Introduction
Breast cancer is the most frequently diagnosed
cancer in women, with 425,000 new cases reported each year and an
annual mortality of 78,000 individuals in China (1). Despite the existence of a variety of
breast cancer treatments, including surgical resection, adjuvant
chemotherapy, radiotherapy, hormone therapy and targeted therapy,
breast cancer remains the second leading cause of cancer-associated
mortality in women worldwide (2). To
date, a number of molecules have been demonstrated to serve roles
in breast cancer progression and metastasis, and the discovery of
biomarkers, including HER2, has led to targeted treatment options
(3); however, the underlying
mechanisms of breast cancer development and progression remain
unclear. Therefore, the identification of novel breast cancer
biomarkers is required to improve the determination of cancer
prognosis and the development of treatments.
Human RNA helicases constitute an extended family of
enzymes that serve important roles in numerous aspects of RNA
metabolism, including splicing, transcription, translation and
degradation (4,5). DEAH-box polypeptide 32 (DHX32) is a
novel RNA helicase containing a unique helicase domain structure
and has been observed to be dysregulated in certain types of tumor
(6,7).
In addition, a number of other RNA helicases have been demonstrated
to be dysregulated in various types of cancer, although their exact
role in carcinogenesis remains to be completely elucidated
(8,9).
RNA helicases are involved in the regulation of multiple
cancer-associated molecules, including DEAD-box helicase 5 (DDX5)
(10), DDX17 (11) and DHX9 (12–14). Human
DHX32 exhibits widespread tissue distribution, including colon,
breast and lung tissue. In addition, the amino acid sequence of
human DHX32 is highly homologous to that of its murine counterpart,
with 84% identity and 90% similarity, indicating that it is an
evolutionally conserved and functionally important gene (15). A previous study demonstrated that
DHX32 is overexpressed in colorectal cancer (CRC) tissue samples
compared with adjacent wild-type tissue (7). In addition, DHX32 expression is
significantly associated with clinicopathological features of CRC,
which suggests that DHX32 may be used as a prognostic biomarker in
patients with CRC (7). A recent study
observed that DHX32 promotes the proliferation, migration and
invasion of CRC cells by activating the Wnt signaling pathway and
downregulating pro-apoptotic gene expression (16). This suggests that DHX32 expression is
associated with CRC development and progression (16). However, the exact role of DHX32 in
breast cancer remains unclear.
In the present study, the expression of DHX32 in
breast cancer and adjacent non-cancerous tissue samples was
investigated, demonstrating that DHX32 was markedly upregulated in
human breast cancer specimens. Furthermore, the association between
DHX32 expression and the clinicopathological features of patients
with breast cancer was examined to assess whether DHX32 is a
potential prognostic indicator in breast cancer.
Materials and methods
Patients and specimens
A total of 193 paraffin-embedded breast cancer
specimens were obtained from the Beijing Tiantan Hospital (Beijing,
China) between June 2007 and December 2009. In addition, a total of
40 pairs of freshly frozen breast cancer tissue samples and
adjacent normal mammary tissue samples were collected during
surgery at the Beijing Tiantan Hospital between May 2014 and
September 2014. All fresh samples were snap-frozen in liquid
nitrogen and stored at −80°C until required and none of the
patients received chemotherapy or radiotherapy prior to surgery.
Breast cancer diagnosis was confirmed by histological analysis of
tissue sections stained with hematoxylin and eosin, and complete
clinical data of the 193 breast cancer cases was obtained and
reviewed. Male breast cancer patients were excluded from the
present study. The clinical follow-up time was 60 months. The
overall survival time (OS) was calculated as the time between the
date of surgery and breast cancer-associated mortality. The
disease-free survival time (DFS) was calculated as the time between
the date of surgery and initial tumor progression, which was
indicative of initial recurrence of cancer. Table I presents the clinicopathological
characteristics of the 193 patients. The present study was approved
by the Ethics Committee of Beijing Tiantan Hospital (Beijing,
China) and written informed consent was obtained from all
subjects.
 | Table I.Clinicopathological characteristics of
193 patients with breast cancer. |
Table I.
Clinicopathological characteristics of
193 patients with breast cancer.
| Characteristic | Number of patients
(%) |
|---|
| Age (years) |
|
| ≤50 | 87 (45.1) |
| ≥50 | 106
(54.9) |
| Tumor size (cm) |
|
| ≤2 | 120
(62.2) |
| ≥2 | 73 (37.8) |
| Histological
grade |
|
| I–II | 114
(59.1) |
| III | 79 (40.9) |
| Clinical stage |
|
| I–II | 128
(66.3) |
|
III–IV | 65 (33.7) |
| Lymph node
metastasis |
|
|
Negative | 117
(60.6) |
|
Positive | 76 (39.4) |
| Estrogen receptor
status |
|
|
Negativeb | 85 (44.0) |
|
Positivec | 108
(56.0) |
| Progesterone receptor
status |
|
|
Negativeb | 74 (38.3) |
|
Positivec | 119
(61.7) |
| HER2 status |
|
|
Negativeb | 136
(70.5) |
|
Positivec | 57 (29.5) |
| Ki-67 expression |
|
|
Negativeb | 60 (31.1) |
|
Positivec | 133
(68.9) |
| Expression of
DHX32a |
|
| Low | 89 (46.1) |
| High | 104
(53.9) |
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR) analysis
DHX32 messenger (m)RNA expression in 40 pairs of
breast cancer and adjacent non-cancerous tissues was detected using
RT-qPCR. Total RNA was extracted using TRIzol® reagent
(Invitrogen; Thermo fisher Scientific, Inc., Waltham, MA, USA)
according to the manufacturer's protocol. RT-qPCR was performed
using a Thermal Cycler Dice Real Time System TP800 (Takara Bio,
Inc., Otsu, Japan) and the SYBR Premix ExTaq kit (Takara
Biotechnology Co., Ltd., Dalian, China) to detect DHX32 mRNA
expression, according to the manufacturer's protocol. GAPDH was
used as an internal control. The PCR primers for DHX32 and GAPDH
are shown in Table II. The
thermocycling conditions for RT-qPCR were as follows: 95°C for 30
sec; and 40 cycles of 95°C for 5 sec, 51°C for 20 sec and 72°C for
30 sec. Each reaction was performed in triplicate, and the mean
DHX32 mRNA level for each tumor sample was compared with its
adjacent non-cancerous tissue sample. The relative expression of
DHX32 was calculated using the 2−ΔΔCq method
(17) and normalized to GAPDH.
| Table II.Sequences of primers used in reverse
transcription- quantitative polymerase chain reaction analysis. |
Table II.
Sequences of primers used in reverse
transcription- quantitative polymerase chain reaction analysis.
| Primer | Sequence |
|---|
| DHX32 |
|
|
Forward |
5′-GCCTGTGAGGATTTGGAACT-3′ |
|
Reverse |
5′-GCTGGTAGTGGATGGAAAGACA-3′ |
| GAPDH |
|
Forward |
5′-CTATAAATTGAGCCCGCAGCC-3′ |
|
Reverse |
5′-GCGCCCAATACGACCAAATC-3′ |
Western blot analysis
A total of eight randomly selected fresh tissue
samples were lysed in protein lysis buffer containing 50 mmol/l
Tris-HCl (pH 7.4), 150 mmol/l NaCl, 1% NP-40, 0.1% SDS and a
protease inhibitor cocktail, followed by centrifugation (12,000 ×
g for 20 min at 4°C). Protein concentrations were determined
using a bicinchoninic acid protein quantitation kit (Applygen
Technologies, Inc., Beijing, China). A total of 50 µg each protein
sample was separated by SDS-PAGE on a 12% gel and transferred to a
polyvinylidene fluoride membrane. Following blocking in PBS with
Tween 20 add 5% skim milk powder for 1 h at room temperature, the
membrane was incubated with anti-DHX32 rabbit antibody (catalog no.
19808-1-AP; dilution, 1:500; Proteintech Group, Inc., Chicago, IL,
USA) at 4°C overnight. Following three washes in TBS plus Tween 20
buffer, the membranes were incubated with a horseradish peroxidase
(HRP)-conjugated anti-rabbit immunoglobulin G (IgG) secondary
antibody (catalog no., HS101-01; dilution, 1:2,000; Beijing
TransGen Biotech Co., Ltd., Beijing, China) for 1 h at room
temperature. Immunoreactive protein bands were visualized using an
enhanced chemiluminescence reagent (Applygen Technologies, Inc.).
β-actin was used as a loading control, and the membrane was
incubated with anti-β-actin mouse monoclonal antibody (catalog no.
HC201-01; dilution, 1:2,000; Beijing TransGen Biotech Co., Ltd.) at
4°C overnight. Upon washing, the membranes were incubated with an
HRP-conjugated anti-mouse IgG secondary antibody (catalog no.
HS201-01; dilution, 1:2,000; Beijing TransGen Biotech Co., Ltd.)
for 1 h at room temperature. Other steps were the same as
above.
Immunohistochemistry (IHC)
analysis
Paraffin-embedded sections from 193 clinical
specimens were deparaffinized in xylene and rehydrated in a
descending ethanol series. Heat-induced antigen retrieval was
performed in 0.01 M citrate buffer (pH 6.0) at 100°C for 10 min.
Endogenous peroxidase activity was inhibited by immersion in 0.3%
hydrogen peroxide for 10 min. To block the sections, 5% bovine
serum albumin (Beijing Solarbio Science & Technology Co., Ltd,
Beijing, China) in PBS was used for 1 h at room temperature. The
sections were next incubated with an anti-DHX32 rabbit monoclonal
antibody (catalog no. 19808-1-AP; dilution, 1:100; Proteintech
Group, Inc.) overnight at 4°C. Following washing with PBS, sections
were incubated with an HRP-labeled IgG secondary antibody (catalog
no., KIHC-1; Proteintech Group, Inc.) for 30 min at room
temperature. The immunoreactive products were visualized using the
3,3′-Diaminobenzidine Color Development kit (ZSGB Biotech, Beijing,
China). Following washing in water, sections were counterstained
with hematoxylin and dehydrated in an ascending series of methanol,
prior to being cleaned in xylene and mounted on a coverslip.
Negative controls were processed in parallel following the same
protocol, but substituting the primary antibody for PBS.
The stained tissue sections were examined by an
evaluator who was unaware of the clinicopathological features of
each sample. DHX32 protein expression was classified
semi-quantitatively according to the synthetic evaluation of the
quantity and intensity of positively stained cells, as described
below. The percentage of positively stained cells was grouped into
four grades: 0 points (0%), 1 point (1–10%), 2 points (10–50%) and
3 points (>50%). Staining intensity was segmented into four
ranks: 0 points (no staining), 1 point (weak staining), 2 points
(moderate staining) and 3 points (strong staining). The status of
DHX32 expression was determined by the total points from percentage
of positive cells and staining intensity, as low expression (0–3
points) or high expression (4–6 points).
Statistical analysis
All data were analyzed using SPSS software version
20.0 (IBM SPSS, Armonk, NY, USA). RT-qPCR results are presented as
the mean ± standard deviation. The difference in DHX32 mRNA
expression between breast cancer and adjacent non-cancerous tissue
samples was assessed using the Wilcoxon signed-rank test. Pearson's
χ2 test and Fisher's exact test were used to analyze the
association between DHX32 expression and clinicopathological
features of breast cancer. Survival data were evaluated using the
Kaplan-Meier estimator and log-rank test. Multivariate analysis was
performed using the Cox proportional hazards model. Univariate and
multivariate Cox proportional hazards regression analyses were
performed to evaluate the impact of DHX32 expression and other
clinicopathological factors on OS and DFS. P<0.05 was considered
to indicate a statistically significant difference.
Results
DHX32 expression is increased in
breast cancer
To identify the role of DHX32 expression in breast
cancer, RT-qPCR was performed to evaluate the mRNA expression in 40
pairs of breast cancer and adjacent normal mammary tissues, with
GAPDH serving as the internal control. Compared with adjacent
non-cancerous tissue, breast cancer tissue exhibited increased
DHX32 mRNA expression (P<0.001; Fig.
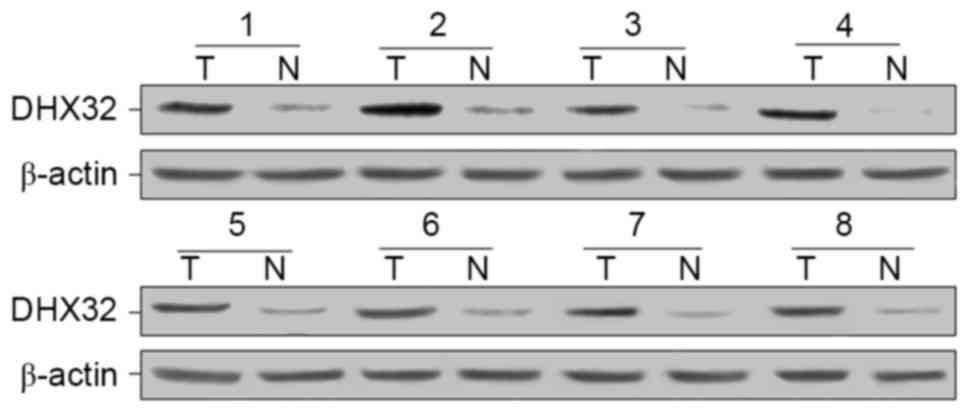
1). Furthermore, the DHX32 protein expression of eight randomly
selected breast cancer and adjacent non-cancerous tissue samples
was evaluated using western blotting. DHX32 was observed to be
overexpressed in the breast cancer tissue samples compared with the
non-cancerous tissue samples (Fig.
2). These results were consistent with the IHC analyses, which
demonstrated increased DHX32 expression in the breast cancer tissue
samples, localized primarily to the cytoplasm, compared with the
adjacent non-cancerous tissue samples (Fig. 3).
Association between DHX32 protein
expression and the clinicopathological characteristics of patients
with breast cancer
DHX32 protein expression was assessed in 193
archived paraffin-embedded breast cancer samples using IHC
staining. The 193 breast cancer patients were divided into two
groups: A low DHX32 expression group and a high DHX32 expression
group. DHX32 protein expression was then compared with the
clinicopathological characteristics of the patients. The
clinicopathological characteristics of all of the subjects are
indicated in Table I. As summarized
in Table III, high expression of
DHX32 was significantly associated with an increased clinical stage
(I–II vs. III–IV; P=0.006) and histological grade (I–II vs. III;
P=0.029), and a positive lymph node metastasis (positive vs.
negative; P<0.001) and Ki-67 expression (positive vs. negative;
P=0.004) status of the tumor, but was not associated with other
clinicopathological parameters.
| Table III.Correlation between DHX32 protein
expression and clinicopathological characteristics of patients with
breast cancer. |
Table III.
Correlation between DHX32 protein
expression and clinicopathological characteristics of patients with
breast cancer.
| Characteristic | Low DHX32
expressiona | High DHX32
expressiona | χ2 | P-value |
|---|
| Age (years) |
|
|
| 0.539 |
|
≤50 | 38 | 49 | 0.378 |
|
|
≥50 | 51 | 55 |
|
|
| Tumor size
(cm) |
|
|
| 0.275 |
| ≤2 | 59 | 61 | 1.190 |
|
| ≥2 | 30 | 43 |
|
|
| Histological
grade |
|
|
| 0.029b |
|
I–II | 60 | 54 | 4.761 |
|
|
III | 29 | 50 |
|
|
| Clinical stage |
|
|
| 0.006c |
|
I–II | 68 | 60 | 7.518 |
|
|
III–IV | 21 | 44 |
|
|
| Lymph node
metastasis |
|
|
|
<0.001c |
|
Negative | 69 | 48 | 19.776 |
|
|
Positive | 20 | 56 |
|
|
| Estrogen receptor
status |
|
|
| 0.815 |
|
Negatived | 40 | 45 | 0.055 |
|
|
Positivee | 49 | 59 |
|
|
| Progesterone
receptor status |
|
|
| 0.795 |
|
Negatived | 35 | 39 | 0.068 |
|
|
Positivee | 54 | 65 |
|
|
| HER-2 status |
|
|
| 0.344 |
|
Negatived | 65 | 71 | 0.897 |
|
|
Positivee | 23 | 34 |
|
|
| Ki-67
expression |
|
|
| 0.004c |
|
Negatived | 37 | 23 | 8.475 |
|
|
Positivee | 52 | 81 |
|
|
Prognostic significance of DHX32
expression in breast cancer
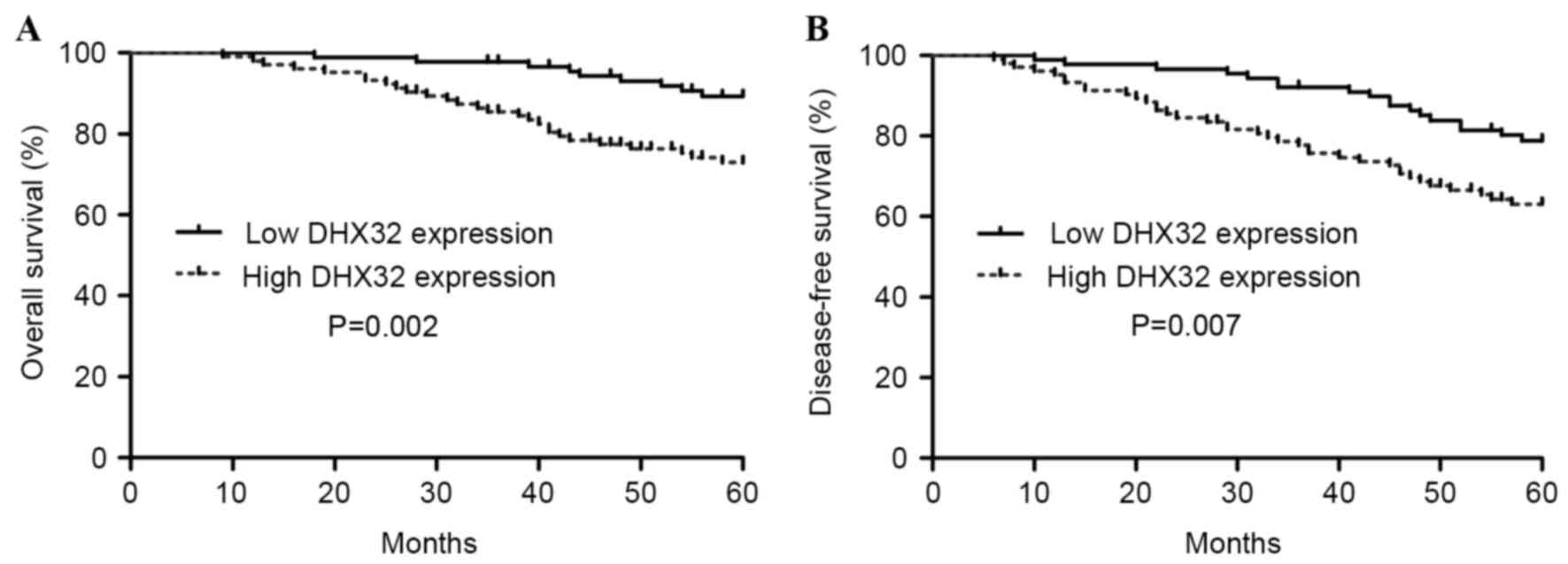
To investigate the prognostic significance of DHX32
in breast cancer, the effect of DHX32 protein expression on OS and
DFS in 193 samples from breast cancer patients was assessed using
the Kaplan-Meier estimator and the log-rank test. DHX32 protein
expression was observed to be associated with OS and DFS in
patients with breast cancer (Fig. 4).
Patients with a high expression of DHX32 exhibited significantly
decreased OS (P=0.002) and DFS (P=0.007) compared with patients
with a low DHX32 expression. To evaluate the impact of each
variable on OS and DFS, univariate and multivariate Cox
proportional hazard regression analyses were used to evaluate the
impact of breast cancer DHX32 protein expression and
clinicopathological parameters on the prognosis of patients
(Table IV). Univariate analysis
indicated that the significant factors associated with OS and DFS
included clinical stage, histological grade, lymph node metastasis,
erb-b2 receptor tyrosine kinase 2 (HER-2) status, Ki-67 expression
and DHX32 expression (all P<0.05; exact P-values shown in
Table IV). The multivariate analyses
indicated that DHX32 protein expression, clinical stage, lymph node
metastasis and HER-2 status are significant independent prognostic
factors for the OS and DFS of patients with breast cancer (all
P<0.05; exact P-values shown in Table
IV).
| Table IV.Univariate and multivariate Cox
proportional hazard regression analysis of overall survival and
disease-free survival in patients with breast cancer. |
Table IV.
Univariate and multivariate Cox
proportional hazard regression analysis of overall survival and
disease-free survival in patients with breast cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Overall
survival |
|
|
|
|
|
|
|
Age | 0.734 | 0.388–1.388 | 0.342 |
|
|
|
| Tumor
size | 1.388 | 0.734–2.624 | 0.313 |
|
|
|
|
Histological grade | 2.002 | 1.055–3.797 | 0.034a | 1.416 | 0.746–2.689 | 0.288 |
|
Clinical stage | 2.500 | 1.322–4.729 | 0.005b | 2.405 | 1.187–4.872 | 0.015a |
| Lymph
node metastasis | 3.715 | 1.899–7.266 |
<0.001b | 2.809 | 1.398–5.644 | 0.004b |
|
Estrogen receptor status | 1.288 | 0.672–2.469 | 0.446 |
|
|
|
|
Progesterone receptor
status | 1.587 | 0.787–3.200 | 0.196 |
|
|
|
| HER-2
status | 2.255 | 1.168–4.352 | 0.015a | 2.086 | 1.032–4.214 | 0.041a |
| Ki-67
expression | 2.256 | 1.059–4.807 | 0.035a | 1.512 | 0.658–3.478 | 0.330 |
| DHX32
Expression | 3.144 | 1.335–7.405 | 0.009b | 3.297 | 1.213–8.961 | 0.019a |
| Disease-free
survival |
|
|
|
|
|
|
|
Age | 0.787 | 0.439–1.412 | 0.422 |
|
|
|
| Tumor
size | 1.380 | 0.768–2.479 | 0.281 |
|
|
|
|
Histological grade | 1.824 | 1.016–3.276 | 0.044a | 1.360 | 0.676–2.737 | 0.389 |
|
Clinical stage | 2.427 | 1.254–4.698 | 0.008b | 2.151 | 1.116–4.143 | 0.022a |
| Lymph
node metastasis | 3.830 | 2.058–7.125 |
<0.001b | 2.712 | 1.478–4.976 | 0.001b |
|
Estrogen receptor status | 1.303 | 0.713–2.381 | 0.390 |
|
|
|
|
Progesterone receptor
status | 1.601 | 0.840–3.050 | 0.153 |
|
|
|
| HER-2
status | 2.346 | 1.310–4.202 | 0.004b | 2.055 | 1.130–3.738 | 0.018a |
| Ki-67
expression | 2.588 | 0.794–3.096 | 0.024a | 1.535 | 0.714–3.298 | 0.273 |
| DHX32
expression | 2.210 | 1.188–4.110 | 0.012a | 2.210 | 1.073–4.551 | 0.031a |
Discussion
Breast cancer is one of the most common cancers in
women worldwide. Although progress has been made in treatment
options for this disease, the morbidity and mortality rates
associated with breast cancer continue to increase in various
countries in South America, Africa and Asia (18). Therefore, in addition to the
established molecular markers, there is a requirement to identify
novel biomarkers and therapeutic targets. In the present study,
DHX32, a novel RNA helicase, was observed to be overexpressed in
breast cancer tissue samples compared with adjacent non-cancerous
tissue samples. In addition, the results of the present study
indicated that increased DHX32 expression in breast cancer is
significantly associated with an increased clinical stage and
histological grade, and a positive lymph node metastasis and Ki-67
expression status of the tumor. Furthermore, increased DHX32
expression in breast cancer cells was significantly associated with
decreased OS and FDS of the patients. These results indicate that
increased DHX32 expression is a prognostic marker in breast
cancer.
DHX32 was identified to be a novel RNA helicase
containing a unique helicase domain, though it shares similarity
with the DHX family of RNA helicases (4). RNA helicases are evolutionarily
conserved enzymes that regulate numerous aspects of RNA metabolism,
including transcription, splicing, translation and degradation
(19). Dysregulation of these
critical steps affects the ultimate expression of cellular proteins
and consequently determines cell fate (20). With a few exceptions, the biochemical
characteristics and functions of the majority of human RNA
helicases, including DHX32, have not been well characterized.
However, RNA helicase gene dysregulation, including downregulation,
upregulation and chromosomal translocation, has been observed in
various tumor types (9). DDX1 was
reported to be overexpressed in breast cancer and associated with
poor survival (21,22). Furthermore, DDX5 was reported to be
overexpressed in and to serve an important role in the
proliferation of breast cancer cells (23,24). In
addition, RNA helicases have been demonstrated to be involved in
the interaction and regulation of various cancer-associated
molecules (8–12). Therefore, increasing evidence
indicates that RNA helicases serve an important role in cancer
initiation and progression.
The widespread expression of DHX32, and the high
level of similarity between human and murine DHX32, suggests that
DHX32 is a functionally important gene (25). DHX32 was observed to be dysregulated
in lymphoid malignancies (6).
Furthermore, it was observed that DHX32 protein expression is
increased in CRC tissue compared with adjacent wild-type tissues
(7). DHX32 protein expression was
also significantly associated with cancer location, lymph node
metastasis, nodal status, differentiation grade and Dukes' stage
(7). A recent study by Lin et
al (16) indicated that DHX32
promotes the proliferation, migration and invasion of CRC cells,
which suggests that abnormal DHX32 expression is associated with
tumor development and progression. Meng et al (26) reported that DHX32 interacts with BRCA2
and CDKN1A interacting protein, which is the interacting protein
gene of the DNA repair-associated protein breast cancer 2 (BRCA2)
and cyclin-dependent kinase inhibitor 1A (CDKN1A). It has been
demonstrated that BRCA2 and CDKN1A serve important roles in breast
cancer development (27–29), which suggests that DHX32 is associated
with breast cancer progression. The results of the present study
indicated that the increased expression of DHX32 in breast cancer
is significantly associated with an increased clinical stage and
histological grade, and a positive lymph node metastasis and Ki-67
expression status, further suggesting that DHX32 serves a critical
role in human breast cancer development. Univariate and
multivariate analyses revealed that DHX32 may serve as an
independent prognostic factor in patients with breast cancer. To
the best of our knowledge, this is the first study that has
evaluated the association between DHX32 expression and breast
cancer prognosis. However, the exact function and underlying
mechanism of DHX32-mediated breast cancer progression remains
unclear.
In conclusion, the present study demonstrates that
DHX32 expression is associated with the development of breast
cancer. In addition, increased DHX32 expression was observed to be
associated with poor prognosis in breast cancer, suggesting that
DHX32 is a novel prognostic marker. However, large-scale studies
are required to verify the prognostic value of DHX32 in breast
cancer and further research into the tumor-regulatory mechanisms
associated with DHX32 is warranted.
Acknowledgements
The present study was supported by the Beijing
Natural Science Foundation (grant nos. 7154193 and 7142051), the
High Level Technical Talent Development Fund of the Beijing Health
System (grant no. 2013-3-052), and the National Key Technology
Research and Development Program of the Ministry of Science and
Technology of China (grant no. 2013BAI09B03).
References
|
1
|
Fan L, StrasserWeippl K, Li JJ, St Louis
J, Finkelstein DM, Yu KD, Chen WQ, Shao ZM and Goss PE: Breast
cancer in China. Lancet Oncol. 15:e279–e289. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kittaneh M, Montero AJ and Glück S:
Molecular profiling for breast cancer: A comprehensive review.
Biomark Cancer. 5:61–70. 2013.PubMed/NCBI
|
|
4
|
Abdelhaleem M, Maltais L and Wain H: The
human DDX and DHX gene families of putative RNA helicases.
Genomics. 81:618–622. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fuller-Pace FV: DExD/H box RNA helicases:
Multifunctional proteins with important roles in transcriptional
regulation. Nucleic Acids Res. 34:4206–4215. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Abdelhaleem M: The novel helicase
homologue DDX32 is down-regulated in acute lymphoblastic leukemia.
Leuk Res. 26:945–954. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang C, Liang X, Huang R and Zhang Z:
Up-regulation and clinical relevance of novel helicase homologue
DHX32 in colorectal cancer. J Exp Clin Cancer Res. 28:112009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Abdelhaleem M: Do human RNA helicases have
a role in cancer? Biochim Biophys Acta. 1704:37–46. 2004.PubMed/NCBI
|
|
9
|
Robert F and Pelletier J: Perturbations of
RNA helicases in cancer. Wiley Interdiscip Rev RNA. 4:333–349.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Guil S, Gattoni R, Carrascal M, Abiáán J,
Stévenin J and Bach-Elias M: Roles of hnRNP A1, SR proteins, and
p68 helicase in c-H-ras alternative splicing regulation. Mol Cell
Biol. 23:2927–2941. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hönig A, Auboeuf D, Parker MM, O'Malley BW
and Berget SM: Regulation of alternative splicing by the
ATP-dependent DEAD-box RNA helicase p72. Mol Cell Biol.
22:5698–5707. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Myöhänen S and Baylin SB:
Sequence-specific DNA binding activity of RNA helicase A to the
p16INK4a promoter. J Biol Chem. 276:1634–1642. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Anderson SF, Schlegel BP, Nakajima T,
Wolpin ES and Parvin JD: BRCA1 protein is linked to the RNA
polymerase II holoenzyme complex via RNA helicase A. Nat Genet.
19:254–256. 1998. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schlegel BP, Starita LM and Parvin JD:
Overexpression of a protein fragment of RNA helicase A causes
inhibition of endogenous BRCA1 function and defects in ploidy and
cytokinesis in mammary epithelial cells. Oncogene. 22:983–991.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Alli Z, Ho M, Ackerley C and Abdelhaleem
M: Characterization of murine Dhx32. Exp Mol Pathol. 83:115–118.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lin H, Liu W, Fang Z, Liang X, Li J, Bai
Y, Lin L, You H, Pei Y, Wang F and Zhang ZY: Overexpression of
DHX32 contributes to the growth and metastasis of colorectal
cancer. Sci Rep. 5:92472015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Torre LA, Bray F, Siegel RL, Ferlay J,
LortetTieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Abdelhaleem M: Helicases: An overview.
Methods Mol Biol. 587:1–12. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Abdelhaleem M: Over-expression of RNA
helicases in cancer. Anticancer Res. 24:3951–3953. 2004.PubMed/NCBI
|
|
21
|
Taunk NK, Goyal S, Wu H, Moran MS, Chen S
and Haffty BG: DEAD box 1 (DDX1) expression predicts for local
control and overall survival in early stage, node-negative breast
cancer. Cancer. 118:888–898. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Germain DR, Graham K, Glubrecht DD, Hugh
JC, Mackey JR and Godbout R: DEAD box 1: A novel and independent
prognostic marker for early recurrence in breast cancer. Breast
Cancer Res Treat. 127:53–63. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mazurek A, Luo W, Krasnitz A, Hicks J,
Powers RS and Stillman B: DDX5 regulates DNA replication and is
required for cell proliferation in a subset of breast cancer cells.
Cancer Discov. 2:812–825. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang D, Huang J and Hu Z: RNA helicase
DDX5 regulates microRNA expression and contributes to cytoskeletal
reorganization in basal breast cancer cells. Mol Cell Proteomics.
11:M111.011932. 2012. View Article : Google Scholar
|
|
25
|
Alli Z, Ackerley C, Chen Y, AlSaud B and
Abdelhaleem M: Nuclear and mitochondrial localization of the
putative RNA helicase DHX32. Exp Mol Pathol. 81:245–248. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Meng X, Liu J and Shen Z: Genomic
structure of the human BCCIP gene and its expression in cancer.
Gene. 302:139–146. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wooster R, Bignell G, Lancaster J, Swift
S, Seal S, Mangion J, Collins N, Gregory S, Gumbs C and Micklem G:
Identification of the breast cancer susceptibility gene BRCA2.
Nature. 378:789–792. 1995. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Xia W, Chen JS, Zhou X, Sun PR, Lee DF,
Liao Y, Zhou BP and Hung MC: Phosphorylation/cytoplasmic
localization of p21Cip1/WAF1 is associated with HER2/neu
overexpression and provides a novel combination predictor for poor
prognosis in breast cancer patients. Clin Cancer Res. 10:3815–3824.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dai M, AlOdaini AA, Arakelian A, Rabbani
SA, Ali S and Lebrun JJ: A novel function for p21Cip1 and
acetyltransferase p/CAF as critical transcriptional regulators of
TGFb-mediated breast cancer cell migration and invasion. Breast
Cancer Res. 14:R1272012. View
Article : Google Scholar : PubMed/NCBI
|