Introduction
Colorectal cancer (CRC) survivors are at high risk
of cancer recurrence, with recurrent disease being detected in
30–50% of patients undergoing curative resection (1). The primary goal of post-treatment
surveillance is to detect recurrences at an early stage when they
are potentially curable. It has been demonstrated that although the
majority of cases of relapsed CRC are inoperable at the time of
diagnosis, one-third of patients with isolated locoregional or
distant metastases survive 5 years (2).
Carcinoembryonic antigen (CEA) is a glycoprotein
oncofetal antigen that is expressed by a number of epithelial
tumors and whose serum levels could also increase in non-malignant
conditions such as inflammatory bowel diseases (3). In total, 70% CRC patients will exhibit
an elevated CEA level at the time of diagnosis, meaning that it may
be a useful marker for curing and monitoring the disease
post-surgery (1). Nevertheless, a
recent meta-analysis of 20 studies, which included 4,285 patients,
revealed controversies regarding the utility of the technique in
the detection of recurrent disease (4). An overall sensitivity of 64% and a
specificity of 90% was found, which is poor for the use of a
biomarker on its own. It was concluded that the optimal balance of
sensitivity and specificity occurred at 2.2 ng/ml (4).
Carbohydrate antigen 19–9 (CA 19–9) assays measure a
tumor-related mucin (5). The poor
performance of this biomarker compared with CEA has been reported,
with serum CA 19–9 being greater than normal in only 20–40% of
metastatic CRC cases (6). In the
post-operative follow-up, additional CA 19–9 measurements do not
increase the likelihood of detecting recurrence and monitoring the
levels of this sole biomarker during chemotherapy (CHT) is not
sufficient (7).
The major limitation of morphological imaging in the
assessment of recurrence across all common types of cancer is the
use of size and/or the disappearance of normal features in tissues.
Therefore, in common clinical routine, fluorodeoxyglucose
(2-deoxy-2-(18F)fluoro-D-glucose;
18F-FDG) positron emission
tomography/computed tomography (PET/CT) has a major role in the
assessment of recurrent CRC (8–12). PET/CT
has the ability to detect cancer via the evaluation of tissue
metabolism, which is pathologically increased prior to the
appearance of morphological changes.
The present study aimed to investigate the potential
role of the CEA and CA 19–9 biomarkers in the selection of subjects
for imaging, in those individuals with a previous history of CRC,
by analyzing 18F-FDG PET/CT results in a population with
normal or abnormal serum CEA and CA 19–9 levels (normal range, 0–5
ng/ml and 0–37 U/ml, respectively).
Patients and methods
Patients
A total of 100 consecutive patients (mean age ±
standard deviation, 67.7±8 years; range, 35–82 years) undergoing a
PET/CT examination for the follow-up of CRC at the Policlinico Tor
Vergata (Rome, Italy) between January 2014 and December 2015 were
retrospectively evaluated. Of these 100 subjects, 25 were smokers.
All patients had suspected recurrence based on elevated CEA or CA
19–9 levels, clinical symptoms and/or other imaging modalities.
Patients with a clinical history that was positive for other tumors
were excluded from the study. Patients with comorbidities (i.e.,
Parkinson's disease and cardiovascular disease) were included in
the study. All patients underwent whole-body 18F-FDG
PET/CT following treatment. A general overview of the population
examined is shown in Table I. Of the
100 patients examined, the primitive lesion was located in the
colon in 58 subjects and in the sigmoid colon in 17 subjects, while
25 had a lesion detectable in the rectum.
 | Table I.General overview of the population
examined in the study. |
Table I.
General overview of the population
examined in the study.
| Factor | Whole population
(n=100) | Recurrence-positive
on PET/CT (n=60) | Recurrence-negative
on PET/CT (n=40) | P-value (positive vs.
negative) |
|---|
| Age, years | 66.75±8.12 | 69.23±6.33 | 66.33±5.54 | >0.05 |
| CEA, ng/ml | 23.78±107.63 | 33.07±136.74 | 10.15±30 | 0.001; AUC=0.70 |
| CA 19–9, U/ml | 72.07±190.31 | 67.76±190.41 | 75.24±192.33 | 0.44; AUC=0.55 |
The initial treatment consisted of surgery, CHT and
radiotherapy (RT). At the time of the examination all the patients
had been subjected to surgery, 3 to RT and 47 to CHT. In
particular, 13 patients were subjected to all three treatments
(surgery, RT and CHT); 37 to two treatments (surgery and CHT) and
50 to surgery alone. Therapy was discontinued according to standard
guidelines, with all the patients having a maximum of 6 months wash
out from the various treatments prior to the PET/CT scan (13). The mean time between the measurement
of CEA and CA 19–9 and the PET/CT scan was 30 (±12) days.
The level of serum CEA was above the normal range in
61.0% of the patients (61/100), while the level of CA 19–9 was
increased in 48 subjects (48.0%). No evidence of paraneoplastic
syndrome was found in any of the 100 patients at the time of
presentation.
Informed consent was obtained from all patients, in
accordance with the Declaration of Helsinki of 1975, as revised in
2008 (14).
PET/CT scanning
The PET/CT system Discovery ST16 (GE Medical
Systems, Knoxville, TN, USA) was used to assess 18F-FDG
distribution in all patients by three-dimensional (3D) mode
standard technique. Reconstruction was performed using the ordered
subsets expectation maximization 3D reconstruction method, with 30
subsets and 2 iterations. The system combines a high-speed ultra
16-detector row (912 detectors per row) CT unit and a PET scanner
with 10,080 bismuth germanate crystals in 24 rings. The axial
full-width at a half-maximum 1-cm radius is 5.2 mm in 3D mode and
the axial field of view is 157 mm. All patients fasted for a
minimum of 5 h prior to the intravenous (i.v.) injection of
18F-FDG; the level of serum glucose was ≤107 mg/dl in
all patients. All patients received 2.5 MBq/kg ±10% (210–410 MBq)
of i.v. 18F-FDG and were hydrated with 500 ml of 0.9%
i.v. saline sodium chloride. A dedicated room was used for the
injection of 18F-FDG for each patient. The lights were
turned off and the patients were required to remain resting with
their eyes closed prior to the PET/CT scan. A whole-body PET/CT
scan was performed 60 min after 18F-FDG injection. A
low-amperage whole-body CT scan for attenuation correction (40 mA
and 120 kV) was performed prior to image acquisition using PET
according to standard guidelines.
Evaluation of PET/CT images
Two nuclear medicine physicians reviewed the PET/CT
images at the applicable dedicated PET/CT workstation (Advantage
4.4 and Xeleris 2; GE Healthcare, Fairfield, Connecticut, USA),
allowing visualization of PET and CT images separately or in fusion
mode in the axial, coronal and sagittal planes. According to our
previously reported study in this field (15), pathological uptake was considered when
a focal tracer uptake area greater than the background was detected
visually. The patients were thereby classified as positive or
negative for recurrence. Maximum standardized uptake values were
also measured and considered, however, no absolute cut-off value
was used for the diagnosis. If a difference in opinion was recorded
when assessing the results, the patients were re-examined and a
consensus was reached.
Truth standard
A true-positive PET/CT result was defined by the
following criteria: Histopathological findings obtained at a
subsequent biopsy or a reduced biomarker level following salvage
therapy with respect to local recurrence (LR); histopathological
findings obtained at subsequent surgical lymphadenectomy or biopsy
with respect to lymph node (LN) metastases; histopathological
findings that were confirmed by biopsy or subsequent confirmation
with dedicated CT or magnetic resonance (MR) imaging with regard to
skeletal metastases; and a follow-up time of >6 months (using MR
imaging, CT or PET/CT) revealing that the suspected lesions had
increased in size. Alternatively, resolution of the lesions or a
reduction in the size of the suspected lesions associated with
salvage therapy were considered.
Statistical analysis
The mean and standard deviation for CEA and CA 19–9
were calculated (Table I).
Associations between the serum levels of CEA and CA 19–9 were
evaluated by Spearman's rank correlation (since data were not
normally distributed as detectable by means of the D'Agostino and
Pearson omnibus normality test).
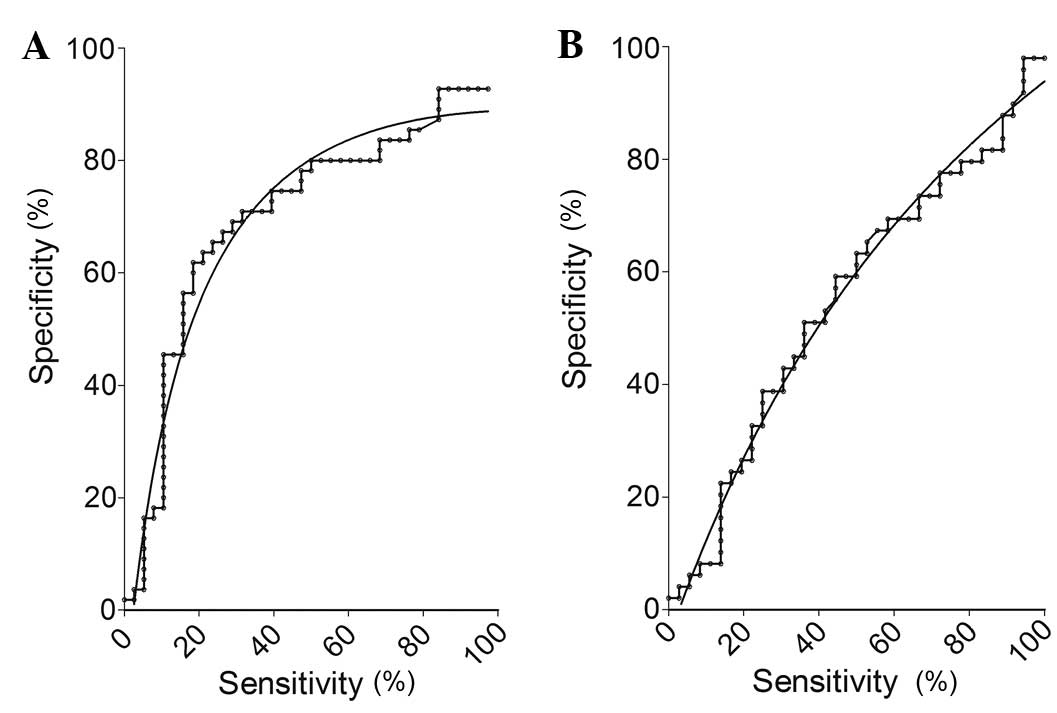
Differences in CA and CA 19–9 serum values among
patients with either negative or positive scans (Table I) were studied by means of a receiver
operating characteristics (ROC) curve. A ROC curve was used in
order to establish the optimal threshold for CEA and CA 19–9. Since
no significant difference in CA 19–9 were detected when comparing
patients with positive vs. negative PET/CT results, no thresholds
for this biomarker were selected. Differences in CEA and CA 19–9
serum levels between smokers and non-smokers were evaluated by
Mann-Whitney U test.
In agreement with the values reported in Table I and the ROC curve results, patients
were classified into groups depending on a CEA value of ≤3.5 or
>3.5 ng/ml.
Fisher's exact test was used in order to investigate
the differences in the detection rate (DR) of PET/CT among groups.
P≤0.05 was used to indicate a statistically significant
difference.
Results
Overall, 59 out of the 100 patients examined showed
normal serum CEA levels (<5 ng/ml), while 33 showed abnormal CA
19–9 levels (>37 U/ml). No significant differences were found
when comparing CEA and CA 19–9 serum levels between smokers and
non-smokers, with serum levels in these subjects being equal to
28.87 (±92.83) ng/ml for CEA and to 82.17 (±188.2) U/ml for CA 19–9
(P>0.05). As shown in Table I,
PET/CT was positive for recurrence in 60/100 patients (60.0%) and
negative for recurrence in 40/100 patients (40.0%). Patients with a
positive scan exhibited higher CEA levels compared with those with
negative scans (P<0.05). A CEA value of ≤3.5 ng/ml was
associated with a positive scan in 15/43 subjects (34.9%), while
45/57 subjects (78.9%) with a CEA cut-off value of >3.5 ng/ml
were positive for recurrence on PET/CT [sensitivity, 80%; 95%
confidence interval (CI), 67%-89%; and specificity, 60%; 95% CI,
45–78%). ROC curve analyses for CEA and CA 19–9 are provided in
Fig. 1. The DRs were significantly
different (P=0.027).
No statistically significant differences were found
in the comparison between the CA19.9 levels of patients with
positive or negative scans (P>0.05). However, a significant
association was found between the serum levels of CEA and CA 19–9
(r=0.316; P=0.006).
At the PET/CT examination, 13 out of the 100
subjects examined were positive for LR only, 7 were positive for LR
and LN, 2 presented with LR and liver lesions, 2 with LR and liver
and peritoneal lesions, and 2 with LR and lung lesions.
Furthermore, 2 patients were positive for LR, LN and adrenal
lesions, 4 presented with lesions in the LNs only and 7 with
lesions in the LNs and lungs. Lung lesions only were detectable in
5 subjects, liver lesions only were detectable in 11 subjects, and
lung and liver lesions were detectable in 9 subjects.
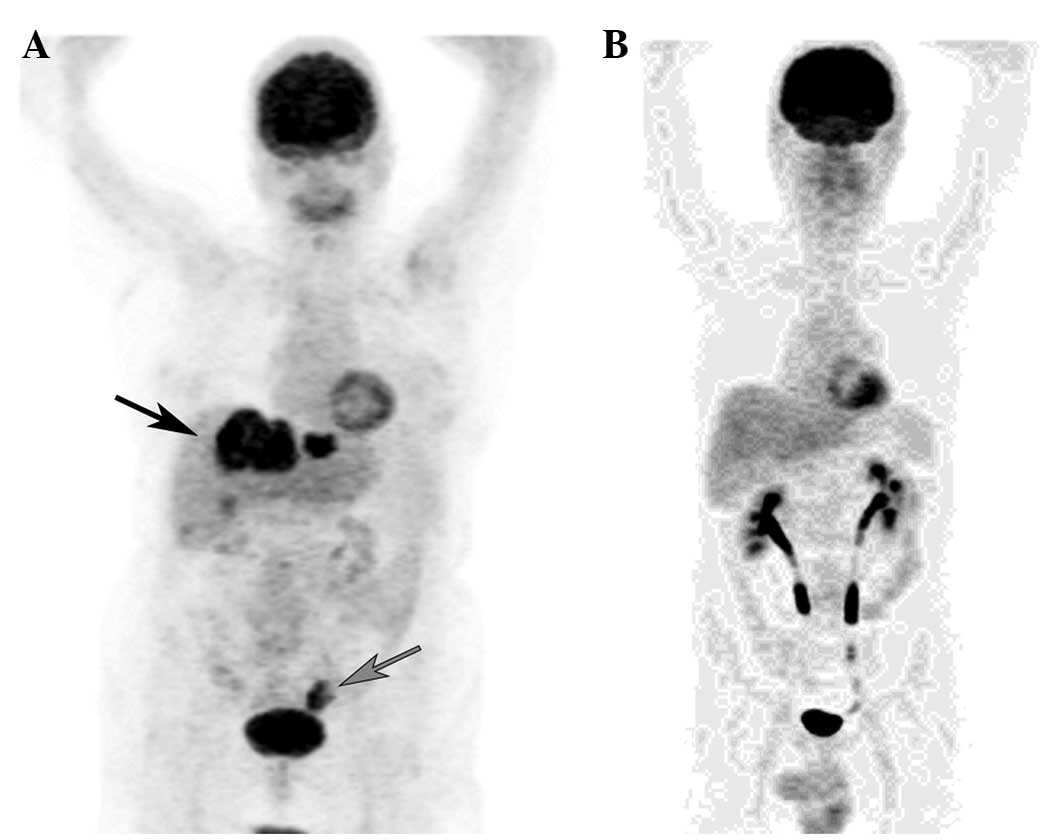
Representative PET images of recurrence-positive and
recurrence-negative cases are shown in Fig. 2.
With the exception of 2 subjects that experienced
liver recurrence that was not detectable upon 18F-FDG
PET/CT (false-negative), all the findings of PET/CT images were
confirmed by clinical, imaging and follow-up data.
Discussion
The main finding of the present study in that the DR
of PET/CT increases when a cut-off level of 3.5 ng/ml is used for
the CEA level. The DR in fact was equal to 79% when a cut-off value
of ≥3.5 ng/ml was used for patient selection, which was
significantly higher compared with the DR of PET/CT in the whole
population examined (60.0%) and in the subjects with CEA serum
levels of <3.5 ng/ml (35.0%). On the other hand, no significant
differences in CA 19–9 serum levels were detected in the subjects
with either a positive or a negative PET/CT scan, suggesting that
this biomarker represents a poor parameter for patient selection in
the present study.
18F-FDG PET/CT has been proven to be a
meaningful diagnostic modality in the management of various
cancers, with accuracy in the detection of recurrence and treatment
response evaluation in patients with CRC and other types of tumors,
such as s ovarian cancer, and Hodgkin and non-Hodgkin lymphomas
(15–17). It has been shown that PET has higher
sensitivity as compared with CT in the detection of abdominal and
extra-abdominal metastatic sites (17). However, PET alone has the limitation
of poor localization and thereby increases the number of
false-positive results that lead to a lower specificity (18). In a recent meta-analysis that included
11 studies with a total of 510 patients, it was estimated that the
sensitivity and specificity of 18F-FDG PET/CT in the
detection of tumor recurrence in CRC patients with elevated CEA
were 90.3% (95% CI, 67.0–89.6%) and 80.0% (95% CI, 67–89.6%),
respectively (19).
To the best of our knowledge, few studies have been
performed in order to investigate the performance of
18F-FDG PET/CT in the detection of recurrent CRC in
patients with normal CEA and CA 19–9 serum levels. One of the most
cited papers aimed at the comparison of PET/CT performance in
patients with normal and elevated CEA levels was performed on a
pool of 235 patients (11). CRC
recurrence was detected in 64.4% of patients with CEA levels <5
ng/ml (sensitivity and specificity of 100 and 84%, respectively)
and 88% of patients with levels >5 ng/ml (sensitivity and
specificity of 97.1 and 95.7%, respectively) (11).
In past years, several studies have been performed
in order to define the ideal parameters in patient selection aimed
to decrease the number of patients undergoing 18F-FDG
PET/CT (20–25). The main reason for this concern is
cost-effectiveness, with this nuclear medicine imaging modality
being an expensive examination. Together with the cited study by
Sanli et al (11), the results
of the present study suggested that satisfactory sensitivity and
specificities for detecting CRC recurrences can be obtained in
patients with a previous history of CRC even at normal CEA levels,
ruling out the selection of a patient based on abnormal levels of
this biomarker.
The sub-optimal levels of sensitivity and
specificity obtained in the present study may be explained by the
poor performance of PET/CT due to the tumor response to CHT, which
is typically associated with reduced glucose consumption that
causes the lesions less detectable on PET (26). While, on one hand, this imaging
modality has shown a high sensitivity in the detection of tumor
response to therapy in various diseases (18), the absence of pathological metabolism
does not mean a complete response to therapy, 85% of lesions that
exhibit the disappearance of pathological glucose consumption after
CHT showing detectable cancer cells (27). It is possible that the conjunction of
PET with contrast-enhanced CT could assist in identifying
physiological 18F-FDG in normal tissues and could
conversely identify the pathological 18F-FDG uptake in
tissues with no pathological abnormalities, increasing the
sensitivity and specificity.
As a last aspect, in addition to the absolute CEA
and CA 19–9 levels, the pattern of rise of these biomarkers over
time appears as a relevant index in patient selection (12). A recent study concluded that patients
with a single large increase in CEA may be referred directly for
PET, whereas a minor increase led to referral only when the
increasing trend had been confirmed in further assays (12). The use of serum biomarkers kinetics
indexes such as ‘velocity’ and ‘doubling time’ has proven to be a
significant advance in the selection of patients undergoing PET/CT
in the restaging of other oncological diseases, such as prostate
cancer (28). Additional studies are
required in order to investigate the performance of
18F-FDG PET/CT with regard to CEA and CA 19–9 kinetic
indexes.
In conclusion, the present study indicated that
18F-FDG PET/CT is able to detect recurrent CRC even in
patients with normal CEA levels. This imaging modality should be
recommended in patients with the suspected recurrence of CRC
regardless of the levels of serum biomarkers.
Acknowledgements
The present study was presented as abstract no. P678
at the Annual Congress of the European Association of Nuclear
Medicine October 10–14, 2015, Hamburg, Germany. This study was
supported by the PICASo project (grant no. 689209).
References
|
1
|
van de Velde CJ, Boelens PG, Borras JM,
Coebergh JW, Cervantes A, Blomqvist L, Beets-Tan RG, van den Broek
CB, Brown G, Van Cutsem E, et al: EURECCA colorectal:
Multidisciplinary management: European consensus conference colon
& rectum. Eur J Cancer. 50:1.e1–1.e34. 2014. View Article : Google Scholar
|
|
2
|
Bowne WB, Lee B, Wong WD, Ben-Porat L,
Shia J, Cohen AM, Enker WE, Guillem JG, Paty PB and Weiser MR:
Operative salvage for locoregional recurrent colon cancer after
curative resection: An analysis of 100 cases. Dis Colon Rectum.
48:897–909. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen CH, Hsieh MC, Lai CC, Yeh CY, Chen
JS, Hsieh PS, Chiang JM, Tsai WS, Tang R, Changchien CR and Wang
JY: Lead time of carcinoembryonic antigen elevation in the
postoperative follow-up of colorectal cancer did not affect the
survival rate after recurrence. Int J Colorectal Dis. 25:567–571.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tan E, Gouvas N, Nicholls RJ, Ziprin P,
Xynos E and Tekkis PP: Diagnostic precision of carcinoembryonic
antigen in the detection of recurrence of colorectal cancer. Surg
Oncol. 18:15–24. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Magnani JL, Steplewski Z, Koprowski H and
Ginsburg V: Identification of the gastrointestinal and pancreatic
cancer-associated antigen detected by monoclonal antibody 19-9 in
the sera of patients as a mucin. Cancer Res. 43:5489–5492.
1983.PubMed/NCBI
|
|
6
|
Filella X, Molina R, Piqué JM,
Garcia-Valdecasas JC, Grau JJ, Novell F, Astudillo E, de Lacy A,
Daniels M and Ballesta AM: Use of CA 19-9 in the early detection of
recurrences in colorectal cancer: Comparison with CEA. Tumour Biol.
15:1–6. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bast RC Jr, Ravdin P, Hayes DF, Bates S,
Fritsche H Jr, Jessup JM, Kemeny N, Locker GY, Mennel RG and
Somerfield MR: American Society of Clinical Oncology Tumor Markers
Expert Panel: 2000 update of recommendations for the use of tumor
markers in breast and colorectal cancer: Clinical practice
guidelines of the American Society of Clinical Oncology. J Clin
Oncol. 19:1865–1878. 2001.PubMed/NCBI
|
|
8
|
Panagiotidis E, Datseris IE, Rondogianni
P, Vlontzou E, Skilakaki M, Exarhos D and Bamias A: Does CEA and CA
19-9 combined increase the likelihood of 18F-FDG in detecting
recurrence in colorectal patients with negative CeCT? Nucl Med
Commun. 35:598–605. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ozkan E, Soydal C, Araz M and Aras G:
Serum carcinoembryonic antigen measurement, abdominal
contrast-enhanced computed tomography, and fluorine-18
fluorodeoxyglucose positron emission tomography/computed tomography
in the detection of colorectal cancer recurrence: A correlative
study. Nucl Med Commun. 33:990–994. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ozkan E, Soydal C, Araz M, Kir KM and Ibis
E: The role of 18F-FDG PET/CT in detecting colorectal cancer
recurrence in patients with elevated CEA levels. Nucl Med Commun.
33:395–402. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sanli Y, Kuyumcu S, Ozkan ZG, Kilic L,
Balik E, Turkmen C, Has D, Isik G, Asoglu O, Kapran Y and Adalet I:
The utility of FDG-PET/CT as an effective tool for detecting
recurrent colorectal cancer regardless of serum CEA levels. Ann
Nucl Med. 26:551–558. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gade M, Kubik M, Fisker RV,
Thorlacius-Ussing O and Petersen LJ: Diagnostic value of (18)F-FDG
PET/CT as first choice in the detection of recurrent colorectal
cancer due to rising CEA. Cancer Imaging. 15:112015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Boellaard R, Delgado-Bolton R, Oyen WG,
Giammarile F, Tatsch K, Eschner W, Verzijlbergen FJ, Barrington SF,
Pike LC, Weber WA, et al: FDG PET/CT: EANM procedure guidelines for
tumour imaging: Version 2.0. Eur J Nucl Med Mol Imaging.
42:328–354. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Puri KS, Suresh KR, Gogtay NJ and Thatte
UM: Declaration of Helsinki, 2008: Implications for stakeholders in
research. J Postgrad Med. 55:131–134. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chiaravalloti A, Danieli R, Caracciolo CR,
Travascio L, Cantonetti M, Gallamini A, Guazzaroni M, Orlacchio A,
Simonetti G and Schillaci O: Initial staging of Hodgkin's disease:
Role of contrast-enhanced 18F FDG PET/CT. Medicine (Baltimore).
93:e502014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ogunbiyi OA, Flanagan FL, Dehdashti F,
Siegel BA, Trask DD, Birnbaum EH, Fleshman JW, Read TE, Philpott GW
and Kodner IJ: Detection of recurrent and metastatic colorectal
cancer: Comparison of positron emission tomography and computed
tomography. Ann Surg Oncol. 4:613–620. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Caobelli F, Alongi P, Evangelista L,
Picchio M, Saladini G, Rensi M, Geatti O, Castello A, Laghai I and
Popescu CE: Predictive value of F-FDG PET/CT in restaging patients
affected by ovarian carcinoma: A multicentre study. Eur J Nucl Med
Mol Imaging. 43:404–413. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chiaravalloti A, Rubello D, Chondrogiannis
S, Giammarile F, Colletti PM and Schillaci O: Low-dose CT and
contrast-medium CT in hybrid PET/CT systems for oncologic patients.
Nucl Med Commun. 36:867–870. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lu YY, Chen JH, Chien CR, Chen WT, Tsai
SC, Lin WY and Kao CH: Use of FDG-PET or PET/CT to detect recurrent
colorectal cancer in patients with elevated CEA: A systematic
review and meta-analysis. Int J Colorectal Dis. 28:1039–1047. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fletcher JW, Djulbegovic B, Soares HP,
Siegel BA, Lowe VJ, Lyman GH, Coleman RE, Wahl R, Paschold JC,
Avril N, et al: Recommendations on the use of F-18-FDG PET in
oncology. J Nucl Med. 49:480–508. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Delgado-Bolton RC, Fernández-Pérez C,
González-Maté A and Carreras JL: Meta-analysis of the performance
of 18F-FDG PET in primary tumor detection in unknown primary
tumors. J Nucl Med. 44:1301–1314. 2003.PubMed/NCBI
|
|
22
|
Delgado-Bolton RC, Carreras JL and
Pérez-Castejón MJ: A systematic review of the efficacy of F-18-FDG
PET in unknown primary tumors. Curr Med Imaging Rev. 2:215–225.
2006. View Article : Google Scholar
|
|
23
|
Boellaard R, O'Doherty MJ, Weber WA, et
al: FDG PET and PET/CT: EANM procedure guidelines for tumour PET
imaging: Version 1.0. Eur J Nucl Med Mol Imaging. 37:181–200. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Delbeke D, Coleman RE, Guiberteau MJ,
Brown ML, Royal HD, Siegel BA, Townsend DW, Berland LL, Parker JA,
Hubner K, et al: Procedure guideline for tumor imaging with 18F-FDG
PET/CT 1.0. J Nucl Med. 47:885–895. 2006.PubMed/NCBI
|
|
25
|
Boellaard R, Delgado-Bolton R, Oyen WJ,
Giammarile F, Tatsch K, Eschner W, Verzijlbergen FJ, Barrington SF,
Pike LC, Weber WA, et al: European Association of Nuclear Medicine
(EANM): FDG PET/CT: EANM procedure guidelines for tumour imaging:
Version 2.0. Eur J Nuclear Med Mol Imaging. 42:328–354. 2015.
View Article : Google Scholar
|
|
26
|
de Geus-Oei LF, van Laarhoven HW, Visser
EP, Hermsen R, van Hoorn BA, Kamm YJ, Krabbe PF, Corstens FH, Punt
CJ and Oyen WJ: Chemotherapy response evaluation with FDG-PET
inpatients with colorectal cancer. Ann Oncol. 19:348–352. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tan MC, Linehan DC, Hawkins WG, Siegel BA
and Strasberg SM: Chemotherapy-induced normalization of FDG uptake
by colorectal liver metastases does not usually indicate complete
pathologic response. J Gastrointest Surg. 11:1112–1119. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Calabria F, Rubello D and Schillaci O: The
optimal timing to perform 18F/11C-choline PET/CT in patients with
suspicion of relapse of prostate cancer: Trigger PSA versus PSA
velocity and PSA doubling time. Int J Biol Markers. 29:e423–e430.
2014. View Article : Google Scholar : PubMed/NCBI
|