bureau (Shanghai, China; grant
no. 2012L051A), Fund of Shanghai Municipal Health Bureau (Shanghai,
China; grant no. 20124Y123), and the Science and Technology
Commission of Shanghai Municipality (Shanghai, China; grant nos.
14401932200 and 12401907500). The authors would also like to thank
Professor Rongzheng Ren for revising the present manuscript.
References
|
1
|
Schouten LJ, Rutten J, Huveneers HA and
Twijnstra A: Incidence of brain metastases in a cohort of patients
with carcinoma of the breast, colon, kidney, and lung and melanoma.
Cancer. 94:2698–2705. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Patchell RA, Tibbs PA, Walsh JW, Dempsey
RJ, Maruyama Y, Kryscio RJ, Markesbery WR, Macdonald JS and Young
B: A randomized trial of surgery in the treatment of single
metastases to the brain. N Engl J Med. 322:494–500. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nakade M, Kohno K and Watanabe H:
Treatment strategies for lung cancer brain metastases. Nihon Kyobu
Geka Gakkai Zasshi. 45:1911–1915. 1997.(In Japanese). PubMed/NCBI
|
|
4
|
Wroński M, Arbit E, Burt M and Galicich
JH: Survival after surgical treatment of brain metastases from lung
cancer: A follow-up study of 231 patients treated between 1976 and
1991. J Neurosurg. 83:605–616. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sørensen JB, Hansen HH, Hansen M and
Dombernowsky P: Brain metastases in adenocarcinoma of the lung:
Frequency, risk groups, and prognosis. J Clin Oncol. 6:1474–1480.
1988.PubMed/NCBI
|
|
6
|
Martini N, Bains MS, Burt ME, Zakowski MF,
McCormack P, Rusch VW and Ginsberg RJ: Incidence of local
recurrence and second primary tumors in resected stage I lung
cancer. J Thorac Cardiovasc Surg. 109:120–129. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
al-Kattan K, Sepsas E, Fountain SW and
Townsend ER: Disease recurrence after resection for stage I lung
cancer. Eur J Cardiothorac Surg. 12:380–384. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yoshino I, Yohena T, Kitajima M, Ushijima
C, Nishioka K, Ichinose Y and Sugimachi K: Survival of non-small
cell lung cancer patients with postoperative recurrence at distant
organs. Ann Thorac Cardiovasc Surg. 7:204–209. 2001.PubMed/NCBI
|
|
9
|
Martin J, Ginsberg RJ, Venkatraman ES,
Bains MS, Downey RJ, Korst RJ, Kris MG and Rusch VW: Long-term
results of combined-modality therapy in resectable non-small-cell
lung cancer. J Clin Oncol. 20:1989–1995. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sasaki H, Suzuki A, Tatematsu T, Shitara
M, Hikosaka Y, Okuda K, Moriyama S, Yano M and Fujii Y: Prognosis
of recurrent non-small cell lung cancer following complete
resection. Oncol Lett. 7:1300–1304. 2014.PubMed/NCBI
|
|
11
|
Hiyoshi Y, Yoshida N, Watanabe M,
Kurashige J, Karashima R, Iwagami S, Baba Y and Baba H: Late
recurrence after radical resection of esophageal cancer. World J
Surg. Nov 9–2015.(Epub ahead of print). PubMed/NCBI
|
|
12
|
Kang WM, Meng QB, Yu JC, Ma ZQ and Li ZT:
Factors associated with early recurrence after curative surgery for
gastric cancer. World J Gastroenterol. 21:5934–5940.
2015.PubMed/NCBI
|
|
13
|
Quan AL, Videtic GM and Suh JH: Brain
metastases in small cell lung cancer. Oncology (Williston Park).
18:961–972; discussion 974, 979–80, 987. 2004.PubMed/NCBI
|
|
14
|
On NH, Mitchell R, Savant SD, Bachmeier
CJ, Hatch GM and Miller DW: Examination of blood-brain barrier
(BBB) integrity in a mouse brain tumor model. J Neurooncol.
111:133–143. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sundström JT, Minn H, Lertola KK and
Nordman E: Prognosis of patients treated for intracranial
metastases with whole-brain irradiation. Ann Med. 30:296–299. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sperduto PW: What is your patient's GPA
and why does it matter? Managing brain metastases and the cost of
hope. Int J Radiat Oncol Biol Phys. 77:643–644. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zabel A and Debus J: Treatment of brain
metastases from non-small-cell lung cancer (NSCLC): Radiotherapy.
Lung Cancer. 45(Suppl 2): S247–S252. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yokouchi H, Miyazaki M, Miyamoto T, Tsuji
F, Ebisui C and Murata K: Post-recurrence survival after surgical
resection of non-small cell lung cancer with local recurrence. Gan
To Kagaku Ryoho. 41:2050–2052. 2014.(In Japanese). PubMed/NCBI
|
|
19
|
Williams BA, Sugimura H, Endo C, Nichols
FC, Cassivi SD, Allen MS, Pairolero PC, Deschamps C and Yang P:
Predicting postrecurrence survival among completely resected
nonsmall-cell lung cancer patients. Ann Thorac Surg. 81:1021–1027.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sugimura H, Nichols FC, Yang P, Allen MS,
Cassivi SD, Deschamps C, Williams BA and Pairolero PC: Survival
after recurrent nonsmall-cell lung cancer after complete pulmonary
resection. Ann Thorac Surg. 83:409–418. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hung JJ, Hsu WH, Hsieh CC, Huang BS, Huang
MH, Liu JS and Wu YC: Post-recurrence survival in completely
resected stage I non-small cell lung cancer with local recurrence.
Thorax. 64:192–196. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shimada Y, Saji H, Yoshida K, Kakihana M,
Honda H, Nomura M, Usuda J, Kajiwara N, Ohira T and Ikeda N:
Prognostic factors and the significance of treatment after
recurrence in completely resected stage I non-small cell lung
cancer. Chest. 143:1626–1634. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Maeda R, Yoshida J, Ishii G, Aokage K,
Hishida T, Nishimura M, Nishiwaki Y and Nagai K: Long-term outcome
and late recurrence in patients with completely resected stage IA
non-small cell lung cancer. J Thorac Oncol. 5:1246–1250. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Luketich JD, Martini N, Ginsberg RJ,
Rigberg D and Burt ME: Successful treatment of solitary
extracranial metastases from non-small cell lung cancer. Ann Thorac
Surg. 60:1609–1611. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shahidi H and Kvale PA: Long-term survival
following surgical treatment of solitary brain metastasis in
non-small cell lung cancer. Chest. 109:271–276. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kagohashi K, Satoh H, Yamashita YT and
Sekizawa K: Brain metastasis as the first manifestation of lung
cancer. Am J Med. 114:4202003. View Article : Google Scholar : PubMed/NCBI
|