Introduction
Breast cancer represents a major health problem and
is the most common malignancy among women, with 400,000 new cases
being diagnosed each year worldwide (1). A total of 232,000 women were diagnosed
with breast cancer in 2014 in the United States, corresponding to
~28.6% of all cancer incidents among women (1). Breast cancer is responsible for 40,000
mortalities annually and the lifetime risk of succumbing to the
disease is ~3.4% (1). Despite novel
approaches in the therapeutic management of breast cancer,
including surgical treatment, and additional chemotherapy and
radiation therapy, metastatic disease remains a great clinical
challenge, and the therapeutic arsenal remains inadequate in
impeding relapse and metastasis. Therefore, novel predictive
markers are required to identify high-risk patients who may develop
metastases during postoperative surveillance, which may permit
oncologists to utilize more efficient patient-tailored treatment
strategies.
Systemic inflammatory response has been identified
to affect survival in a number of malignancies (2,3). White
blood cells are key mediators in this response (2), in addition to platelets, which are
involved in mechanisms promoting tumor growth and metastasis
(4–6).
Various white blood cell and platelet indices, including
neutrophil-to-lymphocyte ratio, platelet count, mean platelet
volume and platelet-to-lymphocyte ratio, have been reported as
potential markers for predicting the progression or recurrence of
disease and/or overall survival in several forms of cancer
(7–10). The present study aimed to investigate
whether changes in white blood cell and platelet indices possess
prognostic value regarding the development of distant metastases in
patients with newly diagnosed breast cancer.
Patients and methods
Patients
A total of 90 female patients (mean age, 58.6 years;
range, 28–86 years) with newly diagnosed, non-metastatic invasive
ductal breast carcinoma, who were treated in the Breast Unit,
Second Department of Propaedeutic Surgery, Athens Medical School,
University of Athens (Athens, Greece) between February 2005 and
December 2014, were included in the current study. Of these
patients, 53 (mean age, 55.9 years; range, 28–84 years) developed
metastasis at a distant site during the surveillance period and
were categorized as the metastasis group, while 37 patients (mean
age, 62.5 years; range, 31–86 years) did not develop distant
metastasis during surveillance and were used as a control group.
The two groups were matched for age, disease stage and duration of
surveillance. Data regarding white blood cell count, neutrophil
count, neutrophil percentage, lymphocyte count, lymphocyte
percentage, neutrophil-to-lymphocyte ratio, platelet count, mean
platelet volume, platelet distribution width, plateletcrit,
platelet-to-neutrophil ratio and platelet-to-lymphocyte ratio was
retrospectively collected from complete blood count tests performed
upon admission to the Breast Unit. In addition, clinical data
concerning age, type of surgery and development of distant
metastasis during the follow-up period was obtained, along with
pathological data regarding tumor diameter, extent of primary tumor
infiltration (T), number of infiltrated lymph nodes, degree of
lymph node infiltration (N), tumor-node-metastasis stage (11), grade, presence or absence of
lymphovascular invasion, and status of estrogen receptors,
progesterone receptors and c-erb-B2 expression, which was collected
from the pathology reports of excised specimens.
Clinicopathological parameters of the patients are listed in
Table I. The present study conforms
to the Declaration of Helsinki.
 | Table I.Clinicopathological data of patients
with invasive ductal breast carcinoma. |
Table I.
Clinicopathological data of patients
with invasive ductal breast carcinoma.
| Parameters | n, % |
|---|
| Tumor stage |
|
| T1 | 28 (31.1) |
| T2 | 45 (50.0) |
| T3 | 9
(10.0) |
| T4 | 8 (8.9) |
| Lymph node
infiltration |
|
| N0 | 42 (46.7) |
| N1 | 16 (17.8) |
| N2 | 12 (13.3) |
| N3 | 20 (22.2) |
| TNM
stagea |
|
| I | 23 (25.6) |
| II | 33 (36.7) |
| III | 34 (37.8) |
| Tumor grade |
|
| Low | 49 (54.4) |
| High | 41 (45.6) |
| Estrogen receptor
expression |
|
|
Positive | 61 (67.8) |
|
Negative | 29 (32.2) |
| Progesterone receptor
expression |
|
|
Positive | 46 (51.1) |
|
Negative | 44 (48.9) |
| c-erb-B2
expression |
|
|
Positive | 49 (54.4) |
|
Negative | 41 (45.6) |
Complete blood count measurement
A total of 3 ml blood was collected in EDTA
Vacutainer® Tubes from each patient. All specimens were
processed using an XT-4000i Automated Hematology Analyzer (Sysmex
Corporation, Kobe, Japan) within 30 min of the blood being
drawn.
Statistical analysis
Normality of data distribution was assessed using
the Shapiro-Wilk test. Two group comparisons were performed using
the t-test or the Mann-Whitney U test when data were
normally or not normally distributed, respectively. The optimal
cut-off points of parameters that provided significant differences
were assessed with the use of receiver operating characteristic
(ROC) curves. These cut-off points were taken into account for the
calculation of specificity, sensitivity, negative predictive value
(NPV), positive predictive value (PPV) and accuracy. For the
assessment of time until metastasis development, patients were
divided into 4 groups according to the levels of each white blood
cell and platelet parameter: Group 1, ≤25th percentile; group 2,
>25th and ≤50th percentile; group 3, >50th and ≤75th
percentile; group 4, >75th percentile. The Kaplan-Meier method
was used for the estimation of time to metastasis development and
comparisons among groups according to each tested parameter.
Multivariate survival analysis was performed with the use of Cox
regression with the forward conditional method. All the tests were
two-tailed and P<0.05 was considered to indicate a statistically
significant difference.
Results
Complete blood count test results
according to the development of secondary distant metastasis
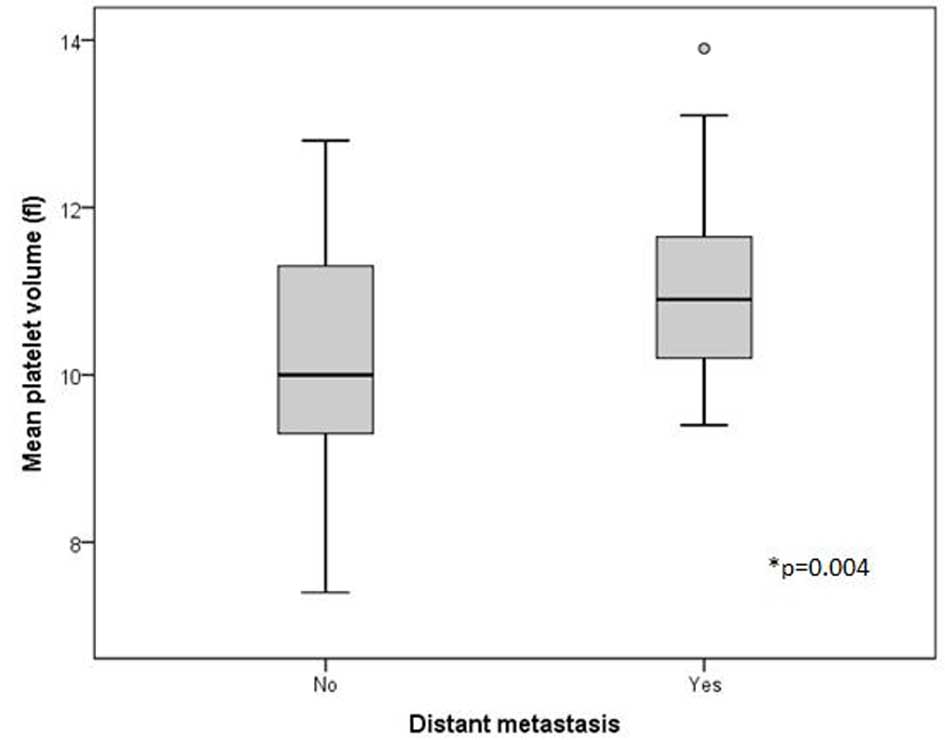
The only parameters that appeared to differentiate
between the patients who developed metastasis and those who did not
were the mean platelet volume and neutrophil count. Specifically,
patients who presented with distant metastasis during the follow-up
period had an increased mean platelet volume [mean ± standard
deviation (SD), 10.9 fl ± 0.9] in comparison with patients who did
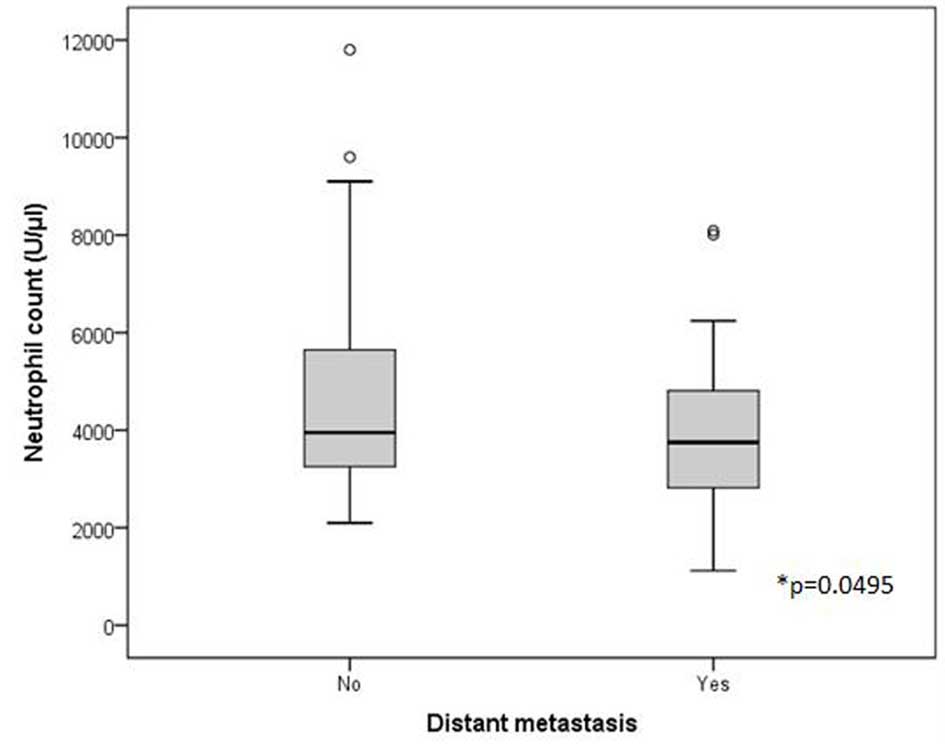
not (mean ± SD, 10.1 fl ± 1.5) (P=0.004) (Fig. 1). Furthermore, patients who presented
with distant metastasis during the surveillance period had
decreased neutrophil counts (median, 3,640 U/µl; range, 1,120–8,090
U/µl) compared with patients who did not present with metastasis
(median, 3,950 U/µl; range, 2,100–11,800 U/µl) (P=0.0495) (Fig. 2). By contrast, no significant
differences were observed between the patients with and without
distant metastasis with regards to white blood cell count
(P=0.114), neutrophil percentage (P=0.071), lymphocyte count
(P=0.571), lymphocyte percentage (P=0.207),
neutrophil-to-lymphocyte ratio (P=0.191), platelet count (P=0.116),
platelet distribution width (P=0.187), plateletcrit (P=0.669),
platelet-to-neutrophil ratio (P=0.211) or platelet-to-lymphocyte
ratio (P=0.664).
ROC curve analysis and calculation of
sensitivity, specificity, PPV, NPV and accuracy
Regarding mean platelet volume, ROC curve analysis
provided an area under the curve (AUC) of 0.674 [95% confidence
interval (CI): 0.553–0.795; standard error (SE): 0.062; P=0.006]
and an optimal cut-off point of 10 fl (>10 fl sensitivity,
80.4%; specificity, 52.8%; PPV, 70.7%; NPV, 65.5%; accuracy, 69%)
(data not shown). Regarding neutrophil count, ROC curve analysis
provided an AUC of 0.622 (95% CI, 0.506–0.738; SE, 0.059; P=0.0495)
and an optimal cut-off point of 4,000 U/µl (<4,000 U/µl
sensitivity, 60.4%; specificity, 51.4%; PPV, 64%; NPV, 47.5%;
accuracy, 56.7%) (data not shown).
Survival analysis
The mean and the median period of surveillance was
65 months (range, 3–121 months). When group 1 (≤25th percentile)
was compared with groups 2, 3 and 4 (>25th percentile) for each
parameter, significant differences were observed in mean platelet
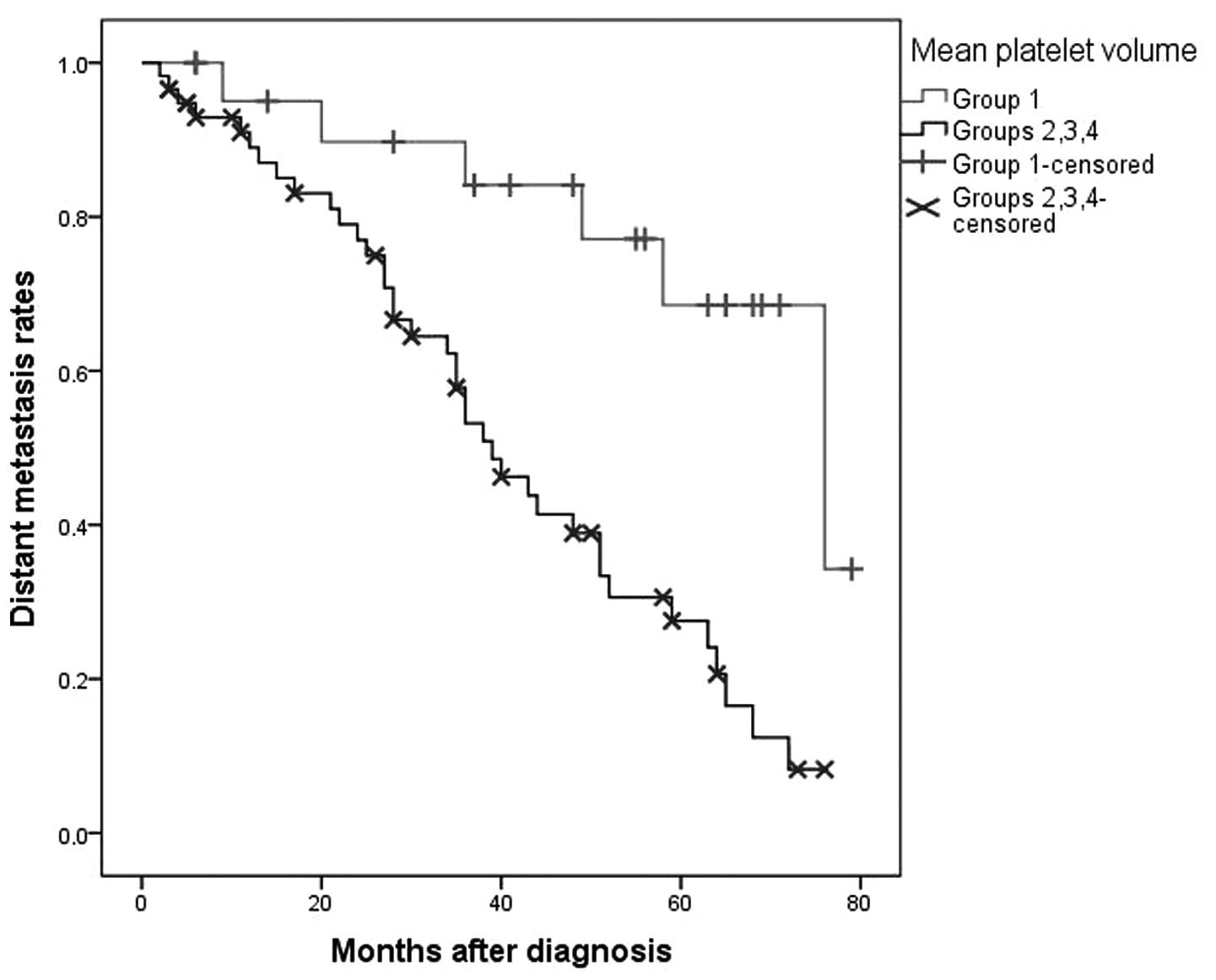
volume and neutrophil count. In particular, patients with a lower
mean platelet volume (group 1) experienced a longer period of time
to distant metastasis development than patients with a higher mean
platelet volume (groups 2, 3 and 4) [P=0.001; group 1: Mean time ±
SE, 65±5 months (95% CI, 55.2–74.9); groups 2, 3 and 4: Mean time ±
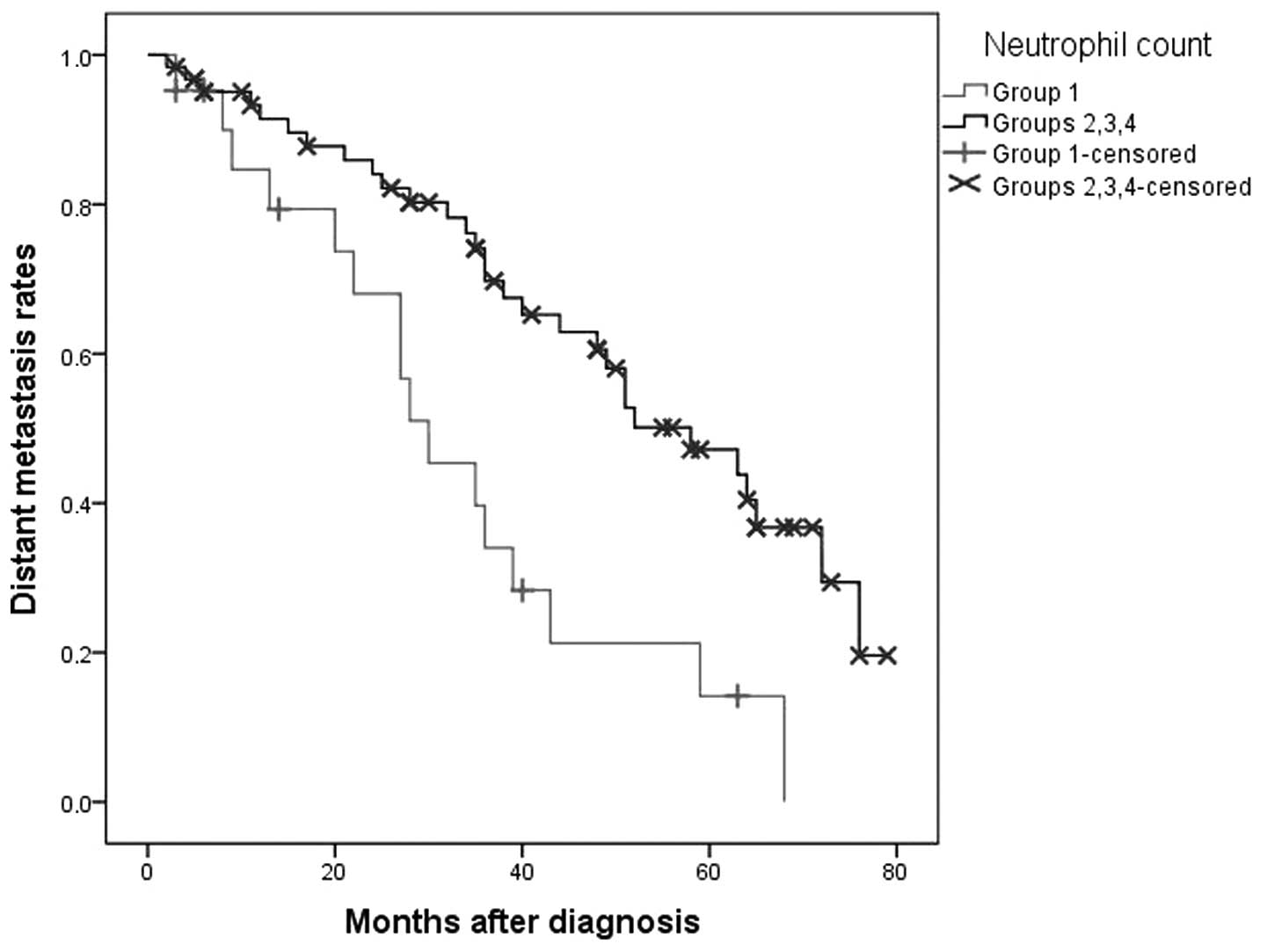
SE, 41.6±3.1 months (95% CI, 35.4–47.7)] (Fig. 3). In addition, patients with a lower
neutrophil count (group 1) experienced a shorter time to distant
metastasis development than patients with a higher neutrophil count
(groups 2, 3 and 4) [P=0.001; group 1: Mean time ± SE, 33.6±4.7
months (95% CI, 24.3–42.9); groups 2, 3 and 4: Mean time ± SE,
52.5±3.4 months (95% CI, 45.9–59.1)] (Fig. 4). By contrast, no significant
differences were detected between the patients with and without
distant metastasis regarding white blood cell count (P=0.105),
neutrophil percentage (P=0.17), lymphocyte count (P=0.587),
lymphocyte percentage (P=0.108), neutrophil-to-lymphocyte ratio
(P=0.34), platelet count (P=0.17), platelet distribution width
(P=0.104), plateletcrit (P=0.683), platelet-to-neutrophil ratio
(P=0.647) or platelet-to-lymphocyte ratio (P=0.433). However, the
multivariate survival analysis provided high T (P=0.0002) and high
grade (P=0.001) as independent risk factors for future development
of distant metastasis, but not mean platelet volume (P=0.096) or
neutrophil count (P=0.993).
Discussion
There is a growing body of evidence to suggest that
immune cells and platelets are implicated in complex crosstalk with
malignant cells and their microenvironment in various malignancies
(2,4–6). Regarding
white blood cells, increased tumor infiltration by inflammatory
cells has been associated with favorable histopathological features
and prognosis in numerous types of cancer (2). Furthermore, it has been observed that
platelets interact with malignant cells and suppress the
inflammatory response against them. In addition, platelets secrete
various growth factors and cytokines that promote angiogenesis,
tumor growth, invasion and metastasis either directly or indirectly
(4–6).
Several clinical studies (7–10) have
aimed to evaluate whether these interactions between white blood
cells and platelets on one side and tumor cells on the other side
may cause measurable alterations in blood parameters, as they are
depicted in the complete blood count test. Furthermore, studies
have attempted to detect any potential diagnostic and/or prognostic
values of blood test parameters (7–10).
Parameters that have been examined regarding breast cancer include
mean platelet volume, platelet-to-lymphocyte ratio and
neutrophil-to-lymphocyte ratio.
Neutrophil-to-lymphocyte ratio is the most studied
parameter in breast cancer. In particular, Ozyalvacli et al
(12) observed that
neutrophil-to-lymphocyte ratio was increased in patients with
breast cancer compared with patients with benign proliferative
breast disease. In addition, Dirican et al (13) and Jia et al (14) reported that patients with breast
cancer with a low neutrophil-to-lymphocyte ratio present longer
disease-free and overall survival times than those who have a high
neutrophil-to-lymphocyte ratio. Similar results have been yielded
by several studies (15–19), which concluded that patients with a
high pretreatment neutrophil-to-lymphocyte ratio have higher 5-year
mortality rates than patients with a low pretreatment
neutrophil-to-lymphocyte ratio. By contrast, Ulas et al
(20) did not detect any significant
associations between clinicopathological parameters or survival
rate and neutrophil-to-lymphocyte ratio in patients with breast
cancer.
Regarding platelet-to-lymphocyte ratio in patients
with breast cancer, several studies have also attempted to identify
any potential prognostic value. Patients with a higher
platelet-to-lymphocyte ratio experienced poorer survival times
(15,16,21) and a
larger number of infiltrated lymph nodes (22) compared with patients with a lower
platelet-to-lymphocyte ratio. By contrast, Ulas et al
(20) and Yao et al (18) reported that platelet-to-lymphocyte
ratio does not significantly affect survival times in patients with
breast cancer.
Gu et al (23)
reported that mean platelet volume is higher in patients with
breast cancer than in patients with benign breast tumors.
Additionally, it was observed that increased mean platelet volume
was associated with larger tumors, higher stage, distant metastases
and a poorer prognosis in patients with breast cancer (23). By contrast, Yao et al (18) reported that there was no significant
difference in survival between higher and lower mean platelet
volumes.
The present study aimed to evaluate the potential
prognostic role of white blood cell and platelet indices in
determining which high-risk patients with newly diagnosed invasive
ductal breast carcinoma are likely develop distant metastasis in
the future. According to the results, patients who are predicted to
develop distant metastasis have a higher mean platelet volume and
lower neutrophil count in comparison with those who are unlikely to
develop metastasis. This is also confirmed by survival analysis,
which demonstrated that patients with a lower mean platelet volume
had a longer time to metastasis development, whereas patients with
a lower neutrophil count had a shorter time to metastasis
development. However, these two parameters yielded only moderate
sensitivity and specificity in identifying the patients with breast
cancer who will develop distant metastasis.
In conclusion, mean platelet volume and neutrophil
count are two blood test parameters that may be useful in
identifying patients with newly diagnosed invasive ductal breast
carcinoma that are likely to present with distant metastasis in the
future. Nevertheless, further studies are required to confirm the
findings of the current study, which may allow the construction of
a predictive model for patients with breast cancer, including mean
platelet volume and neutrophil count, amongst other blood test
parameters.
References
|
1
|
Siegel R, Ma J, Zou Z and Jemal A: Cancer
statistics, 2014. CA Cancer Clin. 64:9–29. 2014. View Article : Google Scholar
|
|
2
|
Giraldo NA, Becht E, Vano Y,
Sautès-Fridman C and Fridman WH: The immune response in cancer:
From immunology to pathology to immunotherapy. Virchows Arch.
467:127–135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wu Y, Fu X, Zhu X, He X, Zou C, Han Y, Xu
M, Huang C, Lu X and Zhao Y: Prognostic role of systemic
inflammatory response in renal cell carcinoma: A systematic review
and meta-analysis. J Cancer Res Clin Oncol. 137:887–896. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Menter DG, Tucker SC, Kopetz S, Sood AK,
Crissman JD and Honn KV: Platelets and cancer: A casual or causal
relationship: Revisited. Cancer Metastasis Rev. 33:231–269. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yan M and Jurasz P: The role of platelets
in the tumor microenvironment: From solid tumors to leukemia.
Biochim Biophys Acta. 1863:392–400. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Franco AT, Corken A and Ware J: Platelets
at the interface of thrombosis, inflammation, and cancer. Blood.
126:582–588. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Templeton AJ, McNamara MG, Šeruga B,
Vera-Badillo FE, Aneja P, Ocaña A, Leibowitz-Amit R, Sonpavde G,
Knox JJ, Tran B, et al: Prognostic role of neutrophil-to-lymphocyte
ratio in solid tumors: A systematic review and meta-analysis. J
Natl Cancer Inst. 106:dju1242014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Paramanathan A, Saxena A and Morris DL: A
systematic review and meta-analysis on the impact of pre-operative
neutrophil lymphocyte ratio on long term outcomes after curative
intent resection of solid tumours. Surg Oncol. 23:31–39. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Xin-Ji Z, Yong-Gang L, Xiao-Jun S, Xiao-Wu
C, Dong Z and Da-Jian Z: The prognostic role of neutrophils to
lymphocytes ratio and platelet count in gastric cancer: A
meta-analysis. Int J Surg. 21:84–91. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Templeton AJ, Ace O, McNamara MG,
Al-Mubarak M, Vera-Badillo FE, Hermanns T, Seruga B, Ocaña A,
Tannock IF and Amir E: Prognostic role of platelet to lymphocyte
ratio in solid tumors: A systematic review and meta-analysis.
Cancer Epidemiol Biomarkers Prev. 23:1204–1212. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sobin LH, Gospodarowicz MK and Wittekind
CH: Breast tumours. TNM Classification of Malignant Tumours (7th).
Wiley-Blackwell. (Chichester, West Sussex, UK). 181–193. 2010.
|
|
12
|
Ozyalvacli G, Yesil C, Kargi E, Kizildag
B, Kilitci A and Yilmaz F: Diagnostic and prognostic importance of
the neutrophil lymphocyte ratio in breast cancer. Asian Pac J
Cancer Prev. 15:10363–10366. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dirican A, Kucukzeybek BB, Alacacioglu A,
Kucukzeybek Y, Erten C, Varol U, Somali I, Demir L, Bayoglu IV,
Yildiz Y, et al: Do the derived neutrophil to lymphocyte ratio and
the neutrophil to lymphocyte ratio predict prognosis in breast
cancer? Int J Clin Oncol. 20:70–81. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jia W, Wu J, Jia H, Yang Y, Zhang X, Chen
K and Su F: The peripheral blood neutrophil-to-lymphocyte ratio is
superior to the lymphocyte-to-monocyte ratio for predicting the
long-term survival of triple-negative breast cancer patients. PLoS
One. 10:e01430612015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Azab B, Shah N, Radbel J, Tan P, Bhatt V,
Vonfrolio S, Habeshy A, Picon A and Bloom S: Pretreatment
neutrophil/lymphocyte ratio is superior to platelet/lymphocyte
ratio as a predictor of long-term mortality in breast cancer
patients. Med Oncol. 30:4322013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Koh CH, Bhoo-Pathy N, Ng KL, Jabir RS, Tan
GH, See MH, Jamaris S and Taib NA: Utility of pre-treatment
neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as
prognostic factors in breast cancer. Br J Cancer. 113:150–158.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Noh H, Eomm M and Han A: Usefulness of
pretreatment neutrophil to lymphocyte ratio in predicting
disease-specific survival in breast cancer patients. J Breast
Cancer. 16:55–59. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yao M, Liu Y, Jin H, Liu X, Lv K, Wei H,
Du C, Wang S, Wei B and Fu P: Prognostic value of preoperative
inflammatory markers in Chinese patients with breast cancer. Onco
Targets Ther. 7:1743–1752. 2014.PubMed/NCBI
|
|
19
|
Koh YW, Lee HJ, Ahn JH, Lee JW and Gong G:
Prognostic significance of the ratio of absolute neutrophil to
lymphocyte counts for breast cancer patients with ER/PR-positivity
and HER2-negativity in neoadjuvant setting. Tumour Biol.
35:9823–9830. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ulas A, Avci N, Kos T, Cubukcu E, Olmez
OF, Bulut N and Degirmenci M: Are neutrophil/lymphocyte ratio and
platelet/lymphocyte ratio associated with prognosis in patients
with HER2-positive early breast cancer receiving adjuvant
trastuzumab? J BUON. 20:714–722. 2015.PubMed/NCBI
|
|
21
|
Krenn-Pilko S, Langsenlehner U, Thurner
EM, Stojakovic T, Pichler M, Gerger A, Kapp KS and Langsenlehner T:
The elevated preoperative platelet-to-lymphocyte ratio predicts
poor prognosis in breast cancer patients. Br J Cancer.
110:2524–2530. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Seretis C, Seretis F, Lagoudianakis E,
Politou M, Gemenetzis G and Salemis NS: Enhancing the accuracy of
platelet to lymphocyte ratio after adjustment for large platelet
count: A pilot study in breast cancer patients. Int J Surg Oncol.
2012:6536082012.PubMed/NCBI
|
|
23
|
Gu M, Zhai Z, Huang L, Zheng W, Zhou Y,
Zhu R, Shen F and Yuan C: Pre-treatment mean platelet volume
associates with worse clinicopathologic features and prognosis of
patients with invasive breast cancer. Breast Cancer. Aug
26–2015.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|