Introduction
The results of Pap tests performed during routine
screenings at the beginning of prenatal care are abnormal in 8–12%
of cases (1). Overall, the prevalence
of abnormal cervical cytology in pregnancy is similar to that of
age-matched, non-pregnant women (2).
The incidence of cervical intraepithelial neoplasia (CIN) in
pregnancy varies among different patient populations, as it does in
non-pregnant women, but when age-matched, the risk of CIN is not
higher than that among women who are not pregnant, ranging between
3.4 and 10.0% (3). The management of
pregnant women with abnormal cytology depends on the degree of
cytological abnormality, the outcome of colposcopy, and, when
necessary, directed biopsy. Since, the only diagnosis that may
alter management in pregnancy is invasive cancer, the management of
pregnant women with abnormal cervical cytology or biopsy-proven CIN
is generally more conservative compared with management of similar
cytology and histology in non-pregnant women. However, management
guidelines for cervical dysplasia are not well defined and are
based on data collected from non-pregnant women, the opinion of
experts, anecdotal experiences or retrospective series of pregnant
women.
Previous studies show a varying postpartum
regression rate of CIN of 12–97% and a persistence/progression rate
of 2–60%; however, there are no definitive data or evidence-based
guidelines available for cervical dysplasia diagnosed in pregnancy
(4–8).
Functional biomarkers, such as Ki-67, p16, p53 and cytokeratin
13/14, have proven useful in the prediction of regressing and
non-regressing CIN2-3 lesions. Ki-67 is a non-histone protein that
exists as two isoforms encoded by cDNA sequences of 11.5 and 12.5
kb organized over 15 exons and localized on chromosome 10 (9). Its expression is applied to assess the
growth fraction of a cell population (10). p16 is a cellular protein encoded by a
gene on chromosome 9p21. In cervical cancer, p16 expression is
correlated with increased expression of oncogenic E6/E7 human
papilloma virus (HPV) mRNA (11,12).
Based on the aforementioned data, the present study
evaluated Ki-67 and p16 immunostaining in CIN lesions diagnosed in
pregnancy compared with those diagnosed in non-pregnant women. The
aim was to identify any differences in order to better understand
the behavior of CIN in pregnancy.
Patients and methods
Patients
The present retrospective case-control study
included 17 pregnant patients with first-time onset of CIN that
were consecutively referred to the affiliated outpatient services
of the Lower Genital Tract Disease at the Woman's Health Sciences
Department, Gynecologic Section of the Woman's Health Sciences
Department, Marche Polytechnic University (Ancona, Italy) and the
Gynecological Oncology Unit, Department of Surgical Oncology,
Oncologic Referral Centre, National Cancer Institute (Pordenone,
Italy) between January 2010 and December 2010. The inclusion
criteria were as follows: i) First diagnosis of CIN occurred prior
to the 16th gestational week and ii) pregnancies were not obtained
by assisted reproductive technologies. Exclusion criteria included:
i) Previous cervical treatment (not only for HPV-associated
disease); ii) immunocompromised status; iii) chronic hepatitis B
and/or C; and iv) cigarette smoking.
The control group included 17 non-pregnant patients
with first-time onset of CIN that were consecutively referred to
the same institutes during the same study period, and matched for
age, parity and number of previous sexual partners. The control
group also complied with the same exclusion criteria.
Ethics statement
The present study was designed as a basic scientific
research study and, therefore, did not require approval from a
Research Ethics Committee. Approval was obtained from the Ethics
Committee of Marche Polytechnic University in order to routinely
collect data. Written informed consent for the use of personal data
was obtained from each patient.
Immunohistochemistry
Following colposcopy, punch cervical biopsies were
obtained from the transformation zone and fixed in 10% buffered
formaldehyde (Diapath S.P.A., Martinengo, Italy), embedded in
paraffin (AppliChem GmbH, Darmstadt, Germany), sectioned to a
thickness of 5–6 µm and stained with hematoxylin-eosin (Bio-Optica
S.P.A., Milano, Italy) for routine histological examination.
The sections were dewaxed in xylene (Carlo Erba
Reagents, Val-de-Reuil, France) and rehydrated through a graded
series of ethanol (Carlo Erba Reagents). The p16 mouse monoclonal
antibody (clone E6H4; ready-to-use) was included in the
CINtec® Histology kit (catalog no. 9517; Ventana Medical
Systems, Inc., Heidelberg, Germany), which was used according to
the manufacturer's protocol.
The Ki-67 mouse monoclonal antibody (clone MIB-1;
catalog no. M7240; Dako, Golstrup, Denmark) was used at a 1:80
dilution in Antibody Diluent (Dako). Briefly, to better enhance
antigenic sites, a low pH Dako Target Retrieval solution (catalog
no. K8005) was applied, by incubating sections in a Dako PT-Link
autostainer at 750 Kw for 20 min.
Endogenous peroxidase activity was quenched by
incubating the sections in 3% (v/v) hydrogen peroxide (Dako) for 7
min at room temperature. Tissue sections were incubated with the
anti-Ki-67 monoclonal antibody for 60 min. The antigen-antibody
complex was subsequently detected using the Dako EnVision™
Detection System, Peroxidase/DAB (catalog no. K801021; Dako).
Sections were counterstained with Mayer's haematoxylin (Bio-Optica
S.P.A.) and cover-slipped with Eukitt (Bio-Optica S.P.A.).
All histological specimens with stained with
hematoxylin-eosin were initially examined by a pathologist to
assess the grade of CIN (CIN1/2/3), using a Nikon Eclipse E800
light microscope (Nikon Italia, Firenze, Italy). The evaluation of
p16 and Ki-67 positive cells on cervical biopsy sections was
performed by light microscopy at appropriate magnifications.
Immunoreactivity for the antibody was evaluated by two observers
and experiments were repeated three times; discordant results were
reconsidered in a consensus review. The cells considered positive
exhibited nuclear and/or cytoplasmic staining for p16 and nuclear
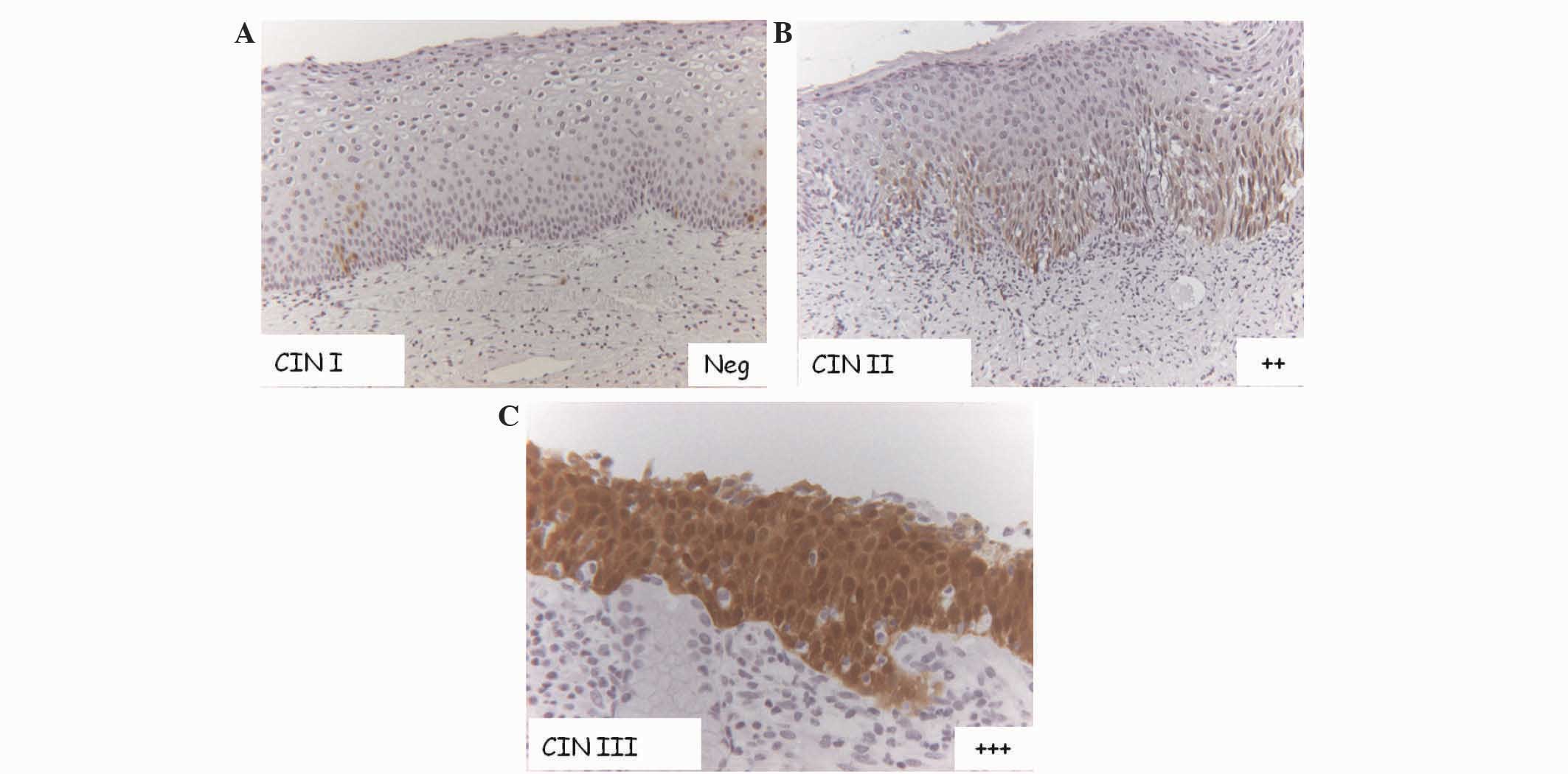
staining for Ki-67. Immunoreactivity was evaluated using a
semi-quantitative three point-scale system, as it follows: i) -/+,
if there was a complete lack of immunostaining or if positivity was
confined to the lower third of the squamous epithelium; ii) ++, if
positivity was confined to less than two thirds of the squamous
epithelium; iii) +++, if reactivity was observed in all epithelial
levels, regardless of the staining intensity (Fig.1).
Statistical analysis
Data were analyzed using STATA software (version 11;
StataCorp LP, College Station, TX, USA). Fisher's exact test was
used to assess the association between categorical variables.
Experiments were performed twice. P<0.05 was considered to
indicate a statistically significant difference.
Results
Characteristics of the population
Of the 34 patients involved in the present study, 4
were classified as CIN1 (25% of cases; 75% of controls), 13 as CIN2
(70% of cases; 30% of controls) and 17 as CIN3 (35% of cases; 75%
of controls). There were no statistically significant differences
in CIN grade distribution between pregnant and not-pregnant
patients. The mean age of the women was the same in both groups
(mean ± standard deviation, 34.6±4.8 years). Cases and controls
were also comparable for parity, smoking status and number of
previous sexual partners (data not shown). p16 and Ki-67 expression
in the cervical biopsies and their association with CIN grade in
the entire study population were evaluated (Tables I and II).
 | Table I.Correlation between p16 expression and
CIN grade in the total study population (P=0.008). |
Table I.
Correlation between p16 expression and
CIN grade in the total study population (P=0.008).
|
| Patients, n (%) |
|---|
|
|
|
|---|
| p16 expression | CIN1 | CIN2 | CIN3 |
|---|
| −/+ | 4 (100.0) | 2 (15.4) | 3 (17.6) |
| ++ | 0 (0.0) | 6 (46.1) | 3 (17.6) |
| +++ | 0 (0.0) | 5 (38.5) | 11 (64.8) |
| Total | 4 (100.0) | 13 (100.0) | 17 (100.0) |
| Table II.Correlation between Ki-67 expression
and CIN grade in the total study population (P<0.001). |
Table II.
Correlation between Ki-67 expression
and CIN grade in the total study population (P<0.001).
|
| Patients, n (%) |
|---|
|
|
|
|---|
| Ki-67 expression | CIN1 | CIN2 | CIN3 |
|---|
| −/+ | 4 (100.0) | 3 (23.1) | 0 (0.0) |
| ++ | 0 (0.0) | 7 (53.8) | 8 (47.1) |
| +++ | 0 (0.0) | 3 (23.1) | 9 (52.9) |
| Total | 4 (100.0) | 13 (100.0) | 17 (100.0) |
p16 expression
By analyzing p16 immunoreactivity, negative staining
or positive staining confined at the lower third of the squamous
epithelium (−/+) was observed in 9 patients. Diffuse positive
staining was observed in significantly more CIN2/3 samples than
CIN1 samples (P=0.008). In particular, a complete lack of
immunostaining or positivity confined to the lower third of the
squamous epithelium (−/+) was observed in 100.0% (4/4) of CIN1,
15.4% (2/13) of CIN2 and 17.6% (3/17) of CIN3 samples; positivity
confined to less than two thirds of the squamous epithelium (++)
was observed in 0.0% (0/4) of CIN1, 46.1% (6/13) of CIN2 and 17.6%
(3/17) of CIN3 samples; and diffuse positivity in all epithelial
levels (+++) was observed in 0.0% (0/4) of CIN1, 38.5% (5/13) of
CIN2 and 64.8% (11/17) of CIN3 samples (Table I). In CIN3, diffuse positivity for p16
(+++) was observed in 72.7% of non-pregnant women, but only in
50.0% of pregnant women. Positivity for Ki-67 was confined at the
lower third of the epithelium or complete absent (−/+) in 100%
(4/4) of CIN1, 23.1% (3/13) of CIN2 and 0% (0/17) of CIN3;
positivity confined to less than two thirds of the epithelium (++)
was observed in 0% (0/0) of CIN1, 53.8% (7/13) of CIN2 and 47.1%
(8/17) of CIN3; and diffuse positive immunostaining (+++) was
observed in 0% (0/4) of CIN1, 23.1% (3/13) of CIN2 and 52.9% (9/17)
of CIN3 (Table II). Statistical
analysis revealed that the association between p16 immunostaining
and CIN grade was significant in non-pregnant patients (P=0.003)
but not in pregnant patients (P=0.344) (Table III).
| Table III.Correlation between p16 expression
and CIN grade in pregnant (cases) (P=0.344) and in non-pregnant
(controls) (P=0.003) women. |
Table III.
Correlation between p16 expression
and CIN grade in pregnant (cases) (P=0.344) and in non-pregnant
(controls) (P=0.003) women.
|
| CIN1, n (%) | CIN2, n (%) | CIN3, n (%) |
|---|
|
|
|
|
|
|---|
| p16 expression | Cases | Controls | Cases | Controls | Cases | Controls |
|---|
| −/+ | 1 (100.0) | 3 (100.0) | 2 (20.0) | 0 (0.0) | 0 (0.0) | 3 (27.3) |
| ++ | 0 (0.0) | 0 (0.0) | 4 (40.0) | 2 (66.7) | 3 (50.0) | 0 (0.0) |
| +++ | 0 (0.0) | 0 (0.0) | 4 (40.0) | 1 (33.3) | 3 (50.0) | 8 (72.7) |
| Total | 1 (100.0) | 3 (100.0) | 10 (100.0) | 3 (100.0) | 6 (100.0) | 11 (100.0) |
Ki-67 expression
Positivity for Ki-67 was less intense in pregnant
patients than in non-pregnant patients. Ki-67 was expressed in all
epithelial levels in 16.7% of pregnant patients with CIN3 compared
with 72.7% of non-pregnant patients with CIN3 (Table IV). Ki-67 immunostaining was
significantly associated with CIN grade in non-pregnant patients
(P=0.003) but not in pregnant patients (P=0.236).
| Table IV.Correlation between Ki-67 expression
and CIN grade in pregnant (cases) (P=0.236) and non-pregnant
(controls) (P=0.003) women. |
Table IV.
Correlation between Ki-67 expression
and CIN grade in pregnant (cases) (P=0.236) and non-pregnant
(controls) (P=0.003) women.
|
| CIN1, n (%) | CIN2, n (%) | CIN3, n (%) |
|---|
|
|
|
|
|
|---|
| Ki-67
expression | Cases | Controls | Cases | Controls | Cases | Controls |
|---|
| −/+ | 1 (100.0) | 3 (100.0) | 3 (30.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| ++ | 0 (0.0) | 0 (0.0) | 5 (50.0) | 2 (66.7) | 5 (83.3) | 3 (27.3) |
| +++ | 0 (0.0) | 0 (0.0) | 2 (20.0) | 1 (33.3) | 1 (16.7) | 8 (72.7) |
| Total | 1 (100.0) | 3 (100.0) | 10 (100.0) | 3 (100.0) | 6 (100.0) | 11 (100.0) |
Association between p16 and Ki-67
immunoreactivity
The expression of the two biomarkers was compared,
revealing an association with the CIN grade (P=0.002) in the total
patient cohort. The association between Ki-67 and p16 expression
persisted when the analysis was narrowed exclusively to pregnant
women (P=0.019) (Table V), but not in
non-pregnant women (data not shown).
| Table V.Correlation between p16 and Ki-67
expression in pregnant women (P=0.019). |
Table V.
Correlation between p16 and Ki-67
expression in pregnant women (P=0.019).
|
| Ki-67 expression,
n |
|---|
|
|
|
|---|
| p16 expression,
n | −/+ | ++ | +++ |
|---|
| −/+ | 3 | 0 | 0 |
| ++ | 0 | 6 | 1 |
| +++ | 1 | 4 | 2 |
Discussion
Few clinical studies have been performed concerning
cervical intraepithelial lesions during pregnancy and data
regarding the influence of pregnancy on the natural history of CIN
are discordant. However, the risk of progression of CIN2/3 to
invasive cervical cancer during pregnancy appears to be minimal
(4–8)
however, the rate of spontaneous regression post-partum is
relatively high. Spontaneous regression is reported in 12–97% of
cases, while persistence in the severity of CIN is reported in
25–47% of cases (13–15). Based on this data, it is established
that patients with any grade of CIN in pregnancy should be
conservatively managed after an invasive disease has been excluded
(16). However, this topic continues
to have a great clinical relevance, as premalignant lesions are
typically diagnosed in the fertile age range and cervical cancer is
the most commonly occurring malignancy during pregnancy, with an
incidence of 1.2–4.5 per 10,000 women (17).
In the present study, p16 and Ki-67 immunostaining
was analyzed in patients diagnosed with CIN lesions during
pregnancy compared with those diagnosed in non-pregnant women. The
results showed an increased variability in the expression of these
biomarkers in pregnant patients.
p16 and Ki-67 were selected for analysis in the
present study, as they are two biomarkers with available
standardized, commercial assays and have been most commonly
evaluated in clinical studies. Overexpression of p16 and Ki-67 have
proven to be useful indicators of clinically significant infections
and lesion severity in numerous studies (11,18,19);
several properties of p16 and Ki-67 enable them to be promising
biomarkers for HPV-associated cancer, since they are associated
with histological grade and infection for HR-HPV (17). In addition, p16 immunostaining appears
to be a useful adjunctive test in the examination of
colposcopically-directed cervical biopsies and in the diagnostic
cascade of women investigated for abnormal Papanicolaou smears, due
to its capacity to reveal the integration of high-risk HPV DNA into
the host cell genome (20).
p16 is a cellular correlate of increased expression
of oncogenic E6/E7 HPV mRNA (21–25). Its
expression is directly associated with the action of the HPV
oncogene, as continuous expression of E7 is necessary to maintain a
malignant phenotype in HPV-associated cancer (26). Several studies have shown that
positive p16 immunostaining is significantly associated with CIN2/3
or carcinoma (27–34). Although varying efficacy of p16
immunostaining in CIN2-3 or carcinoma has been reported, the
majority of studies have reported that p16 immunostaining has a
high sensitivity to CIN2/3 or carcinoma (range, 82–100%),
supporting the hypothesis that p16 is a suitable biomarker for
CIN2/3 (35). Klaes et al
identified p16 expression in 60% of CIN1 cases, while 40% had no
expression or only focal expression (25). In a study by Benevolo et al,
none of the normal cervical tissues analyzed exhibited p16 positive
staining, whereas a constant and significant increase in protein
overexpression was observed in CIN1 (30%), CIN2 (90%), CIN3 (100%)
and carcinoma (100%) tissues (36).
More recently, p16 was evaluated as a prognostic marker of
progression and regression in series of prospectively recruited
patients with CIN1, suggesting that a negative result for p16 may
exclude the possibility of progression during follow-up (37).
The Ki-67 protein is a human nuclear antigen
strictly associated with cell proliferation. It is present during
all active phases of the cell cycle (G1, S, G2 and mitosis) but is
absent in resting cells (G0); therefore, it is used to determine
the growth fraction of a given cell population. The fraction of
Ki-67-positive tumor cells (the Ki-67 labeling index) is commonly
correlated with the clinical course of the disease. Previous
studies have shown an association between Ki-67 expression and
lesion severity or growth rate, and demonstrated the use of Ki-67
expression in the analysis of vulvar and vaginal lesions caused by
HPV (38,39). Therefore, the determination of Ki-67
expression appears to be a relevant complementary examination in
the detection and distinction of different lesion grades of the
uterine cervix.
Data obtained in the present study revealed that p16
and Ki-67 staining occur in a less deep section of the CIN squamous
epithelium in pregnant patients than in non-pregnant patients. In
contrast to the consistent positive staining for p16 and Ki-67 in
non-pregnant women with CIN2/3, CIN2/3 lesions typically exhibited
markedly more variable staining in pregnant women. Similarly, the
correlation between p16/Ki-67 expression and the severity of CIN
was significant in non-pregnant women but not in pregnant women,
where increased p16 and Ki-67 staining according to CIN grade was
proportionally lower. These results indicate that the pregnancy
status of a patient interferes with the expression of cellular
proteins involved in cell-cycle regulation and the carcinogenic
process induced by high-risk HPV, with increased variability in
staining observed in pregnant women. Although it is not known
whether this immunohistochemical variability in p16 and Ki-67
staining is also able to provide information on the evolution of
CIN lesions in pregnancy, it is important to identify a suitable
interpretation for the aforementioned phenomenon. A possible
mechanism is associated with changes in the hormonal status during
gestation. p16 and Ki-67 staining may depend on altered
transcriptional regulation of the viral E6/E7 oncogenes, which
affect almost all the cellular pathways involved in HPV-associated
carcinogenesis. Thus, the modulation of p16 and Ki-67 expression
may be attributed to increased levels of progesterone, the
essential hormone for pregnancy. In fact, progesterone influences
the gene expression levels of proteases, transcription factors,
cell-adhesion molecules, modulators of vascular activities and
regulators of inflammation (40).
Furthermore, modulation of the individual immune system performed
according to the pregnancy status may have a significant influence
on the balance of early oncogenic status.
The present study is important for a number of
reasons. To the best of our knowledge, it is the first study to
evaluate p16 and Ki-67 expression in pregnant women. Furthermore,
it was performed over a short period of time at affiliated medical
centers, to ensure the samples were homogeneous, and by two
colposcopists highly experienced in evaluating lesions in
pregnancy. However, the present study did not consider additional
factors possibly associated with the evolution of CIN during
pregnancy, such as co-infections other than HPV, including
Chlamydia trachomatis, herpes simplex virus and
cytomegalovirus. Another limitation of the study is the small
sample size.
In conclusion, the findings concerning p16 and Ki-67
expression suggest that pregnant patients may exhibit a less
aggressive biological behavior of cervical dysplasia than
non-pregnant patients. Further clinical studies should be performed
to support these findings and apply them to a ‘watchful waiting’
strategy for the management of cervical dysplasia during pregnancy.
From a scientific point of view, the results of the present study
encourage further research to identify other biomarkers to aid in
better understanding the clinical evolution of CIN during
pregnancy, and the influence of the hormonal gestational pattern
and the immune system on the natural history of HPV infection.
References
|
1
|
Wu YM, Wang T, He Y, Song F, Wang Y, Zhu
L, Kong WM, Duan W and Zhang WY: Clinical management of cervical
intraepithelial neoplasia in pregnant and postpartum women. Arch
Gynecol Obstet. 289:1071–1077. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Saslow D, Solomon D, Lawson HW, Killackey
M, Kulasingam SL, Cain J, Garcia FA, Moriarty AT, Waxman AG, Wilbur
DC, et al: American Cancer Society; American Society for Colposcopy
and Cervical Pathology; American Society for Clinical Pathology:
American Cancer Society, American Society for Colposcopy and
Cervical Pathology, and American Society for Clinical Pathology
screening guidelines for the prevention and early detection of
cervical cancer. Am J Clin Pathol. 137:516–542. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fader AN, Alward EK, Niederhauser A,
Chirico C, Lesnock JL, Zwiesler DJ, Guido RS, Lofgren DJ, Gold MA
and Moore KN: Cervical dysplasia in pregnancy: A
multi-institutional evaluation. Am J Obstet Gynecol. 203:113.e1–e6.
2010. View Article : Google Scholar
|
|
4
|
Insinga RP, Glass AG and Rush BB:
Diagnoses and outcomes in cervical cancer screening: A
population-based study. Am J Obstet Gynecol. 191:105–113. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Morimura Y, Fujimori K, Soeda S, Hashimoto
T, Takano Y, Yamada H, Yanagida K and Sato A: Cervical cytology
during pregnancy-comparison with non-pregnant women and management
of pregnant women with abnormal cytology. Fukushima J Med Sci.
48:27–37. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Douvier S, Filipuzzi L and Sagot P:
Management of cervical intra-epithelial neoplasm during pregnancy.
Gynecol Obstet Fertil. 31:851–855. 2003.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Frega A, Scirpa P, Corosu R, Verrico M,
Scarciglia ML, Primieri MR, Palazzo A, Iacovelli R and Moscarini M:
Clinical management and follow-up of squamous intraepithelial
cervical lesions during pregnancy and postpartum. Anticancer Res.
27:2743–2746. 2007.PubMed/NCBI
|
|
8
|
Wright TC Jr, Massad LS, Dunton CJ,
Spitzer M, Wilkinson EJ and Solomon D: 2006 ASCCP-Sponsored
Consensus Conference: 2006 consensus guidelines for the management
of women with abnormal cervical cancer screening tests. J Low Genit
Tract Dis. 11:201–222. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Duchrow M, Schlüter C, Key G, Kubbutat MH,
Wohlenberg C, Flad HD and Gerdes J: Cell proliferation-associated
nuclear antigen defined by antibody Ki-67: A new kind of cell
cycle-maintaining proteins. Arch Immunol Ther Exp (Warsz).
43:117–121. 1995.PubMed/NCBI
|
|
10
|
Scholzen T and Gerdes J: The Ki-67
protein: From the known and the unknown. J Cell Physiol.
182:311–322. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tornesello ML, Buonaguro L, Rossi P Giorgi
and Buonaguro FM: Viral and cellular biomarkers in the diagnosis of
cervical Intraepithelial neoplasia and cancer. Biomed Res Int.
2013:5196192013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
von Knebel Doeberitz M: New molecular
tools for efficient screening of cervical cancer. Dis Markers.
17:123–128. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Palle C, Bangsbøll S and Andreasson B:
Cervical intraepithelial neoplasia in pregnancy. Acta Obstet
Gynecol Scand. 79:306–310. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Vlahos G, Rodolakis A, Diakomanolis E,
Stefanidis K, Haidopoulos D, Abela K, Georgountzos V and Michalas
S: Conservative management of cervical intraepithelial neoplasia
(CIN (2–3)) in pregnant women. Gynecol Obstet Invest. 54:78–81.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yost NP, Santoso JT, Mcintire DD and Iliya
FA: Postpartum regression rates of antepartum cervical
intraepithelial neoplasia II and III lesions. Obstet Gynecol.
93:359–362. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sorosky JI: Cervical carcinoma
complicating pregnancy. Postgrad Obstet Gynecol. 15:1–6. 1995.
|
|
17
|
Kaplan KJ, Dainty LA, Dolinsky B, Rose GS,
Carlson J, McHale M and Elkas JC: Prognosis and recurrence risk for
patients with cervical squamous intraepithelial lesions diagnosed
during pregnancy. Cancer. 102:228–232. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zappacosta R, Colasante A, Viola P,
D'Antuono T, Lattanzio G, Capanna S, Gatta DM and Rosini S:
Chromogenic in situ hybridization and p16/Ki67 dual staining on
formalin-fixed paraffin-embedded cervical specimens: Correlation
with HPV-DNA test, E6/E7 mRNA test, and potential clinical
apllications. Biomed Res Int. 2013:4536062013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Carozzi F, Confortini M, Palma P Dalla,
Del Mistro A, Gillio-Tos A, De Marco L, Giorgi-Rossi P, Pontenani
G, Rosso S, Sani C, et al: Use of p16-INK4A overexpression to
increase the specificity of human papillomavirus testing: A nested
substudy of the NTCC randomised controlled trial. Lancet Oncol.
9:937–945. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dray M, Russell P, Dalrymple C, Wallman N,
Angus G, Leong A, Carter J and Cheerala B: p16(INK4a) as a
complementary marker of high-grade intraepithelial lesions of the
uterine cervix. I: Experience with squamous lesions in 189
consecutive cervical biopsies. Pathology. 37:112–124. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mantovani F and Banks L: The human
papillomavirus E6 protein and its contribution to malignant
progression. Oncogene. 20:7874–7887. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Munger K, Basile JR, Duensing S, Eichten
A, Gonzalez SL, Grace M and Zacny VL: Biological activities and
molecular targets of the human papillomavirus E7 oncoprotein.
Oncogene. 20:7888–7898. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Khleif SN, DeGregori J, Yee CL, Otterson
GA, Kaye FJ, Nevins JR and Howley PM: Inhibition of cyclin
D-CDK4/CDK6 activity is associated with an E2F-mediated induction
of cyclin kinase inhibitor activity. Proc Natl Acad Sci USA.
93:4350–4354. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sano T, Oyama T, Kashiwabara K, Fukuda T
and Nakajima T: Expression status of p16 protein is associated with
human papillomavirus oncogenic potential in cervical and genital
lesions. Am J Pathol. 153:1741–1748. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Klaes R, Friedrich T, Spitkovsky D, Ridder
R, Rudy W, Petry U, Dallenbach-Hellweg G, Schmidt D and von Knebel
Doeberitz M: Overexpression of p16(INK4A) as a specific marker for
dysplastic and neoplastic epithelial cells of the cervix uteri. Int
J Cancer. 92:276–284. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
von Knebel Doeberitz M, Rittmüller C, zur
Hausen H and Dürst M: Inhibition of tumorigenicity of cervical
cancer cells in nude mice by HPV E6-E7 anti-sense RNA. Int J
Cancer. 51:831–834. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kong CS, Balzer BL, Troxell ML, Patterson
BK and Longacre TA: p16INK4A immunohistochemistry is superior to
HPV in situ hybridization for the detection of high-risk HPV in
atypical squamous metaplasia. Am J Surg Pathol. 31:33–43. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Walts AE and Bose S: p16, Ki-67 and BD
ProExC immunostaining: A practical approach for diagnosis of
cervical intraepithelial neoplasia. Hum Pathol. 40:957–964. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Pinto AP, Schlecht NF, Woo TY, Crum CP and
Cibas ES: Biomarker (ProEx C, p16INK4A, and MiB-1) distinction of
high-grade squamous intraepithelial lesion from its mimics. Mod
Pathol. 21:1067–1074. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Badr RE, Walts AE, Chung F and Bose S: BD
ProEx C: A sensitive and specific marker of HPV-associated squamous
lesions of the cervix. Am J Surg Pathol. 32:899–906. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shi J, Liu H, Wilkerson M, Huang Y,
Meschter S, Dupree W, Schuerch C and Lin F: Evaluation of p16INK4a,
minichromosome maintenance protein 2, DNA topoisomerase IIalpha,
ProEX C, and p16INK4a/ProEX C in cervical squamous intraepithelial
lesions. Hum Pathol. 38:1335–1344. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Branca M, Ciotti M, Santini D, Di Bonito
L, Giorgi C, Benedetto A, Paba P, Favalli C, Costa S, Agarossi A,
et al: p16(INK4A) expression is related to grade of CIN and
high-risk human papillomavirus but does not predict virus clearance
after conization or disease outcome. Int J Gynecol Pathol.
23:354–365. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Carreon JD, Sherman ME, Guillén D, Solomon
D, Herrero R, Jerónimo J, Wacholder S, Rodríguez AC, Morales J,
Hutchinson M, et al: CIN2 is a much less reproducible and less
valid diagnosis than CIN3: Results from a histological review of
population-based cervical samples. Int J Gynecol Pathol.
26:441–446. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Baak JP, Kruse AJ, Janssen E and van
Diermen B: Predictive testing of early CIN behaviour by molecular
biomarkers. Cell Oncol. 27:277–280. 2005.PubMed/NCBI
|
|
35
|
Roelens J, Reuschenbach M, von Knebel
Doeberitz M, Wentzensen N, Bergeron C and Arbyn M: p16INK4a
immunocytochemistry versus human papillomavirus testing for triage
of women with minor cytologic abnormalities: A systematic review
and meta-analysis. Cancer Cytopathol. 120:294–307. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Benevolo M, Terrenato I, Mottolese M,
Marandino F, Muti P, Carosi M, Rollo F, Ronchetti L, Mariani L,
Vocaturo G and Vocaturo A: Comparative evaluation of nm23 and p16
expression as biomarkers of high-risk human papillomavirus
infection and cervical intraepithelial neoplasia 2(+) lesions of
the uterine cervix. Histopathology. 57:580–586. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Pacchiarotti A, Ferrari F, Bellardini P,
Chini F, Collina G, Palma P Dalla, Ghiringhello B, Maccallini V,
Musolino F, Negri G, et al: Prognostic value of p16-INK4A protein
in women with negative or CIN1 histology result: A follow-up study.
Int J Cancer. 134:897–904. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sarian LO, Derchain SF, Yoshida A,
Vassallo J, Pignataro F and De Angelo Andrade LA: Expression of
cycloxygenase-2 (COX-2) and Ki67 as related to disease severity and
HPV detection in squamous lesions of the cervix. Gynecol Oncol.
102:537–541. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Calil LN, Edelweiss MI, Meurer L, Igansi
CN and Bozzetti MC: p16 INK4a and Ki67 expression in normal,
dysplastic and neoplastic uterine cervical epithelium and human
papillomavirus (HPV) infection. Pathol Res Pract. 210:482–487.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kim J, Bagchi IC and Bagchi MK: Control of
ovulation in mice by progesterone receptor-regulated gene networks.
Mol Hum Reprod. 15:821–828. 2009. View Article : Google Scholar : PubMed/NCBI
|