Introduction
Urothelial carcinoma (UC) arising from the renal
pelvis or the ureter is uncommon in Western countries (1), accounting for ~7% of all kidney tumors
and ~5% of all urothelial tumors (2).
Despite the frequency of microscopic vascular invasion in UC, tumor
thrombus into the renal vein or inferior vena cava (IVC) is a rare
occurrence (3), with no more than 30
cases reported in the literature to date (1). Even more limited are reports of renal UC
with pancreatic infiltration, with only one case reported (4). Isolated adrenal metastasis from UC is
also rare (5).
The present study reports an rare case of
synchronous massive renal UC with renal vein tumor thrombus,
pancreatic infiltration and a solitary adrenal metastasis. This
study was approved by Ethics Committee of West China Hospital,
Sichuan University.
Case report
A 49-year-old female patient presented to the West
China Hospital, Sichuan University (Chengdu, China) in March 2014
with a 9-month history of repeated left flank pain and gross
hematuria. Symptoms were controlled by the administration of
antibiotics and a weight loss of ~4 kg was observed during this
9-month period. Upon admission in March 2014, physical examination
results were normal. Laboratory test results indicated anemia
(hemoglobin, 66 g/l; normal range, 115–150 g/l) and leukocytosis
[white blood cell (WBC) count, 13.95×109/l; normal
range, 3.5–9.5×109/l], and urinalysis revealed hematuria
[red blood cells, 52/high power field (HP); normal range, 0–3/HP],
leukocyturia (WBCs, 39/HP; normal range, 0–5/HP) and pyuria
(pyocytes, 5/HP; normal value, 0/HP); however, blood and urine
cultures were sterile, and urinary cytology showed no malignant
cells. All other laboratory test results were within the normal
ranges.
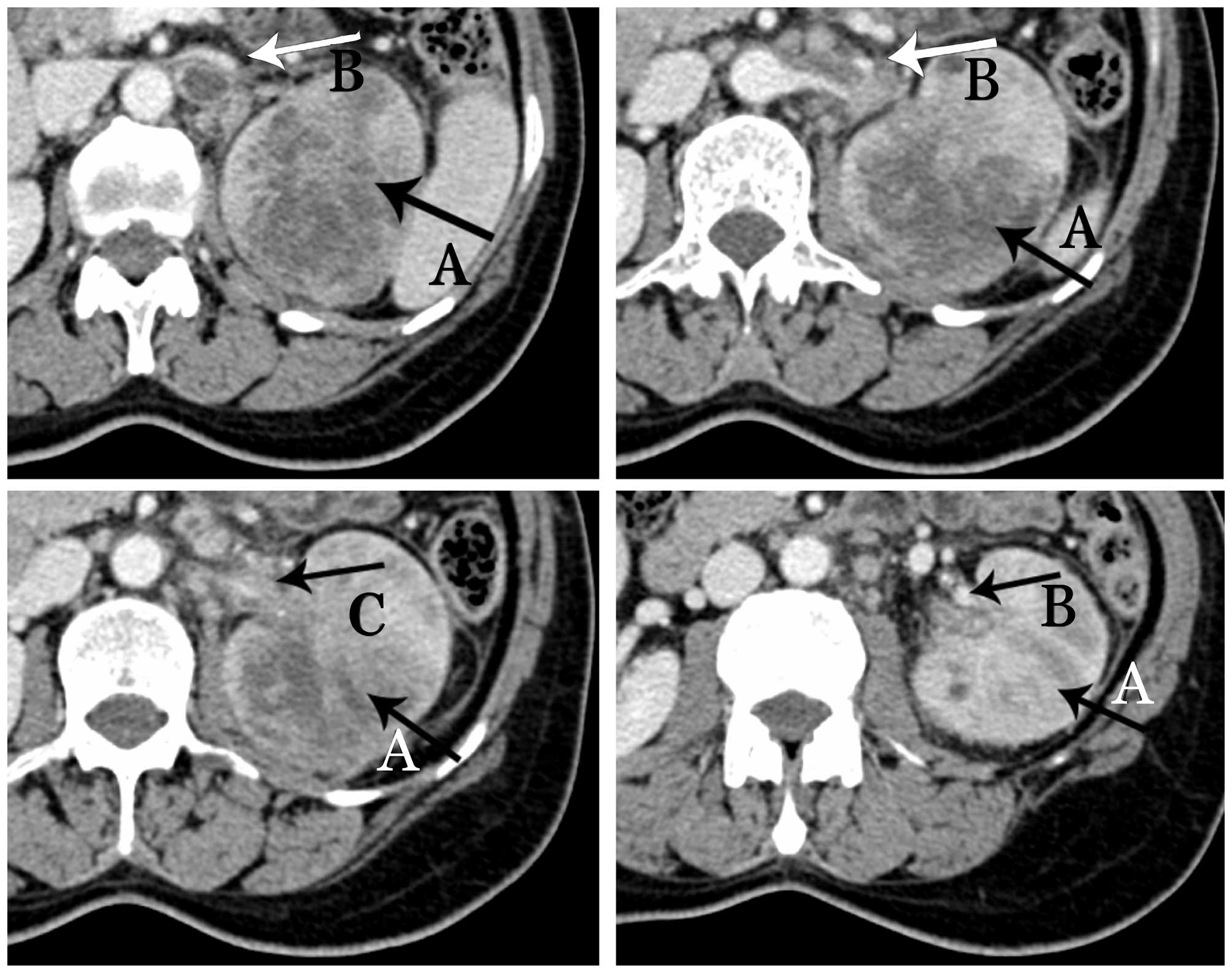
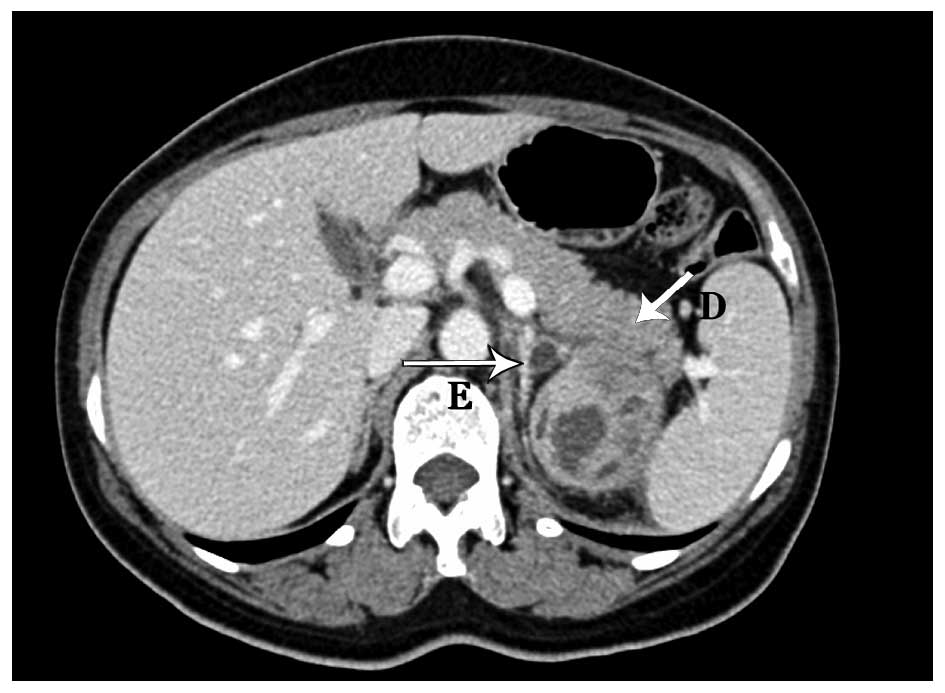
Contrast-enhanced computed tomography (CT) scans
revealed a mixed-density mass (6.9×5.9×7.7 cm) in the upper pole of
the left kidney with left renal vein invasion (Figs. 1 and 2)
and possible infiltration of the pancreatic tail (Fig. 3). The left adrenal gland was thickened
with a clear boundary, and a low-density nodule in the adrenal
bifurcation was detected (Fig. 3).
Dynamic radionuclide renal imaging showed severely impaired left
renal function. The preliminary diagnosis was left-sided renal cell
carcinoma (RCC) combined with renal vein thrombus with suspected
pancreatic infiltration and left adrenal metastasis.
Left radical nephrectomy, distal pancreatectomy and
ipsilateral adrenalectomy were performed in March 2014. In
addition, the splenic hilum was observed to be surrounded by
reactive fibrotic tissue. The two tissues were difficult to
separate, therefore, splenectomy was also performed.
Histopathological examination of the kidney, pancreatic tail and
adrenal gland were conducted. Tissues were fixed with
paraformaldehyde, paraffin-embedded, and cut into 5-mm sections.
Immunohistochemical studies using the avidin-biotin-complex
immunoperoxidase technique were performed. The following
commercially available antibodies were used: Pan cytokeratin (CK)
(cat. no. C2931; Sigma-Aldrich, St. Louis, MO, USA), P63 (cat. no.
SRP5112; Sigma-Aldrich), CK5 (cat. no. ab52635; Abcam, Cambridge,
MA, USA), CK6 (cat. no. ab124821; Abcam), CK7 (cat. no. ab82253;
Abcam), CK20 (cat. no. ab76126; Abcam), CD10 (cat. no. ab126593;
Abcam) and RCC1 (cat. no. ab109379; Abcam). Appropriate positive
and negative controls were run concurrently for all the markers
tested. The findings revealed poorly differentiated carcinoma, and
immunohistochemical staining revealed positivity for panCK, P63,
CK5, CK6, CK7 and CD10 and negativity for RCC1 CK20, which
indicated high-grade UC. The thrombus arose from the UC, which had
histologically invaded the wall of the renal vein.
The patient was excluded from chemotherapy due to
personal reluctance and poor postoperative physical condition.
Postoperative CT scans performed 3 months after the surgery
detected tumor recurrence and metastasis in several sites,
including in the lung, retroperitoneal space, pancreatic resection
margin and psoas muscle. The patient succumbed during follow-up 1
month later.
Discussion
With the development of novel diagnostic modalities,
the preoperative diagnosis of a renal tumor with renal vein or IVC
tumor thrombus, as well as the assessment of the infiltrating range
of the tumor, are relatively simple; however, distinguishing UC
from RCC remains a challenge. Urinary cytological analysis was
reported to have a diagnostic accuracy of 59%, but with a high
ratio of false negatives for malignancy (5). A CT scan finding of preserved reniform
kidney shape by an infiltrating neoplastic process supports the
diagnosis of UC (2). In addition to
CT and magnetic resonance urography, flexible ureteroscopy
techniques, fluorescent in situ hybridization and
narrow-band imaging may also facilitate diagnosis, and have thus
been widely accepted (6). However,
none of these methods is sufficiently accurate or effective for
differentiating UC from RCC; therefore, intraoperative frozen
section examination is recommended and additional attention must be
paid to the renal neoplasm to determine the most appropriate
surgical strategy, as surgical strategies for RCC and UC
differ.
Therapeutic strategies for UC vary. Despite the
associated toxicity, platinum-based chemotherapy is currently the
primary treatment option for upper tract UC; however, certain
studies have reported that it has no impact on survival (6) and resulted in repeated relapses, even
following an initial response to systemic chemotherapy (7,8).
Furthermore, surgical excision of metastatic UCs
with curative intent has been introduced as a treatment strategy,
and the results of several studies have proposed adrenalectomy for
isolated or multiple adrenal metastases (4,7,8). Several case reports and small-scale
studies have also favored pancreatic metastasectomy, particularly
for primary RCC (9,10); however, studies regarding UC are
lacking. According to Nikfarjam et al (3), right nephrectomy combined with
pancreaticoduodenectomy was performed in a single case of adhesion
of renal UC to the duodenal wall, resulting in a disease-free
condition for 3 months. Therefore, distal pancreatectomy and
adrenalectomy should be considered in the setting of pancreatic
infiltration and adrenal metastasis arising from UC.
Notably, the present case posed an additional
challenge due to the presence of a tumor thrombus. According to the
literature, aggressive surgery for the removal of an IVC thrombus
proven beneficial for patients with RCC; however, its value in the
management of renal UC remains unclear, due to limited data and the
aggressive nature of UC (1,2). Existing data indicates that patients who
present with UC and an IVC tumor thrombus have a poor prognosis,
despite aggressive radical nephrectomy or nephroureterectomy, as
the majority of patients succumbed within 6 months of the initial
diagnosis (2). Although no benefits
of surgery have been reported in such advanced cases of UC
(6), surgical intervention may serve
as a palliative treatment option or as a means to decrease the risk
of thrombus shedding, as in the present case.
The current case indicates that cases of late-stage
aggressive renal UC, characterized by massive renal UCs with renal
vein tumor thrombi, pancreatic infiltration and adrenal metastasis,
may not benefit from surgery or chemotherapy; therefore, strategies
aimed at the early identification and treatment of such cases are
required.
In conclusion, it is crucial to distinguish UC from
RCC in order to determine the appropriate surgical treatment
strategy; however, differential diagnosis remains a challenge.
Furthermore, the present case and those in the literature indicate
that massive renal UC with tumor thrombus, organ infiltration and
metastasis is associated with a poor prognosis, regardless of
whether surgery or chemotherapy is used.
Acknowledgements
The present study was supported by the Science &
Technology Pillar Program of Sichuan Province (grant no.
2012SZ0009), the 2013 Young Investigator Award of the Prostate
Cancer Foundation, and the Project of Natural Science Foundation of
China (grant no. 81300627). The authors would also like to thank
Enago (New York, NY, USA) for their assistance in the revision of
this manuscript.
Glossary
Abbreviations
Abbreviations:
|
UC
|
urothelial carcinoma
|
|
IVC
|
inferior vena cava
|
|
CT
|
computed tomography
|
|
RCC
|
renal cell carcinomas
|
References
|
1
|
Tseng YS, Chen KH, Chiu B, Chen Y and
Chung SD: Renal urothelial carcinoma with extended venous thrombus.
South Med J. 103:813–814. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Miyazato M, Yonou H, Sugaya K, Koyama Y,
Hatano T and Ogawa Y: Transitional cell carcinoma of the renal
pelvis forming tumor thrombus in the vena cava. Int J Urol.
8:575–577. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nikfarjam M, Gusani NJ, Kimchi ET, Mahraj
RP and Staveley-O'Carroll KF: Combined right nephrectomy and
pancreaticoduodenectomy. Indications and outcomes. JOP. 9:449–455.
2008.PubMed/NCBI
|
|
4
|
Washino S, Hirai M, Matsuzaki A and
Kobayashi Y: Long-term survival after adrenalectomy for
asynchronous metastasis of bladder cancer to the bilateral adrenal
glands. Case Rep Urol. 2012:4252302012.PubMed/NCBI
|
|
5
|
Ljungberg B, Stenling R, Osterdahl B,
Farrelly E, Aberg T and Roos G: Vein invasion in renal cell
carcinoma: Impact on metastatic behavior and survival. J Urol.
154:1681–1684. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rouprêt M, Babjuk M, Compérat E, Zigeuner
R, Sylvester R, Burger M, Cowan N, Böhle A, Van Rhijn BW, Kaasinen
E, et al: European guidelines on upper tract urothelial carcinomas:
2013 update. Eur Urol. 63:1059–1071. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Siefker-Radtke AO, Walsh GL, Pisters LL,
Shen Y, Swanson DA, Logothetis CJ and Millikan RE: Is There a role
for surgery in the management of metastatic urothelial cancer? The
M. D. Anderson Experience. J Urol. 171:145–148. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lehmann J, Suttmann H, Albers P, Volkmer
B, Gschwend JE, Fechner G, Spahn M, Heidenreich A, Odenthal A, Seif
C, et al: Surgery for metastatic urothelial carcinoma with curative
intent: The German experience (AUO AB 30/05). Eur Urol.
55:1293–1299. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Machado NO and Chopra P: Pancreatic
metastasis from renal carcinoma managed by Whipple resection. A
case report and literature review of metastatic pattern, surgical
management and outcome. JOP. 10:413–418. 2009.PubMed/NCBI
|
|
10
|
Reddy S and Wolfgang CL: The role of
surgery in the management of isolated metastases to the pancreas.
Lancet Oncol. 10:287–293. 2009. View Article : Google Scholar : PubMed/NCBI
|