Introduction
Colorectal cancer is the third most common cancer
and one of the most frequent causes of cancer-associated mortality
worldwide (1). The main method of
treating it is by complete resection, however, metastatic
colorectal cancer (mCRC) cannot be treated by surgical resection
alone, and the prognosis of such patients is poor. Although there
have been substantial advances in mCRC treatment, the median
survival rate of patients with mCRC remains <3 years and <5%
of patients survive >5 years following disease onset (2–4).
The introduction of 5-fluorouracil (5-FU),
oxaliplatin and irinotecan (FOLFOX), as a therapeutic strategy has
improved mCRC treatment (3,5,6). The
addition of targeted therapies to conventional mCRC chemotherapy
regimens has improved treatment efficacy further. Cetuximab is a
chimeric human mouse monoclonal antibody of the immunoglobulin G1
(IgG1) subclass that targets the epidermal growth factor receptor
(EGFR). Cetuximab binds to human EGFR with high affinity and
inhibits the multiplication of various EGFR-positive cancer cell
lines in vitro in a concentration-dependent manner (6,7). Previous
studies have indicated that cetuximab is an effective treatment of
mCRC when administered either as monotherapy or in combination with
other chemotherapeutic agents (8,9).
Furthermore, two randomized clinical trials have demonstrated the
clinical efficacy of adding weekly cetuximab to irinotecan- or
oxaliplatin-based chemotherapy regimens to treat patients with mCRC
who do not exhibit the mutated KRAS proto-oncogene, GTPase (KRAS
wild-type mCRC) (10,11).
Cetuximab is approved in a number of countries for
clinical use in patients with KRAS wildtype mCRC. The current
dosing regimen of cetuximab, both as a monotherapy and in
combination with chemotherapy, consists of an initial intravenous
infusion of 400 mg/m2 with subsequent weekly doses of
250 mg/m2. Changing the cetuximab treatment schedule to
biweekly administration would improve convenience (12). These benefits would be even greater
for mCRC treatment regimens as the standard chemotherapy regimens
used in combination with cetuximab in KRAS wild-type mCRC; FOLFOX
(4 or 6), or irinotecan plus 5-FU infusion and leucovorin
(FOLFIRI), are already administered every two weeks. Moreover, the
synchronous administration of cetuximab and chemotherapy would
improve patient quality of life, as hospital visits would be less
frequent, and patients would not experience the unpleasant side
effects associated with chemotherapy treatment as often.
The present phase II study aimed to evaluate the
efficacy and safety of the biweekly administration of cetuximab in
combination with FOLFOX-6 as a first-line treatment of KRAS
wild-type mCRC. Changing to a biweekly regimen may be more
convenient and markedly improve patient quality of life.
Patients and methods
Study design
The present study was a multicenter, open-label,
prospective phase II study investigating the safety and efficacy of
cetuximab combined with FOLFOX as a first-line treatment of mCRC.
The study data and informed consent were obtained in accordance
with the Declaration of Helsinki, and the study protocol was
approved by the Ethics Review Board of each institution
involved.
Inclusion and exclusion criteria
Patients were eligible if they were ≥20 years of
age; had histologically confirmed, nonresectable, EGFR-expressing
mCRC with at least one radiologically measurable lesion; an Eastern
Cooperative Oncology Group performance status <1; and adequate
hepatic, renal, and bone marrow function (white blood cell count:
3,000–12,000/mm3, neutrophil count
≥1,500/mm3, platelet count ≥100,000/mm3,
aspartate aminotransferase and alanine aminotransferase ≤100 U/l,
total bilirubin <1.5 mg/dl, creatinine <1.5 mg/dl, and normal
electrocardiogram). Patients were ineligible if they had a history
of previous exposure to EGFR-targeted therapy, previous
chemotherapy for mCRC, or uncontrolled severe organ/metabolic
dysfunction.
Study treatment
Patients received a biweekly intravenous infusion of
cetuximab (500 mg/m2 on day 1) followed by FOLFOX-6 (2-h
oxaliplatin 85 mg/m2 infusion on day 1 in tandem with a
2-h leucovorin 200 mg/m2 infusion on days 1 and 2, and
5-FU as a 400 mg/m2 bolus followed by a 46-h 2,400
mg/m2 infusion on days 1–3). Cetuximab was administered
over 2 h in the first cycle, over 1.5 h in the second cycle and
over 1 h thereafter. Appropriate prophylactic medication was
administered before each cetuximab treatment to prevent acute
hypersensitivity reaction. Protocol dose modifications were
permitted in the event of predefined toxic effects related to
chemotherapy or cetuximab. In the event of unacceptable toxicity
due to 5-FU/leucovorin, oxaliplatin, or cetuximab, the trial was
discontinued, and the patient was transferred to an alternate
treatment regimen. However, protocol modifications did not allow
the maintenance of oxaliplatin as a monotherapy or in combination
with cetuximab. Treatment was continued until disease progression,
the onset of unacceptable toxic effects, patient/physician's
decision to discontinue, or surgery for metastases.
KRAS and BRAF mutations
DNA was extracted from formalin-fixed,
paraffin-embedded tumor tissues. Mutations of KRAS at codons 12,
13, and 61 and BRAF mutations at codon 600 were detected by direct
sequencing, as described previously (13,14).
Statistical analysis
The primary endpoint was the best overall response.
The response evaluation criteria in solid tumors (RECIST) 1.1
criteria were applied to assess and confirm overall response
(15). A radiological assessment of
the response was performed at the end of the fourth and sixth
cycles and then every six cycles until the end of the study. If
progressive disease (PD) had not been observed, the radiological
assessment was subsequently performed every 12 weeks, as per
routine clinical practice. Secondary endpoints were:
Progression-free survival (PFS), overall survival (OS), and the
safety of the combination therapy. Computed tomography or magnetic
resonance imaging were performed at baseline, every 8 weeks during
the first 6 months of the study, and every 12 weeks thereafter,
until disease progression. Adverse events were recorded throughout
the study period and were graded according to the Common Toxicity
Criteria of the National Cancer Institute ver. 3.0 (16).
All summary statistics on time-to-event variables
were calculated according to Kaplan-Meier methods. The 95%
confidence intervals (CI) for median time-to event and the
time-specific incidence rate were constructed using Greenwood's
formula, and Brookmeyer and Crowley's method, respectively. The PFS
of patients without disease progression before the end of the study
was calculated from the last on-study tumor assessment date at
which the patient was considered to be progression-free. PFS was
defined as the number of days between enrollment and the first
on-study assessment of PD; OS was defined as the number of days
between enrollment and any cause of death or the last follow-up.
Patients without disease progression who discontinued the study for
any reason were restricted to the last on-study tumor assessment
date.
A sample size of 55 patients was deemed as the
smallest sample size from which accurate conclusions could be
formed and was calculated to detect a 95% CI for the overall
response rate (ORR), with a half-width of 13%, assuming an
estimated rate of 60% calculated from previous studies. Therefore,
the target sample size was set at 60 patients, with an anticipated
10% patient loss to follow-up.
Results
Patient characteristics
From October 2011 to February 2013, 33 institutions
collaborated with the CELINE study, and 65 patients were registered
from 21 institutions. Five patients were excluded from the study:
Three patients had EGFR mutations, one patient had no information
regarding EGFR status, and one patient was unable to begin
treatment. In the end, 60 patients were deemed eligible for the
present study, and regarded as ready-to-treat. A safety analysis
was carried out on all patients following administration of ≥1 dose
of any component of the study treatment. Patient clinical
characteristics at baseline were documented and are presented in
Table I. The median age of the
patients was 64 years (range, 38–82 years). There were 34 patients
(56.7%) with metastatic lesions in one organ, and 26 patients
(43.3%) with metastatic lesions in >1 organ. Hepatic metastases
were the most common lesion, with such lesions detected in 50
patients (83.3%). The median duration of follow-up was 22.7
months.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | No. patients | Percentage of
patients (%) |
|---|
| Gender |
|
|
| Male | 47 | 78.3 |
|
Female | 13 | 21.7 |
| Age (years) |
|
|
|
Median | 64 | N/A |
|
Range | 38–82 | N/A |
| ECOG performance
status |
|
|
| 0 | 51 | 85.0 |
| 1 | 9 | 15.0 |
| Cancer location |
|
|
|
Colon | 30 | 50.0 |
|
Rectum | 30 | 50.0 |
| Previous adjuvant
therapy |
|
|
|
Chemotherapy | 4 | 6.7 |
| Non | 56 | 93.3 |
| Number of organs with
metastases |
|
|
| 1 | 34 | 56.7 |
| 2 | 14 | 23.3 |
| ≥3 | 12 | 20.0 |
Efficacy
Efficacy data are summarized in Table II. The best confirmed ORR was 70%
(95% CI, 56.8–81.2%; 2 complete and 40 partial responses).
Moreover, the best confirmed ORR was 72% in patients with hepatic
metastases (n=50, 95% CI, 57.5–83.8%), 73.3% in patients with lung
metastases (n=15, 95% CI, 44.9–92.2%), and 63.2% in patients with
lymphatic metastases (n=19, 95% CI, 38.4–83.7%); there were no
observable differences in the ORR between different metastatic
organs. There were 15 patients (25%) with stable disease, and
objective disease progression was observed in 1 patient. Therefore,
the disease control rate (DCR) was 95% (95% CI, 86.1–99.0%),
demonstrating treatment efficacy. In the 42 patients exhibiting
partial or complete response, the median time to onset of response
was 2.1 months.
| Table II.Efficacy data. |
Table II.
Efficacy data.
| Parameter | No. patients (%)
(n=60) | 95% confidence
interval |
|---|
| Best overall response
rate |
|
|
| Complete response
(CR) | 2 (3.3) |
|
| Partial response
(PR) | 40 (66.7) |
|
| Stable disease
(SD) | 16 (26.7) |
|
| Progressive disease
(PD) | 1 (1.7) |
|
| Not assessable | 1 (1.7) |
|
| Best overall
response rate (CR+PR) | 42 (70.0) | 56.8–81.2 |
| Disease control
rate (CR+PR+SD) | 58 (96.7) | 88.5–99.6 |
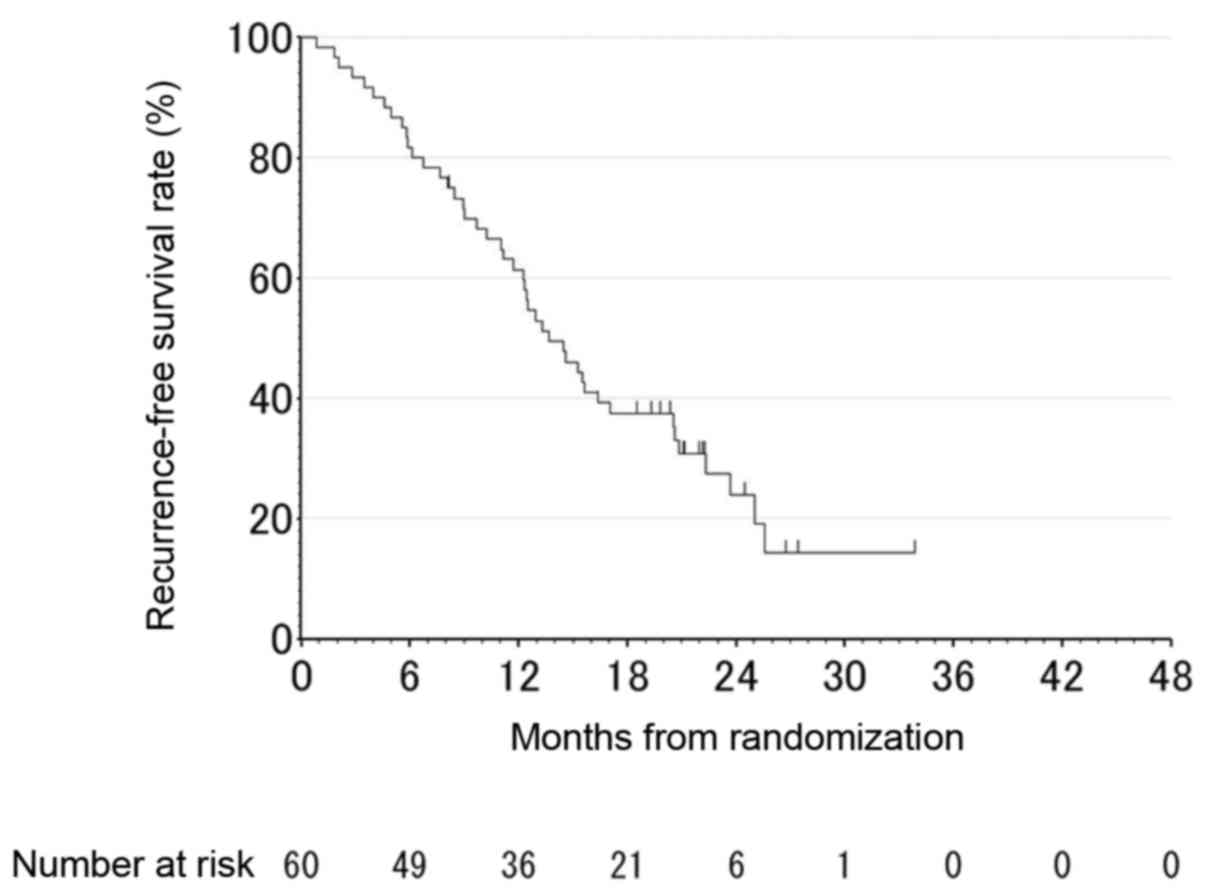
| Median progression
free survival, months | 13.7 | 11.2–16.4 |
| Progression
events | 46 |
|
| Censored | 14 |
|
| Progression free
rate at 12 months | 61.4 | 47.8–72.4 |
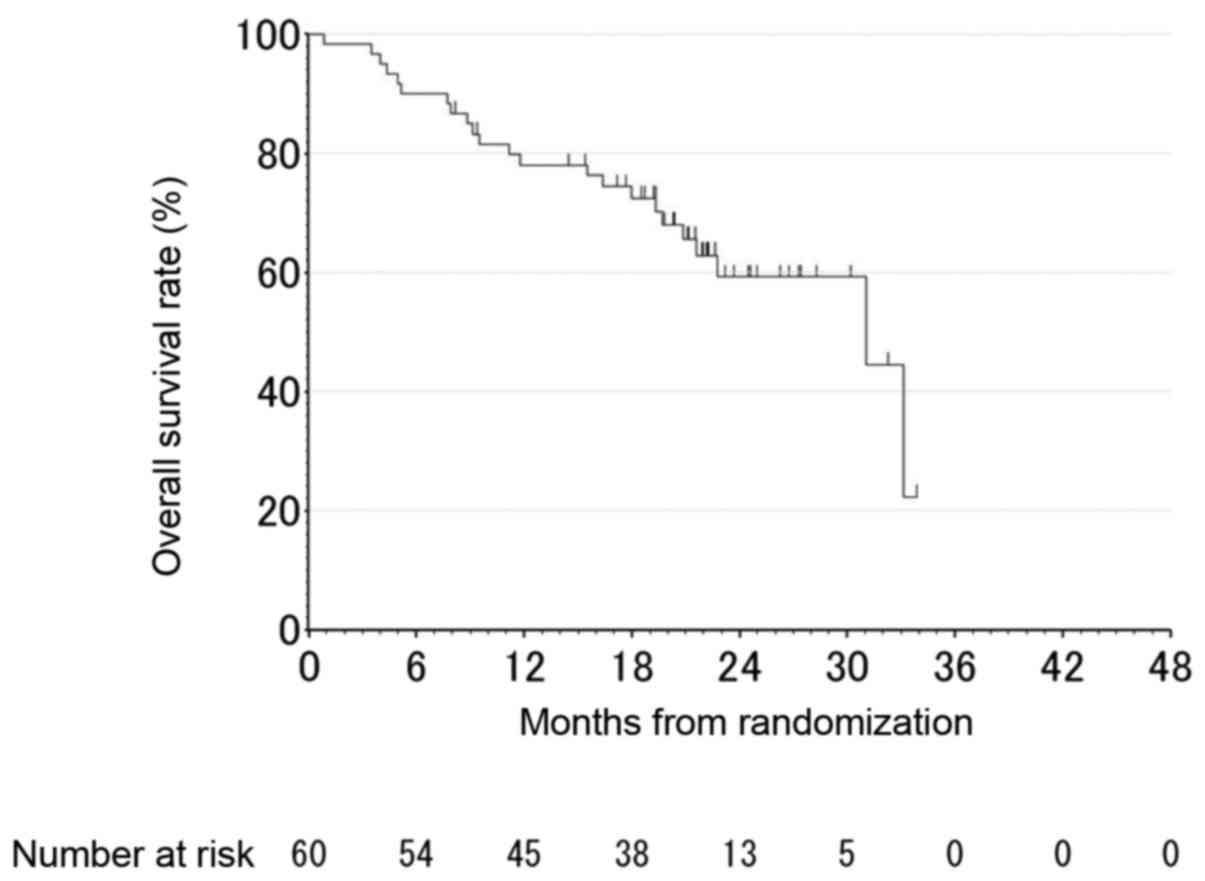
| Median overall
survival, months | 31.0 | 21.6-N/A |
| Deaths | 24 |
|
| Censored | 36 |
|
| 1-year survival
rate | 78.1 | 65.2–86.6 |
| 2-year survival
rate | 55.3 | 38.8–69.1 |
| Surgery for
metastatic disease | 20 |
|
| Liver surgery | 13 |
|
| Lung surgery | 2 |
|
| Other organ
surgery | 7 |
|
| Results of
surgery |
|
|
| No
residual tumor after the resection | 13 |
|
|
Microscopic (R1) residual
lesion | 3 |
|
After a median follow-up of 22.7 months, the median
PFS was 13.8 months (95% CI, 11.7–17.1; Fig. 1), and the median OS was 31.0 months
(95% CI, 21.6-NA; Fig. 2).
There were 13 patients (21.7%) who underwent surgery
for liver metastases, and complete surgical resection was observed
in 10 patients. The median PFS following surgical resection of the
metastases was 14.9 months. Median OS was not evaluable. Nine of
the 26 patients receiving second-line chemotherapy continued with
cetuximab-containing regimens following surgery.
Treatment compliance and safety
The treatment exposure is summarized in Table III. The median course of study
treatment was 10.5 months (range, 2.0–52.0). Patients achieving
relative dose intensity ≥80% for each drug is presented (Table III). Adverse events (AEs) of any
grade occurred in all patients (100%), and grade 3 or 4 AEs
(classed as severe or life-threatening) were observed in 66.7%
(40/60 patients). Patient AEs are summarized in Table IV. The most common grade 3 or 4 AEs
were leutropenia (41.7%) and paronychia (18.3%). Out of all the
patients presenting with grade 3 or 4 AE, 8.3% presented with an
acne-like rash and one patient presented with infusion-related
reactions (this special event category included the preferred terms
‘infusion-related reaction’ and ‘pyrexia’).
| Table III.Treatment exposure. |
Table III.
Treatment exposure.
| Treatment
parameter | Cetuximab | Oxaliplatin | Fluorouracil |
|---|
| Median
dose-intensity (mg/m2/week) | 227 | 32 | 1010 |
| Median
dose-intensity (mg/m2/2 weeks) | 430 | 61 | 1917 |
| Relative
dose-intensity (%) |
|
|
|
|
Median | 86.3 | 72.5 | 79.9 |
|
≥90 | 38.3 | 16.7 | 31.7 |
| ≥80 to
<90 | 31.7 | 15.0 | 18.3 |
| ≥60 to
<80 | 21.7 | 35.0 | 36.7 |
|
<60 | 8.3 | 33.3 | 13.3 |
| Table IV.Relevant adverse events in ≥10% of
patients (highest grade/patient). |
Table IV.
Relevant adverse events in ≥10% of
patients (highest grade/patient).
|
| Grade III or
IV | All grade |
|---|
|
|
|
|
|---|
| Adverse event | No. patients | Percentage, % | No. patients | Percentage, % |
|---|
| Hematological |
|
|
|
|
| White
blood cell decrease | 6 | 10.0 | 38 | 63.3 |
|
Leukopenia | 25 | 41.7 | 32 | 53.3 |
|
Anemia | 2 | 3.3 | 45 | 75.0 |
|
Thrombocytopenia | 0 | 0 | 38 | 63.3 |
| Non
hematological |
|
|
|
|
|
Elevated AST/ALT | 0 | 0 | 41 | 68.3 |
|
Elevated serum bilrubin | 0 | 0 | 5 |
8.3 |
|
Elevated creatine | 0 | 0 | 14 | 23.3 |
|
Stomatitis | 2 | 3.3 | 27 | 45.0 |
|
Nausea/vomiting | 2 | 3.3 | 27 | 45.0 |
|
Diarrhea | 0 | 0 | 16 | 26.7 |
|
Rash | 5 | 8.3 | 53 | 88.3 |
|
Paronychia | 11 | 18.3 | 45 | 75.0 |
|
Anorexia | 2 | 3.3 | 31 | 51.7 |
|
Fatigue | 1 | 1.7 | 28 | 46.6 |
|
Infusion related reaction | 1 | 1.7 | 4 |
6.7 |
|
Paresthesia | 5 | 8.3 | 53 | 88.3 |
Discussion
The current study aimed to evaluate the response
rate of patients with KRAS wild-type mCRC to the first-line
treatment of FOLFOX-6 combined with biweekly cetuximab. The results
indicated that the efficacy and safety of this method of treatment
is similar to those observed in previous phase II studies that
evaluated the biweekly administered cetuximab regimen and reported
the standard weekly cetuximab dosing regimen as a first-line
treatment of KRAS wild-type mCRC (17,18).
The confirmed best ORR was 70% (95% CI, 56.8–81.2%),
and similar ORR was observed regardless of the metastatic organ
site. The ORR results obtained from the present study are similar
to a previous phase II study evaluating the efficacy of biweekly
administration of cetuximab in combination with FOLFOX-4.
Furthermore, two other phase II trials have evaluated the efficacy
and safety of a biweekly administration of cetuximab in combination
with FOLFOX-4 to treat mCRC. One study was performed by the Central
European Cooperative Oncology Group (CECOG) (19). This randomized phase II study
investigated the efficacy and safety of chemotherapy plus cetuximab
administered every second week as a first-line treatment for KRAS
wild-type mCRC. In this trial, the ORR was 62% (95% CI, 51–73%) in
the biweekly cetuximab arm. Another phase II, open-label clinical
trial (the OPTIMIX-ACROSS study), evaluated biweekly cetuximab in
combination with FOLFOX-4 as first-line treatment for KRAS
wild-type mCRC (17). This phase II
study was carried out in 15 Spanish centers and the ORR was 60.6%
(95% CI, 50.3–70.3%) in the biweekly cetuximab arm. In addition,
the confirmed best ORR achieved in the current study was similar to
a previous phase II study, Oxaliplatin and Cetuximab in First-Line
Treatment of Metastatic Colorectal Cancer (OPUS), investigating the
efficacy of a weekly administration of cetuximab in combination
with FOLFOX-4. The ORR was reported as 57% (95% CI, 46–68%) in the
KRAS wild-type population and 60% (95% CI, 48–71%) in the KRAS/BRAF
wild-type population in patients receiving weekly infeusions of
cetuximab and FOLFOX-4 (11).
The median PFS was 13.8 months (95% CI, 11.7–17.1
months) in the present study. This was similar to the median PFS
reported in the OPTIMIX-ACROSS study and the CECOG trial, which
were 10.1 months and 9.2 months respectively (17,19).
Furthermore, it was slightly longer than the range of 8.4–9.1
months previously reported for the standard weekly cetuximab
administration in combination with other oxaliplatin-based
chemotherapy regimens in patients with KRAS wild-type mCRC
(18).
The feasibility of a biweekly cetuximab
administration schedule was previously investigated in a two-part
phase I dose escalation study (20).
This study demonstrated that cetuximab may be safely administered
as a single agent or in combination with FOLFIRI at doses of
400–700 mg/m2 in a biweekly schedule, and 500
mg/m2 was established as the recommended dose according
to the pharmacokinetic exposure data. Therefore, in the present
study, the patients received a biweekly intravenous infusion of
cetuximab (500 mg/m2 on day 1) followed by FOLFOX-6.
Most patients (66.7%) experienced severe AEs (grade 3 or 4),
however, this is normal compared with patients undergoing other
treatment regimes, demonstrating that the combination of cetuximab
and FOLFOX was generally well tolerated. There was no evidence in
the current study suggesting that cetuximab increased the frequency
or severity of characteristic toxicities associated with FOLFOX
treatment. Indeed, the proportion of patients with grade 3 or 4 AEs
observed in the current study was similar to those in previous
studies: 77.8% in the OPTIMIX-ACROSS study and 71% in the biweekly
arm of the CECOG trial (17,19). Moreover, typical and manageable
EGFR-inhibitor-related AEs, such as a rash or acne-like rash, were
reported at grades 3 or 4 for 8.3% of the patients, similar to
previous studies.
The frequency of bone marrow suppression recorded
was markedly higher than that of previous studies. Incidences of
leukopenia, neutropenia, anemia, and thrombocytopenia were 63.3,
53.3, 75.0, and 63.3%, respectively, in the present study, compared
with 15.2, 49.5, 11.1, and 23.2% in the OPTIMIX-ACROSS study
(17). However, the frequency of
severe bone marrow suppression (grade 3 or 4) requiring
dose-reduction or treatment delay was similar. The incidences of
leukopenia, neutropenia, anemia, and thrombocytopenia were 10.0,
41.7, 3.3, and 0%, respectively, in the present study, compared
with 1.0, 32.3, 2.0, and 2.0%, respectively in the OPTIMIX-ACROSS
Study. Moreover, the Multicenter Phase II study of FOLFOX or
biweekly XELOX and Erbitux (cetuximab) as first-line therapy in
patients with wild-type KRAS/BRAF metastatic
colorectal cancer (The FLEET study), documented a similar toxicity:
The incidences of grade 3 or 4 leukopenia, neutropenia, and
thrombocytopenia were 10.8, 29.7, and 5.4% in patients treated with
FOLFOX-6 and cetuximab (20).
The present study demonstrated the equivalent
efficacy and safety of biweekly cetuximab in combination with
FOLFOX-6 for patients with KRAS wild-type mCRC compared with the
current standard first-line treatment. There are numerous
advantages of administering cetuximab biweekly instead of weekly
(14). Synchronous cetuximab and
chemotherapy administration is much more convenient for patients
with mCRC. A reduction in the frequency of hospital visits may
improve patient quality of life. Furthermore, the biweekly
combination regimen may simplify treatment administration for
health care workers and be more economical; a simplified
administration schedule may decrease the costs associated with
frequent cetuximab administration as well as frequent hospital
visits. Thus, biweekly-administered cetuximab in combination with
FOLFOX-6 may benefit governments, patients, physicians, and other
health care workers involved in treating mCRC.
One important limitation of the present study is the
lack of information regarding tumor makers. Tumor makers are an
important measurement of treatment efficacy, however; tumor marker
measurement was not included as an endpoint. Instead, the primary
endpoint of the present study was the overall response rate, and
secondary endpoints were progression-free survival, overall
survival, disease control rate, the incidence of adverse events,
and response rate at each metastatic site. Therefore further
studies collecting tumor marker measurements and taking them into
consideration are required.
In conclusion, the present study demonstrated that
biweekly administration of cetuximab in combination with FOLFOX-6
has a feasible and manageable safety profile for the first-line
treatment of KRAS wild-type mCRC. The results support a biweekly
cetuximab regimen as a novel therapeutic strategy to treat KRAS
wild-type mCRC, which may be more convenient for patients and
provide more flexibility for those administering the treatment.
Acknowledgements
The present study was supported, in part, by the
non-profit organization Epidemiological & Clinical Research
Information Network (ECRIN). The authors are especially grateful to
Ms. Mai Hatta and Ms. Chikako Ikeda for their excellent
contributions as clinical research coordinators of this study.
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Douillard JY, Cunningham D, Roth AD,
Navarro M, James RD, Karasek P, Jandik P, Iveson T, Carmichael J,
Alakl M, et al: Irinotecan combined with fluorouracil compared with
fluorouracil alone as first-line treatment for metastatic
colorectal cancer: A multicentre randomised trial. Lancet.
355:1041–1047. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Saltz LB, Cox JV, Blanke C, Rosen LS,
Fehrenbacher L, Moore MJ, Maroun JA, Ackland SP, Locker PK, Pirotta
N, et al: Irinotecan plus fluorouracil and leucovorin for
metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med.
343:905–914. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Köhne CH, van Cutsem E, Wils J, Bokemeyer
C, El-Serafi M, Lutz MP, Lorenz M, Reichardt P, Rückle-Lanz H,
Frickhofen N, et al: Phase III study of weekly high-dose infusional
fluorouracil plus folinic acid with or without irinotecan in
patients with metastatic colorectal cancer: European Organisation
for Research and Treatment of Cancer Gastrointestinal Group Study
40986. J Clin Oncol. 23:4856–4865. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
de Gramont A, Figer A, Seymour M, Homerin
M, Hmissi A, Cassidy J, Boni C, CortesFunes H, Cervantes A, Freyer
G, et al: Leucovorin and fluorouracil with or without oxaliplatin
as first-line treatment in advanced colorectal cancer. J Clin
Oncol. 18:2938–2947. 2000.PubMed/NCBI
|
|
6
|
Sunada H, Magun BE, Mendelsohn J and
MacLeod CL: Monoclonal antibody against epidermal growth factor
receptor is internalized without stimulating receptor
phosphorylation. Proc Natl Acad Sci USA. 83:3825–3829. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li S, Schmitz KR, Jeffrey PD, Wiltzius JJ,
Kussie P and Ferguson KM: Structural basis for inhibition of the
epidermal growth factor receptor by cetuximab. Cancer Cell.
7:301–311. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cunningham D, Humblet Y, Siena S, Khayat
D, Bleiberg H, Santoro A, Bets D, Mueser M, Harstrick A, Verslype
C, et al: Cetuximab monotherapy and cetuximab plus irinotecan in
irinotecan-refractory metastatic colorectal cancer. N Engl J Med.
351:337–345. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Goldstein NS and Armin M: Epidermal growth
factor receptor immunohistochemical reactivity in patients with
American Joint Committee on Cancer Stage IV colon adenocarcinoma:
Implications for a standardized scoring system. Cancer.
92:1331–1346. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Van Cutsem E, Köhne CH, Láng I, Folprecht
G, Nowacki MP, Cascinu S, Shchepotin I, Maurel J, Cunningham D,
Tejpar S, et al: Cetuximab plus irinotecan, fluorouracil, and
leucovorin as first-line treatment for metastatic colorectal
cancer: Updated analysis of overall survival according to tumor
KRAS and BRAF mutation status. J Clin Oncol. 29:2011–2019. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bokemeyer C, Bondarenko I, Hartmann JT, de
Braud F, Schuch G, Zubel A, Celik I, Schlichting M and Koralewski
P: Efficacy according to biomarker status of cetuximab plus
FOLFOX-4 as first-line treatment for metastatic colorectal cancer:
The OPUS study. Ann Oncol. 22:1535–1546. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tabernero J, Pfeiffer P and Cervantes A:
Administration of cetuximab every 2 weeks in the treatment of
metastatic colorectal cancer: An effective, more convenient
alternative to weekly administration? Oncologist. 13:113–119. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Okayama N, Nishioka M, Hazama S, Sakai K,
Suehiro Y, Maekawa M, Sakamoto J, Iwamoto S, Kato T, Mishima H, et
al: The importance of evaluation of DNA amplificability in KRAS
mutation testing with dideoxy sequencing using formalin-fixed and
paraffin-embedded colorectal cancer tissues. Jpn J Clin Oncol.
41:165–171. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Iwamoto S, Hazama S, Kato T, Miyake Y,
Fukunaga M, Matsuda C, Bando H, Sakamoto J, Oba K, Mishima H, et
al: Multicenter phase II study of second-line cetuximab plus
folinic acid/5-fluorouracil/irinotecan (FOLFIRI) in KRAS wild-type
metastatic colorectal cancer: The FLIER study. Anticancer Res.
34:1967–1973. 2014.PubMed/NCBI
|
|
15
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
National Cancer and Institute Cancer
Therapy Evaluation Program, . Common Terminology Criteria for
Adverse Events v3.0 (CTCAE). https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf
|
|
17
|
Fernandez-Plana J, Pericay C, Quintero G,
Alonso V, Salud A, Mendez M, Salgado M, Saigi E and Cirera L:
ACROSS Study Group: Biweekly cetuximab in combination with FOLFOX-4
in the first-line treatment of wild-type KRAS metastatic colorectal
cancer: Final results of a phase I. BMC Cancer. 14:8652014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Soda H, Maeda H, Hasegawa J, Takahashi T,
Hazama S, Fukunaga M, Kono E, Kotaka M, Sakamoto J, Nagata N, et
al: Multicenter Phase II study of FOLFOX or biweekly XELOX and
Erbitux (cetuximab) as first-line therapy in patients with
wild-type KRAS/BRAF metastatic colorectal cancer: The FLEET study.
BMC Cancer. 15:6952015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Brodowicz T, Ciuleanu TE, Radosavljevic D,
ShachamShmueli E, Vrbanec D, Plate S, MrsicKrmpotic Z, Dank M,
Purkalne G, Messinger D and Zielinski CC: FOLFOX4 plus cetuximab
administered weekly or every second week in the first-line
treatment of patients with KRAS wild-type metastatic colorectal
cancer: A randomized phase II CECOG study. Ann Oncol. 24:1769–1777.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tabernero J, Ciardiello F, Rivera F,
RodriguezBraun E, Ramos FJ, Martinelli E, VegaVillegas ME, Roselló
S, Liebscher S, Kisker O, et al: Cetuximab administered once every
second week to patients with metastatic colorectal cancer: A
two-part pharmacokinetic/pharmacodynamic phase I dose-escalation
study. Ann Oncol. 21:1537–1545. 2010. View Article : Google Scholar : PubMed/NCBI
|