Introduction
Malignant spinal cord tumors make up ~22% of all
primary spinal cord tumors (1).
Intramedullary spinal cord tumors are the rarest of these neoplasms
and can severely impair the neurological function and quality of
life of patients (2). Therefore, the
accurate and early diagnosis of these tumors is essential to obtain
an optimal outcome. Diagnosis is based on contrast-enhanced
magnetic resonance imaging (MRI) of the spine, which is considered
the diagnostic method of choice, enabling excellent delineation of
the spinal cord and adjacent structures (3). However, diagnosis in patients with
spinal cord diseases may be challenging, particularly in patients
with a suspected malignant spinal cord disease, which requires
biopsy for definitive diagnosis; this is because spinal cord
surgery carries the risk of irreversible neurological deficits
(4,5).
New imaging techniques that help to provide
additional justification for spinal cord biopsy/surgery are
desperately required. With improved spatial resolution of positron
emission tomography (PET) techniques, PET using the tracer
18F-fluorodeoxyglucose (18F-FDG) has been
explored in small series to assess neoplastic spinal cord lesions
(6,7).
18FDG-PET, however, does not allow the reliable
differentiation between neoplastic and inflammatory lesions
(8). Thus, new imaging techniques are
necessary to achieve this differentiation.
18F-fluoroethyl-L-tyrosine
(18F-FET) PET may particularly lend itself for this
purpose because of its potential for differentiating between
neoplastic and inflammatory lesions (9,10). In this
regard, it has been shown to be a promising tool for the detection
of pseudoprogression in glioblastoma patients (11), and for the identification of patients
with radiation necrosis in brain metastases (12). The current study presents the first
case of 18F-FET PET imaging in a patient with a
malignant tumor of the spinal cord.
Case report
A 74-year-old male presented at the Department of
Neurology, University of Bonn Medical Center on April 28, 2014 with
a progressive symmetric distal numbness and dysesthesia of the
legs. The patient reported no associated back pain or weight loss,
and no pre-existing neoplastic disease. Due to a disconnected
electrode wire in his implanted cardiac defibrillator, the patient
was unsuitable for MRI.
A contrast-enhanced computed tomography (CT) scan of
the whole spine, and a CT scan with myelogram did not show any
evidence of a tumor mass or spinal cord or root compression. A CT
scan of the brain was also unremarkable. Cerebral spinal fluid
analysis, an infectious disease screening (including human
immunodeficiency virus, Epstein-Barr virus, varicella-zoster virus,
cytomegalovirus and herpes simplex virus screening), onconeural
antibodies and full blood analysis did not reveal any relevant
pathological findings. Staging with contrast-enhanced CT scan of
neck/chest/abdomen, as well as fundoscopic and skin evaluations did
not show an extraspinal tumor. Despite the use of corticosteroids,
symptoms progressed to paraplegia with an ankle clonus and
pathological Babinski's sign on the left side. 18F-FDG
PET revealed a pathologically accumulating intramedullary lesion,
indicating elevated focal glucose metabolism at the 12th thoracic
vertebra (Th12). Considering that the 18F-FDG PET had
insufficient ability to differentiate between inflammatory and
neoplastic lesions, an additional 18F-FET PET was
performed to aid in ruling out an inflammatory lesion; preclinical
data have previously indicated no significant accumulation of
18F-FET in inflammatory spinal cord lesions, as opposed
to 18F-FDG (13).
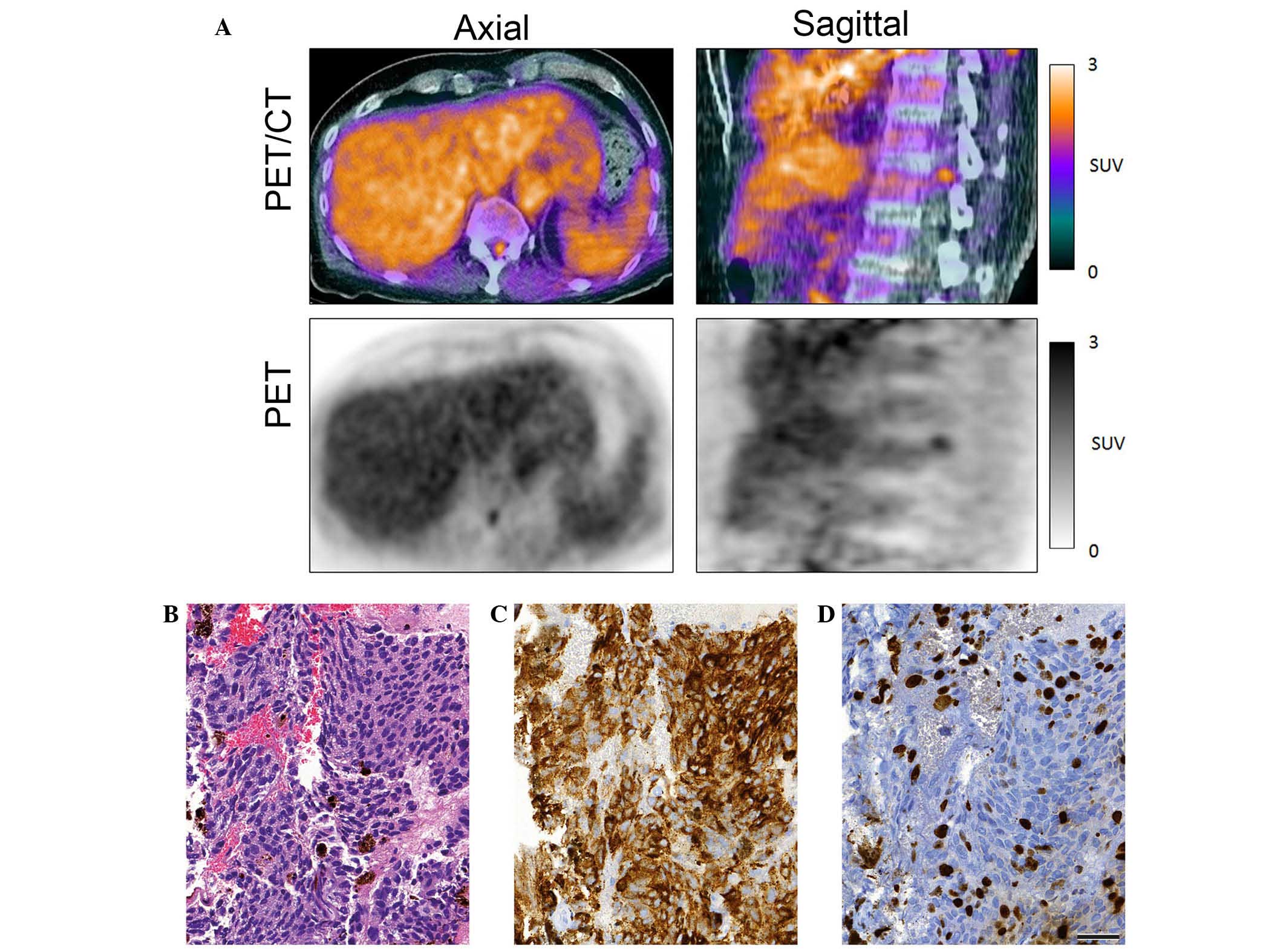
18F-FET PET confirmed focal tracer
accumulation at Th12, indicating a high-grade malignancy of the
spinal cord (Fig. 1A). The ratio of
the maximal standardized uptake value (SUV) of the tumor to the SUV
of the surrounding normal tissue, which is referred to as the
tumor-to-normal tissue ratio (TNR), was 2.21. The mean TNR was
1.82. Based on these findings, the patient underwent a diagnostic
biopsy. Intraoperative localization of the tumor area was performed
under the guidance of 18F-FET PET data. The biopsy
material was fixed with formaldehyde overnight, embedded in
paraffin, cut into 4-µm sections and mounted on slides. The
neuropathological analysis involved immunostaining with mouse
anti-Ki67 (cat. no. M70240; 1:1,000; Dako Denmark A/S, Glastrop,
Denmark) and anti-melanosome (HMB45) monoclonal antibodies (cat.
no. M0634; 1:100; Dako Denmark A/S). Histological analysis revealed
a melanocytic tumor with high proliferative activity and
cellularity, compatible with malignant melanoma (Fig. 1B-D).
After stereotactic irradiation of the spinal cord
(at the Th12 level) with 42.65 Gy in 16 fractions, the patient's
clinical status improved gradually over a period of 6 months until
he was able to walk a few steps independently. The patient is
currently alive at 2-years following a spinal cord tumor diagnosis.
Written informed consent was obtained from the patient prior to the
publication of this study.
Discussion
To the best of our knowledge, this is the first
report of the utilization of 18F-FET PET imaging in a
patient with a malignant spinal cord tumor. 18F-FET PET
in this patient was shown to provide valuable information to
differentiate between inflammatory and neoplastic lesions of the
spinal cord and to warrant surgery/biopsy in such eloquent
areas.
These findings are in accordance with the findings
in brain tumors, where a growing body of evidence supports the role
of 18F-FET PET imaging in discerning between neoplastic
tumors and inflammatory lesions and/or post-treatment effects
(12,14). If MRI is contraindicated,
18F-FET PET and 18F-FDG PET resolution in
conjunction with CT imaging may be sufficient to map a spinal cord
biopsy site. However, as has been demonstrated in preclinical
studies, 18F-FDG has inferior capability in
distinguishing neoplastic from inflammatory or treatment-related
lesions as opposed to an amino-acid PET tracer (13,15).
18F-FET, a commonly used radiolabeled amino acid, is
characterized by a long half-life and is thus suitable for
widespread clinical usage (16).
However, despite its promising properties, 18F-FET PET
has not yet gained a foothold in imaging of suspected spinal cord
neoplasms.
The current study is the first case demonstrating
the metabolic phenotype of a malignant melanoma of the spinal cord,
as detected by 18F-FET PET. The intense metabolic
activity is likely what makes this tumor amenable to
18F-FET PET imaging. Based on the findings of the
presented case, 18F-FET PET imaging should be explored
further in malignant spinal cord disease and melanoma.
In summary, this is the first report of 18F-FET PET
imaging in a patient with a malignant spinal cord tumor. 18F-FET
PET in this patient was shown to provide valuable information to
differentiate between inflammatory and neoplastic lesions of the
spinal cord and to warrant surgery/biopsy in eloquent spinal cord
areas. This is the first case demonstrating the metabolic phenotype
of a malignant melanoma of the spinal cord, as detected by 18F-FET
PET. In patients unable or unsuited to have an MRI, in whom a
spinal cord tumor is suspected, 18F-FET PET provides valuable
information to determine whether a tumor is likely to be malignant.
In this scenario, 18F-FET PET may assist in deciding whether a
patient should be subjected to biopsy/resection.
References
|
1
|
Duong LM, McCarthy BJ, McLendon RE,
Dolecek TA, Kruchko C, Douglas LL and Ajani UA: Descriptive
epidemiology of malignant and nonmalignant primary spinal cord,
spinal meninges, and cauda equina tumors, United States, 2004–2007.
Cancer. 118:4220–4227. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chamberlain MC and Tredway TL: Adult
primary intradural spinal cord tumors: A review. Curr Neurol
Neurosci Rep. 11:320–328. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sevick RJ and Wallace CJ: MR imaging of
neoplasms of the lumbar spine. Magn Reson Imaging Clin N Am.
7539–553. (ix)1999.PubMed/NCBI
|
|
4
|
Ando M, Tamaki T, Yoshida M, Kawakami M,
Kubota S, Nakagawa Y, Iwasaki H, Tsutsui S and Yamada H:
Intraoperative spinal cord monitoring using combined motor and
sensory evoked potentials recorded from the spinal cord during
surgery for intramedullary spinal cord tumor. Clin Neurol
Neurosurg. 133:18–23. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Farrokh D, Fransen P and Faverly D: MR
findings of a primary intramedullary malignant melanoma: Case
report and literature review. AJNR Am J Neuroradiol. 22:1864–1866.
2001.PubMed/NCBI
|
|
6
|
Sandu N, Pöpperl G, Toubert ME, Spiriev T,
Arasho B, Orabi M and Schaller B: Current molecular imaging of
spinal tumors in clinical practice. Mol Med. 17:308–316. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tomura N, Ito Y, Matsuoka H, Saginoya T,
Numazawa SI, Mizuno Y and Watanabe K: PET findings of
intramedullary tumors of the spinal cord using [18F] FDG and [11C]
methionine. AJNR Am J Neuroradiol. 34:1278–1283. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Belohlávek O, Simonová G, Kantorová I,
Novotný J Jr and Liscák R: Brain metastases after stereotactic
radiosurgery using the Leksell gamma knife: Can FDG PET help to
differentiate radionecrosis from tumour progression? Eur J Nucl Med
Mol Imaging. 30:96–100. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pauleit D, Floeth F, Hamacher K,
Riemenschneider MJ, Reifenberger G, Müller HW, Zilles K, Coenen HH
and Langen KJ: O-(2-[18F]fluoroethyl)-L-tyrosine PET combined with
MRI improves the diagnostic assessment of cerebral gliomas. Brain.
128:678–687. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kebir S, Gaertner FC, Mueller M, Nelles M,
Simon M, Schäfer N, Suplich M, Schaub C, Niessen M, Mack F, et al:
18F-fluoroethyl-L-tyrosine positron emission tomography
for the differential diagnosis of tumefactive multiple sclerosis
versus glioma: A case report. Oncol Lett. 11:2195–2198.
2016.PubMed/NCBI
|
|
11
|
Kebir S, Fimmers R, Galldiks N, Schäfer N,
Mack F, Schaub C, Stuplich M, Niessen M, T Simon M Tzaridis, et al:
Late Pseudoprogression in Glioblastoma: Diagnostic Value of Dynamic
O-(2-[18F]fluoroethyl)-L-Tyrosine PET. Clin Cancer Res.
22:2190–2196. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Galldiks N, Stoffels G, Filss CP, Piroth
MD, Sabel M, Ruge MI, Herzog H, Shah NJ, Fink GR, Coenen HH and
Langen KJ: Role of O-(2-(18)F-fluoroethyl)-L-tyrosine PET for
differentiation of local recurrent brain metastasis from radiation
necrosis. J Nucl Med. 53:1367–1374. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Buck D, Forschler A, Lapa C, Schuster T,
Vollmar P, Korn T, Nessler S, Stadelmann C, Drzezga A, Buck AK, et
al: 18F-FDG PET detects inflammatory infiltrates in spinal cord
experimental autoimmune encephalomyelitis lesions. J Nucl Med.
53:1269–1276. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Galldiks N, Dunkl V, Stoffels G, Hutterer
M, Rapp M, Sabel M, Reifenberger G, Kebir S, Dorn F, Blau T, et al:
Diagnosis of pseudoprogression in patients with glioblastoma using
O-(2-[(18)F]fluoroethyl)-L-tyrosine PET. Eur J Nucl Med Mol
Imaging. 42:685–695. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rau FC, Weber WA, Wester HJ, Herz M,
Becker I, Krüger A, Schwaiger M and Senekowitsch-Schmidtke R:
O-(2-[(18)F]Fluoroethyl)-L-tyrosine (FET): A tracer for
differentiation of tumour from inflammation in murine lymph nodes.
Eur J Nucl Med Mol Imaging. 29:1039–1046. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Floeth FW, Sabel M, Stoffels G, Pauleit D,
Hamacher K, Steiger HJ and Langen KJ: Prognostic value of
18F-fluoroethyl-L-tyrosine PET and MRI in small nonspecific
incidental brain lesions. J Nucl Med. 49:730–737. 2008. View Article : Google Scholar : PubMed/NCBI
|