Introduction
Bladder cancer (BCa) is the most common malignancy
of the urinary tract in the elderly population, and the sixth most
common cancer in men worldwide (1).
More than 75% of all newly diagnosed BCa cases are
non-muscle-invasive lesions and ~70% of patients present with pTa,
20% with pT1 and 10% with carcinoma in situ (pTIS) lesions
(2,3).
Although these BCa tumors can be resected completely by
transurethral resection of the bladder (TURB), patients harbor a
significant risk of tumor recurrence and progression (3). Consequently, lifelong and frequent
follow-up and tumor surveillance are necessary, making BCa one of
the most expensive diseases worldwide (4). Considering the current European
Association of Urology guidelines on non-muscle-invasive bladder
carcinoma (NMIBC), cystoscopy in combination with voided urine
cytology (VUC) and histological evaluation of multiple bladder
biopsies is the only reliable method for the diagnosis of BCa to
date (2). In contrast to cystoscopy,
VUC is relatively inexpensive. It demonstrates high sensitivity for
high-grade/G3 tumors, however, due to its low sensitivity for
well-differentiated, low-grade/G1 tumors, VUC may only be used as
an adjunct to cystoscopy rather than replacing it (5). An additional drawback of VUC is its
strong observer-dependence and the requirement for trained,
experienced cytopathologists or urologists (6). However, to date it is the most commonly
utilized non-invasive method for the detection of BCa in the
current clinical routine. Previously, great effort was put into the
investigation of putative urinary biomarkers suitable for the
non-invasive diagnosis of BCa (7–10). The
challenge is to develop an inexpensive test, which shows high
sensitivity and specificity and which is objective and easy to
perform. Despite typically demonstrating higher sensitivities
compared to VUC, the majority of the current tests available lack
high specificities (11).
Consequently, although some of the investigated biomarkers are
commercially available, a routine application of these tests is not
recommended for the primary detection of BCa or for surveillance of
NMIBC (2).
Midkine (also known as neurite growth-promoting
factor 2) is a heparin-binding growth factor of 13 kDa (12). As secretory protein, midkine is
readily available in biofluids including blood and urine (13). Although midkine gene expression has
been detected in several tissues of healthy individuals, including
the gastrointestinal tract, kidney, spleen, lungs and thyroid,
corresponding midkine protein expression could not be observed
(13). By contrast, in a genome-wide
search for abundantly expressed genes in cancerous vs. normal
tissue, midkine was identified as the second highest expressed gene
in the most common types of human cancer (14). Consistently, midkine protein was
demonstrated to be highly expressed in various malignancies,
including neuroblastoma, breast cancer, hepatocellular carcinoma,
colorectal cancer and BCa (15,16).
Although the expression of midkine protein in BCa and its
correlation with a poor outcome in patients with invasive cancers
has been previously reported (16),
to the best of our knowledge there are only three studies reporting
the measurement of midkine protein in urine specimens from BCa
patients (15,17,18). Only
one study investigated whether there is a correlation between
midkine protein concentration in urine and disease progression in
terms of tumor stage and grade (17).
Furthermore, the lack of comparison with VUC as a reference method
for the non-invasive detection of BCa is a major drawback of these
studies.
In the present study midkine was analyzed in an
independent patient cohort and its diagnostic performance was
compared with that of VUC. The present study aimed to evaluate the
suitability of midkine as a non-invasive biomarker for BCa.
Materials and methods
Study population, data and sample
collection
BCa patients and control subjects were consecutively
recruited by the Department of Urology, Technische Universität
Dresden (Dresden, Germany) between May 2014 and May 2015. Urine
specimens from BCa patients and control subjects were prospectively
collected. The study was approved by the institutional review board
of the Technische Universität Dresden. Written informed consent was
obtained from all participants. Criteria for the inclusion of
patients into the study were as follows: Age 45–80 years with
suspicion of new-onset or recurrent BCa on the basis of initial
findings during cystoscopy or during imaging examinations, who were
planned to undergo primary TURB (Fig.
1). Individuals with suspected or confirmed renal cell
carcinoma (RCC), cystic disease or nephrolithiasis served as
controls. Those who were diagnosed with chronic cystitis (CC) as
cause of their symptoms during TURB represented a distinct control
group. Patients with other non-urological cancers, who had received
earlier pelvic radiotherapy, as well as those who were diagnosed
with papilloma or papillary urothelial neoplasm of low malignant
potential or who underwent a second or third TURB were excluded
from the study. Finally, a total of 162 individuals comprising 92
BCa patients and 70 controls were selected for analysis. The final
allocation to the patient and control groups was performed
following histopathological examination of the resected bladder
specimens that served as the reference standard in the present
study. Only patients with histopathologically confirmed BCa were
designated as BCa patients. Tumor staging was assessed according to
Union for International Cancer Control Tumor-Node-Metastasis
classification (19), and tumor
grading was assessed according to World Health Organization (WHO)
classification (20,21). Tumor stage was evaluated as pTa, pTIS,
pT1 and ≥pT2a and tumor grade as low-grade and high-grade, as well
as G1, G2 and G3. VUC was prepared for every urine specimen. The
evaluation of all VUC specimens was performed by a single,
experienced examiner, in accordance with the WHO classification
(20). In cases of low cellularity,
urinary cytology could not be evaluated, and therefore these
samples were excluded from the analysis aimed at comparing VUC with
urinary midkine. The data are reported according to the Standards
for the Reporting of Diagnostic accuracy studies statements
(22).
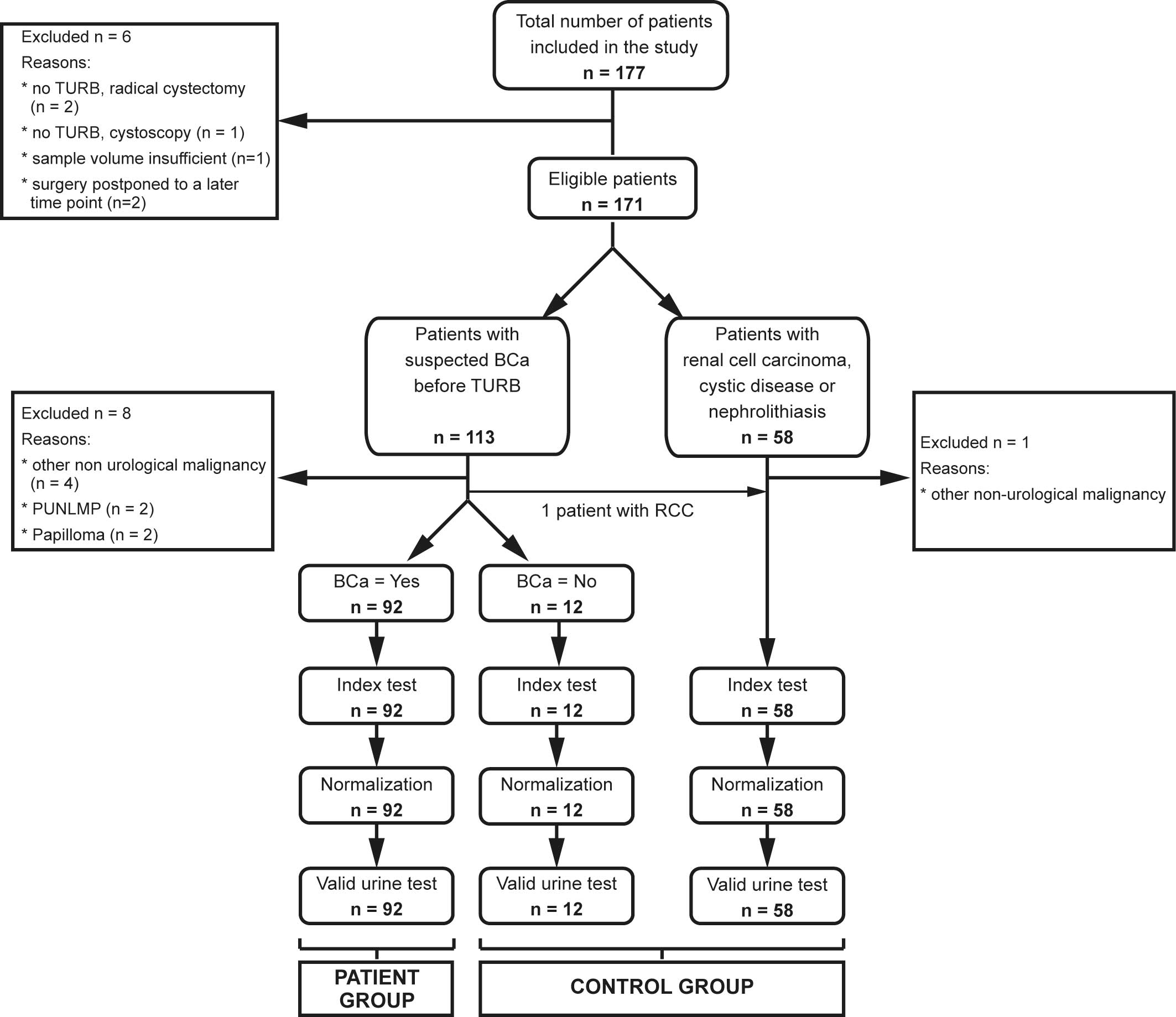 | Figure 1.Flow chart showing patient
recruitment and number of eligible patients. A total of 177
patients were initially recruited for the study. Due to the
indicated reasons, 6 patients were subsequently excluded. Of the
remaining 171 patients, 113 were suspected to have BCa and 58
patients constituted the control group. Following histopathological
examination of the resected bladder tissue, an additional 9
patients were excluded. One patient initially suspected to have BCa
was diagnosed with RCC and therefore switched to the control group.
Therefore, urinary midkine was analyzed for 92 BCa patients and 70
controls. A total of 12 patients initially suspected to have BCa,
which could not be confirmed following TURB, formed the distinct
control group of chronic cystitis. PUNLMP, papillary urothelial
neoplasm of low malignant potential; RCC, renal cell carcinoma;
BCa, bladder cancer; TURB, transurethral resection of the
bladder. |
Processing of urine samples
A total of 50 ml of random non-first-morning urine
samples were obtained from every patient and control subject
preoperatively. Urine dipstick analysis was performed immediately
following the collection and evaluated using the automated Urisys
1800 urine analyzer (Roche Diagnostics Deutschland GmbH, Mannheim,
Germany). A total of 10 ml of urine was centrifuged at 380 × g for
3 min at 20°C, and urine sediment was analyzed microscopically,
using an Axio Lab.A1 microscope (Zeiss AG, Oberkochen, Germany) at
magnification ×400, for the presence of erythrocytes, leucocytes
and bacteria. The remaining urine specimen was centrifuged at 1,500
× g for 10 min at 4°C. The supernatant was decanted and frozen in 1
ml aliquots using tubes with protein low-binding capacity (Protein
LoBind Tubes; Eppendorf, Hamburg, Germany) at −80°C until the
analysis of midkine. One aliquot of every urine sample was sent to
the Institute of Clinical Chemistry and Laboratory Medicine
(Technische Universität Dresden) for the quantification of urinary
creatinine, which was used to normalize midkine concentrations. The
remaining cell pellet was prefixed with Esposti's fixative
overnight, centrifuged on glass slides at 1,000 × g for 4 min at
20°C, fixed with Cytofix N (Niepötter Labortechnik, Bürstadt,
Germany) and stained by the Papanicolaou procedure (23).
Measurement of midkine by
enzyme-linked immunosorbent assay (ELISA)
Human midkine was determined in urine supernatants
using the commercially available Human Midkine DuoSet ELISA (DY258;
R&D Systems, Inc., Minneapolis, MN, USA) according to the
manufacturer's instructions, except for the concentrations of
capture and detection antibodies, which were 3.2 µg/ml and 800
ng/ml, respectively. The optical density (OD) was measured
immediately following assay development using the Mithras LB 940
Multimode Microplate Reader (Berthold Technologies GMBH & Co.
KG, Bad Wildbad, Germany) set to 450 nm. The OD at 570 nm
(reference wavelength) was subtracted from the readings at 450 nm.
Samples were randomized across multiple ELISA plates and measured
consecutively. A standard curve was constructed by generating a
four parameter logistic curve-fit using GraphPad Prism version 6.05
for Windows (GraphPad Software Inc., La Jolla, CA, USA). The
measured midkine concentrations in urine were normalized to the
corresponding creatinine values and expressed as µg midkine/g
creatinine.
Statistical analysis
The two-tailed Mann Whitney U nonparametric test was
performed to evaluate differences in urinary midkine concentrations
between BCa patients and controls, and with respect to tumor stage
and grade. Determination of Spearman's rank correlation coefficient
(rs) revealed potential correlations between midkine
concentrations and tumor stage and grade. Statistical analyses were
performed using GraphPad Prism version 6.05 for Windows. Data are
plotted as box plots, where the bottom and top of the boxes
represent the first and third quartiles, respectively. The median
is shown as a solid line within the box, and the ends of the
whiskers represent the 10–90 percentile. Data not included between
the whiskers are defined as outliers and are marked as single
circle symbols. The diagnostic performance of urinary midkine was
determined using receiver operating characteristic (ROC) curve
analyses and the corresponding area under the curve (AUC) values.
ROC analyses were performed using IBM SPSS Statistics for Windows
version 23.0 (IBM SPSS, Armonk, NY, USA). Youden's Index helped to
calculate the best cut-off values for midkine with the best
combination of sensitivity and specificity (24). For all analyses, P<0.05 was
considered to indicate a statistically significant difference.
Positive predictive value (PPV), negative predictive value (NPV),
positive likelihood ratio (pLR), negative likelihood ratio (nLR)
and accuracy were calculated according to standard statistical
methods (25).
Results
Characteristics of BCa patients and
control subjects
A total of 177 patients and control subjects were
recruited for participation in the present study. A total of 162
individuals were eligible for analysis (Fig. 1). Among them there were 92 patients
diagnosed with BCa and 70 controls. The majority of control
subjects suffered from RCC (48.6%), followed by nephrolithiasis
(22.9%), CC (17.1%) and other benign urological diseases (11.4%).
Almost 80% of the BCa patients were male, compared to 74% of the
control subjects. The median age was 71 years (range, 50–80 years)
and 64.5 years (range, 43–80 years) in the patient group vs. the
control group, respectively. There were seven times more cases of
new-onset bladder tumors than recurrent tumors. The relative
distributions of pTa, pT1 and ≥pT2a tumors were 50.0, 22.8 and
15.2%, respectively. A single patient exhibited a tumor categorized
as pTIS only, whereas 10 patients showed concomitant pTIS.
According to the severity of the diagnosed tumor stage, patients
with pTa and pT1 tumors and concomitant pTIS were assigned pTIS,
whereas BCa patients with muscle invasive tumors, who exhibited
concomitant pTIS, were allocated to the group ≥pT2a. A total of
9/92 BCa patients (9.8%) simultaneously exhibited prostate cancer
(PCa). Furthermore, the patient cohort comprised 4.4 times more
patients with high-grade tumors than low-grade tumors. In
accordance to the WHO classification, these tumors were classified
as 17.5% G1, 44.0% G2 and 38.5% G3 (21). A summary of all demographic, clinical
and histopathological data is depicted in Tables I and II.
 | Table I.Demographic, clinical and
histopathological characteristics of patients with bladder
carcinoma.a |
Table I.
Demographic, clinical and
histopathological characteristics of patients with bladder
carcinoma.a
| Category | n | % |
|---|
| Total patients | 92 | 100.0 |
| Gender |
|
|
|
Male | 73 | 79.3 |
|
Female | 19 | 20.7 |
| Ageb, years |
|
|
|
<71 | 44 | 47.8 |
|
≥71 | 48 | 52.2 |
| Tumor |
|
|
|
Primary | 80 | 87.0 |
|
Recurrent | 12 | 13.0 |
| Voided urine
cytology |
|
|
|
Positive | 78 | 84.8 |
|
Negative | 11 | 12.0 |
| Not
evaluable | 3 |
3.2 |
| Tumor stage |
|
|
|
pTa | 46 | 50.0 |
|
pT1 | 21 | 22.8 |
|
pTIS | 11 | 12.0 |
|
pTIS only | 1 |
1.2 |
|
+pTa | 2 |
2.2 |
|
+pT1 | 4 |
4.3 |
|
+≥pT2a | 4 |
4.3 |
|
≥pT2a | 14 | 15.2 |
| Concomitant
PCa |
|
|
|
Yes | 9 |
9.8 |
| No | 83 | 90.2 |
| Tumor grade (WHO
2004) |
|
|
|
Low | 17 | 18.5 |
|
High | 75 | 81.5 |
| Tumor
gradec (WHO 1973) |
|
|
| G1 | 16 | 17.5 |
| G2 | 40 | 44.0 |
| G3 | 35 | 38.5 |
| Table II.Demographic, clinical and
histopathological characteristics of control subjects.a |
Table II.
Demographic, clinical and
histopathological characteristics of control subjects.a
| Category | n | % |
|---|
| Total patients | 70 | 100.0 |
| Gender |
|
|
|
Male | 52 | 74.3 |
|
Female | 18 | 25.7 |
| Age,
yearsb |
|
|
|
<64.5 | 35 | 50.0 |
|
≥64.5 | 35 | 50.0 |
| Voided urine
cytology |
|
|
|
Positive | 8 | 11.4 |
|
Negative | 57 | 81.4 |
| Not
evaluable | 5 |
7.2 |
| Diagnosis |
|
|
| Renal
cell carcinoma | 34 | 48.6 |
|
Nephrolithiasis | 16 | 22.9 |
| Chronic
cystitis | 12 | 17.1 |
| Benign
urological disease | 8 | 11.4 |
Utility of urinary midkine as a
biomarker for the detection of BCa
BCa patients often simultaneously suffer from PCa.
To exclude any influence of PCa on urinary midkine concentration,
patients with and without concomitant PCa were compared regarding
their urinary midkine levels. No statistically significant
difference was observed in the urinary midkine levels of BCa
patients and those who additionally were diagnosed with PCa
(P=0.777; Mann Whitney U test; data not shown). For this reason,
patients diagnosed with BCa and PCa were not excluded from the
patient group. In addition, subdividing the group of control
subjects into patients with RCC, nephrolithiasis and benign
urological disease also revealed no statistically significant
differences in midkine concentrations (data not shown). Patients
diagnosed with CC as the cause of their symptoms were initially
examined separately from the remaining control subjects.
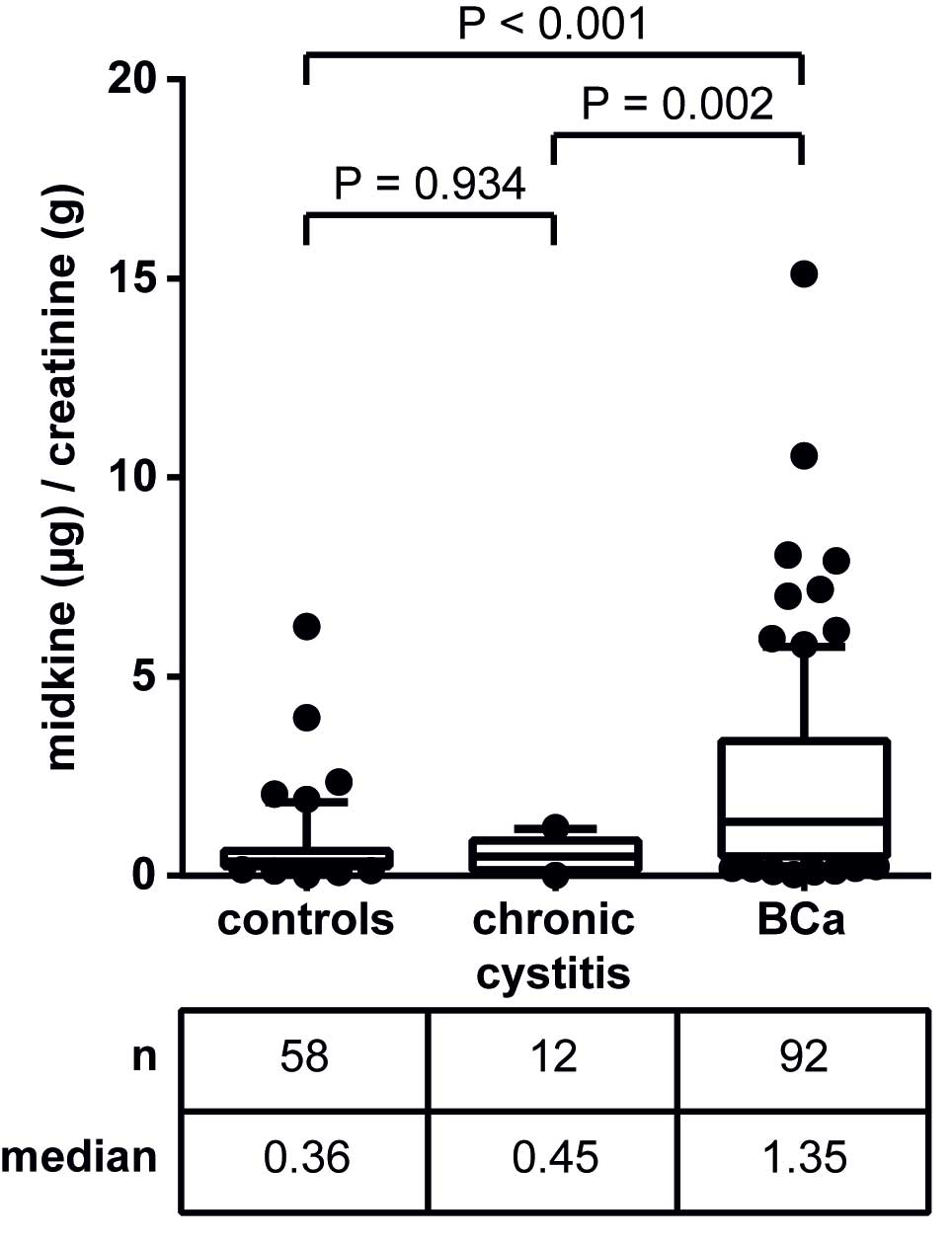
The levels of urinary midkine in the respective
groups are shown in Fig. 2. The
median midkine concentrations in urine specimens from patients with
CC and BCa were 0.45 and 1.35 µg midkine/g creatinine,
respectively. Thus, urinary midkine levels were significantly
elevated in patients with BCa compared to CC patients (3-fold
increase; P=0.002). This was also true for the comparison of
patients with RCC, nephrolithiasis and other benign urological
diseases with BCa patients (3.8-fold increase; P<0.001). In
addition, both control subgroups (group 1, patients with RCC,
nephrolithiasis and other benign urological disease; group 2,
patients with chronic cystitis) were not significantly different
when compared with each other (P=0.934). Consequently, patients
with CC, RCC, nephrolithiasis and other benign urological diseases
were considered together as a single control group for further
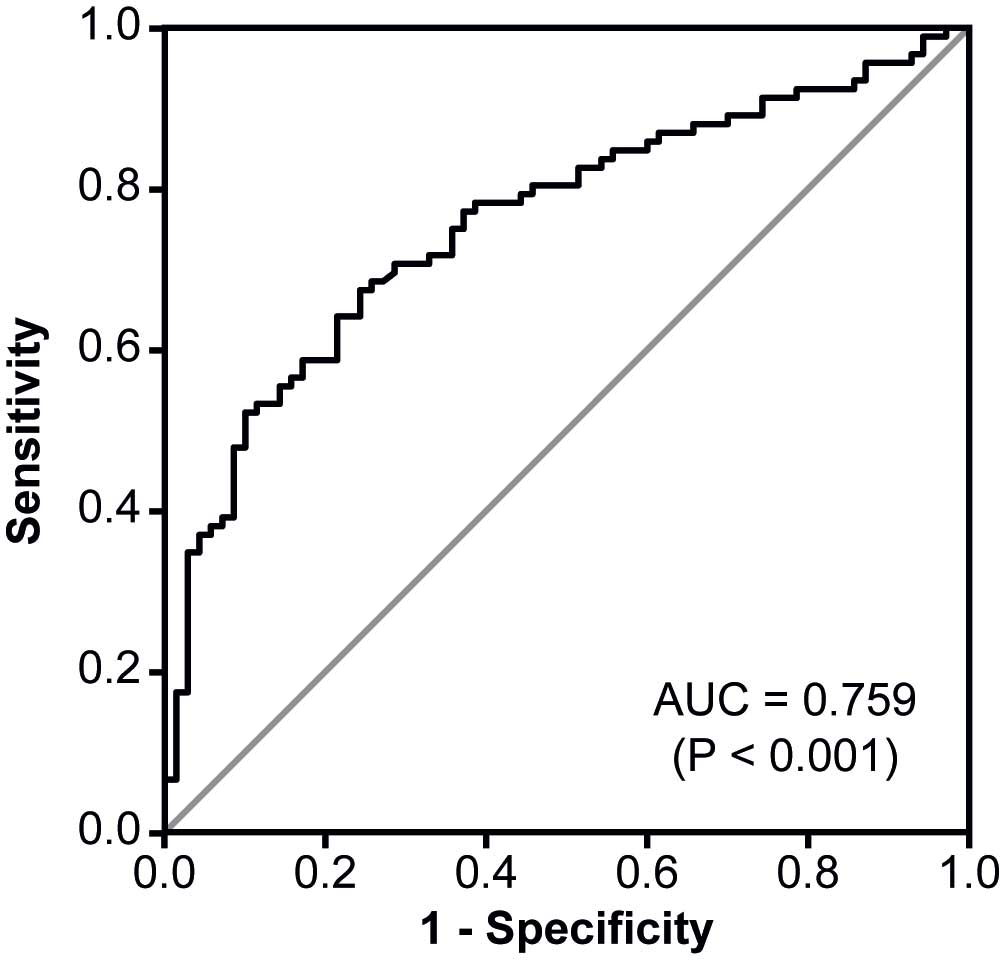
analyses. ROC analysis for urinary midkine as a diagnostic BCa
marker revealed an AUC of 0.759 (Fig.
3).
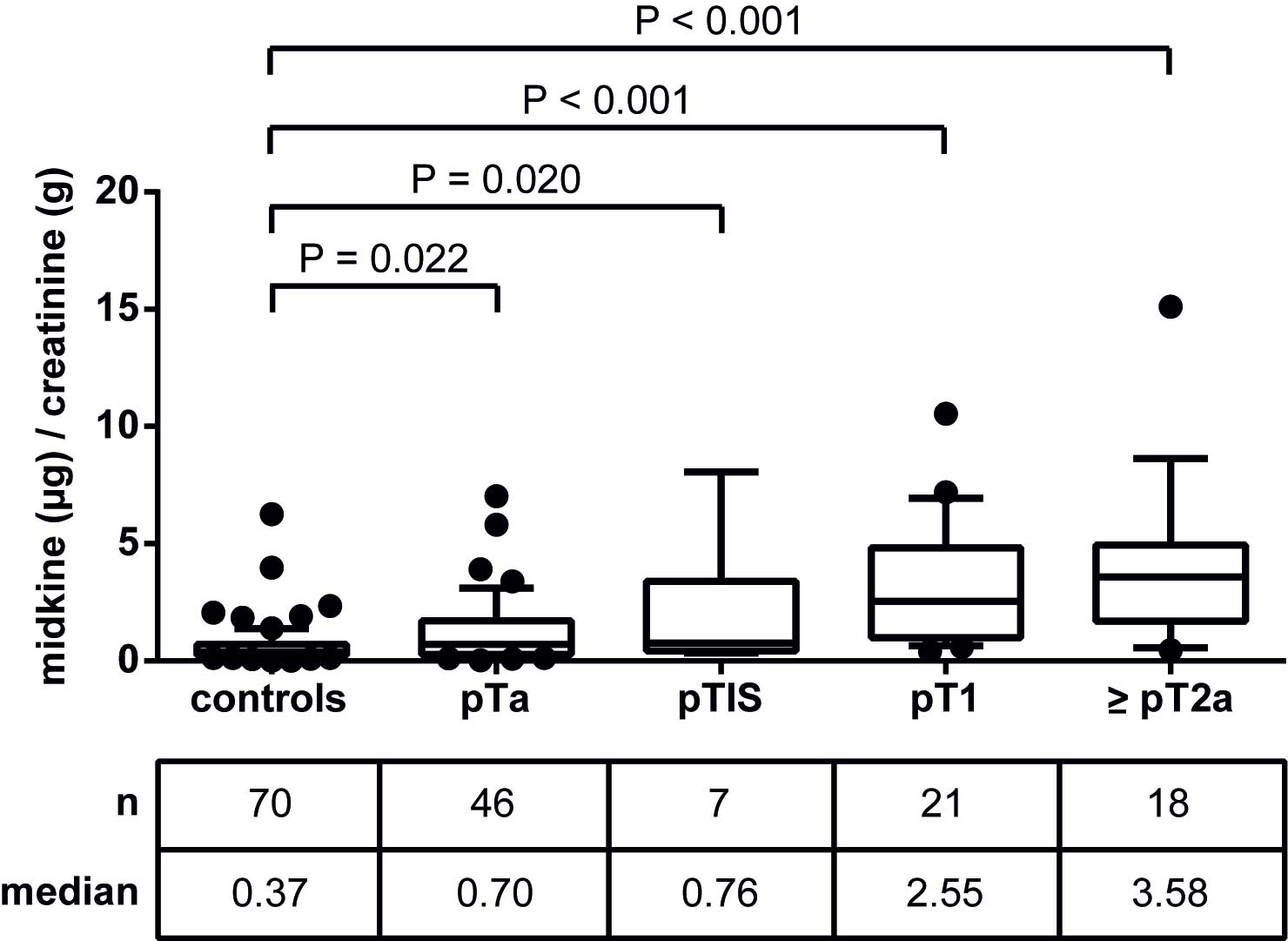
To assess potential associations of midkine with
tumor stage and grade, the patient group was subdivided into pTa,
pTIS, pT1 and ≥pT2a, as well as low-grade vs. high-grade, and
midkine levels were evaluated relative to controls (Fig. 4). Urinary midkine levels were
significantly elevated in all four patient groups relative to
controls, however, the more progressed the tumor, the higher the
median midkine concentration. Therefore, patients with pT1 and
muscle-invasive ≥pT2a tumors were more distinguishable from
controls compared with patients with pTa and pTIS tumors.
Spearman's rank correlation coefficient was 0.536 (P<0.001),
reflecting a moderate positive, but highly significant correlation
between midkine levels and tumor stage.
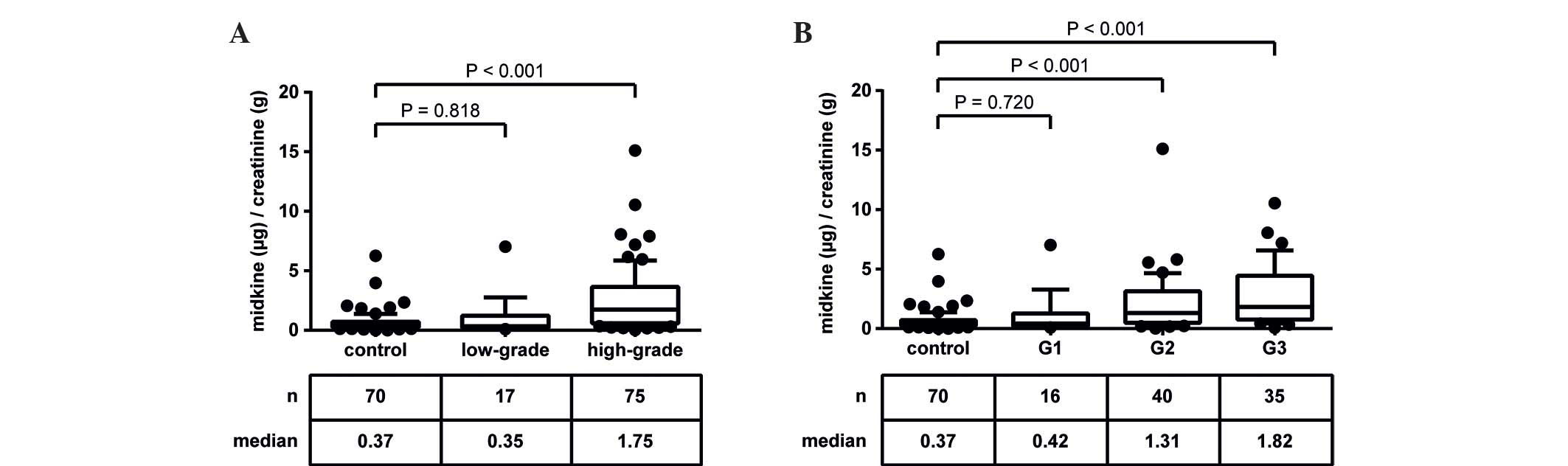
A similar observation was made with regard to tumor
grade (Fig. 5). Midkine
concentrations in patients with low-grade tumors were not
significantly different from controls (P=0.818), whereas high-grade
tumors demonstrated significantly elevated urinary midkine levels
(P<0.001; Fig. 5A). Using the WHO
classification, in the present patient cohort almost all patients
with low-grade tumors corresponded to G1 tumors, whereas the
high-grade group included patients with G2 and G3 tumors (21). Patients with G2 and G3 tumors showed
significantly increased urinary midkine concentrations compared to
controls (P<0.001), whereas patients with G1 tumors did not
(P=0.720; Fig. 5B). The calculation
of Spearman's rank correlation coefficient revealed a moderate
positive, highly significant correlation (rs=0.453;
P<0.001).
Comparison of diagnostic performance
of urinary midkine and VUC
As VUC is the reference standard for non-invasive
detection of BCa, the present study aimed to compare the diagnostic
power of VUC with that of urinary midkine. For this comparison,
only urine specimens that exhibited a valid urine test for midkine
and an evaluable VUC were included. This was true for 154/162 urine
specimens. ROC curve analyses helped to assess the diagnostic
performance of urinary midkine for the discrimination of BCa
patients and controls, and to calculate the best cut-off value.
Using a cut-off concentration of 0.71 µg midkine/g creatinine the
AUC was 0.784 and the sensitivity and specificity of urinary
midkine were 69.7 and 76.9%, respectively. VUC clearly outperformed
urinary midkine determination with 87.6% sensitivity and 87.7%
specificity (Table III). In
addition, VUC more convincingly detected the disease than urinary
midkine with positive and negative likelihood ratios of 7.1 and 0.1
(VUC) and 3.0 and 0.4 (urinary midkine), respectively. In the next
step, the capability of VUC and urinary midkine to discriminate
patients with various tumor stages and grades from controls was
assessed. AUC values were determined for pTa, pTIS, pT1 and ≥pT2a
to be 0.659, 0.774, 0.926 and 0.935, respectively. The lowest
diagnostic performance for the selected cut-off values was observed
for pTa tumors with a sensitivity of 65.9%, followed by pTIS tumors
(100.0%), pT1 tumors (95.0%) and ≥pT2a tumors (88.9%). The
corresponding specificities were 64.6% (pTa), 46.2% (pTIS), 80.0%
(pT1) and 93.8% (≥pT2a). The best discriminatory power of the test
could be reached for patients diagnosed with pT1 and ≥pT2a tumors,
whereas the identification of less progressed pTa tumors was
diminished. In contrast, VUC achieved similar sensitivities (pTa,
79.6%; pTIS, 100.0%; pT1, 95.0%; ≥pT2a, 94.4%) but higher
specificities (87.7% each) compared to midkine. Regarding tumor
grade, low-grade tumors could not be discriminated from controls by
VUC (sensitivity, 60.0%; specificity, 87.7%) or urinary midkine
(AUC, 0.578; sensitivity: 46.7%; specificity, 76.9%). By contrast,
high-grade tumors were highly distinguishable by VUC (sensitivity,
93.2%; specificity, 87.7%) and urinary midkine (AUC, 0.826;
sensitivity, 59.5%; specificity, 92.3%; Table III).
| Table III.Comparison of the ability of VUC and
urinary MDK for differentiation between control and BCa patients,
and patients with various tumor stages and grades.a |
Table III.
Comparison of the ability of VUC and
urinary MDK for differentiation between control and BCa patients,
and patients with various tumor stages and grades.a
|
|
Control
group (n=65)b vs. |
|---|
|
|
|
|---|
| Diagnostic
performance | BCa | pTa | pTIS | pT1 | ≥pT2a | Low-grade | High-grade | G1 | G2 | G3 |
|---|
| Total
numberb | 89 | 44 | 7 | 20 | 18 | 15 | 74 | 14 | 39 | 35 |
| AUC |
|
MDK | 0.784 | 0.659 | 0.774 | 0.926 | 0.935 | 0.578 | 0.826 | 0.593 | 0.772 | 0.886 |
| 95% confidence
interval |
|
MDK | 0.712–0.856 | 0.551–0.767 | 0.617–0.930 | 0.871–0.980 | 0.876–0.994 | 0.401–0.756 | 0.756–0.895 | 0.408–0.779 | 0.672–0.871 | 0.822–0.950 |
|
P-valuec |
|
MDK |
<0.001d | 0.005d | 0.018d |
<0.001d |
<0.001d | 0.346 |
<0.001d | 0.275 |
<0.001d |
<0.001d |
| Cut-off value, µg/g
creatinine |
|
MDK | 0.71 | 0.49 | 0.34 | 0.83 | 1.5 | 0.71 | 1.31 | 0.71 | 0.64 | 1.31 |
| Sensitivity, % |
|
MDK | 69.7 | 65.9 | 100.0 | 95.0 | 88.9 | 46.7 | 59.5 | 50.0 | 71.8 | 68.6 |
|
VUC | 87.6 | 79.6 | 100.0 | 95.0 | 94.4 | 60.0 | 93.2 | 57.1 | 92.3 | 94.3 |
| Specificity, % |
|
MDK | 76.9 | 64.6 | 46.2 | 80.0 | 93.8 | 76.9 | 92.3 | 76.9 | 75.4 | 92.3 |
|
VUC | 87.7 | 87.7 | 87.7 | 87.7 | 87.7 | 87.7 | 87.7 | 87.7 | 87.7 | 87.7 |
| PPV, % |
|
MDK | 80.5 | 55.8 | 16.7 | 59.4 | 80.0 | 31.8 | 89.8 | 31.8 | 63.6 | 82.8 |
|
VUC | 90.7 | 81.4 | 46.7 | 70.4 | 68.0 | 52.9 | 89.6 | 50.0 | 81.8 | 80.5 |
| NPV, % |
|
MDK | 64.9 | 73.7 | 100.0 | 98.1 | 96.8 | 86.2 | 66.7 | 87.7 | 82.3 | 84.5 |
|
VUC | 83.8 | 86.4 | 100.0 | 98.3 | 98.3 | 90.5 | 91.9 | 90.5 | 95.0 | 96.6 |
| pLR |
|
MDK | 3.0 | 1.9 | 1.9 | 4.8 | 14.4 | 2.0 | 7.7 | 2.2 | 2.9 | 8.9 |
|
VUC | 7.1 | 6.5 | 8.1 | 7.7 | 7.7 | 4.9 | 7.6 | 4.6 | 7.5 | 7.7 |
| nLR |
|
MDK | 0.4 | 0.5 | 0.0 | 0.1 | 0.1 | 0.7 | 0.4 | 0.7 | 0.4 | 0.3 |
|
VUC | 0.1 | 0.2 | 0.0 | 0.1 | 0.1 | 0.5 | 0.1 | 0.5 | 0.1 | 0.1 |
| Accuracy, % |
|
MDK | 72.7 | 65.1 | 51.4 | 83.5 | 92.8 | 71.3 | 74.8 | 72.2 | 74.0 | 84.0 |
|
VUC | 87.7 | 84.4 | 88.9 | 89.4 | 89.4 | 82.5 | 90.6 | 82.3 | 89.4 | 90.0 |
Combinatory ability of urinary midkine
and VUC to detect BCa
To investigate whether the combination of urinary
midkine and VUC had a synergistic effect on the detection of BCa,
diagnostic sensitivity and specificity, PPV and NPV, pLR and nLR,
as well as accuracy of urinary midkine and VUC were calculated when
tested independently or in combination (Table IV). Patients with a positive VUC in
combination with urinary midkine above the cut-off value of 0.71
µg/g creatinine (variant 1) or patients with a positive VUC and/or
urinary midkine above the cut-off value (variant 2) were considered
BCa positive.
| Table IV.Combinatory utility of MDK and VUC
for the diagnosis of bladder cancer.a |
Table IV.
Combinatory utility of MDK and VUC
for the diagnosis of bladder cancer.a
| Diagnostic
performance | VUC
onlyb | MDK
onlyc | VUC and
MDKd | VUC and/or
MDKe |
|---|
| Sensitivity, % | 87.6 | 69.7 | 64.0 | 93.3 |
| Specificity, % | 87.7 | 77.9 | 98.5 | 66.2 |
| PPV, % | 90.7 | 80.5 | 98.3 | 79.0 |
| NPV, % | 83.8 | 64.9 | 66.7 | 87.8 |
| pLR |
7.1 |
3.0 | 41.6 |
2.8 |
| nLR |
0.1 |
0.4 |
0.4 |
0.1 |
| Accuracy, % | 87.7 | 72.7 | 78.6 | 81.8 |
The addition of midkine to VUC on the basis of
variant 1 lowered the sensitivity considerably, from 87.6% (VUC)
and 69.7% (midkine) to 64.0%, but increased the specificity from
87.7% (VUC) and 77.9% (midkine) to 98.5%. By contrast, the
combination of VUC and midkine according to variant 2 improved the
sensitivity to 93.3%, but reduced the specificity to 66.2%.
Therefore, urinary midkine was not able to complement VUC or
replace it as a non-invasive method to detect BCa in the present
study.
Discussion
The aim of the present study was to validate urinary
midkine protein, suggested as a convenient biomarker for the
non-invasive detection of BCa (17,18), in an
independent patient cohort and to compare its diagnostic utility
with that of VUC.
With 3.8 times more male than female subjects and a
median age of 71 years, the present patient cohort reflected the
stated epidemiological parameters for BCa in Europe (2). In addition, >80% of patients with
new-onset and recurrent BCa exhibited NMIBC, which is in line with
the observations of Babjuk et al (2). By the inclusion of patients with RCC,
nephrolithiasis and non-malignant urological diseases (of the
bladder or kidney) in the control group, the present study was able
to investigate potential impacts of these conditions on the
determination of urinary midkine levels. This is an important
issue, as it was reported that expression of midkine protein may
only be detected in the kidney of adults at very low levels
(12). Furthermore, a potential
influence of renal function on the performance of urine-based
markers to detect BCa was demonstrated (26). A major advantage of the present study
in contrast to existing reports is that the recruited control
subjects appear more suitable than healthy individuals for
evaluation of putative urinary biomarkers, as they more closely
reflect the target population and permit the definition of better
cut-off values for the tested parameters. In particular, the CC
group is of great value, as these patients resemble the BCa
patients most closely with regard to clinical symptoms. Using
healthy controls with no evidence of urological disease may lead to
overestimation of the obtained results, as the calculated threshold
value may be too low.
The analysis of urinary midkine protein revealed
significantly elevated midkine concentrations in BCa patients vs.
controls. This observation is in agreement with two previous
reports that also described increased midkine protein levels in
urine specimens of BCa patients (17,18). In
the present study, the calculated AUC value of urinary midkine for
the prediction of BCa was 0.759, which was lower compared to the
AUC value of 0.857 for midkine reported by Soukup et al
(18). This may be due to the
differing composition of the control group used by Soukup et
al (18), who compared patients
with primary occurrence of BCa with healthy controls. Due to the
aforementioned reasons, using healthy controls may lead to an
overestimation of the obtained differences between BCa patients and
controls. Although overexpression of midkine protein has been
reported for cancerous prostate tissue (27), the comparison of midkine
concentrations in urine specimens from BCa patients with
concomitant PCa revealed no statistically significant difference
compared with BCa patients without PCa (data not shown).
Contrasting with survivin, one of the most promising biomarkers in
the diagnosis of BCa (28), PCa does
not contribute to urinary midkine concentrations in the present
study.
Additional evaluation of midkine protein levels in
urine specimens of BCa patients with various tumor stages and
grades revealed a correlation between urinary midkine concentration
and disease severity. This result is in agreement with other
molecular-based tests, aimed at the quantification of soluble
proteins associated with BCa, for example, the analysis of vascular
endothelial growth factor or bladder tumor antigen in urine
(29–31). The more progressed the tumor was, the
higher the median urinary midkine concentration. Despite
significantly elevated midkine levels in the urine of BCa patients
with pTa tumors compared to controls, the diagnostic performance of
midkine for the identification of these patients was low (AUC,
0.659). By contrast, pT1 and ≥pT2a tumors were highly
distinguishable from controls (AUC, 0.926 and 0.935, respectively),
however, a further discrimination of pT1 and muscle-invasive
bladder tumors using midkine failed. In addition, urinary midkine
levels of patients with low-grade tumors were not significantly
different from controls, whereas patients with high-grade tumors
exhibited significantly elevated urinary midkine levels. These
observations are in accordance with Shimwell et al (17), who reported substantial elevation of
midkine protein in the urine of BCa patients, although not in those
with early-stage, low-grade disease. Notably, these and the present
results may reflect the transcript level (17), as it has been demonstrated that
urinary midkine mRNA ia more sensitive in the detection of
high-grade and high-stage BCa (32).
In addition, a number of other solid tumors express midkine at high
levels, and its expression increases with advancing tumor stage
(15,33). The low benefit of midkine as a
diagnostic marker for low-grade pTa and pTIS tumors is unfortunate
but comparable to other urine-based protein markers, including
cytokeratin 18 (34) and survivin
(35). However, as 70% of patients
with NMIBC have pTa tumors and recurrence is the main problem in
these patients (3), urinary midkine
alone is not reliable as a diagnostic marker for the surveillance
of patients with a history of BCa. Nevertheless, midkine was
observed to be highly suitable for the identification of more
severe pT1 and ≥pT2a lesions. This may offer the opportunity to use
midkine as a marker for the identification of high-risk
patients.
The comparison of urinary midkine with VUC as the
current reference standard for non-invasive diagnosis of BCa may
assist with evaluation of this biomarker. VUC clearly outperformed
urinary midkine, with an overall sensitivity and specificity of
87.6 and 87.7% compared with 69.7 and 77.9%, respectively.
Comparable to Soukup et al (18), but in contrast to further reports,
which claimed sensitivities of ~35% for VUC (8,36–38), the sensitivity of VUC was markedly
high in the present study, at >87%. This observation most
probably resulted from the 4.4-fold higher number of high-grade
tumors compared to low-grade tumors in the present patient cohort,
as it is well known that VUC is most suitable for the diagnosis of
high-grade tumors (39–41). Taking this into account, the
sensitivity of VUC for BCa patients with low-grade and G1 tumors
was only 60.0 and 57.1%, respectively. However, with sensitivities
of 46.7% (low-grade tumors) and 50.0% (G1 tumors), urinary midkine
was an even poorer detection method. The comparison of midkine with
other biomarker studies is limited by variations in study design,
composition of investigated patient and control cohorts or applied
analysis methods. Nevertheless, contrasting with urinary midkine,
survivin was more sensitive and less specific than urine cytology
according to previously published data (35,42–44).
A newly developed urinary test must achieve
sensitivities of 90–95% to earn a broad acceptance as an
alternative to cystoscopy (45,46). The
challenge is to identify adjunct biomarkers that assist with
increasing the low sensitivity of VUC while maintaining its high
specificity. Previously, the concept of a single marker for the
diagnosis of BCa was replaced by the idea to establish multi-marker
panels that facilitate higher sensitivities (18,47,48).
However, with the combined use of VUC and urinary midkine, the
present study was not able to improve the diagnostic performance
compared with VUC alone. An increased combined sensitivity was
accompanied by a reduced combined specificity. Similar observations
were made by several other groups, who showed that the more markers
used in parallel for the detection of BCa the lower the specificity
of the test (18,49). Therefore, the approach suggested by
Lalkhen and McCluskey may serve as good alternative (25). Patients who are initially positive to
a test with high sensitivity/low specificity should be subjected to
a second test with low sensitivity/high specificity. They proposed
that in this way, almost all of the false positives may be
correctly identified as disease negative. Although the utility of
urinary midkine protein for the early, non-invasive diagnosis of
low-grade, less progressed bladder tumors is limited, urinary
midkine was observed to be a suitable marker for the identification
of patients at high risk of tumor progression. In addition, in
combination with additional transcriptional or proteomic markers
(e.g. keratin 20, hyaluronic acid/hyaluronidase), that will
recognize low-grade tumors more effectively (50,51),
midkine may have the potential to contribute to the non-invasive
diagnosis and monitoring of BCa.
Acknowledgements
The present study was funded by the German Federal
Ministry of Education and Research (grant no., 16SV6070).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Babjuk M, Burger M, Zigeuner R, Shariat
SF, van Rhijn BW, Compérat E, Sylvester RJ, Kaasinen E, Böhle A,
Redorta J Palou and Rouprêt M: European Association of Urology: EAU
guidelines on non-muscle-invasive urothelial carcinoma of the
bladder: Update 2013. Eur Urol. 64:639–653. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
van Rhijn BWG, Burger M, Lotan Y, Solsona
E, Stief CG, Sylvester RJ, Witjes JA and Zlotta AR: Recurrence and
Progression of disease in non-muscle-invasive bladder cancer: From
epidemiology to treatment strategy. Eur Urol. 56:430–442. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Svatek RS, Hollenbeck BK, Holmäng S, Lee
R, Kim SP, Stenzl A and Lotan Y: The economics of bladder cancer:
Costs and considerations of caring for this disease. Eur Urol.
66:253–262. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Talwar R, Sinha T, Karan SC, Doddamani D,
Sandhu A, Sethi GS, Srivastava A, Narang V, Agarwal A and Adhlakha
N: Voided urinary cytology in bladder cancer: Is it time to review
the indications? Urology. 70:267–271. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Raitanen MP, Aine R, Rintala E, Kallio J,
Rajala P, Juusela H and Tammela TL: FinnBladder Group: Differences
between local and review urinary cytology in diagnosis of bladder
cancer. An interobserver multicenter analysis. Eur Urol.
41:284–289. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lokeshwar VB, Habuchi T, Grossman HB,
Murphy WM, Hautmann SH, Hemstreet GP III, Bono AV, Getzenberg RH,
Goebell P, Schmitz-Dräger BJ, et al: Bladder tumor markers beyond
cytology: International Consensus Panel on bladder tumor markers.
Urology. 66(6): Suppl 1. S35–S63. 2005. View Article : Google Scholar
|
|
8
|
van Rhijn BW, van der Poel HG and van der
Kwast TH: Urine markers for bladder cancer surveillance: A
systematic review. Eur Urol. 47:736–748. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Vrooman OP and Witjes JA: Urinary markers
in bladder cancer. Eur Urol. 53:909–916. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xylinas E, Kluth LA, Rieken M, Karakiewicz
PI, Lotan Y and Shariat SF: Urine markers for detection and
surveillance of bladder cancer. Urol Oncol. 32:222–229. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Smith ZL and Guzzo TJ: Urinary markers for
bladder cancer. F1000Prime Reports. 5:212013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sakamoto K and Kadomatsu K: Midkine in the
pathology of cancer, neural disease, and inflammation. Pathol Int.
62:445–455. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jones DR: Measuring midkine: The utility
of midkine as a biomarker in cancer and other diseases. Br J
Pharmacol. 171:2925–2939. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Velculescu VE, Madden SL, Zhang L, Lash
AE, Yu J, Rago C, Lal A, Wang CJ, Beaudry GA, Ciriello KM, et al:
Analysis of human transcriptomes. Nat Genet. 23:387–388. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ikematsu S, Okamoto K, Yoshida Y, Oda M,
Sugano-Nagano H, Ashida K, Kumai H, Kadomatsu K, Muramatsu H,
Muramatsu T and Sakuma S: High levels of urinary midkine in various
cancer patients. Biochem Biophys Res Commun. 306:329–332. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
O'Brien T, Cranston D, Fuggle S, Bicknell
R and Harris AL: The angiogenic factor midkine is expressed in
bladder cancer, and overexpression correlates with a poor outcome
in patients with invasive cancers. Cancer Res. 56:2515–2518.
1996.PubMed/NCBI
|
|
17
|
Shimwell NJ, Bryan RT, Wei W, James ND,
Cheng KK, Zeegers MP, Johnson PJ, Martin A and Ward DG: Combined
proteome and transcriptome analyses for the discovery of urinary
biomarkers for urothelial carcinoma. Br J Cancer. 108:1854–1861.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Soukup V, Kalousová M, Capoun O, Sobotka
R, Breyl Z, Pešl M, Zima T and Hanuš T: Panel of urinary diagnostic
markers for non-invasive detection of primary and recurrent
urothelial urinary bladder carcinoma. Urol Int. 95:56–64. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sobin LH, Gospodarowicz M and Wittekind C:
TNM Classification of Malignant Tumors. 7th. Wiley-Blackwell;
Hoboken, NJ: pp. 262–265. 2009
|
|
20
|
Eble JN, Sauter G, Epstein JI and
Sesterhenn IA: World Health Organization Classification of
TumoursPathology and Genetics of Tumours of the Urinary System and
Male Genital Organs. IARC Press; Lyon: pp. 87–157. 2004
|
|
21
|
Mostofi FK, Sobin LH and Torlonie H:
Histological Typing of Urinary Bladder Tumours. 10. World Health
Organization; Geneva: pp. 171973
|
|
22
|
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis
CA, Glasziou PP, Irwig LM, Moher D, Rennie D, de Vet HC and Lijmer
JG: Standards for Reporting of Diagnostic Accuracy Group: The STARD
statement for reporting studies of diagnostic accuracy: Explanation
and elaboration. The Standards for Reporting of Diagnostic Accuracy
Group. Croat Med J. 44:639–650. 2003.PubMed/NCBI
|
|
23
|
Papanicolaou GN and Marshall VF: Urine
sediment smears as a diagnostic procedure in cancers of the urinary
tract. Science. 101:519–520. 1945. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Youden WJ: Index for rating diagnostic
tests. Cancer. 3:32–35. 1950. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lalkhen AG and McCluskey A: Clinical
tests: Sensitivity and specificity. Contin Educ Anaesth Crit Care
Pain. 8:221–223. 2008. View Article : Google Scholar
|
|
26
|
Todenhöfer T, Hennenlotter J, Witstruk M,
Gakis G, Aufderklamm S, Kuehs U, Stenzl A and Schwentner C:
Influence of renal excretory function on the performance of urine
based markers to detect bladder cancer. J Urol. 187:68–73. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Konishi N, Nakamura M, Nakaoka S, Hiasa Y,
Cho M, Uemura H, Hirao Y, Muramatsu T and Kadomatsu K:
Immunohistochemical analysis of midkine expression in human
prostate carcinoma. Oncology. 57:253–257. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Davies B, Chen J, Modugno F, Weissfeld J,
Landsittel D, Dhir R, Nelson J and Getzenberg RH: Contribution of
the prostate limits the usefulness of survivin for the detection of
bladder cancer. J Urol. 174:1767–1770. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Boman H, Hedelin H and Holmäng S: Four
bladder tumor markers have a disappointingly low sensitivity for
small size and low grade recurrence. J Urol. 167:80–83. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lotan Y and Roehrborn CG: Sensitivity and
specificity of commonly available bladder tumor markers versus
cytology: Results of a comprehensive literature review and
meta-analyses. Urology. 61:109–118. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sun Y, He DL, Ma Q, Wan XY, Zhu GD, Li L,
Luo Y, He H and Yang L: Comparison of seven screening methods in
the diagnosis of bladder cancer. Chin Med J (Engl). 119:1763–1771.
2006.PubMed/NCBI
|
|
32
|
Holyoake A, O'Sullivan P, Pollock R, Best
T, Watanabe J, Kajita Y, Matsui Y, Ito M, Nishiyama H, Kerr N, et
al: Development of a multiplex RNA urine test for the detection and
stratification of transitional cell carcinoma of the bladder. Clin
Cancer Res. 14:742–749. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ikematsu S, Nakagawara A, Nakamura Y,
Sakuma S, Wakai K, Muramatsu T and Kadomatsu K: Correlation of
elevated level of blood midkine with poor prognostic factors of
human neuroblastomas. Br J Cancer. 88:1522–1526. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sánchez-Carbayo M, Urrutia M, González de
Buitrago JM and Navajo JA: Evaluation of two new urinary tumor
markers: Bladder tumor fibronectin and cytokeratin 18 for the
diagnosis of bladder cancer. Clin Cancer Res. 6:3585–3594.
2000.PubMed/NCBI
|
|
35
|
Abd El-Hakim TF, El-Shafie MK, Abdou AG,
Azmy RM, El-Naidany SS and El-Din MO Badr: Value of urinary
survivin as a diagnostic marker in bladder cancer. Anal Quant
Cytopathol Histpathol. 36:121–127. 2014.PubMed/NCBI
|
|
36
|
Konety BR: Molecular markers in bladder
cancer: A critical appraisal. Urol Oncol. 24:326–337. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yafi FA, Brimo F, Steinberg J, Aprikian
AG, Tanguay S and Kassouf W: Prospective analysis of sensitivity
and specificity of urinary cytology and other urinary biomarkers
for bladder cancer. Urol Oncol. 33:e25–e31. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ye F, Wang L, Castillo-Martin M, McBride
R, Galsky MD, Zhu J, Boffetta P, Zhang DY and Cordon-Cardo C:
Biomarkers for bladder cancer management: Present and future. Am J
Clin Exp Urol. 2:1–14. 2014.PubMed/NCBI
|
|
39
|
Raab SS, Grzybicki DM, Vrbin CM and
Geisinger KR: Urine cytology discrepancies-Frequency, causes, and
outcomes. Am J Clin Pathol. 127:946–953. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Reid MD, Osunkoya AO, Siddiqui MT and
Looney SW: Accuracy of grading of urothelial carcinoma on urine
cytology: An analysis of interobserver and intraobserver agreement.
Int J Clin Exp Pathol. 5:882–891. 2012.PubMed/NCBI
|
|
41
|
Sullivan PS, Chan JB, Levin MR and Rao JY:
Urine cytology and adjunct markers for detection and surveillance
of bladder cancer. Am J Transl Res. 2:412–440. 2010.PubMed/NCBI
|
|
42
|
Ku JH, Godoy G, Amiel GE and Lerner SP:
Urine survivin as a diagnostic biomarker for bladder cancer: A
systematic review. BJU Int. 110:630–636. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Schultz IJ, Witjes JA, Swinkels DW and de
Kok JB: Bladder cancer diagnosis and recurrence prognosis:
Comparison of markers with emphasis on survivin. Clin Chim Acta.
368:20–32. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Srivastava AK, Singh PK, Srivastava K,
Singh D, Dalela D, Rath SK, Goel MM and Bhatt ML Brahma: Diagnostic
role of survivin in urinary bladder cancer. Asian Pac J Cancer
Prev. 14:81–85. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Vriesema JL, Poucki MH, Kiemeney LA and
Witjes JA: Patient opinion of urinary tests versus flexible
urethrocystoscopy in follow-up examination for superficial bladder
cancer: A utility analysis. Urology. 56:793–797. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yossepowitch O, Herr HW and Donat SM: Use
of urinary biomarkers for bladder cancer surveillance: Patient
perspectives. J Urol. 177:1277–1282. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Todenhöfer T, Hennenlotter J, Esser M,
Mohrhardt S, Tews V, Aufderklamm S, Gakis G, Kuehs U, Stenzl A and
Schwentner C: Combined application of cytology and molecular urine
markers to improve the detection of urothelial carcinoma. Cancer
cytopathology. 121:252–260. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Todenhöfer T, Hennenlotter J, Guttenberg
P, Mohrhardt S, Kuehs U, Esser M, Aufderklamm S, Bier S, Harland N,
Rausch S, et al: Prognostic relevance of positive urine markers in
patients with negative cystoscopy during surveillance of bladder
cancer. BMC Cancer. 15:1552015. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Eissa S, Salem AM, Zohny SF and Hegazy MG:
The diagnostic efficacy of urinary TGF-beta1 and VEGF in bladder
cancer: Comparison with voided urine cytology. Cancer Biomark.
3:275–285. 2007.PubMed/NCBI
|
|
50
|
Lokeshwar VB, Obek C, Pham HT, Wei D,
Young MJ, Duncan RC, Soloway MS and Block NL: Urinary hyaluronic
acid and hyaluronidase: Markers for bladder cancer detection and
evaluation of grade. J Urol. 163:348–356. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Schmidt J, Propping C, Siow WY,
Lohse-Fischer A, Toma M, Baldauf-Twelker A, Hakenberg OW, Wirth MP
and Fuessel S: Diagnostic and prognostic value of bladder
cancer-related transcript markers in urine. J Cancer Res Clin
Oncol. 142:401–414. 2016. View Article : Google Scholar : PubMed/NCBI
|