Introduction
Sertoli-Leydig cell tumors (SLCTs) are an uncommon
subtype of sex-cord stromal tumors of the ovary. The tumors account
for <0.5% of all ovarian tumors and are most frequently located
in one ovary (1,2). SLCTs may produce androgens or estrogens,
and their prognosis is associated with tumor differentiation and
disease stage (1).
SLCTs are most commonly diagnosed in young women,
creating an issue with regard to the preservation of fertility
(3). Oncologists should consider the
risk of infertility in women of reproductive age who undergo
treatment for SLCTs. Patients must be thoroughly informed about the
conservative treatment alternatives for genital tract preservation,
as well as the potential risk of recurrent disease. The
conservative management consists of unilateral
salpingo-oophorectomy, usually accompanied by biopsy of the
contralateral ovary. Hysterectomy and bilateral
salpingo-oophorectomy comprise the radical treatment strategies
(4).
The current study presents the case of young female
patient with a Sertoli-Leydig ovarian tumor, who underwent
conservative management. The obstetric outcome following the
conservative treatment approach is presented. A review of the
relevant literature is additionally conducted.
Case report
A 20-year-old woman was admitted to the ‘Agios
Dimitrios’ General Hospital of Thessaloniki (Thessaloniki, Greece)
in March 2013 for gynecological investigation due to abdominal
pain. The patient mentioned no other symptoms or pathologies. The
obstetric history consisted of one vaginal delivery of a live
infant. Diagnostic exploration by intravaginal ultrasonography
revealed a pelvic mass with a maximum diameter of 13 cm, which
originated from the left ovary. These findings were additionally
confirmed by computed tomography (CT), and no other pelvic or
abdominal features were observed. Tumor serum markers, including
cancer antigen (CA)125, CA19-9, carcinoembryonic antigen and
α-fetoprotein, were all negative.
The patient underwent laparotomic exploration, and
gross inspection certified the presence of a cystic tumor of the
left ovary with solid components. Peritoneal liquid was sampled for
cytological investigation, and a salpingo-oophorectomy of the
pathological adnexal mass was performed. Palpation of the
retroperitoneal space was negative, while the contralateral adnexa
were of normal appearance and size.
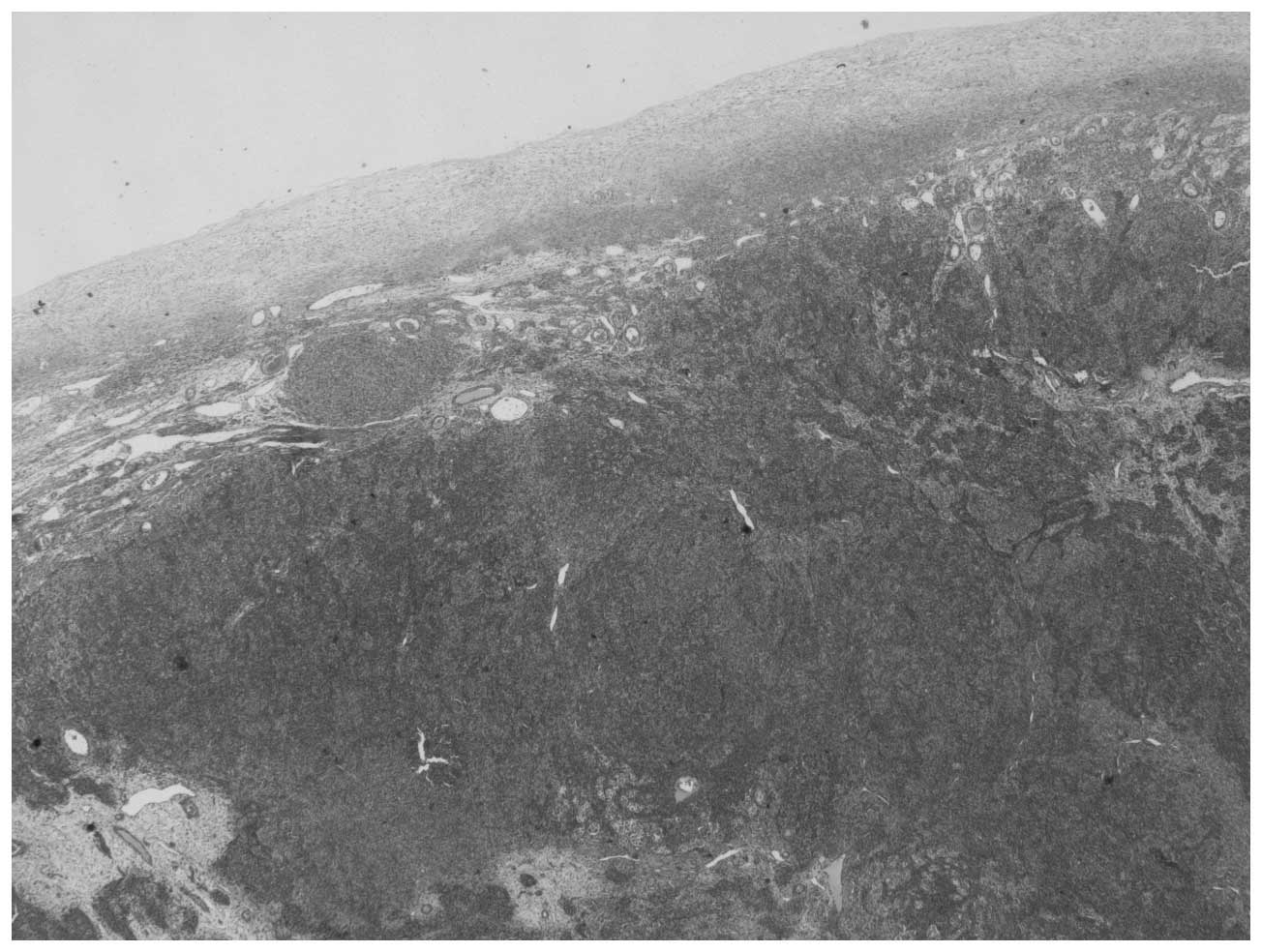
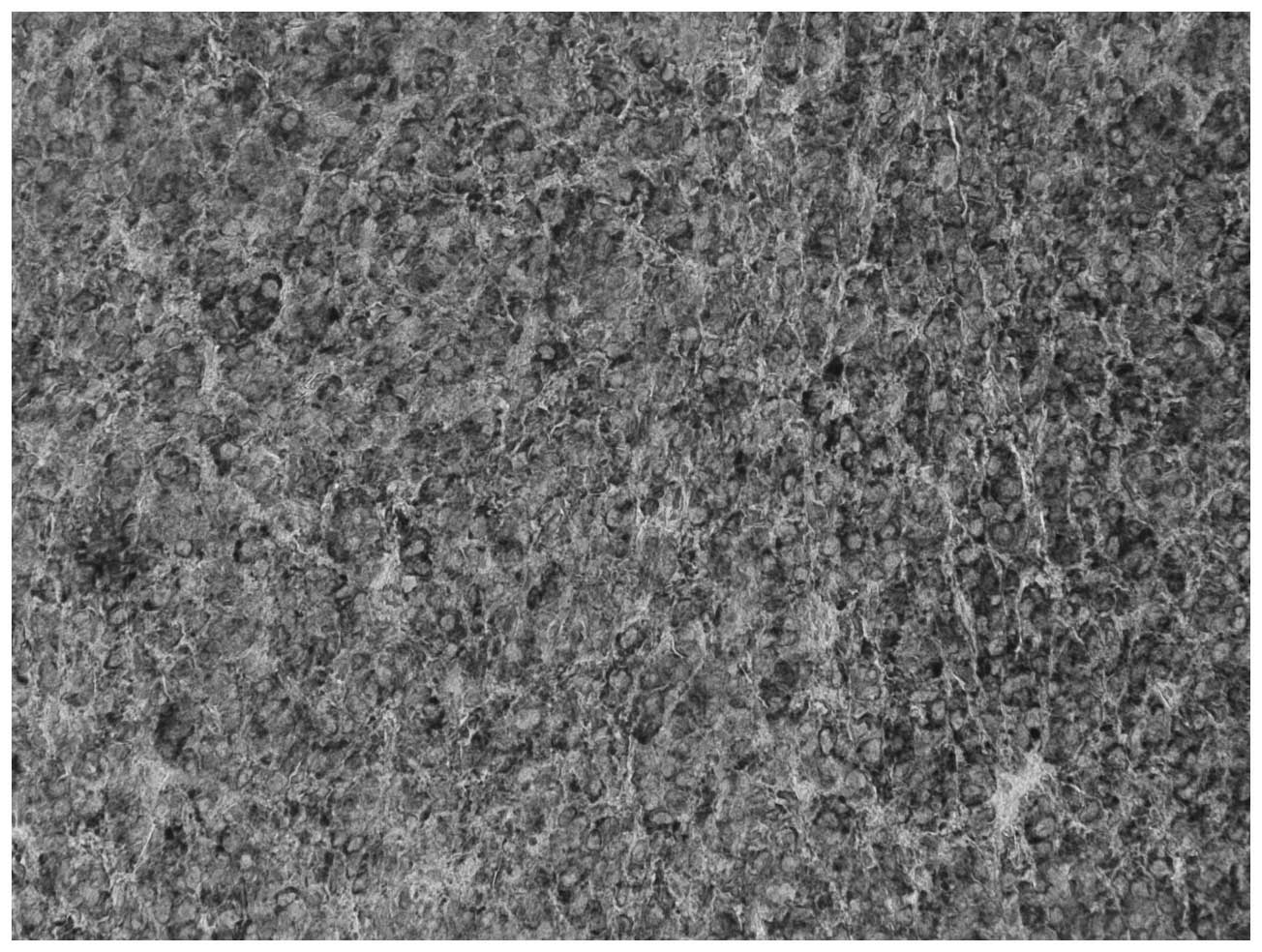
Histopathological examination was performed
postoperatively. Macroscopically, the tumor consisted of a
well-circumscribed, non-encapsulated, ovoid, solid, cystic tumor of
the left ovary measuring 13×8×5.5 cm. Microscopically, the tumor
was composed of nodules of primitive gonadal stroma and exhibited
compact nesting, irregular branching rows and tubules or cysts of
sertoli-like cells separated by fibrous, edematous and hyalinized
stroma with few Leydig-like cells. The tumor cells were pleomorphic
with hyperchromatic nuclei and numerous mitoses (20 per 10 high
power fields). Immunohistochemical staining showed that the tumor
cells were positive for cytokeratin AE1/AE3, vimentin and
α-inhibin. Based on these features, the diagnosis of a
poorly-differentiated SLCT (grade 3) without heterogeneous elements
(Figs. 1–3) was established. SLCTs are divided into
three subtypes: Well, moderately and poorly differentiated SLCTs.
The latter two subtypes may contain heterologous elements, a
retiform component, or both (5,6).
Three courses of chemotherapy with bleomycin (30
mg/dl on days 1, 8 and 15), etoposide (100 mg/m2 on days
1–5) and cisplatin (20 mg/m2 on days 1–5) were
administered to the patient every 21 days following surgery. The
tolerance of the patient to the chemotherapy treatment was
satisfactory, and only minor side effects, such as tiredness, loss
of appetite and temporary hair loss, were observed. Following
chemotherapy, the patient attended follow-up appointments every 3
months, consisting of gynecological clinical examination,
ultrasonography of the pelvis, tumor marker testing and CT imaging
of the abdomen and thorax. At 9 months after the primary surgical
treatment, a suspicious mass was detected in the patient's left
thorax. A pulmonary biopsy was performed (via a left thoracotomy),
which revealed fibrotic tissue and no metastatic disease.
A total of 23 months after the diagnosis of SLCT,
the patient achieved a normal conception. The pregnancy was
uneventful, with no indications of premature labor. At the 38th
week of gestation, the patient vaginally delivered a healthy infant
with a birth weight of 3,750 g. Follow-up of the SLCT was continued
based on pelvic ultrasonography and tumor markers during pregnancy.
CT imaging of the abdomen and thorax was performed prior to
conception (during the follow-up period) and again at the end of
the puerperium period. A total of 36 months after the initial
diagnosis, the patient remains under follow-up and demonstrates no
evidence of recurrent disease. Written informed consent was
obtained from the patient.
Discussion
The disease management strategy for the current case
was designed based on the patient's reproductive age.
Fertility-sparing surgery and adjuvant chemotherapy was the
selected treatment approach. Following treatment, a natural
conception with an uncomplicated pregnancy was achieved during the
patient's follow-up period.
SLCTs are a type of sex-cord stromal tumor of the
ovary and may occur at any age; however, they are most frequently
observed in younger women, creating an issue with regard to the
preservation of fertility (3).
Arrhenoblastoma or androblastoma are terminologies that have been
previously used to describe SLCTs (1). It has been observed that certain SLCTs
are associated with mutations in the dicer 1, ribonuclease type III
gene (7,8). Patients presenting with this type of
SLCT frequently experience a multinodular thyroid goiter or
alternative uncommon tumors, including Wilms' tumors, cervical
rhabdomyosarcoma and pleuropulmonary blastoma, which appear to be
hereditary and may be observed in the family history (7,8).
SLCTs of the ovary are classified into 3 grades
according to their level of differentiation: Grade 1,
well-differentiated; grade 2, moderately-differentiated; and grade
3, poorly-differentiated (9). SLCTs
have been reported to most commonly occur unilaterally (1,10,11). The tumor may present as solid, cystic
or a combination of the two (1). In
the present case, histopathological examination revealed a
poorly-differentiated grade 3 tumor.
The diagnosis of an SLCT of the ovary may require
considerable time and effort. SLCTs may consist of testicular
elements and produce androgens or estrogens (1). Due to androgen secretion, certain SLCT
patients may present with masculinization, with symptoms that
include anovulation, amenorrhea, defeminization, hirsutism,
cliteromegaly, laryngeal protuberance and voice raucity (10). The presence of an ovarian tumor with
clinical signs of hormonal disturbances, particularly in younger
women, should alert clinicians to the potential presence of an
ovarian SLCT. According to a study by Chang et al (12), serum testosterone levels of >200
ng/dl primarily indicate the presence of an androgen-producing
tumor, commonly confined to the adrenal gland or ovary. The time
interval between the oversupply of androgen secretion and the
diagnosis of SLCT typically varies from 6–9 months (1). However, as in the present case, in 1/3
of cases, the patient does not exhibit a hormonal disorder
(13). Precise diagnosis is achieved
via histopathological examination. When handling cases of patients
exhibiting secondary amenorrhea with or without virilization, serum
androgen levels should be measured during diagnostic procedures, as
in certain cases, elevated serum androgen levels may be the only
pre-operative indication of an SLCT. A differential diagnosis for
alternative causes of hyperandrogenemia (Cushing's syndrome,
pituitary tumors or medicine causing androgen hypersecretion)
should be performed (14). In
addition, less frequently observed estrogenic manifestations (for
example, hemorrhage) may be present, particularly in postmenopausal
women, and diagnostic curettage typically reveals an irregular
proliferative endometrium, hyperplasia or endometrial carcinoma
(3).
In certain cases the tumor may be accidentally found
during a routine gynecological ultrasound, when suspicious
abdominal masses may be observed. If the mass is large it may cause
abdominal pain and distension. In addition, rupture of the mass
with acute abdominal pain is possible (10). CT and magnetic resonance imaging have
made a poor contribution to the diagnosis of SLCTs; ~20% of SLCTs
are small in size, and thus unidentifiable, rendering their
accurate diagnosis and localization challenging (10). Furthermore, SLCTs are able to coexist
with alternative types of ovarian tumors, resulting in patients
presenting with mixed symptoms, making diagnosis more challenging.
Previous studies have demonstrated that SLCT is associated with
mucinous adenocarcinoma and a Brenner tumor of the ovary (15,16).
In the present case, the patient was 20 years old at
the time of initial diagnosis. SLCT may be diagnosed at any age,
however, is most frequently observed in younger women of
reproductive age (3). In a
clinicopathological analysis of 207 cases, the average patient age
was 34.5 years (1). In a similar
study of 40 cases, the median patient age was 28 years (10). In a retrospective study of 21 patients
conducted by Sigismondi et al (17), the median patient age was 37 years
(range, 16–76 years).
Well-differentiated SLCTs typically present with
benign behavior (10). Malignancy is
observed in 11% of moderately-differentiated SLCTs (10-year
survival rate, 87%) and 59% of poorly-differentiated SLCTs (10-year
survival rate, 41%). Furthermore, the 5-year overall survival rate
in cases of stage I disease is almost 92% (17). The primary treatment for SLCTs is
surgery, based on the patient age, disease stage and tumor grade
(6,9).
However, a significant issue arising from disease occurrence in
patients of reproductive age is the preservation of fertility
(afforded by a cystectomy/adnexectomy with preservation of the rest
of the female genital tract). Hysterectomy with bilateral
salpingo-oophorectomy, as well as staging surgery (cytology,
omentectomy, pelvic-paraaortic lymphadenectomy or peritoneal
biopsies), is the optimal approach for patients beyond childbearing
age, although the necessity of a lymphadenectomy remains
controversial (17). Brown et
al (w) demonstrated that in SLCTs, lymph node metastasis is
markedly reduced, and sampling of retroperitoneal nodes may be
omitted. However, for young women, fertility-sparing surgery (with
or without staging surgery) is required, particularly for patients
exhibiting stage I disease (1,17).
Chemotherapy may be administered following surgical treatment,
particularly for tumors demonstrating poor or moderate
differentiation (10). According to
Gui et al (10), adjuvant
chemotherapy does not provide any significant advantages, and it
should be considered primarily in cases of poorly- and
moderately-differentiated tumors or disease recurrence.
Additionally, a previous study (MITO) was able to demonstrate the
benefit of the administration of post-operative chemotherapy for
patients exhibiting advanced stage (II–IV) disease (17).
In conclusion, SLCTs of the ovary present with a
wide range of biological and histopathological features. Precise
treatment is based on patient age, tumor differentiation and
disease stage. Overall the prognosis of SLCTs is good, particularly
in stage I cases, although recurrence may be observed, most
commonly in patients exhibiting tumors with moderate or poor
differentiation. However, in younger patients conservative surgery
for the preservation of fertility is an acceptable approach, which
may lead to successful and uneventful conception and pregnancy, as
in the present case. Close follow-up must be undertaken in order to
monitor the risk of disease recurrence.
Glossary
Abbreviations
Abbreviations:
|
SLCTs
|
Sertoli-Leydig cell tumors
|
|
CT
|
computed tomography
|
References
|
1
|
Young RH and Scully RE: Ovarian
Sertoli-Leydig cell tumors. A clinicopathological analysis of 207
cases. Am J Surg Pathol. 9:543–569. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tomlinson MW, Treadwell MC and Deppe G:
Platinum based chemotherapy to treat recurrent Sertoli-Leydig cell
ovarian carcinoma during pregnancy. Eur J Gynaecol Oncol. 18:44–46.
1997.PubMed/NCBI
|
|
3
|
Sachdeva P, Arora R, Dubey C, Sukhija A,
Daga M and Singh DK: Sertoli-Leydig cell tumor: A rare ovarian
neoplasm. Case report and review of literature. Gynecol Endocrinol.
24:230–234. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Litta P, Saccardi C, Conte L, Codroma A,
Angioni S and Mioni R: Sertoli-Leydig cell tumors: Current status
of surgical management: Literature review and proposal of
treatment. Gynecol Endocrinol. 29:412–417. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Young R: Sex cord-stromal, steroid cell,
and other ovarian tumors with endocrine, paraendocrine, and
paraneoplastic manifestations. Blaustein's Pathology of the Female
Genital Tract. Kurman RJ, Hedrick Ellenson L and Ronnett BM: (6th).
Springer-Verlag. (New York, NY). 8152011.
|
|
6
|
National Comprehensive Cancer Network
(NCCN): NCCN Clinical Practice Guidelines in Oncology: Ovarian
Cancer. 2013.https://www.nccn.org/professionals/physician_gls/f_guidelines.aspAccessed.
November 24–2014
|
|
7
|
Rio Frio T, Bahubeshi A, Kanellopoulou C,
Hamel N, Niedziela M, Sabbaghian N, Pouchet C, Gilbert L, O'Brien
PK, Serfas K, et al: DICER1 mutations in familial multinodular
goiter with and without ovarian Sertoli-Leydig cell tumors. JAMA.
305:68–77. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Slade I, Bacchelli C, Davies H, Murray A,
Abbaszadeh F, Hanks S, Barfoot R, Burke A, Chisholm J, Hewitt M, et
al: DICER1 syndrome: Clarifying the diagnosis, clinical features
and management implications of a pleiotropic tumour predisposition
syndrome. J Med Genet. 48:273–278. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Meyer R: The pathology of some special
ovarian tumors and their relation to sex characteristics. Am J
Obstet Gynecol. 22:697–713. 1931. View Article : Google Scholar
|
|
10
|
Gui T, Cao D, Shen K, Yang J, Zhang Y, Yu
Q, Wan X, Xiang Y, Xiao Y and Guo L: A clinicopathological analysis
of 40 cases of ovarian Sertoli-Leydig cell tumors. Gynecol Oncol.
127:384–389. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Novak ER and Long JH: Arrhenoblastoma of
the ovary. Am J Obstet Gynecol. 92:1082–1093. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chang PL, Lindheim SR, Lowre C, Ferin M,
Gonzalez F, Berglund L, Carmina E, Sauer MV and Lobo RA: Normal
ovulatory women with polycystic ovaries have hyperandrogenic
pituitary-ovarian responses to gonadotropin-releasing
hormone-agonist testing. J Clin Endocrinol Metab. 85:995–1000.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lenhard M, Kuemper C, Ditsch N, Diebold J,
Stieber P, Friese K and Burges A: Use of novel serum markers in
clinical follow-up of Sertoli-Leydig cell tumours. Clin Chem Lab
Med. 45:657–661. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fleckenstein G, Sattler B, Hinney B,
Wuttke W, Osmers R and Emons G: Androblastoma of the ovary:
Clinical, diagnostic and histopathologic features. Onkologie.
24:286–291. 2001.(In German). PubMed/NCBI
|
|
15
|
Virk R and Lu D: Mucinous adenocarcinoma
as heterologous element in intermediately differentiated
Sertoli-Leydig cell tumor of the ovary. Pathol Res Pract.
206:489–492. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Persechini ML, Motton S, Leguevaque P,
Donadille F, Escourrou G, Vierasu B, Hamdi S, Bennet A and Caron P:
Virilising ovarian tumour: A case associating a Sertoli-Leydig cell
tumour and a Brenner tumour. Gynecol Endocrinol. 27:345–350. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sigismondi C, Gadducci A, Lorusso D,
Candiani M, Breda E, Raspagliesi F, Cormio G, Marinaccio M and
Mangili G: Ovarian Sertoli-Leydig cell tumors. A retrospective MITO
study. Gynecol Oncol. 125:673–676. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brown J, Sood AK, Deavers MT, Milojevic L
and Gershenson DM: Patterns of metastasis in sex cord-stromal
tumors of the ovary: Can routine staging lymphadenectomy be
omitted? Gynecol Oncol. 113:86–90. 2009. View Article : Google Scholar : PubMed/NCBI
|