Introduction
Cholangiocarcinoma (CCA), an extremely rare and
highly aggressive malignant tumor was first described in 1957
(1). They are cancers of the
epithelial cells in the extrahepatic or intrahepatic biliary tree
of the bile duct from the bile ductules to the Ampulla of Vatar
(2–4).
CCA is often diagnosed in patients >60 years and the prognosis
is poor in the majority of cases (5,6).
Furthermore, CCA is often difficult to diagnose and treat due to
its growth pattern, silent nature (wherein its symptoms go
unnoticed by the patient until the advanced stage), anatomical
location, non-specific clinical presentation and limited clinical
approaches. CCA is the second most common primary hepatic tumor
globally, accounting for 3% of all gastrointestinal tumors, though
that rate is increasing (7,8). Worldwide, the highest CCA rates have
been reported in Eastern Asia, particularly Thailand, where its
high incidence is attributable to liver fluke infection (9). To the best of our knowledge, case
reports of distal extrahepatic CCA with two positive resection
margins are rare. This is the first reported CCA case from the
Caribbean (30 island nations, population, 39.8 million) and more
specifically, Trinidad and Tobago (population, 1.3 million).
Case report
The present study presents a case of a distal
extrahepatic cholangiocarcinoma with its imaging and
clinicopathological details, as well as the epidemiology of CCA in
Trinidad and Tobago. A 60-year-old male non-smoker of African and
Indian ethnicity, with no previously known medical conditions
presented to the Eric Williams Medical Sciences Complex, Champ
Fleurs (Trinidad and Tobago) with a 3-week history of painless
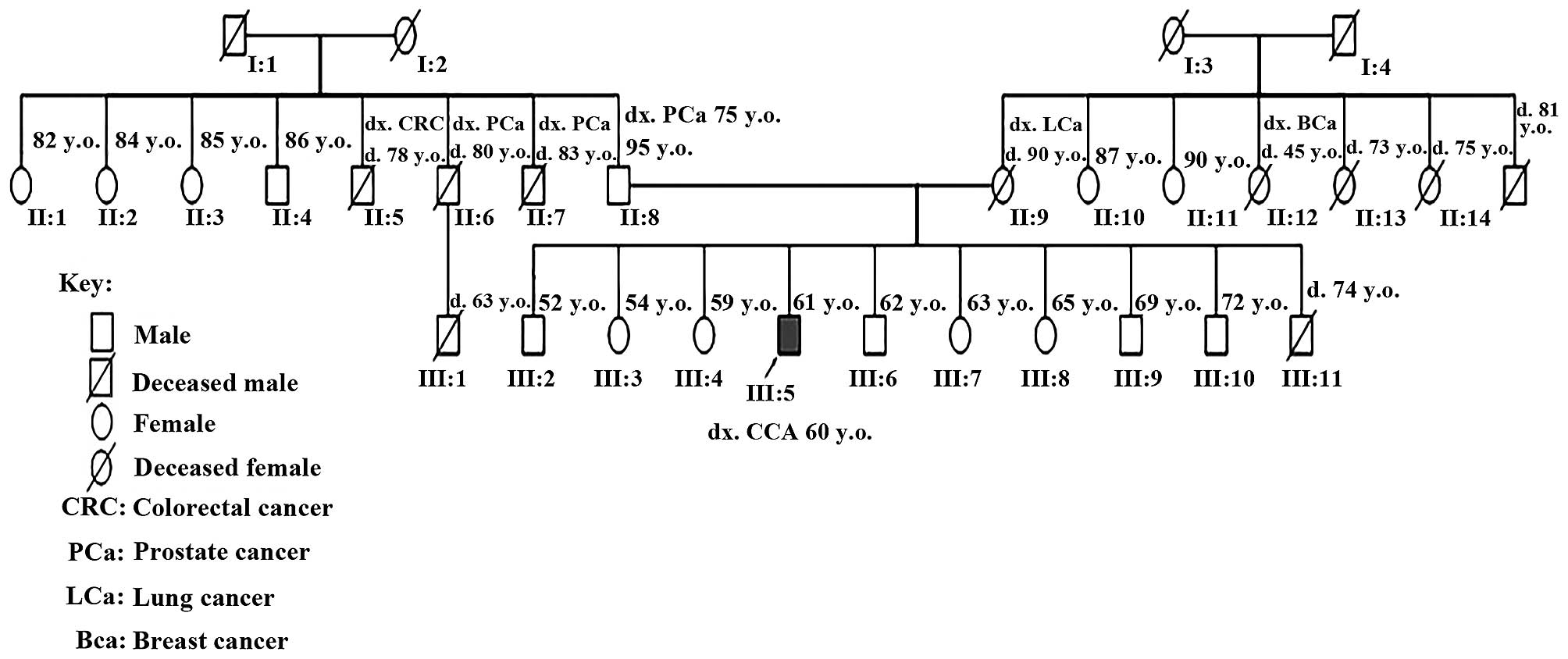
obstructive jaundice symptoms and subjective weight loss. The
patient has a family history of breast, prostate and lung cancer
(Fig. 1). The patient's mother and an
aunt succumbed to lung and breast cancer, respectively; the
patient's father has prostate cancer and several of his uncles have
prostate and/or colon cancer.
On examination, the patient had icterus and a
palpable gallbladder. Complete blood count, renal function and
international normalized ratio tests were normal, but his liver
function tests were abnormal: Total bilirubin, 9.1 mg/dl and
bilirubin, 4.5 mg/dl. Computed tomography (CT) of the chest,
abdomen and pelvis scan revealed dilated intra-hepatic ducts,
gallbladder, cystic duct and common hepatic duct, just distal to
entrance of cystic duct (Fig. 2).
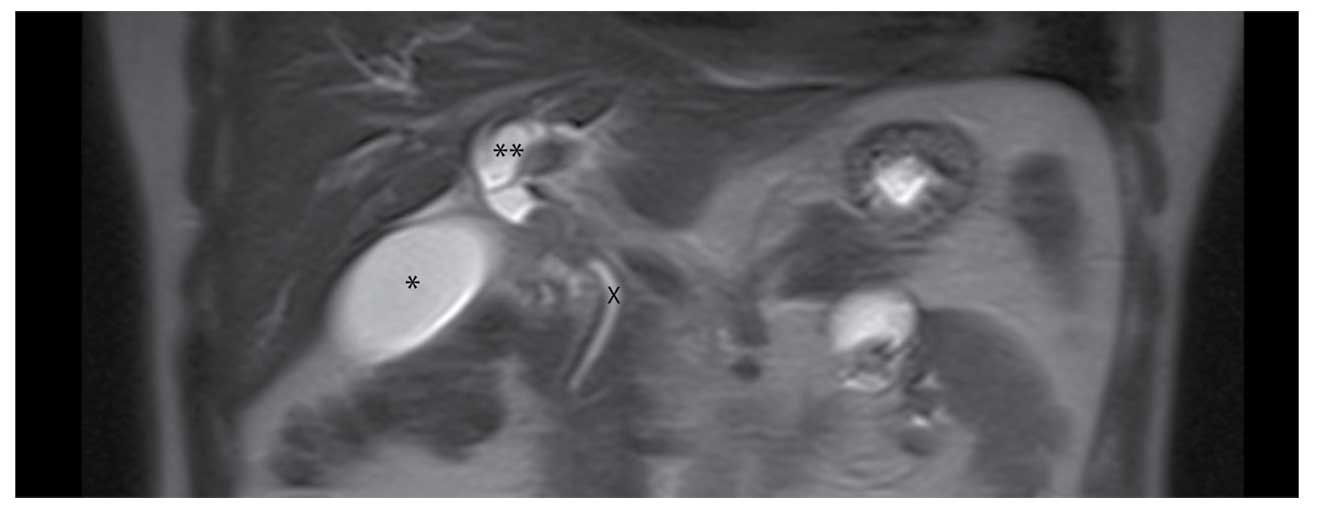
Magnetic resonance cholangiopancreatography (MRCP) revealed an
obstructing lesion in the common bile duct with proximal extent
just distal to the cystic duct and distal extent just superior to
the upper border of the pancreas (Fig.
3).
An initial bile duct excision was made 1 cm proximal
to the tumor and distally down to the upper border of the pancreas.
Kocherization of the duodenum allowed exposure of the
retroperitoneum and visualization of the neighboring structures. A
lymph node at station 8A was excised. Following bile duct excision,
imprint cytology demonstrated that both superior and inferior
margins were invaded by the tumor. The proximal bile duct was
re-excised to the hepatic ductal confluence, however, this margin
was also positive. A pancreaticoduodenectomy (Whipple procedure)
was performed to gain a clear distal margin but no further
resection was done on the proximal bile duct, due to the lack of
intra-operative imprint cytology at that time leaving us unable to
perform a right vs. left hepatectomy, as we were unsure which
hepatic duct was involved. The MRCP demonstrated it was free of
tumor and macroscopically both ducts appeared normal.
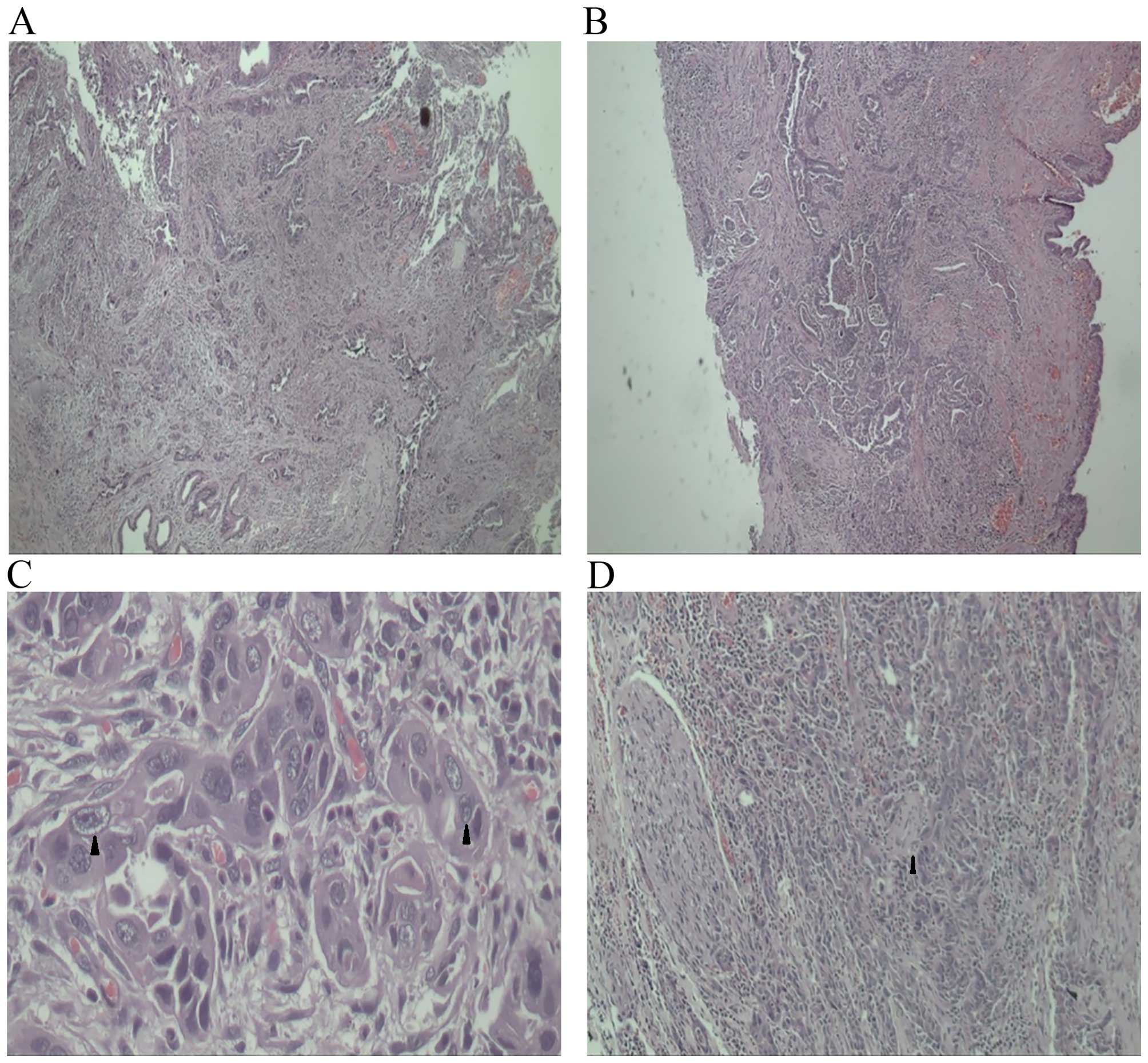
Macroscopically, the cut surface of common bile duct
revealed an ulcero-proliferative lesion (3.0×2.0×1.5 cm), 0.2 cm
from the proximal bile duct margin and 1.0 cm from the distal bile
duct margin. Histology revealed T2N1M0 moderately differentiated
CCA with a positive proximal resection margin and metastatic
deposits in station 8A lymph node along with peri-neural invasion
(Fig. 4). Post-operatively, the
patient had bile noted from the drains with resolution after two
weeks. Six-months postoperative, the patient is receiving adjuvant
chemotherapy (capecitabine) and has completed 30 cycles of external
beam radiotherapy to the porta hepatis due to the positive proximal
margin. At six months follow up, the patient showed small hepatic
metastasis upon CT screening.
Discussion
In Trinidad and Tobago there were 65 reported CCA
cases from 1995–2007, accounting for 0.41% of all incident cancer
cases (personal communication from the Trinidad and Tobago National
Cancer Registry). There was a slight male predilection (56.9%) and
the overall average incident age was 60–69 years. The present case
report, in addition to the majority of cases (66.1%) in TT
originate in the extrahepatic bile duct, with the remaining cases
occurring in the biliary track NOS (13.8%) followed by the Ampulla
of Vater (0.2%). Forty-six percent of cases were diagnosed at
autopsy and the majority of the other cases were diagnosed by
histology of the primary tumor. The majority of cases occurred in
nationals of African (63.1%), Indian (29.2%) then Mixed
(African-Indian) ancestry (7.7%). This contrasts with data from the
USA, where Hispanics and Asians have higher incident rates compared
to African Americans (7).
The general risk factors for cholangiocarcinoma are
primary sclerosing cholangitis (PSC), recurrent pyogenic
cholangitis, hepatolithiasis, primary biliary cirrhosis,
cholelithiasis, Asian liver flukes, biliary malformation (Caroli's
disease, choledochal cysts), toxins (thorotrast, dioxin, polyvinyl
chloride and heavy alcohol use), and viral infection (HIV,
hepatitis B and hepatitis C and EBV) (10–14). There
was no evidence that our patient was exposed to these risk factors.
In fact, most CCA cases like the one presented in the current study
arise de novo (12).
Clinical management of these cases is challenging
and requires a multimodality approach. While surgical resection is
an optimal treatment approach, many patients are not candidates as
the disease is often diagnosed at an advanced stage given that
diagnostic symptoms like night sweats, malaise, jaundice, abdominal
pain and cachexia are not uniquely informative (15). Another compounding factor is the
possibility of metastatic spread to the hepatic vasculature,
regional lymph nodes, lung, bones (especially vertebrae), adrenal
system and brain.
According to the 8th edition of the Union for
International Cancer Control-American Joint Committee on Cancer
(UICC-AJCC) classification there are two divisions of extrahepatic
cholangiocarcinoma-distal and perihilar. For distal extrahepatic
CCA, tumor depth invasion, number of lymph node metastases,
perineural, microscopic vascular invasion, R0 resection and
pancreatic invasion are reported to be predictors of long term
survival (16–23). A single positive bile duct resection
margin is usually correlated with increased risk of recurrence and
poor prognosis, as is a positive lymph node (24,25). A
recent study that examined 27 patients with distal bile duct cancer
who underwent pancreatoduodenectomy with extended lymphadenectomy
identified that factors for improved survival included up to two
positive nodes, negative resection margins, and clinical
administration of postoperative adjuvant chemotherapy (21).
Generally the prognosis for CCA is poor with 5-year
survival of 5–10%, and a median survival of 3–6 months if
unresectable (13,26). Post surgery survival time depends on a
thorough resection with negative resection margins. It is well
established that recurrences occur in 60–80% of patients within two
years after the initial surgery (27). In the present case, given that the
regional lymph nodes were positive our challenge was deciding how
far to resect. We had to weigh the probability of local vs. distant
recurrence and the morbidity and potential mortality of trying to
gain a R0 proximal margin. It was ultimately decided that the
probability of distant recurrence outweighed that of local
recurrence.
Adjuvant therapy is often considered as part of the
clinical management for post operative CCA where there are positive
margins given the high rate of recurrence in these circumstances
(28). Studies have reported survival
benefits for chemoradiotherapy with incompletely resected tumors
(3,29). A recent study looking at
chemoradiation with 5-fluorouracil (5-FU) and external beam
irradiation reported improved survival for distal tumors
particularly in patients with histologically positive resection
(30,31). It has been reported that
gemcitabine-based approaches have better survival outcomes than
5-FU and should be considered as part of the clinical intervention
(13). A recent report demonstrated
that a low bilirubin level <10 mg/dl and chemotherapy
administration are independent predictors associated with better
survival (32).
Despite the genetic heterogeneity of CCA,
perturbation of the RAS-MAPK pathway has been increasingly viewed
as a potential signature genetic aberration in CCA (33–37). In
Trinidad and Tobago, CCA provides an opportunity to integrate
epidemiological data, genomics, and novel clinical approaches to
better screen and treat CCA cases (38). One such schema integrates diagnostic
tests, and identification of targetable cancer driver pathways
leading to personalized targeted therapy (33,34).
In conclusion, the present case demonstrates clearly
that intra-operative assessment of margins in resection of CCA are
paramount. Aggressive surgical resection followed by adjuvant
therapy shows a definitive survival advantage. This case presented
challenges given the difficulties to obtain a correct preoperative
diagnosis, and to achieve R0 margins. Further studies are required
to identify modalities to better diagnose and clinically intervene
in these cases.
Acknowledgements
The authors of the present study appreciate the
contributions of the Department of Pathology, Eric Williams Medical
Sciences Complex, Trinidad and the assistance of Krishna Vyas,
Washington University, St. Louis, USA with figure preparation. WAW
was supported by Washington University School of Medicine-St. Louis
(grant no., GSAS/CGFP Fund 94028C).
References
|
1
|
Steiner PE: Carcinoma of the liver in the
United States. Acta Unio Int Contra Cancrum. 13:628–645.
1957.PubMed/NCBI
|
|
2
|
Esposito I and Schirmacher P: Pathological
aspects of cholangiocarcinoma. HPB (Oxford). 10:83–86. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nakeeb A, Pitt HA, Sohn TA, Coleman J,
Abrams RA, Piantadosi S, Hruban RH, Lillemoe KD, Yeo CJ and Cameron
JL: Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and
distal tumors. Ann Surg. 224:463–475. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Klöppel G, Adsay V, Konukiewitz B, Kleeff
J, Schlitter AM and Esposito I: Precancerous lesions of the biliary
tree. Best Pract Res Clin Gastroenterol. 27:285–297. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nuzzo G, Giuliante F, Ardito F, Giovannini
I, Aldrighetti L, Belli G, Bresadola F, Calise F, Valle R Dalla,
D'Amico DF, et al: Improvement in perioperative and long-term
outcome after surgical treatment of hilar cholangiocarcinoma:
Results of an Italian multicenter analysis of 440 patients. Arch
Surg. 147:26–34. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yamamoto M and Ariizumi S: Surgical
outcomes of intrahepatic cholangiocarcinoma. Surg Today.
41:896–902. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rizvi S and Gores GJ: Pathogenesis,
diagnosis, and management of cholangiocarcinoma. Gastroenterology.
145:1215–1229. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khan SA, Davidson BR, Goldin RD, Heaton N,
Karani J, Pereira SP, Rosenberg WM, Tait P, Taylor-Robinson SD,
Thillainayagam AV, et al: Guidelines for the diagnosis and
treatment of cholangiocarcinoma: An update. Gut. 61:1657–1669.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Parkin DM, Ohshima H, Srivatanakul P and
Vatanasapt V: Cholangiocarcinoma: Epidemiology, mechanisms of
carcinogenesis and prevention. Cancer Epidemiol Biomarkers Prev.
2:537–544. 1993.PubMed/NCBI
|
|
10
|
Chung YE, Kim MJ, Park YN, Choi JY, Pyo
JY, Kim YC, Cho HJ, Kim KA and Choi SY: Varying appearances of
cholangiocarcinoma: Radiologic-pathologic correlation.
Radiographics. 29:683–700. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Welzel TM, Graubard BI, El-Serag HB, Shaib
YH, Hsing AW, Davila JA and McGlynn KA: Risk factors for
intrahepatic and extrahepatic cholangiocarcinoma in the United
States: A population-based case-control study. Clin Gastroenterol
Hepatol. 5:1221–1228. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lazaridis KN and Gores GJ:
Cholangiocarcinoma. Gastroenterology. 128:1655–1667. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Reddy SB and Patel T: Current approaches
to the diagnosis and treatment of cholangiocarcinoma. Curr
Gastroenterol Rep. 8:30–37. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shaib YH, El-Serag HB, Davila JA, Morgan R
and McGlynn KA: Risk factors of intrahepatic cholangiocarcinoma in
the United States: A case-control study. Gastroenterology.
128:620–626. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
El Rassi ZE, Partensky C, Scoazec JY,
Henry L, Lombard-Bohas C and Maddern G: Peripheral
cholangiocarcinoma: Presentation, diagnosis, pathology and
management. Eur J Surg Oncol. 25:375–380. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ito K, Ito H, Allen PJ, Gonen M, Klimstra
D, D'Angelica MI, Fong Y, DeMatteo RP, Brennan MF, Blumgart LH and
Jarnagin WR: Adequate lymph node assessment for extrahepatic bile
duct adenocarcinoma. Ann Surg. 251:675–681. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hong SM, Pawlik TM, Cho H, Aggarwal B,
Goggins M, Hruban RH and Anders RA: Depth of tumor invasion better
predicts prognosis than the current American joint committee on
cancer T classification for distal bile duct carcinoma. Surgery.
146:250–257. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yoshida T, Matsumoto T, Sasaki A, Morii Y,
Shibata K, Ishio T and Kitano S: Lymphatic spread differs according
to tumor location in extrahepatic bile duct cancer.
Hepatogastroenterology. 50:17–20. 2003.PubMed/NCBI
|
|
19
|
Ebata T, Nagino M, Nishio H, Igami T,
Yokoyama Y and Nimura Y: Pancreatic and duodenal invasion in distal
bile duct cancer: Paradox in the tumor classification of the
American joint committee on cancer. World J Surg. 31:2008–2015.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Murakami Y, Uemura K, Hayashidani Y, Sudo
T, Ohge H and Sueda T: Pancreatoduodenectomy for distal
cholangiocarcinoma: Prognostic impact of lymph node metastasis.
World J Surg. 31:337–344. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoshida T, Matsumoto T, Sasaki A, Morii Y,
Aramaki M and Kitano S: Prognostic factors after
pancreatoduodenectomy with extended lymphadenectomy for distal bile
duct cancer. Arch Surg. 137:69–73. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Murakami Y, Uemura K, Hayashidani Y, Sudo
T, Hashimoto Y, Ohge H and Sueda T: Prognostic significance of
lymph node metastasis and surgical margin status for distal
cholangiocarcinoma. J Surg Oncol. 95:207–212. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Woo SM, Ryu JK, Lee SH, Yoo JW, Park JK,
Kim YT, Jang JY, Kim SW, Kang GH and Yoon YB: Recurrence and
prognostic factors of ampullary carcinoma after radical resection:
Comparison with distal extrahepatic cholangiocarcinoma. Ann Surg
Oncol. 14:3195–3201. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sasaki R, Takeda Y, Funato O, Nitta H,
Kawamura H, Uesugi N, Sugai T, Wakabayashi G and Ohkohchi N:
Significance of ductal margin status in patients undergoing
surgical resection for extrahepatic cholangiocarcinoma. World J
Surg. 31:1788–1796. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kitagawa Y, Nagino M, Kamiya J, Uesaka K,
Sano T, Yamamoto H, Hayakawa N and Nimura Y: Lymph node metastasis
from hilar cholangiocarcinoma: Audit of 110 patients who underwent
regional and paraaortic node dissection. Ann Surg. 233:385–392.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Jarnagin WR, Fong Y, DeMatteo RP, Gonen M,
Burke EC, Bodniewicz BSJ, Youssef BAM, Klimstra D and Blumgart LH:
Staging, resectability, and outcome in 225 patients with hilar
cholangiocarcinoma. Ann Surg. 234:507–519. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Soares KC, Kamel I, Cosgrove DP, Herman JM
and Pawlik TM: Hilar cholangiocarcinoma: Diagnosis, treatment
options, and management. Hepatobiliary Surg Nutr. 3:18–34.
2014.PubMed/NCBI
|
|
28
|
Brandi G, Venturi M, Pantaleo MA and
Ercolani G: GICO: Cholangiocarcinoma: Current opinion on clinical
practice diagnostic and therapeutic algorithms: A review of the
literature and a long-standing experience of a referral center. Dig
Liver Dis. 48:231–241. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Serafini FM, Sachs D, Bloomston M, Carey
LC, Karl RC, Murr MM and Rosemurgy AS: Location, not staging, of
cholangiocarcinoma determines the role for adjuvant chemoradiation
therapy. Am Surg. 67:839–844. 2001.PubMed/NCBI
|
|
30
|
Anderson CD, Pinson CW, Berlin J and Chari
RS: Diagnosis and treatment of cholangiocarcinoma. Oncologist.
9:43–57. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Pitt HA, Nakeeb A, Abrams RA, Coleman J,
Piantadosi S, Yeo CJ, Lillemore KD and Cameron JL: Perihilar
cholangiocarcinoma. Postoperative radiotherapy does not improve
survival. Ann Surg. 221:788–798. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Farhat MH, Shamseddine AI, Tawil AN,
Berjawi G, Sidani C, Shamseddeen W and Barada KA: Prognostic
factors in patients with advanced cholangiocarcinoma: Role of
surgery, chemotherapy and body mass index. World J Gastroenterol.
14:3224–3230. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Razumilava N and Gores GJ:
Cholangiocarcinoma. Lancet. 383:2168–2179. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Geynisman DM and Catenacci DV: Toward
personalized treatment of advanced biliary tract cancers. Discov
Med. 14:41–57. 2012.PubMed/NCBI
|
|
35
|
Han W and Lo HW: Landscape of EGFR
signaling network in human cancers: Biology and therapeutic
response in relation to receptor subcellular locations. Cancer
Lett. 318:124–134. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Andersen JB, Spee B, Blechacz BR, Avital
I, Komuta M, Barbour A, Conner EA, Gillen MC, Roskams T, Roberts
LR, et al: Genomic and genetic characterization of
cholangiocarcinoma identifies therapeutic targets for tyrosine
kinase inhibitors. Gastroenterology. 142:1021–1031.e15. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Brandi G, Farioli A, Astolfi A, Biasco G
and Tavolari S: Genetic heterogeneity in cholangiocarcinoma: A
major challenge for targeted therapies. Oncotarget. 6:14744–14753.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Roach A, Warner WA and Llanos AA: Building
capacity for human genetics and genomics research in Trinidad and
Tobago. Rev Panam Salud Publica. 38:425–430. 2015.PubMed/NCBI
|