Introduction
Lynch syndrome or hereditary non-polyposis
colorectal cancer, is an autosomal dominant condition that
predisposes individuals to multiple cancer types and is caused by
germline mutations in one of the mismatch repair genes, usually
(mutL homolog 1 (MLH1), or mutS homolog (MSH)2 or MSH6 (1–3). Affected
individuals are highly susceptible to colorectal and endometrial
cancer, but also to cancers of the stomach, ovary, urinary tract,
hepatobiliary tract, pancreas, and small bowel. In Lynch syndrome,
the risk of developing small bowel cancer within a lifetime is ~4%
(4), which is almost identical to the
risk of developing colorectal cancer for individuals in the general
population (5). A lack of effective
screening methods and the relative paucity of presenting symptoms
contribute to a high percentage of cases at the advanced stage at
the time of diagnosis in small bowel cancer (6). Small bowel adenocarcinoma has a poor
prognosis at all stages, with a 5-year overall survival rate
ranging from 14–33% (7). The present
study describes the case of a patient with small bowel
adenocarcinoma and Lynch syndrome, in whom ascending colon cancer
was diagnosed 1 month earlier. This case highlights the requirement
to consider the extracolonic manifestations of Lynch syndrome,
particularly in patients with upper bowel obstruction, abdominal
pain or occult gastrointestinal bleeding.
Case report
A 51-year-old man was admitted to Department of
Gastroenterology, Kunshan First People's Hospital Affiliated to
Jiangsu University (Kunshan, Jiangsu, China) on September 16, 2014,
due to upper abdominal discomfort after eating and consequent
anorexia that had persisted for 2 weeks. The patient's past medical
history included an endoscopic resection of a 15-mm early-stage
colorectal cancer from the ascending colon on July 30, 2014. A
stool test was positive for fecal occult blood. An
esophagogastroduodenoscopy and colonoscopy were unremarkable. A
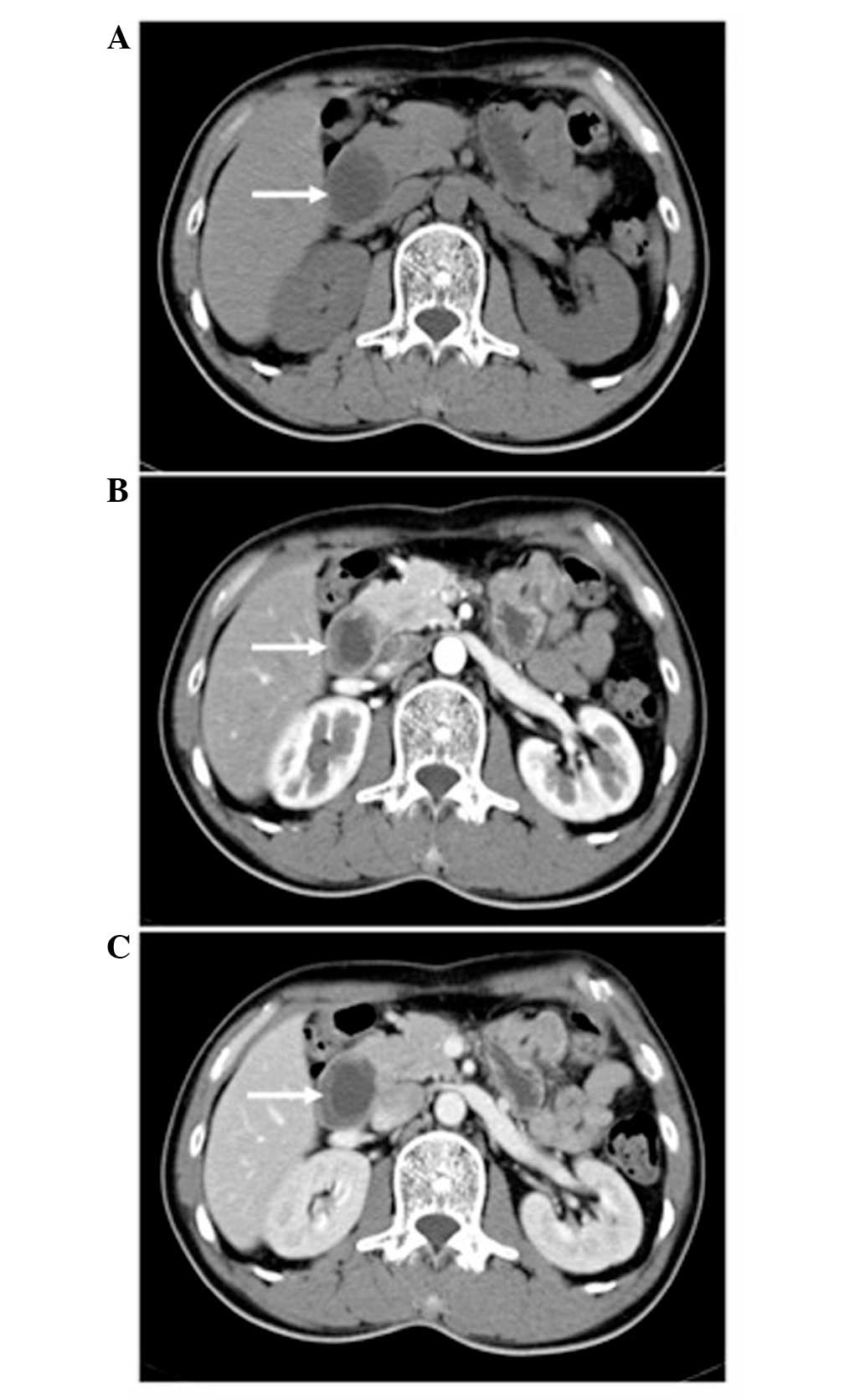
subsequent contrast-enhanced abdominal computed tomography (CT)
scan was required, which demonstrated an obstructing mass in the
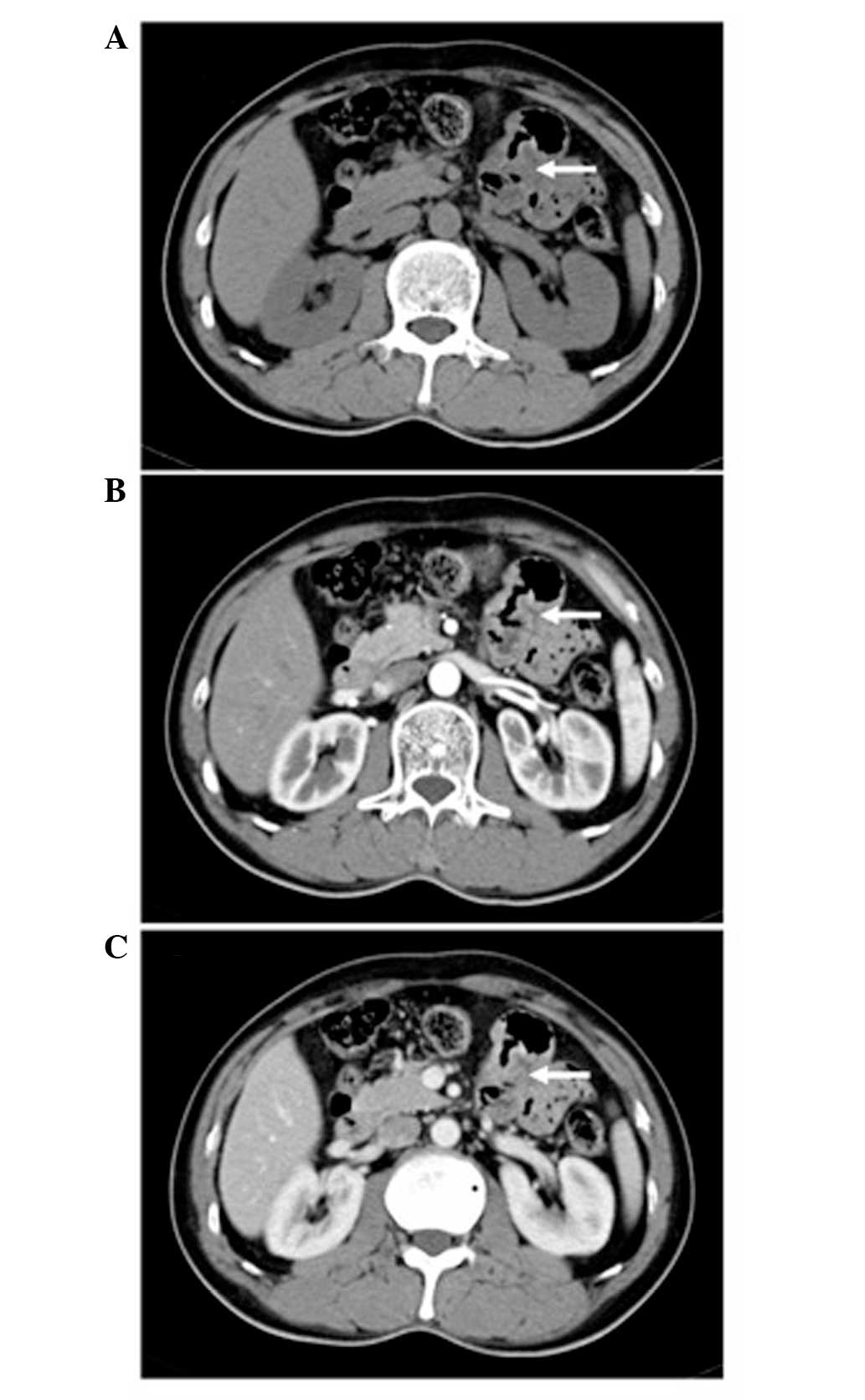
proximal jejunum leading to expansion of the duodenum (Fig. 1). Upon review of the abdominal CT scan
that had been performed at the time of the endoscopic resection 1
month previously, the mucosal thickening of the small intestine was
found to have already existed, although it was not so marked
(Fig. 2).
A laparotomy was performed, resulting in the
resection of a small bowel mass and its surrounding tissue with the
primary anastomosis. The surgery was without complication and
post-operative management was uneventful. The histology report
demonstrated a moderately-differentiated adenocarcinoma partially
comprised of a poorly-differentiated region. The microscopic
findings showed cell clusters and cords with marked tissue
structure atypia and invasion of the the visceral peritoneum, and
metastases of 5/18 lymph nodes. The definitive diagnosis was
primary adenocarcinoma of the duodenal-jejunal junction, T4N1M0,
stage III according to the Tumor-Node-Metastasis classification of
malignant tumors (American Joint Committee on Cancer) (8,9).
Subsequent genetic testing confirmed the germline mutation of MLH1.
DNA was extracted by the use of a High Pure Polymerase Chain
Recation (PCR) Template Purification kit (Roche Diagnostics,
Mannheim, Germany). DNA isolation from whole blood of the patient
and their relatives DNA was extracted with the use of QIAamp DNA
Blood Midi or Mini kits (Qiagen, Hilden, Germany), according to the
manufacturer's instructions. All coding exons of the MLH1 gene were
amplified by polymerase chain reaction. PCR products were purified
and sequenced in both directions. Sequencing reactions were
performed using BigDye terminator cycle sequencing kit v.3.1
(Applied Biosystems, Foster City, CA, USA). The products of the
sequencing reactions were run and analyzed using an ABI-PRISM 3130
Genetic Analyzer (Perkin Elmer, Boston, MA, USA). Large deletion
detection multiple ligation-dependent probe amplification (MLPA)
genomic deletions were tested using SALSA MLPA kit P003 MLH/MSH2
(MRC-Holland BV, Amsterdam, Netherlands) according to the
manufacturer's instructions. The amplification products were
analyzed by capillary gel electrophoresis (ABI-3130). Deletion of
one copy of a probe targeted sequence was stated if the relative
peak area for that probe amplification product had been reduced by
35–55% compared with a negative control sample.
Genetic testing had no effect on the follow-up
treatment, and there was no associated targeted drug on the market.
The patient therefore received 6 cycles of an adjuvant folinic
acid, fluorouracil and ocaliplatin chemotherapy regimen. The latest
CT scan, 16 months after the chemotherapy, did not show any
recurrence.
Combined with patient medical history, these results
meant that the patient was diagnosed with small bowel carcinoma,
revealing Lynch syndrome.
Discussion
Small bowel adenocarcinomas are rare and account for
~2% of all gastrointestinal tumors (10). The incidence of small bowel
adenocarcinomas is more frequent in certain hereditary syndromes,
including familial adenomatous polyposis, Peutz-Jeghers syndrome
and Lynch syndrome (11). Small bowel
cancer is the first malignant manifestation of Lynch syndrome, and
it generally occurs 10–20 years earlier in these patients compared
with individuals in the general population (11,12). In
Lynch syndrome, the risk of developing small bowel cancer within a
lifetime is almost identical to the risk of developing colorectal
cancer for individuals in the general population (4,13). In the
case of Lynch syndrome, the risk of developing small bowel
adenocarcinoma has been estimated at 1–4% (14). Small bowel adenocarcinoma has a poor
prognosis, with the 5-year overall survival rate not exceeding 30%
(15). Clinical symptoms are
frequently non-specific, which explains a late diagnosis at stages
T3 and T4 in the majority of cases. The present case highlights the
requirement to consider the extracolonic manifestations of Lynch
syndrome, particularly in patients with upper bowel obstruction,
abdominal pain or occult gastrointestinal bleeding. Screening for
small bowel cancer is generally recommended (4).
Small bowel tumors are often not visualized by both
esophagogastroduodenoscopy and colonoscopy in the first instance,
and further investigations to visualise the small bowel are
crucial, generally in the form of magnetic resonance enterography,
CT colonography or wireless capsule endoscopy, which have all been
shown to be effective in reaching the diagnosis (16). The treatment of small bowel
adenocarcinoma remains centered around radical surgical resection
(6). A complete resection of the
disease is one of the most important prognostic factors for a
patient's survival, and adjuvant chemotherapy is also necessary
(2). Previous studies have suggested
that chemotherapy is common and beneficial in small bowel
adenocarcinoma (17), but the optimal
chemotherapy regimen and the degree of benefit remain to be
defined.
In conclusion, small bowel adenocarcinoma can be the
first and the only manifestation of Lynch syndrome. A sound
approach to investigate the difference between small bowel
adenocarcinoma in individuals with Lynch syndrome and small bowel
adenocarcinoma in the general population is urgently required.
Patients with Lynch syndrome generally present with small bowel
cancer 10–20 years earlier than the general population, and small
bowel cancer may be the first clinical manifestation of Lynch
syndrome. The present study describes the case of a patient with
small bowel adenocarcinoma and Lynch syndrome, in whom ascending
colon cancer was diagnosed 1 month earlier. In view of the improved
accessibility of the small bowel with the introduction of capsule
endoscopy and double balloon enteroscopy, the question of whether
patients should be screened for small bowel neoplasia has regained
attention.
References
|
1
|
Coco D, Leanza S and Boccoli G: Small
bowel adenocarcinoma (SBA) three years after colonic adenocarcinoma
in an elderly patient: Case report in a National Institute of
Health and Aging (INRCA) and review of the literature. Int J Surg
Case Rep. 5:939–943. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chaaya A and Heller SJ: Introduction to
small bowel tumors. Tech Gastrointest Endosc. 14:88–93. 2012.
View Article : Google Scholar
|
|
3
|
Tanyi M, Olasz J, Tanyi JL, Tóth L,
Antal-Szalmás P, Ress Z, Bubán T, Palatka K, András C, Urbancsek H,
et al: MLH1 and MSH2 mutation screening in HNPCC families of
Hungary-Two new MMR gene mutations. Eur J Surg Oncol. 40:1445–1452.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Koornstra JJ, Kleibeuker JH and Vasen HF:
Small-bowel cancer in Lynch syndrome: Is it time for surveillance?
Lancet Oncol. 9:901–905. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Marmo R, Rotondano G, Riccio G, D'Angella
R, Rescinito M, Rescinito A, Bianco MA and Cipolletta L:
Small-bowel adenocarcinoma diagnosed via capsule endoscopy in a
patient found to have hereditary nonpolyposis colorectal cancer.
Gastrointest Endosc. 65:524–525. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Delaunoit T, Neczyporenko F, Limburg PJ
and Erlichman C: Small bowel adenocarcinoma: A rare but aggressive
disease. Clin Colorectal Cancer. 4:241–251. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bilimoria KY, Bentrem DJ, Wayne JD, Ko CY,
Bennett CL and Talamonti MS: Small bowel cancer in the United
States: Changes in epidemiology, treatment, and survival over the
last 20 years. Ann Surg. 249:63–71. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Overman MJ: Recent advances in the
management of adenocarcinoma of the small intestine. Gastrointest
Cancer Res. 3:90–96. 2009.PubMed/NCBI
|
|
9
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM Classification of Malignant Tumours (7th). Wiley Blackwell.
New York: 153–159. 2009.
|
|
10
|
Aparicio T, Zaanan A, Svrcek M,
Laurent-Puig P, Carrere N, Manfredi S, Locher C and Afchain P:
Small bowel adenocarcinoma: Epidemiology, risk factors, diagnosis
and treatment. Dig Liver Dis. 46:97–104. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Umman P, Adiyodi V and Narayan C: Small
bowel adenocarcinoma - report of two cases and review of
literature. Indian J Surg. 75:123–127. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jovanovic I, Fry LC and Mönkemüller K:
Small-bowel adenocarcinoma. Clin Gastroenterol Hepatol. 9:A282011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Babba T, Schischmanoff O, Lagorce C, Wind
P, Des Guetz G, Aparicio T and Benamouzig R: Small bowel carcinoma
revealing HNPCC syndrome. Gastroenterol Clin Biol. 34:325–328.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Aarnio M, Sankila R, Pukkala E, Salovaara
R, Aaltonen LA, de la Chapelle A, Peltomäki P, Mecklin JP and
Järvinen HJ: Cancer risk in mutation carriers of DNA
mismatch-repair genes. Int J Cancer. 81:214–218. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vasen HF, Wijnen JT, Menko FH, Kleibeuker
JH, Taal BG, Griffioen G, Nagengast FM, Meijers-Heijboer EH,
Bertario L, Varesco L, et al: Cancer risk in families with
hereditary non polyposis colorectal cancer diagnosed by mutation
analysis. Gastroenterology. 110:1020–1027. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kunizaki M, Hidaka S, Isomoto H, Takeshita
H, Nanashima A, Sawai T, Yasutake T and Nagayasu T: Diagnosis of
small-bowel metastasis of hepatocellular carcinoma by
double-balloon enteroscopy. Int J Surg Case Rep. 3:263–265. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Czaykowski P and Hui D: Chemotherapy in
small bowel adenocarcinoma: 10-year experience of the British
Columbia Cancer Agency. Clin Oncol (R Coll Radiol). 19:143–149.
2007. View Article : Google Scholar : PubMed/NCBI
|