Introduction
As the average life span has increased with the
advancement of medicine, there has been an increase in the
proportion of elderly people in the population worldwide (1). Despite advances in medical technology,
the number of elderly people with cancer has increased, and this
population is difficult to treat (2).
In addition, elderly people exhibit an elevated incidence of high
blood pressure (3), and numerous
studies have reported that hypertension is associated with cancer
(4–8).
For anticancer therapy in this population, angiotensin receptor II
blockers (ARBs) are currently being investigated (9–11).
Angiotensin II is the activated form of the protein
angiotensin, resulting from the cleavage of angiotensin I by
angiotensin-converting enzyme, and promotes the reabsorption of
water and sodium ions and the contraction of blood vessels, thereby
reducing blood pressure (12).
Therefore, the blood pressure of patients with hypertension can be
reduced by targeting angiotensin receptor II (13). Angiotensin II receptor antagonists,
also known as sartans, are a group of pharmaceuticals that possess
tetrazole or imidazole groups, which function as anti-hypertensive
drugs (14). Previous studies have
indicated that angiotensin II promotes the proliferation and
metastasis of tumors (15,16), and that ARBs exhibit antiproliferative
and antimetastatic effects on tumors (17–20). In
addition, it has been reported that ARBs inhibit the growth of
prostate cancer cell lines via suppression of the mitogen-activated
protein kinase (MAPK) or signal transducer and activator of
transcription 3 (STAT3) phosphorylation (21) and exhibited an antitumor effect on
patients with prostate cancer (22–24).
The ultimate aim of cancer therapy is the death of
cancer cells, which may be induced by apoptotic or necrotic
pathways (25,26). However, cancer cells are able to evade
cell death mechanisms (27),
therefore a novel approach to target anti-apoptotic mechanisms in
cancer is required. Previous reports have indicated that the
induction of autophagic signals led to the death of cancer cells,
despite autophagy being used as a survival strategy in cells
experiencing insufficient supply of nutrients under hypoxic
conditions (28–30). The phenomenon is termed
autophagy-induced cell death, and is an alternative therapeutic
approach to apoptosis-resistant cancer cells.
In the present study, the dose- and time-dependent
anticancer effects of commercially available ARBs, and whether the
ARBs were able to induce autophagy-induced cell death, were
investigated in prostate cancer cells. Furthermore, the inhibitory
effect of the ARBs with respect to the migration and proliferation
of tumor cells was investigated.
Materials and methods
Reagents
Fimasartan was obtained from Boryung Pharmaceutical
Co., Ltd. (Seoul, Korea). Losartan potassium (Merck Sharp &
Dohme, Hoddesdon, UK), eprosartan mesylate (Solvay Pharmaceuticals,
Weesp, Netherlands) and valsartan (Novartis AG, Basel, Switzerland)
were used in the present study. All ARBs were used at
concentrations of 100, 200 and 400 µM. The inhibitors
3-methyladenine (3-MA; Sigma-Aldrich; Merck KGaA, Darmstadt,
Germany), Z-VAD-FMK (Calbiochem, Billerica, MA, USA), a pan-caspase
inhibitor, and Necrostatin-1 (Sigma-Aldrich, St Louis, MO, USA)
were used to treat the human cancer cell lines to inhibit each type
of cell death.
Cell lines and cell culture
The human prostate cancer cell lines PC3 [Korean
Cell Line Bank (KCLB) no. 21435], DU145 (KCLB no. 30081) and
LNCap-LN3 (KCLB no. 80018) were obtained from the KCLB (Seoul,
Korea). A total of 3×105 of each type of prostate cancer
cell was plated in 60-mm cell culture dishes (SPL Life Sciences,
Pocheon, Korea). Cells were grown in RPMI-1640 medium (GE
Healthcare Life Sciences, Logan, UT, USA) and supplemented with 10%
heat inactivated fetal bovine serum (FBS; Lonza Group Ltd.,
Walkersville, MD, USA) and antibiotics (1,000 U/ml penicillin and
1,000 µg/ml streptomycin; both GE Healthcare Life Sciences). The
FBS was heat inactivated for 1 h at 56°C. The prostate cancer cells
were cultured at 37°C, in a humidified atmosphere containing 5%
CO2. To verify the mechanisms of cell death with
treatment of ARBs, PC-3 cells were pretreated with 10 mM 3-MA, 50
µM Z-VAD-FMK or 50 µM Necrostatin-1 or 3 h at 37°C prior to
fimasartan treatment at a concentration of 200 µM.
Protein extraction and western
blotting
The prostate cancer cell lines (3×105
cells per cell line) were treated with 200 µM ARBs for 0, 24, 48,
72 and 96 h at 37°C under 5% CO2. The cells were then
harvested and the proteins were extracted, using
radioimmunoprecipitation assay buffer containing 10 mM Tris-HCl, 1
mM EDTA, 140 mM NaCl, 0.1% deoxycholate, 0.1% SDS, 100% Triton
X-100 and 100X Protease Inhibitor Cocktail Set I (EMD Millipore,
Billerica, MA, USA). The protein samples of the cell lysates were
quantified using a Bradford assay. In total, 30 µg of each protein
samples loaded onto the gel. Each sample was separated by 10–15%
SDS-PAGE and transferred onto a 0.45 µm polyvinylidene fluoride
membrane (Millipore, Billerica, MA, USA) for 2 h at 100 constant
voltage on ice. The membranes were blocked with 5% skimmed milk in
TBS-T (TBS and Tween-20) buffer for 1 h at room temperature. The
primary antibodies used were anti-LC3B (cat. no. 2775; Cell
Signaling Technology, Inc., Danvers, MA, USA), anti-Atg12 (cat. no.
4180; Cell Signaling Technology, Inc.), anti-Atg16L1 (cat. no.
8089; Cell Signaling Technology, Inc.), anti-Beclin-1 (cat. no.
3738; Cell Signaling Technology, Inc.) and anti-β-actin (cat. no.
sc-130656; Santa Cruz Biotechnology, Inc., Dallas, TX, USA).
Anti-rabbit IgG (cat. no. 7074; Cell Signaling Technology, Boston,
MA, USA) was used as the secondary antibody. All antibodies were
diluted 1,000-fold with blocking buffer. Membranes were incubated
with primary antibodies for 3.5 h and with secondary antibody for
2.5 h at room temperature. The membranes were washed 3 times in
TBS-T buffer for 10 min. The membranes were developed using an
enhanced chemiluminescence western blotting detection system (BD
Biosciences, San Hose, CA, USA) according to the protocol of the
manufacturer, and exposed to X-ray sheets (Agfa-Gevaert N.V.,
Mortsel, Belgium). The western blotting results were quantified
using densitometry (ImageJ; version 1.48; National Institutes of
Health, Bethesda, MD, USA).
Cell proliferation assay
Cell viability in the presence or absence of the
ARBs was determined using a Premix WST-1 Cell Proliferation Assay
System (Takara Bio, Inc., Otsu, Japan). In total, 1×103
cells (100 µl/well) were incubated in 96-well plates for 24 h at
37°C under 5% CO2. Subsequently, 100, 200 and 400 µM
ARBs in RPMI-1640 were added to the wells and cultured at 37°C for
48 and 72 h for PC3 and DU145 cells, and 60 and 120 h for LNCap-LN3
cells. A total of 10 µl WST-1 solution was added to each well, and
the plates were incubated for 30 min at 37°C, following which the
absorbance at 450 and 690 nm was measured using a microplate
reader.
Confocal microscopy
The PC3 human prostate cancer cells were seeded onto
glass coverslips (Paul Marienfeld GmbH & Co., KG,
Lauda-Königshofen, Germany) at a density of 1×105
cells/well in 6-well plates for 24 h, and were treated with
fimasartan (200 µM) for 24, 48 and 72 h at 37°C under 5%
CO2. Following all treatment and incubation, the cells
were fixed with 4% formaldehyde at room temperature for 15 min. The
cells were permeabilized with 0.2% Triton X-100 in PBS for 15–20
min, then blocked with 1% bovine serum albumin (BSA; Sigma-Aldrich;
Merck KGaA) in PBS solution for 1 h at room temperature. On the
basis of a previous study (30), PC3
cells was incubated with anti-LC3 antibody (cat. no. PM036; Medical
& Biological Laboratories Co., Ltd., Nagoya, Japan; 1:500
dilution in 1% BSA and 0.05% Triton X-100 in PBS) for 2 h at room
temperature. Subsequent to washing with PBS, cells were treated
with anti-rabbit-fluorescein isothiocyanate (cat. no. 111-095-003;
Jackson ImmunoResearch Laboratories, Inc., West Grove, PA, USA;
1:500 dilution in 1% BSA, 0.05% Triton X-100 in PBS) for 2 h at
room temperature. Each well was washed twice with 0.02% Tween-20
and 1% BSA in PBS. The coverslips were mounted and the cells were
examined using confocal microscopy (FV1000; Olympus Corporation,
Tokyo, Japan). The results were quantified by densitometry.
Migration assay
A Transwell (6.5 µm pore; Corning Incorporated,
Corning, NY, USA) migration assay was performed. Top chambers were
seeded with 100 µl RPMI-1640 containing PC3 and DU145 cells
(1×104 cells per well) and the bottom chambers were
filled with 600 µl RPMI-1640, and the chambers were incubated for
24 h at 37°C under 5% CO2. After 24 h, the bottom
chamber was washed with 1xPBS and was filled with 600 µl RPMI-1640
with or without 200 µM fimasartan for 6 h at 37°C. Migrated cells
on the bottom side of the membrane were fixed with 4%
paraformaldehyde for 30 min at room temperature and washed with PBS
twice. Cell migration was evaluated through hematoxylin and eosin
staining. The results were measured as the mean number of migrated
cells counted using a Motic AE31 optical microscope (Motic, Xiamen,
China). Data are expressed as the mean ± standard deviation from 3
independent experiments.
Statistical analysis
All data are presented as the mean ± the standard
deviation. Statistical analysis was performed with one-way analysis
of variance followed by a Tukey-Kramer multiple comparison test by
GraphPad Prism (version 5.0; GraphPad Software, Inc., La Jolla, CA,
USA). P<0.05 was considered to indicate a statistically
significant difference. Experiments were repeated a minimum of 3
times for each condition.
Results
Reduced cell viability in ARB-treated
prostate cancer cell lines
The expression of angiotensin II receptor has been
reported in the human prostate cancer cell lines PC3, DU145 and
LNCap-LN3 (31). Therefore, the
anti-proliferative effects of the ARBs fimasartan, losartar,
eprosartan and valsartan were investigated in human prostate cancer
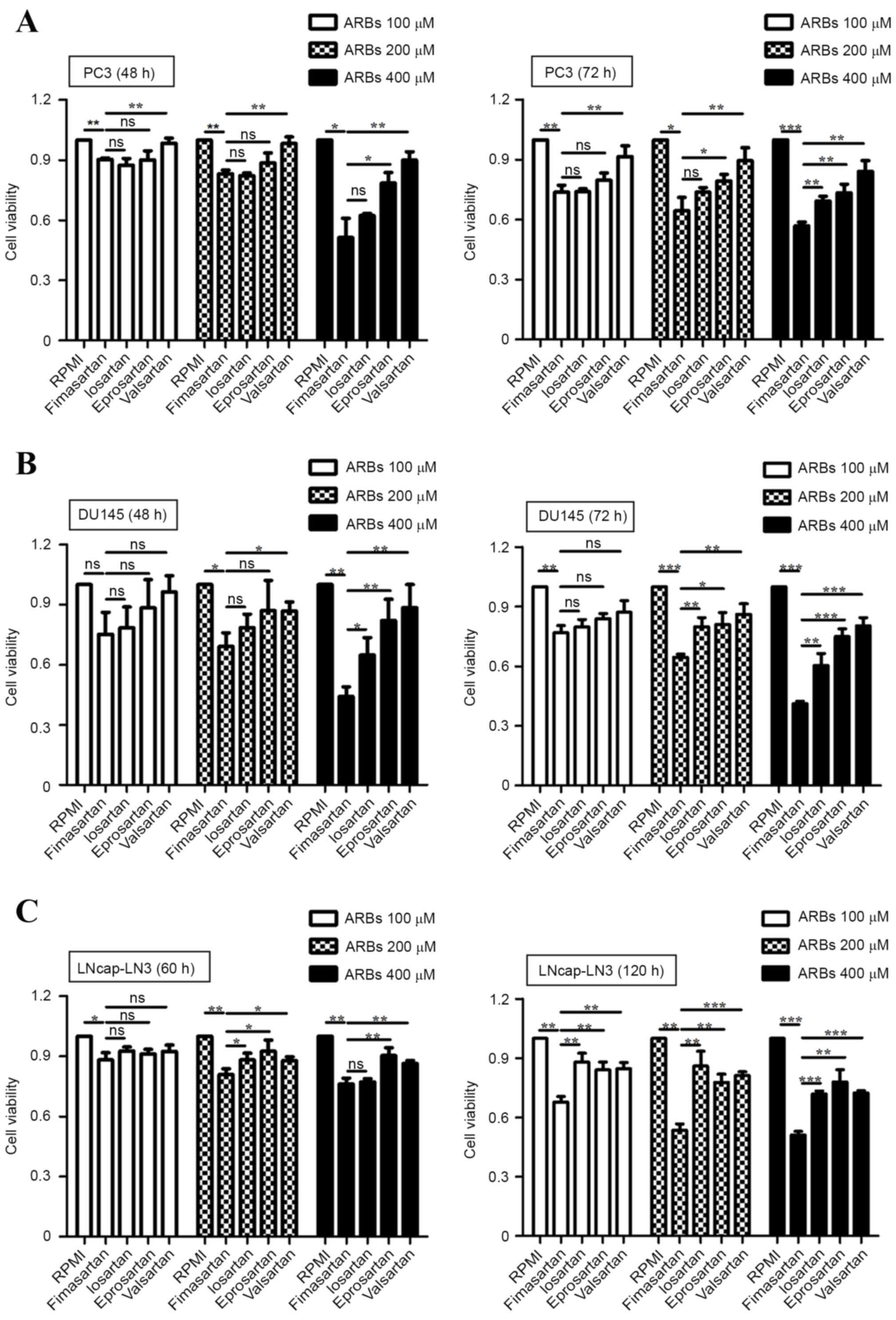
cells in the present study (Fig. 1).
The ARBs at concentrations 100, 200 and 400 µM were applied to PC3,
DU145 and LNCap-LN3 cells, and the cytotoxicity of the ARBs was
evaluated by a WST-1 assay. Considering the difference in the
doubling time of the cells (PC3, 35 h; DU145, 29 h; and LNCap-LN3,
60 h), cell proliferation was measured at 48 and 72 h in the PC3
and DU145 cells, and at 60 and 120 h in the LNCap-LN3 cells.
Compared with the control group, the ARB-treated cells showed
reduced cell viability. At 400 µM all the ARBs exerted
anti-proliferative effects on prostate cancer cells at each time
point, but fimasartan exhibited the greatest cytotoxicity (Fig. 1). Valsartan demonstrated the lowest
anti-proliferative activity compared with other ARBs in the
prostate cancer cells. LNCap-LN3 had the longest doubling time of
the cells investigated, and demonstrated similar cytotoxic effects
in response to ARBs to the other cells (Fig. 1C) The present results are consistent
with previous studies in which ARBs were demonstrated to inhibit
the growth of bladder, breast and gastric cancer (17–20), and
fimasartan was observed to exert the greatest anti-proliferative
effect on prostate cancer cells.
Autophagy-induced cell death in
ARB-treated PC3 cells
To verify the type of cell death mechanism involved
in prostate cancer cells following ARB treatment, specific
inhibitors that block each type of cell death were administered to
PC-3 cells with fimasartan. Although pan-caspase inhibitor, an
apoptosis blocker, slightly reduced ARB-induced cell death at 48 h,
the cell survival fraction was restored significantly when the
cells were treated with 3-MA, an autophagy inhibitor, at 72 h.
Necrostatin-1, a necrosis inhibitor, did not significantly increase
the cell viability in fimasartan-treated PC-3 cells.
Autophagy-induced cell death, also known as type II programmed cell
death, was proposed by Schweichel and Merker (32); it is a cellular suicide process
accompanied by the appearance of a giant cytoplasmic vacuole known
as the autophagosome. This process may be induced in cancer cells
that are resistant to apoptosis due to a deficiency in
apoptosis-associated proteins, including B-cell lymphoma-2-like
protein 4 and B-cell lymphoma-2 homologous antagonist/killer.
Additionally, the inhibition of caspases, which are key
apoptosis-associated proteins, is able to prevent cell death
(33). Therefore, the induction of
autophagic cell death is an alternative death mechanism in
apoptosis-resistant cells. LC3, the mammalian homologue of yeast
Atg8, is a marker of autophagosome formation. When autophagic
signals are activated, a phagophore is formed and LC3-I is
conjugated to phosphatidylethanolamine, forming LC3-II, which, with
the Atg12-Atg5-Atg16 complex, serves an important role in
phagophore elongation. Therefore, the detection of LC3, the Atg12-5
complex, Atg16 and Beclin-1 using western blotting provides
suitable markers by which to measure the signaling initiation of
autophagy. The PC3 cells were treated with 200 µM fimasartan, and
harvested at 0, 24, 48, 72 and 96 h, following which western
blotting was performed. This indicated changes in the expression
levels of autophagy-associated proteins, with the peak level of
LC3-II expression induced at 72 h (6.7-fold increase; Fig. 2B). The inhibitor 3-MA reduced the
expression level of converted LC3-II in fimasartan-treated cells
(Fig. 2C). In addition, numerous
vacuolar compartments were observed in the PC-3 cells subsequent to
treatment with fimasartan at 72 h (Fig.
2C). Therefore, fimasartan may be regarded as an autophagy
inducer in PC3 human prostate cancer cells. Additionally, treatment
with 200 µM losartan, eprosartan and valsartan resulted in
alterations in the expression of autophagy-associated proteins in
PC3 cells, similar to the result following fimasartan treatment
(Fig. 2D). Losartan and eprosartan
induced peak levels of LC3-II at 96 h (18.8- and 11.1-fold
increases, respectively), and valsartan treatment resulted in the
largest increase in the expression of LC3-II at 72 h (11.2-fold
increase), measured using densitometry.
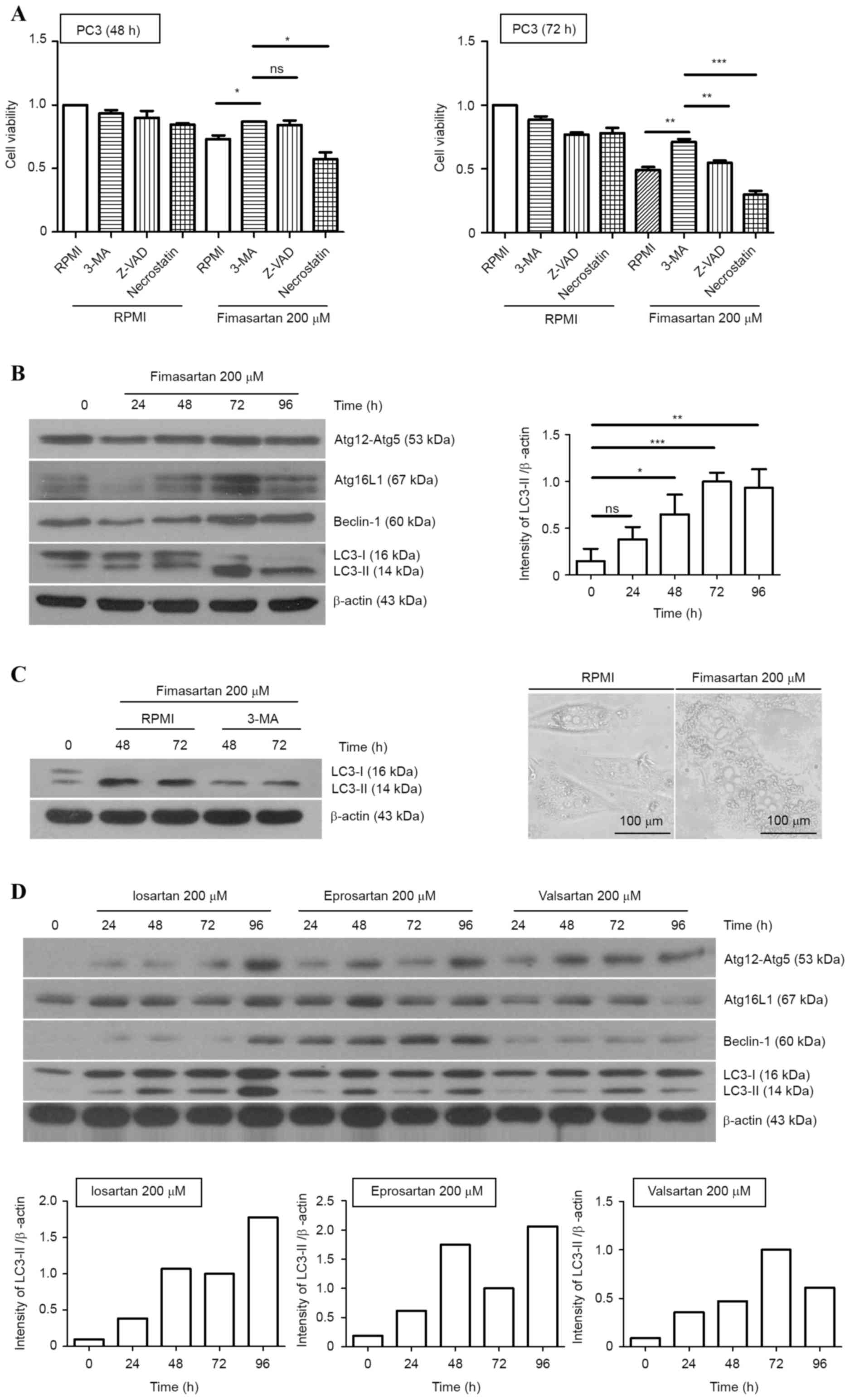 | Figure 2.Autophagy-induced cell death in the
angiotensin II receptor blocker-treated PC3 cells. (A) PC3 cells
were pretreated with 3-MA (10 mM), Z-VAD-FMK (50 µM) or
Necrostatin-1 (50 µM) for 3 h. Each group of cells was stimulated
by fimasartan (200 µM) and cell viability was analyzed for 48 and
72 h via WST-1 assay. (B) PC3 cells were treated with 200 µM
fimasartan, and changes in the expression levels of Atg-12-Atg5,
Atg16L1, Beclin-1 and LC-3 were measured using western blot
analysis at each time point. (C) The expression levels of LC3-II
were significantly reduced with 3-MA pretreatment (left panel). PC3
cells were observed at 72 h subsequent to 200 µM fimasartan
treatment under a microscope. (D) PC3 cells were treated with 200
µM losartan, eprosartan or valsartan, and western blot analysis was
performed to detect alterations in the expression of
autophagy-associated proteins. Densitometry results are presented
as the mean ± standard deviation of triplicate experiments. β-actin
was used as a loading control. ns, non-significant; *P<0.05,
**P<0.01, ***P<0.001. 3-MA, 3-methyladenine; Atg, autophagy
protein; LC3, microtubule-associated protein 1A/1B-light chain
3. |
To evaluate whether autophagy was occurring in the
PC3 cells following treatment with fimasartan, confocal imaging of
immunofluorescent staining was performed. LC3-positive foci were
observed scattered throughout the cytoplasm following fimasartan
treatment (Fig. 3A). Furthermore, the
number of LC3-positive foci increased and the intensity of
fluorescein isothiocyanate-fluorescence was enhanced in a
time-dependent manner. The results were quantified by measuring the
number of cells containing LC3-positive foci compared with the
total number of cells (Fig. 3B).
Therefore, it appears that ARBs are able to induce autophagy and
initiate growth inhibition in human prostate cancer cell lines.
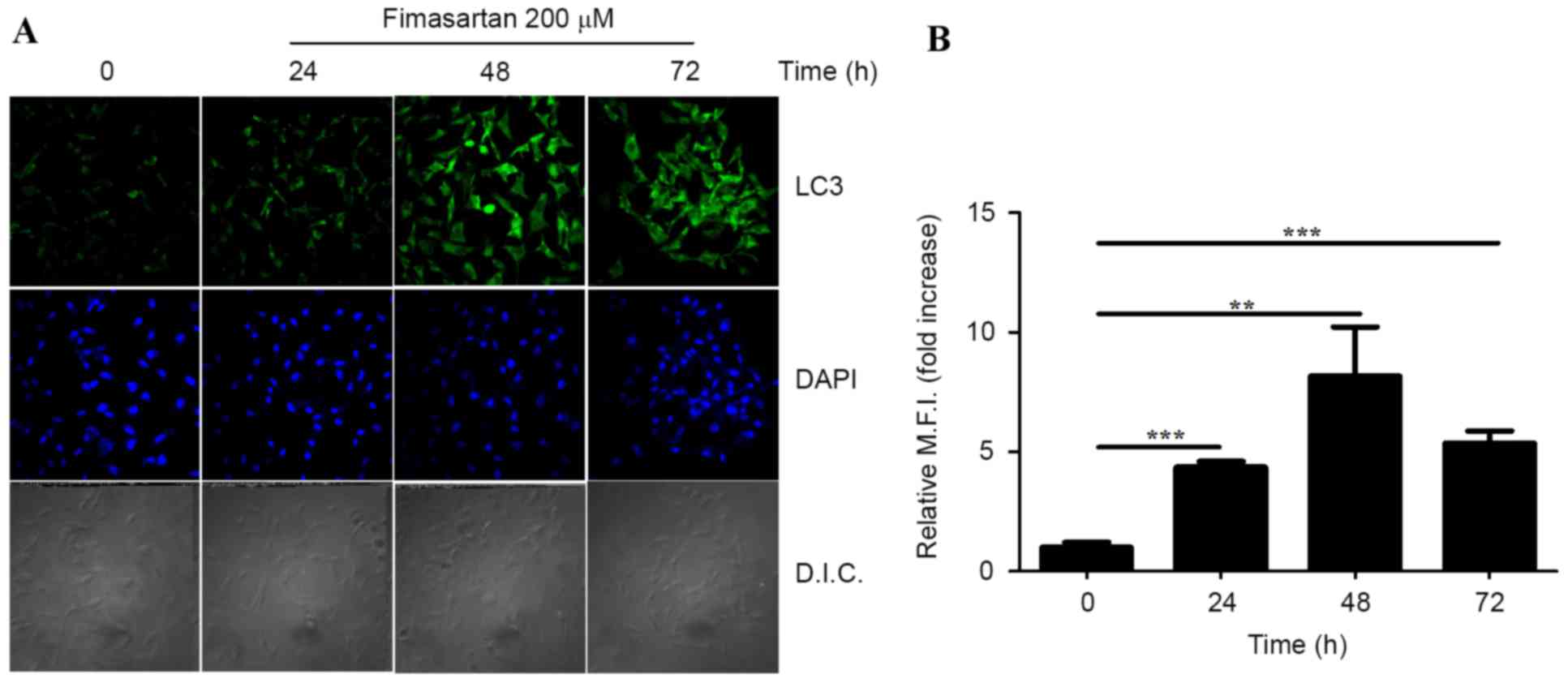 | Figure 3.Formation of LC3-positive foci in the
fimasartan-treated PC3 cells. (A) The PC3 cells were treated with
200 µM fimasartan for 24, 48 or 72 h, and endogenous LC3 was
detected using an immunofluorescence assay. Cells were stained with
DAPI to visualize the nuclei (blue), and immunolabeled with the
anti-LC3 antibody, with the addition of fluorescein
isothiocyanate-conjugated IgG (green). (B) The quantification for
the immunofluorescence images of 3 independent replicates. Values
are presented as the mean ± standard deviation. DAPI,
4,6′-diamidino-2-phenylindole; LC3, microtubule-associated protein
1A/1B-light chain 3; D.I.C, disseminated intravascular coagulation;
M.F.I, mean fluorescent intensity; **P<0.01, ***P<0.001. |
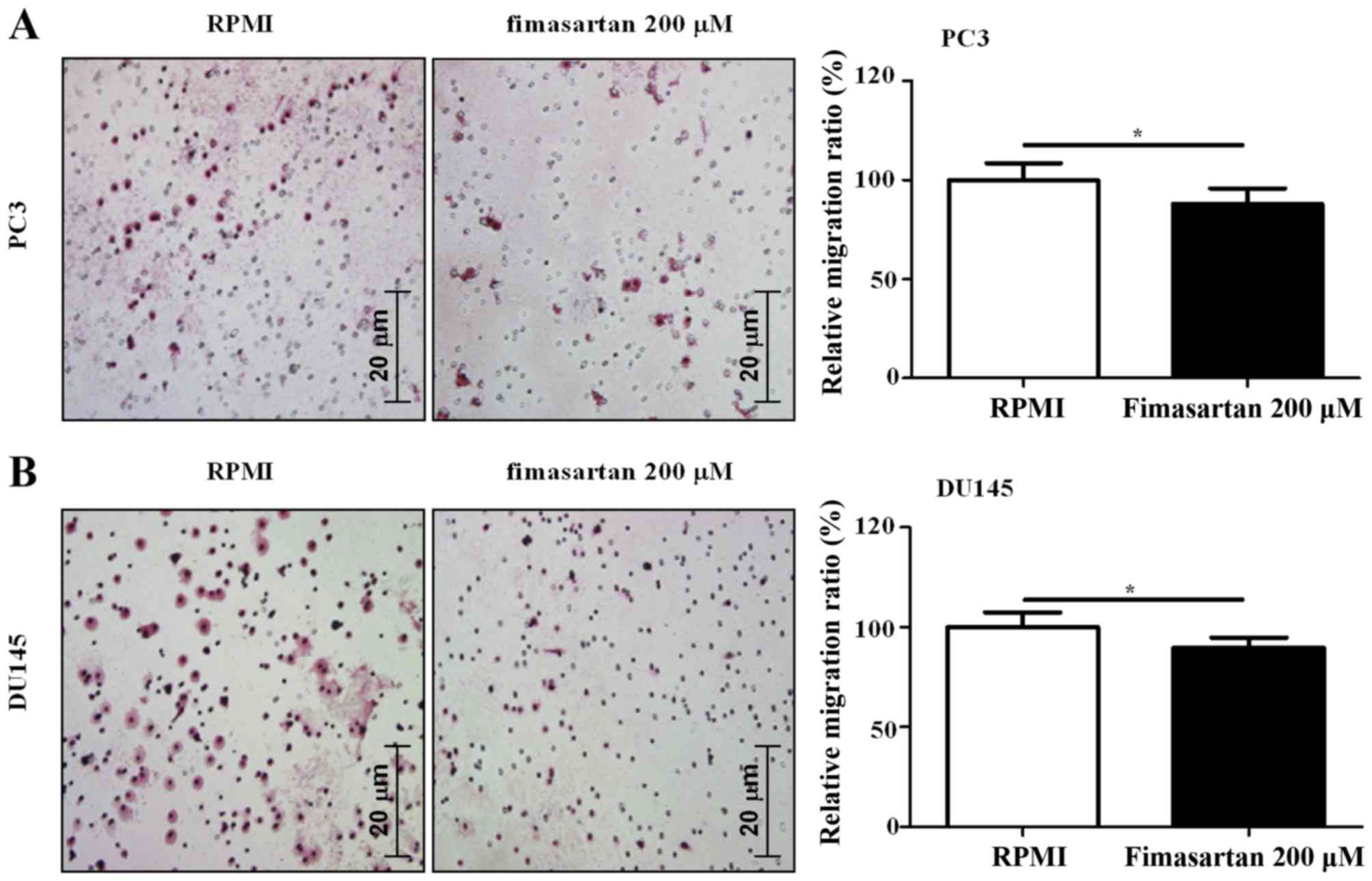
Anti-migratory effect of ARBs
A measurement of the potential of a compound to be
used as an anti-cancer agent is whether it exerts anti-migratory
effects on cancer cells. Therefore, an experiment was designed to
verify anti-migratory activity in PC3 and DU145 cells, using a
Transwell assay, to investigate whether fimasartan exerts a
suppressive effect on tumor metastasis. The results indicated that
treatment with 200 µM fimasartan induced anti-migratory activity in
PC3 and DU145 cells (0.88- and 0.90-fold increase, respectively;
Fig. 4). Thus, fimasartan may possess
the potential to be used as an anti-cancer agent for hypertensive
patients with prostate cancer.
Discussion
Multiple signaling pathways are activated in cells
stimulated by angiotensin II, including the Janus kinase/signal
transducer and activator of transcription Jak2/STAT, MAPK,
phosphoinositide 3 kinase/protein kinase B Akt and extracellular
growth factor signaling pathways, which may result in cell
proliferation, migration and tubulogenesis (34). This suggests that the treatment of
cancer cells with ARBs may inhibit the proliferation and migration
of tumor cells. The present study indicated that ARBs induce
autophagy in prostate cancer cells and may therefore be potential
anti-cancer agents. In addition, the present study suggests that
ARBs may be used as a therapeutic agent for patients with prostate
cancer and hypertension. However, the present study was unable to
ascertain whether autophagy is associated with the
antiproliferation and antimigration effects of ARBs on prostate
cancer cells. The induction of autophagy and inhibition of
proliferation by a 5′-adenosine monophospate-activated protein
kinase inhibitor, compound C, in human colorectal cancer cells has
been reported (35). In addition,
compound C has been reported to inhibit DNA-damage regulated
autophagy modulator 1 and p62, autophagy-associated factors, and to
regulate cell migration and invasion in glioblastoma (36). Furthermore, autophagy was induced in
mice injected with mitoxantrone leading to an anticancer immune
response (37). The aforementioned
studies suggest that ARBs may be potential antitumoral agents via
alterations in the autophagic process. The results of the present
study indicated that ARBs increased autophagy in prostate cancer
cell lines, supported by the increased expression levels of
autophagy-associated genes and observation of LC3-positive foci by
confocal microscopy. In addition, fimasartan exhibited superior
antitumor activity compared with losartan, eprosartan and
valsartan. Low concentrations (0.1, 1 and 10 µM) of ARBs did not
exhibit antitumor effects in prostate cancer cells in a preliminary
study (data not shown), therefore higher doses (100, 200 and 400
µM) of ARBs were used in the present study. These concentrations
were suitable for investigation, as previous studies have not
reported side effects in patients with hypertension prescribed
similar high doses of ARBs (38,39).
Considering the presence of other cells in the tumor
microenvironment in addition to the tumor cells, the degree of
influence of ARB treatment on cancer accessory cells, including
immune cells, should be considered. During tumor formation,
circulating monocytes infiltrate tumor tissue and polarize into
tumor-associated macrophages that express beneficial factors for
the tumor, including vascular endothelial growth factor and
arginase 1 (40). Therefore, it is
important to consider the effect of ARBs on the macrophages present
within the tumor tissue. Angiotensin II is a key mediator of
fibrosis in cardiac fibrosis, and enhances the infiltration of
macrophages into tissues and the subsequent polarization of the
cells into the M2 phenotype via serum-glucocorticoid-regulated
kinase 1 (41). As ARBs exhibited
potential in terms of weakening prostate cancer in clinical trials
(22–24), it may be suggested that the polarizing
of tumor-associated macrophages from monocytes may be inhibited by
ARB treatment. Therefore, the results of this study indicate that
ARBs possess the potential to be a novel therapeutic agent for
patients with prostate cancer and high blood pressure, since ARBs
induce autophagy and lead to anticancer effects in prostate cancer
cells.
Acknowledgements
The present study was supported by a National
Research Foundation of Korea grant funded by the Ministry of
Education, Science and Technology (grant no. 2012R1A1A2006349) and
Ministry of Science, ICT and Future Planning (grant nos.
2014M2B2A9030381 and 2015M2B2A6028602). Funding was also provided
by a 2015 (C1011746-01-01) and 2016 Research Grant from Kangwon
National University.
References
|
1
|
Daniels N: Global aging and the allocation
of health care across the life span. Am J Bioeth. 13:1–2. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Orom H, Penner LA, West BT, Downs TM,
Rayford W and Underwood W: Personality predicts prostate cancer
treatment decision-making difficulty and satisfaction.
Psychooncology. 18:290–299. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Guxens M, Fitó M, Martínez-González MA,
Salas-Salvadó J, Estruch R, Vinyoles E, Fiol M, Corella D, Arós F,
Gómez-Gracia E, et al: Hypertensive status and lipoprotein
oxidation in an elderly population at high cardiovascular risk. Am
J Hypertens. 22:68–73. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lin GM, Liu PY, Wu CF, Wang WB and Han CL:
Carvedilol use and specific cancer risk in the population with
hypertension. Int J Cardiol. 186:52–53. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mouhayar E and Salahudeen A: Hypertension
in cancer patients. Tex Heart Inst J. 38:263–265. 2011.PubMed/NCBI
|
|
6
|
Valcamonico F, Arcangeli G, Consoli F,
Nonnis D, Grisanti S, Gatti E, Berruti A and Ferrari V: Idiopathic
intracranial hypertension: A possible complication in the natural
history of advanced prostate cancer. Int J Urol. 21:335–337. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tahover E, Uziely B, Salah A, Temper M,
Peretz T and Hubert A: Hypertension as a predictive biomarker in
bevacizumab treatment for colorectal cancer patients. Med Oncol.
30:3272013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pant S, Martin LK, Geyer S, Wei L, Van
Loon K, Sommovilla N, Zalupski M, Iyer R, Fogelman D, Ko AH and
Bekaii-Saab T: Treatment-related hypertension as a pharmacodynamic
biomarker for the efficacy of bevacizumab in advanced pancreas
cancer: A pooled analysis of 4 prospective trials of
gemcitabine-based therapy with bevacizumab. Am J Clin Oncol.
39:614–618. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang J, Liu J, Chen J, Li X, Wu Y, Chen
H, Wu W, Zhang K and Gu L: Angiotensin receptor blockers (ARBs)
reduce the risk of lung cancer: A systematic review and
meta-analysis. Int J Clin Exp Med. 8:12656–12660. 2015.PubMed/NCBI
|
|
10
|
Chae YK, Valsecchi ME, Kim J, Bianchi AL,
Khemasuwan D, Desai A and Tester W: Reduced risk of breast cancer
recurrence in patients using ACE inhibitors, ARBs, and/or statins.
Cancer Invest. 29:585–593. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mann SJ and Christos PJ: ACE inhibitors
and ARBs: Do they reduce the risk of cancer? J Clin Hypertens
(Greenwich). 16:6–7. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sigmund CD: Structural biology: On stress
and pressure. Nature. 468:46–47. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Asmar R: Targeting effective blood
pressure control with angiotensin receptor blockers. Int J Clin
Pract. 60:315–320. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
van Zwieten PA: Angiotensin II receptor
antagonists (AT1-blockers, ARBs, sartans): Similarities and
differences. Neth Heart J. 14:381–387. 2006.PubMed/NCBI
|
|
15
|
Imai N, Hashimoto T, Kihara M, Yoshida S,
Kawana I, Yazawa T, Kitamura H and Umemura S: Roles for host and
tumor angiotensin II type 1 receptor in tumor growth and
tumor-associated angiogenesis. Lab Invest. 87:189–198. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rodrigues-Ferreira S, Abdelkarim M,
Dillenburg-Pilla P, Luissint AC, di-Tommaso A, Deshayes F, Pontes
CL, Molina A, Cagnard N, Letourneur F, et al: Angiotensin II
facilitates breast cancer cell migration and metastasis. PLoS One.
7:e356672012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kosugi M, Miyajima A, Kikuchi E, Horiguchi
Y and Murai M: Angiotensin II type 1 receptor antagonist
candesartan as an angiogenic inhibitor in a xenograft model of
bladder cancer. Clin Cancer Res. 12:2888–2893. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rodrigues-Ferreira S, Morel M, Reis RI,
Cormier F, Baud V, Costa-Neto CM and Nahmias C: A novel cellular
model to study angiotensin II AT2 receptor function in breast
cancer cells. Int J Pept. 2012:7450272012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Carl-McGrath S, Ebert MP, Lendeckel U and
Röcken C: Expression of the local angiotensin II system in gastric
cancer may facilitate lymphatic invasion and nodal spread. Cancer
Biol Ther. 6:1218–1226. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Matsuyama M, Funao K, Kuratsukuri K,
Tanaka T, Kawahito Y, Sano H, Chargui J, Touraine JL, Yoshimura N
and Yoshimura R: Telmisartan inhibits human urological cancer cell
growth through early apoptosis. Exp Ther Med. 1:301–306.
2010.PubMed/NCBI
|
|
21
|
Uemura H, Ishiguro H, Nakaigawa N,
Nagashima Y, Miyoshi Y, Fujinami K, Sakaguchi A and Kubota Y:
Angiotensin II receptor blocker shows antiproliferative activity in
prostate cancer cells: A possibility of tyrosine kinase inhibitor
of growth factor. Mol Cancer Ther. 2:1139–1147. 2003.PubMed/NCBI
|
|
22
|
Uemura H, Hoshino K and Kubota Y: Role of
renin-angiotensin system and antitumor effect of ARB in prostate
cancer. Nihon Rinsho. 69:(Suppl 5). S155–S159. 2011.(In
Japanese).
|
|
23
|
Uemura H and Kubota Y: Application of
angiotensin II receptor blocker in prostate cancer. Nihon Rinsho.
67:807–811. 2009.(In Japanese). PubMed/NCBI
|
|
24
|
Funao K, Matsuyama M, Kawahito Y, Sano H,
Chargui J, Touraine JL, Nakatani T and Yoshimura R: Telmisartan is
a potent target for prevention and treatment in human prostate
cancer. Oncol Rep. 20:295–300. 2008.PubMed/NCBI
|
|
25
|
Burikhanov R, Zhao Y, Goswami A, Qiu S,
Schwarze SR and Rangnekar VM: The tumor suppressor Par-4 activates
an extrinsic pathway for apoptosis. Cell. 138:377–388. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Okada H and Mak TW: Pathways of apoptotic
and non-apoptotic death in tumour cells. Nat Rev Cancer. 4:592–603.
2004. View
Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kelly GL and Strasser A: The essential
role of evasion from cell death in cancer. Adv Cancer Res.
111:39–96. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kondo Y, Kanzawa T, Sawaya R and Kondo S:
The role of autophagy in cancer development and response to
therapy. Nat Rev Cancer. 5:726–734. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mathew R, Karantza-Wadsworth V and White
E: Role of autophagy in cancer. Nat Rev Cancer. 7:961–967. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kang SJ, Tak JH, Cho JH, Lee HJ and Jung
YJ: Stimulation of the endosomal TLR pathway enhances
autophagy-induced cell death in radiotherapy of breast cancer.
Genes & Genomics. 32:599–606. 2010. View Article : Google Scholar
|
|
31
|
Bose SK, Gibson W, Giri S, Nath N and
Donald CD: Angiotensin II up-regulates PAX2 oncogene expression and
activity in prostate cancer via the angiotensin II type I receptor.
Prostate. 69:1334–1342. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Schweichel JU and Merker HJ: The
morphology of various types of cell death in prenatal tissues.
Teratology. 7:253–266. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kroemer G and Levine B: Autophagic cell
death: The story of a misnomer. Nat Rev Mol Cell Biol. 9:1004–1010.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yosypiv IV, Schroeder M and El-Dahr SS:
Angiotensin II type 1 receptor-EGF receptor cross-talk regulates
ureteric bud branching morphogenesis. J Am Soc Nephrol.
17:1005–1014. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yang WL, Perillo W, Liou D, Marambaud P
and Wang P: AMPK inhibitor compound C suppresses cell proliferation
by induction of apoptosis and autophagy in human colorectal cancer
cells. J Surg Oncol. 106:680–688. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Galavotti S, Bartesaghi S, Faccenda D,
Shaked-Rabi M, Sanzone S, McEvoy A, Dinsdale D, Condorelli F,
Brandner S, Campanella M, et al: The autophagy-associated factors
DRAM1 and p62 regulate cell migration and invasion in glioblastoma
stem cells. Oncogene. 32:699–712. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Michaud M, Martins I, Sukkurwala AQ,
Adjemian S, Ma Y, Pellegatti P, Shen S, Kepp O, Scoazec M, Mignot
G, et al: Autophagy-dependent anticancer immune responses induced
by chemotherapeutic agents in mice. Science. 334:1573–1577. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Konstam MA, Neaton JD, Dickstein K,
Drexler H, Komajda M, Martinez FA, Riegger GA, Malbecq W, Smith RD,
Guptha S, et al: Effects of high-dose versus low-dose losartan on
clinical outcomes in patients with heart failure (HEAAL study): A
randomised, double-blind trial. Lancet. 374:1840–1848. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Abe M, Okada K, Maruyama T, Matsumoto S
and Matsumoto K: Blood pressure-lowering and antiproteinuric effect
of switching from high-dose angiotensin receptor blockers to
normal-dose telmisartan and low-dose hydrochlorothiazide in
hypertensive patients with chronic kidney disease. Int J Clin
Pharmacol Ther. 48:206–213. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
40
|
Colegio OR, Chu NQ, Szabo AL, Chu T,
Rhebergen AM, Jairam V, Cyrus N, Brokowski CE, Eisenbarth SC,
Phillips GM, et al: Functional polarization of tumour-associated
macrophages by tumour-derived lactic acid. Nature. 513:559–563.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yang M, Zheng J, Miao Y, Wang Y, Cui W,
Guo J, Qiu S, Han Y, Jia L, Li H, et al: Serum-glucocorticoid
regulated kinase 1 regulates alternatively activated macrophage
polarization contributing to angiotensin II-induced inflammation
and cardiac fibrosis. Arterioscler Thromb Vasc Biol. 32:1675–1686.
2012. View Article : Google Scholar : PubMed/NCBI
|