Introduction
Breast cancer is the leading cause of
cancer-associated mortality in women worldwide; ~1.38 million new
breast cancer cases and ~0.46 million breast cancer-associated
mortalities were estimated to have occurred in 2014 (1). In China, the incidence has increased
more than twice as fast as global rates since the 1990s, and is now
the most frequently diagnosed cancer and the sixth leading cause of
cancer-associated mortality among Chinese women (2). Despite an increase in the five-year
survival rate of breast cancer, as a result of early diagnosis and
improved local and systemic treatment over the last 20 years,
long-term prognosis remains unsatisfactory, mainly due to the
recurrence and invasion rates following resection (3). However, little is known about this
aggressive behavior. Finding new favorable prognostic biomarkers
may help to predict the properties of the malignancy, thus
decreasing the rate of unsatisfied outcomes in a high-risk
population.
The oncogenic enzyme sphingosine kinase (SPHK)
catalyzes the phosphorylation of sphingosine to form
sphingosine-1-phosphate, which is suggested to be a bioactive lipid
mediator that serves a vital role in regulating various biological
processes during tumorigenesis (4).
Two functional SPHK isoenzymes, SPHK1 and SPHK2, have been
identified in humans (5). Multiple
lines of evidence indicate that SPHK1 regulates various processes
important for cancer progression (6,7); however,
there are limited studies regarding biological functions of SPHK2
in cancer, and it remains unclear whether SPHK1 and SPHK2 have
redundant, overlapping, complementary or antagonistic functions in
human cancer cells. A previous study showed that downregulation of
SPHK2 in MDA-MB-453 breast cancer cells completely eliminated
migration towards epidermal growth factor (EGF), suggesting it is
similar to SPHK1 (8). Other studies
hypothesized that overexpression of SPHK2 suppresses growth and
enhances apoptosis, preceded by cytochrome c release and
activation of caspase-3 (9,10), indicating that the two isoenzymes have
opposite effects. An additional study suggested that non-small cell
lung cancer patients with higher SPHK2 expression had a shorter
overall survival (OS) time (11). The
present study was only focused on the role of SPHK1, instead of
SPHK2, in breast cancer long-term survival, since there are a
larger number of studies providing evidence of its role in patients
with cancer prognosis, thereby supporting the hypothesis.
SPHK1 mRNA has been revealed to be frequently
overexpressed in a variety of human solid tumors (12). Other studies have demonstrated that
SPHK1 protein expression is unregulated in various types of cancer,
including prostate cancer (13),
gastric cancer (14), glioblastoma
multiforme (15), intestinal adenoma
(16), acute erythroleukemia
(17), colon cancer (18), salivary gland carcinoma (19) and glioma (20). In addition, there is plenty of
evidence indicating that activation of SPHK1 is associated with
anti-apoptosis effects, and the transformation, proliferation and
survival of tumor cells (21,22). Furthermore, while SPHK1 activity may
be stimulated by a variety of cellular stimuli, and anticancer
treatments may cause downregulation of SPHK1 activity, it has been
suggested that the SPHK1 inhibitors camptothecin and docetaxel
suppress tumor growth as well as reduce the occurrence and number
of metastases in nude mice (23).
A previous study reported that downregulation of
SPHK1 in MCF-7 cells could reduce EGF- and serum-stimulated growth
and enhance sensitivity to doxorubicin (a potent chemotherapeutic
agent), suggesting that SPHK1 may perform an important role in the
migration of MCF-7 cells (24).
Increased expression of SPHK1 has been detected in triple-negative
human breast tumors compared with receptor-positive tumors, and the
SPHK1 ectopic expression is associated with poor overall and
progression-free survival in breast cancer patients, as well as
poor response to doxorubicin-based treatment (25). These observations propose that SPHK1
may be involved in cell growth and transformation in cancer
progression.
However, there are limited studies connecting a
comprehensive investigation of the expression and significance of
SPHK1 with the long-time prognosis in patients with breast cancer
in China. In the present study, the expression of SPHK1 was
assessed in mRNA and protein levels in breast cancer tissues and
compared with the clinicopathological parameters and survival of
patients in 122 breast cancer patients. The present results
indicated that SPHK1 may be a promising potential biomarker for
predicting the prognosis of patients with breast cancer and a
promising new target for breast cancer therapy.
Materials and methods
Patients and specimens
The analysis of human tissues was approved by the
Human Research Ethical Committee of Chongqing Medical University
(CQMU; Chongqing, China). Informed consent was obtained from all
patients or their relatives. A total of 32 breast tumors and paired
surgical-margin tissues (>1 cm away from the tumor area) were
obtained from the First Affiliated Hospital of CQMU (Chongqing,
China). Tissues to be subjected to RNA extraction were frozen in
liquid nitrogen. Tissue samples from 122 patients who underwent
surgical resection for primary invasive breast cancer at the First
Affiliated Hospital of CQMU between December 2006 and November 2013
were collected. All samples were evaluated and subject to
histological diagnosis by pathologists. Subsequent to surgery, the
majority of patients were treated with the standard practice
guidelines at that time and were followed up regularly. In total,
15 normal breast specimens were obtained from the defect border
while removing a benign breast tumor using the Mammotome biopsy
technique (26). Formalin-fixed,
paraffin-embedded materials were used for routine staining with
hematoxylin and eosin (H&E; Zhongshan Jinqiao, Beijing, China)
and for staining by immunohistochemical techniques. Grading of
tumors was achieved by staining with H&E.
RNA extraction and reverse
transcription-quantitative polymerase chain reaction (RT-qPCR)
Total RNA was isolated from the tissue of patients
using TRIzol reagent (Molecular Research Center, Cincinnati, OH,
USA). Levels of RNA expression were determined using the 7500 Fast
System SDS software package (version 1.3.1; Applied Biosystems;
Thermo Fisher Scientific, Inc., Waltham, MA, USA).
RT-qPCR was performed in triplicate with an Applied
Biosystems Prism 7500 Fast Sequence Detection System (Thermo Fisher
Scientific, Inc., USA) using Takara universal PCR master mix,
according to the manufacturer's protocol (Takara Bio, Inc., Otsu,
Japan). Primers were purchased from Shanghai Shenggong Genetech Co.
(Shanghai, China). β-actin was used as an endogenous control.
Melting curve analysis was performed to verify specificity of PCR
products. In addition, PCR products were electrophoresed on 2%
agarose gel to confirm product sizes and specificity. The sequences
were as follows: SPHK1 forward, 5′-CTTGCAGCTCTTCCGGAGTC-3′ and
reverse, 5′-GCTCAGTGAGCATCAGCGTG-3′; and β-actin forward,
5′-TCCTGTGGCATCCACGAAACT-3′ and reverse,
5′-GAAGCATTTGCGGTGGACGAT-3′. Reaction conditions were set as
follows: 95°C for 30 sec; followed by 40 cycles of 95°C for 5 sec;
and 60°C for 34 sec. The association stage was set to check the
specificity of primers as follows: 95°C for 15 sec; followed by
60°C for 1 min; 95°C for 15 sec; and then 60°C for 15 sec. Each
sample was performed in triplicate in a 20 µl reaction volume.
Relative quantification of gene expression was performed using the
2−ΔΔCq calculation formula, based on Cq values for
target and reference genes (27).
Immunohistochemistry
A rabbit polyclonal antibody against human SPHK1
(cat. no., ab16491; dilution, 1:300; Abgent, Inc., San Diego, CA,
USA) was used. Immunohistochemistry was performed using a two-step
method. Sections (4 µm) were deparaffinized by 100% xylene (4
times, 10 min each) and rehydrated in a series of ethanol (100, 95,
85 and 70% for 2 min each). The sections were hydrated and
underwent sodium citrate (pH 6.0) antigen retrieval. Antigen
retrieval was performed for 15 min in a microwave by intermittent
heating to avoid boiling buffer, which may damage the tissue or
dislodge it from the slide. Endogenous peroxidase activities were
blocked by 3% hydrogen peroxide. The sections were then incubated
with the primary antibody (cat. no., SP-9000; dilution, 1:250;
Zhongshan Jinqiao) overnight for 18 h at 4°C, followed by
incubation with horseradish peroxidase-conjugated goat anti-rabbit
immunoglobulin G secondary antibody (cat. no., SP-9000; dilution,
1:1,000; Zhongshan Jinqiao) at 37°C for 1 h. Finally, slides were
counterstained with hematoxylin. To eliminate nonspecific staining,
a negative control was performed by replacing the primary antibody
with PBS.
All staining was assessed by two pathologists
blinded to the origination of the samples and subject outcome. The
widely accepted German semi-quantitative scoring system was used to
assess the staining intensity and area extent (28). Each specimen was assigned a score
according to the intensity of the nucleic, cytoplasmic and/or
membrane staining (no staining, 0; weak staining, 1; moderate
staining, 2; and strong staining, 3; and the extent of stained
cells (0%, 0; 1–24%, 1; 25–49%, 2; 50–74%, 3; and 75–100%, 4). The
final score was calculated by multiplying the intensity score with
the extent of staining score, ranging between 0 (the minimum score)
and 12 (the maximum score). Scores ≥8 were defined as high
expression and scores <8 were defined as low expression.
Outcome of patients
Following a median follow-up of 56.5 months (7–106
months), 41 recurrence or metastasis cases and 22 mortalities
occurred in all patients.
Statistical analysis
Statistical analysis was performed using SPSS 17.0
software (SPSS, Inc., Chicago, IL, USA). The OS time was counted
from the date of diagnosis being confirmed as breast carcinoma to
the date of last follow-up or mortality. Disease-free survival
(DFS) time was calculated from the date of confirmed diagnosis to
the date of last follow-up or metastatic diseases. χ2
and Fisher's exact tests were used to compare variables. Survival
analysis was performed using the log-rank test, and survival plots
were created using Kaplan-Meier methods. Multivariate analysis was
performed using Cox proportional hazard regression analysis. All
P-values reported were two-sided, and P<0.05 was considered to
indicate a statistically significant difference.
Results
Demographic and clinicopathological
features
To validate the association between SPHK1,
clinicopathological parameters and clinical outcome, an independent
cohort of breast cancers with follow-up information was included in
the present study. A total of 122 consecutive breast cancer
specimens were collected, including 9 of carcinoma in situ
and 113 of invasive ductal carcinoma. The mean age of the total
patients enrolled was 52 years, ranging from 27–75 years.
Histological types of the total 122 samples were defined according
to the World Health Organization classification criteria (2007)
into grade I (9 cases), grade II (76 cases), grade III (11 cases)
and 26 cases with missing data.
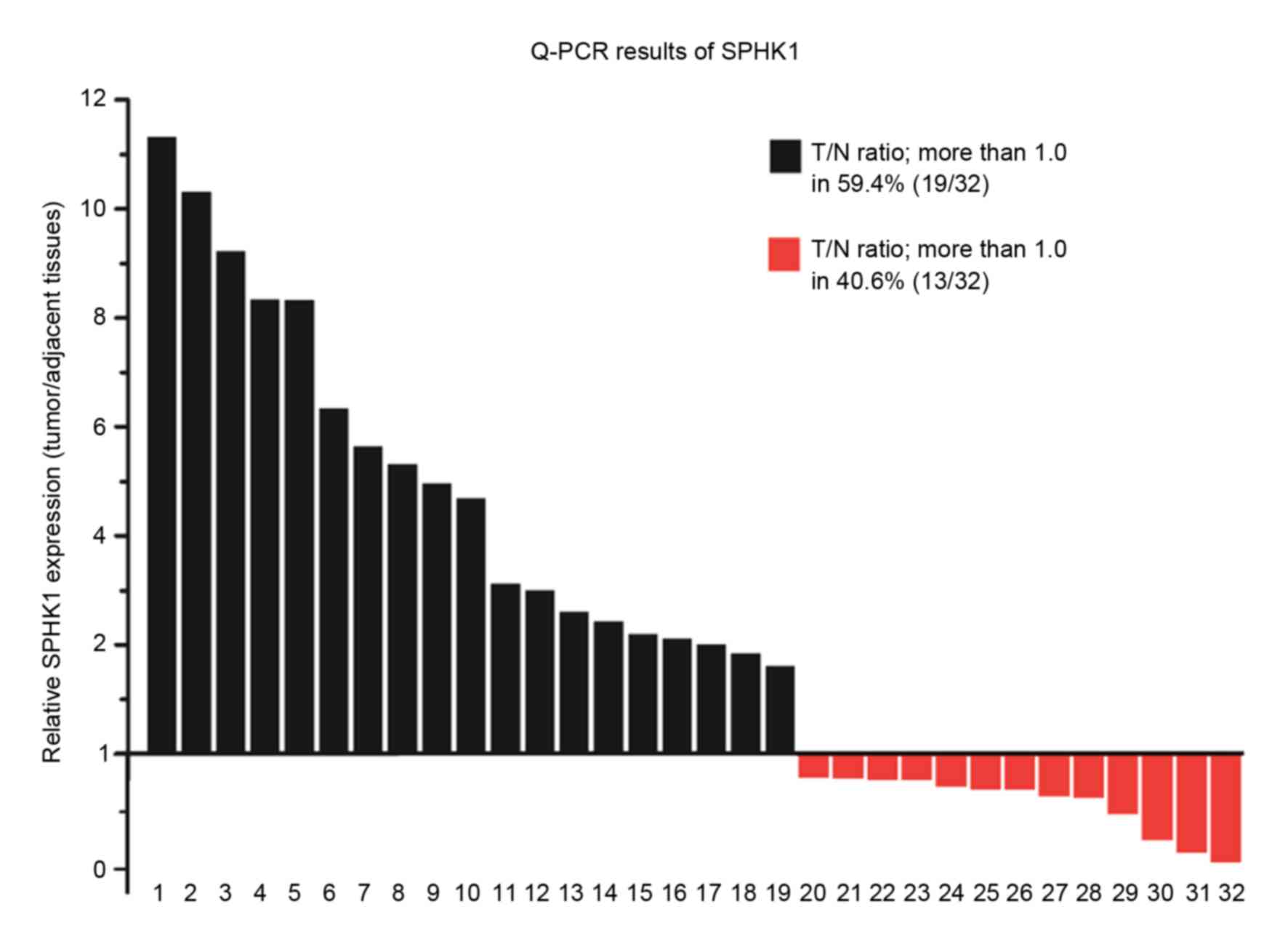
SPHK1 mRNA expression
The mRNA level of SPHK1 in 32 tissues of patients,
determined by RT-qPCR, revealed that the gene expression level of
SPHK1 was significantly upregulated (P<0.0001). SPHK1 mRNA
expression was upregulated [tumor/normal (T/N) ratio >1] in
breast cancer tissues compared with that in matched adjacent breast
tissues (expression=1) in 19 of 32 paired tissue specimens (59.4%).
In 13 of 32 specimens (40.6%), SPHK1 was downregulated (T/N ratio
>1; Fig. 1).
SPHK1 immunostaining
Immunohistochemical analysis was performed using 122
paraffin-embedded breast cancer tissue blocks to evaluate the
expression of the SPHK1 protein. Negative staining was examined in
all 15 normal breast cases (data not shown). Examples of the
different SPHK1 staining of breast tumors are shown in Fig. 2, according to aforementioned methods.
Positive staining for SPHK1 was mainly observed in the cytoplasm of
the breast cancer cells. Among the 122 breast carcinomas, weak
staining was observed in 26 specimens (21.3%), moderate expression
was observed in 57 (46.7%) and strong staining was observed in 39
(32.0%).
Association between SPHK1 expression
and clinicopathological features
The association between the expression of SPHK1 and
various clinicopathological parameters is listed in Table I. A significant association was
observed between the high and low expression groups in the presence
of lymph node metastasis (P=0.0016), number of positive lymph nodes
(P=0.0268) and presence of distant metastasis (P=0.0097). High
SPHK1 expression was also associated with human epidermal growth
factor receptor 2 (HER2) status (P=0.0100), initial symptoms
(P=0.0025) and tumor location (P=0.0457). However, no significant
association was observed between the expression level of SPHK1 and
age, times of pregnancy, age at menarche, tumor histological types,
histological grade, tumor size or hormonal receptor (HR; estrogen
receptor or progesterone receptor) status. There was also no
significant difference in SPHK1 expression among the different
intrinsic subtypes of breast cancer, as defined by the St Gallen
consensus conference (29). These
data showed that the expression of SPHK1 increases as breast cancer
clinically progresses, but cancer intrinsic subtypes do not appear
to be associated with the level of SPHK1 expression in the samples
included in the present study.
 | Table I.Main characteristics of patients with
breast cancer, and the association between the SPHK1 and
clinicopathological parameters (n=122). |
Table I.
Main characteristics of patients with
breast cancer, and the association between the SPHK1 and
clinicopathological parameters (n=122).
|
|
| SPHK1
expression |
|
|
|---|
|
|
|
|
|
|
|---|
| Features | No. | High, n (%) | Low, n (%) | χ2 | P-value |
|---|
| Age, |
|
|
| 2.6011 | 0.1068 |
| <60
years | 93 | 45 (36.9) | 48 (39.3) |
|
|
| ≥60
years | 29 | 19 (15.6) | 10 (8.2) |
|
|
| Gravidity |
|
|
| 0.8801 | 0.9321 |
| 1 | 60 | 30 (24.6) | 30 (24.6) |
|
|
| 2 | 22 | 12 (9.8) | 10 (8.2) |
|
|
| 3 | 7 | 4 (3.3) | 3 (2.5) |
|
|
| 4 | 11 | 7 (5.7) | 4 (3.3) |
|
|
| ≥5 | 5 | 3 (2.5) | 2 (1.6) |
|
|
|
Unknown | 17 | 7 (5.7) | 10 (8.2) |
|
|
| Age at menarche,
years |
|
|
| 2.8928 | 0.4171 |
|
≤12 | 14 | 5 (4.1) | 11 (9.0) |
|
|
|
13–14 | 78 | 40 (32.8) | 38 (31.1) |
|
|
|
15–16 | 15 | 9 (7.4) | 6 (4.9) |
|
|
|
≥17 | 6 | 3 (2.5) | 3 (2.5) |
|
|
| Missing
data | 7 | 7 (5.7) | 0 (0) |
|
|
| Initial
symptoms |
|
|
| 14.3048 | 0.0025a |
|
Lump | 92 | 39 (32.0) | 53 (43.5) |
|
|
|
Pain | 13 | 12 (9.8) | 1 (0.8) |
|
|
| Nipple
changes | 5 | 2 (1.6) | 3 (2.5) |
|
|
|
Clinical screening | 6 | 5 (4.1) | 1 (0.8) |
|
|
|
Unknown | 6 | 6 (4.9) | 0 (0) |
|
|
| Tumor location |
|
|
| 5.3123 | 0.0457a |
|
Right | 61 | 26 (21.3) | 35 (28.7) |
|
|
|
Left | 60 | 37 (30.3) | 23 (18.9) |
|
|
|
Both-sides | 1 | 1 (0.8) | 0 (0) |
|
|
| Tumor
histology |
|
|
| 0.7865 | 0.3752 |
|
Carcinomas in situ | 9 | 6 (4.9) | 3 (2.5) |
|
|
|
Invasive carcinomas | 113 | 58 (47.5) | 55 (45.1) |
|
|
| Types of invasive
carcinomas |
|
|
| 5.5517 | 0.0843 |
|
Ductal | 97 | 53 (46.9) | 44 (38.9) |
|
|
|
Lobular | 4 | 2 (1.8) | 2 (1.8) |
|
|
|
Mucinous adenocarcinoma | 5 | 0 (0) | 5 (4.4) |
|
|
|
Cephaloma | 2 | 1 (0.9) | 1 (0.9) |
|
|
|
Others | 5 | 2 (1.8) | 3 (2.6) |
|
|
| Histological
grade |
|
|
| 2.9182 | 0.2531 |
| I | 10 | 8 (6.6) | 2 (1.6) |
|
|
| II | 70 | 38 (31.1) | 32 (26.3) |
|
|
|
III | 11 | 5 (4.1) | 6 (4.9) |
|
|
|
Unknown | 31 | 10 (8.2) | 21 (17.2) |
|
|
| Tumor size, cm |
|
|
| 0.4706 | 0.8883 |
|
<2.0 | 36 | 15 (12.2) | 11 (9.0) |
|
|
| ≥2.0
and ≤5.0 | 78 | 39 (32.0) | 39 (32.0) |
|
|
|
>5.0 | 6 | 3 (2.5) | 3 (2.5) |
|
|
|
Unknown | 12 | 6 (4.9) | 6 (4.9) |
|
|
| Lymph nodes
status |
|
|
| 10.3477 | 0.0013a |
|
Positive | 62 | 41 (33.6) | 21 (17.2) |
|
|
|
Negative | 55 | 20 (16.4) | 35 (28.7) |
|
|
|
Unknown | 5 | 3 (2.5) | 2 (1.6) |
|
|
| No. of positive
lymph nodes |
|
|
| 7.2395 | 0.0268a |
|
<5 | 92 | 42 (34.4) | 50 (41.0) |
|
|
|
5–10 | 16 | 11 (9.0) | 5 (4.1) |
|
|
|
>10 | 14 | 11 (9.0) | 3 (2.5) |
|
|
| Distant
metastasis |
|
|
| 8.8374 | 0.0030a |
|
Positive | 32 | 24 (19.7) | 8 (6.5) |
|
|
|
Negative | 90 | 40 (32.8) | 50 (41.0) |
|
|
| ER status |
|
|
| 0.0104 | 0.9186 |
|
Positive | 57 | 29 (23.8) | 26 (21.3) |
|
|
|
Negative | 52 | 29 (23.8) | 25 (20.5) |
|
|
|
Unknown | 13 | 6 (4.9) | 7 (5.7) |
|
|
| PR status |
|
|
| 1.2539 | 0.2628 |
|
Positive | 38 | 23 (18.9) | 15 (12.3) |
|
|
|
Negative | 71 | 35 (28.7) | 36 (29.5) |
|
|
|
Unknown | 13 | 6 (4.9) | 7 (5.7) |
|
|
| HER2 status |
|
|
| 6.6422 | 0.0100a |
|
Positive | 44 | 30 (24.6) | 14 (11.5) |
|
|
|
Negative | 65 | 28 (23.0) | 37 (30.3) |
|
|
|
Unknown | 13 | 6 (4.9) | 7 (5.7) |
|
|
| P53 status |
|
|
| 0.0778 | 0.7803 |
|
Positive | 37 | 19 (15.6) | 18 (14.8) |
|
|
|
Negative | 72 | 39 (32.0) | 33 (27.0) |
|
|
|
Unknown | 13 | 6 (4.9) | 7 (5.7) |
|
|
| Intrinsic
subtype |
|
|
| 1.5973 | 0.6600 |
| Luminal
A | 54 | 28 (23.0) | 26 (21.3) |
|
|
| Luminal
B | 7 | 4 (3.3) | 3 (2.5) |
|
|
| HER2
type | 5 | 4 (3.3) | 1 (0.8) |
|
|
|
Basal-like | 43 | 22 (18.0) | 21 (17.2) |
|
|
|
Undefined | 13 | 6 (4.9) | 7 (5.7) |
|
|
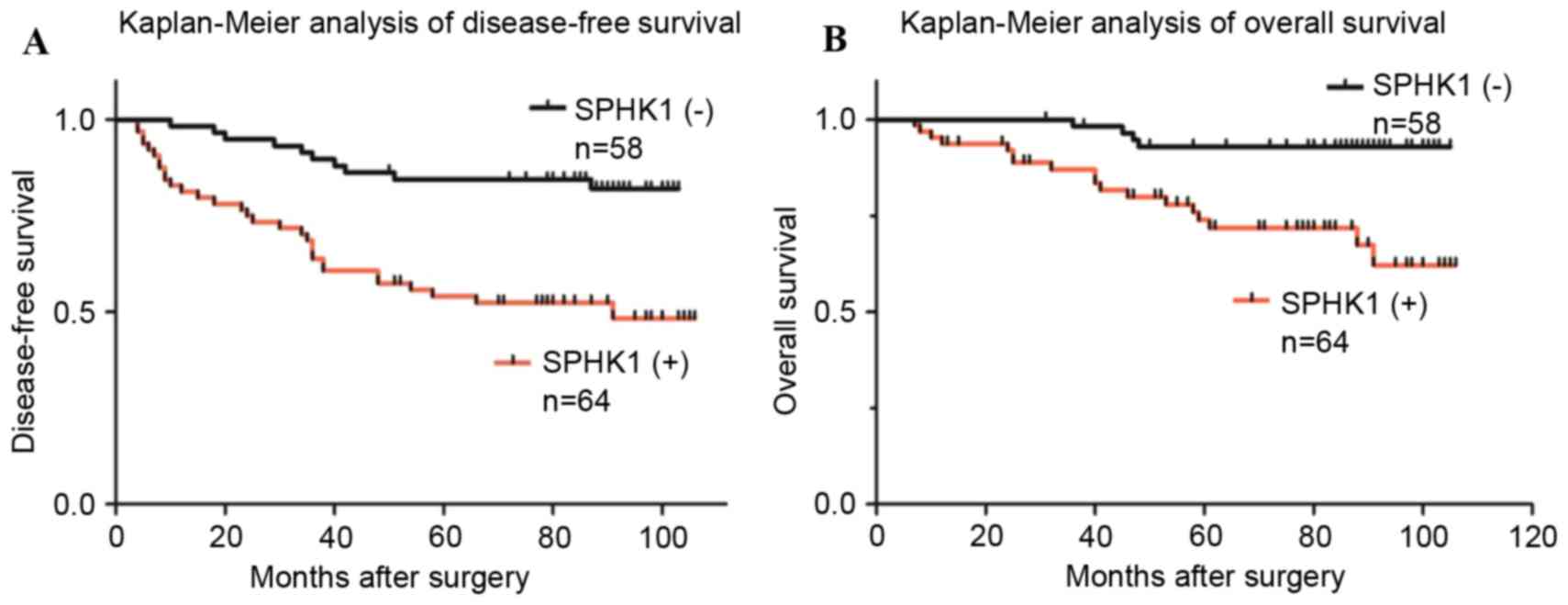
SPHK1 expression and survival of
patients
Survival curves plotted using the Kaplan-Meier
method demonstrated that increased expression of SPHK1 was
associated with a decrease in OS and DFS (Fig. 3). Statistical analysis of the impact
of classic clinicopathological features and protein expression by
the log-rank (Mantel-Cox) test revealed that patients with
SPHK1-positive tumors had a significantly poorer prognosis than
those with SPHK1-negative tumors (P<0.05). Other features
associated with decreased survival were lymph node status, distant
metastasis, HER2 status and intrinsic subtype, whereas other
clinicopathological variables were not significant (Table II). By multivariate analysis, high
SPHK1 expression was independently associated with greater
cancer-specific OS (HR, 0.196; 95% CI, 0.058–0.655; P=0.0081;
Table III).
| Table II.Survival of patients associated with
clinicopathological features and biomarkers. |
Table II.
Survival of patients associated with
clinicopathological features and biomarkers.
| Variables | Patients | Events | DFS rate, % | Median ± SE | P (log-rank) | Events | OS rate, % | Median ± SE | P (log-rank) |
|---|
| Age |
|
|
|
| 0.0938 |
|
|
| 0.0888 |
| <60
years | 93 | 13 | 14.0 | 84±2.6695592 |
| 8 | 8.6 | 84±3.1875801 |
|
| >60
years | 29 | 28 | 96.6 | 70±5.4070979 |
| 14 | 48.3 | 70±6.3744223 |
|
| Tumor size |
|
|
|
| 0.2281 |
|
|
| 0.3939 |
|
<2.0 | 36 | 3 | 8.3 | 87±5.6198349 |
| 5 | 13.9 | 87±4.5836602 |
|
| ≥2.0
and ≤5.0 | 78 | 16 | 20.5 | 82±3.6060642 |
| 26 | 33.3 | 82±3.0635466 |
|
|
>5.0 | 6 | 2 | 33.3 | 73±16.0603030 |
| 3 | 50 | 75±12.8443676 |
|
|
Unknown | 12 | 1 | 8.3 | NA |
| 7 | 58.3 | NA |
|
| Lymph node
status |
|
|
|
|
<0.0001a |
|
|
| 0.0062a |
|
Positive | 62 | 7 | 11.3 | 87±2.0293832 |
| 5 | 8.1 | 87±2.6739158 |
|
|
Negative | 55 | 31 | 56.4 | 63±3.8471953 |
| 14 | 25.5 | 53±4.4754747 |
|
|
Unknown | 5 | 3 | 60 | NA |
| 3 | 60 | NA |
|
| Distant
metastasis |
|
|
|
|
<0.0001a |
|
|
|
<0.0001a |
|
Positive | 32 | 32 | 100 | 87±2.4340914 |
| 22 | 68.8 | 88±2.0415520 |
|
|
Negative | 90 | 9 | 0.03 | 27±3.5732850 |
| 0 | 0 | 40.5±3.7709387 |
|
| ER status |
|
|
|
| 0.0822 |
|
|
| 0.2415 |
|
Positive | 57 | 16 | 28.1 | 87±3.6671959 |
| 8 | 14.0 | 86±4.1966608 |
|
|
Negative | 52 | 22 | 42.3 | 75±3.6619246 |
| 12 | 23.1 | 73±4.5150288 |
|
|
Unknown | 13 | 3 | 23.1 | NA |
| 2 | 14.4 | NA |
|
| PR status |
|
|
|
| 0.2300 |
|
|
| 0.6557 |
|
Positive | 40 | 11 | 27.5 | 82±4.7006779 |
| 7 | 17.5 | 80±5.2390218 |
|
|
Negative | 69 | 27 | 39.1 | 79±3.1488219 |
| 13 | 18.8 | 79±3.9022241 |
|
|
Unknown | 13 | 3 | 23.1 | NA |
| 2 | 15.4 | NA |
|
| HER2 status |
|
|
|
| 0.0097a |
|
|
| 0.7220 |
|
Positive | 48 | 5 | 10.4 | 60±4.8890965 |
| 5 | 10.4 | 53±5.6055087 |
|
|
Negative | 61 | 32 | 52.5 | 82±2.7297154 |
| 14 | 23.0 | 80±3.4181057 |
|
|
Unknown | 13 | 4 | 30.8 | NA |
| 3 | 23.1 | NA |
|
| P53 status |
|
|
|
| 0.1206 |
|
|
| 0.3823 |
|
Positive | 37 | 16 | 43.2 | 82±5.5693640 |
| 7 | 18.9 | 82±6.3899854 |
|
|
Negative | 72 | 22 | 30.6 | 79±2.7109243 |
| 12 | 16.7 | 79±3.3807911 |
|
|
Unknown | 13 | 3 | 23.1 | NA |
| 2 | 15.4 | NA |
|
| SPHK1 |
|
|
|
| 0.0001a |
|
|
| 0.0007a |
|
Positive | 64 | 31 | 48.4 | 70±3.6525019 |
| 18 | 28.1 | 62±4.2430458 |
|
|
Negative | 58 | 10 | 17.2 | 88±2.4733977 |
| 4 | 6.9 | 88±3.1148016 |
|
| Intrinsic
subtype |
|
|
|
| 0.0415a |
|
|
| 0.0005a |
| Luminal
A | 53 | 16 | 30.2 | 86±3.7240436 |
| 9 | 17.0 | 85.5±4.2700536 |
|
| Luminal
B | 8 | 1 | 12.5 | 80±11.8289970 |
| 0 | 0 | 80±13.0198697 |
|
| HER2
type | 6 | 4 | 66.7 | 59±13.6623570 |
| 4 | 66.7 | 30±13.9835618 |
|
|
Basal-like | 42 | 17 | 40.5 | 75±3.9125198 |
| 8 | 19.0 | 75±5.0232251 |
|
|
Undefined | 13 | 3 | 23.1 | NA |
| 1 | 7.8 | NA |
|
| Table III.Multivariate logistic regression
analysis of different prognostic variables in patients with breast
cancer by Cox regression analysis. |
Table III.
Multivariate logistic regression
analysis of different prognostic variables in patients with breast
cancer by Cox regression analysis.
|
| Multivariate
analysis |
|---|
|
|
|
|---|
|
| DFS | OS |
|---|
|
|
|
|
|---|
|
Characteristics | P-value | RR | Hazard ratio, 95%
CI | P-value | RR | Hazard ratio, 95%
CI |
|---|
| Age (<60 vs. ≥
60 years) | 0.4648 | 1.343 | 0.609–2.958 | 0.4762 | 1.471 | 0.509–4.257 |
| Lymph node
metastasis (yes vs. no) | 0.0003a | 6.067 | 2.28–16.082 | 0.0299a | 3.530 | 1.131–11.020 |
| SPHK1 expression
(positive vs. negative) | 0.0518 | 0.453 | 0.204–1.006 | 0.0081a | 0.196 | 0.058–0.655 |
| ER (negative vs.
positive) | 0.0671 | 3.339 | 0.919–12.131 | 0.0411a | 5.107 | 1.068–24.422 |
| PR (negative vs.
positive) | 0.5753 | 1.335 | 0.486–3.666 | 0.3761 | 1.840 | 0.477–7.095 |
| HER2 score
(negative vs. positive) | 0.3707 | 0.707 | 0.331–1.510 | 0.2559 | 1.893 | 0.630–5.692 |
Discussion
Breast cancer is one of the most common malignancies
worldwide; thus, it has been the object of intensive research,
which is now revealing the complexity of this disease. It was
initially reviewed that breast cancer dissemination is a
non-random, organotropic process, originally based on Paget's
theory of seed and soil, which suggests that disseminated cancer
cells (seeds) can form metastases as they reach a microenvironment
(soil), which is congenial enough for their survival and
proliferation (30,31). Nevertheless, how seeds fit in the
exclusive soil has not been fully understood yet. The molecular
subtypes of breast cancer have been proved to provide marginal
metastasis site-specific prognostic information (32), but site-specific biomarkers with
improved accuracy are required.
By contrast, the molecular mechanisms of tumor cell
migration and metastasis to lymph nodes in vivo remain
unclear, although several internal molecules in tumor cells have
been reported to perform critical roles in the process of cell
motility (33). Alteration in
cell-cell adhesion and the secretion and activation of proteolytic
enzymes is considered to be essential for optimal tumor cell
invasion and migration through and across the extracellular
barriers. In these aspects, several internal molecules have been
reported to be associated with lymph node metastasis of breast
carcinoma, including membrane-type 1 matrix metalloproteinase
(34), microRNA-21 (35) and vascular endothelial growth factor C
(36). SPHK1 was previously
identified to be involved in cervical cancer development and
progression and its expression was associated with well-known
prognostic parameters, including lymph node metastasis,
lymphovascular invasion, tumor size, Federation of Gynecology and
Obstetrics stage and invasion depth (37).
Multiple studies have revealed that SPHK1 is a key
enzyme critical to the sphingolipid metabolic pathway, which serves
a vital role in cancer progression. Studies have shown that ectopic
expression of SPHK1 in NIH3T3 fibroblasts may promote the growth of
cells in soft agar and the ability to form tumors in non-obese
diabetic/severe combined immunodeficiency mice (6), and it may be due to its association with
Ras and extracellular-signal regulated kinase 1/2 signaling
(38). The expression of SPHK1 was
revealed to be upregulated in breast cancer by using a microarray
data of 1,269 tumor samples, and the expression status was
positively associated with the survival of patients, indicating a
potential prognostic value of this enzyme (39). It was suggested that SPHK1 is involved
in EGF-mediated activation and migration of breast cancer
MDA-MB-453 cells (40). Consistently,
SPHK1 was revealed to be induced by transforming growth factor-β
(TGF-β) in fibroblasts and mesangioblasts, demonstrating that SPHK1
protein is an important component of the TGF-β signaling pathway
(41,42). A previous study identified that the
regulation of SPHK1 gene expression and kinase activity was
mediated by TGF-β, which is critical to MDA-MB-231 cell viability
(43).
These results support the evidence that SPHK1 has
oncogenic potential in breast cancer progression. The prognostic
role of SPHK1 has been studied in several cancer types, including
gastric cancer (14) and astrocytoma
(44), suggesting that patients with
increased SPHK1 expression had shorter OS time, whereas those with
lower SPHK1 survived longer. These studies indicate that SPHK1 is a
prognostic indicator for a number of diseases. However, the roles
of SPHK1 have not been extensively studied, particularly in the
long-term survival of patients with breast cancer. In the present
study, SPHK1 expression was associated with lymph node metastasis
and the number of metastatic lymph nodes, indicating a role for
SPHK1 in enhancing the progression of tumor cell migration and
metastasis. Significant differences were also observed in other
clinicopathological features and long-term prognosis among
SPHK1-positive and SPHK1-negative samples. Previous studies along
with the present study supported a hypothesis that SPHK1 is
involved in functions other than its intracellular regulating
function; it may also perform a vital role in breast cancer
progression.
However, the present study has certain limitations,
including a lack of intensive study into biological mechanisms
involved in the association of SPHK1 expression and tumor
metastasis. Additional investigations into the mechanisms of SPHK1
in breast cancer metastasis will be performed in future studies,
using a larger sample size with longer follow-up time periods.
In conclusion, SPHK1 may be a potential novel
drug-interfering target for cancer, and additional understanding of
the function and molecular mechanisms of SPHK1 in regulating the
progression of breast cancer may provide new insights into breast
cancer therapy.
Acknowledgments
The authors would like to thank Ms. Ke Yang and Qian
Liu from the Clinical and Pathological Diagnosis Center of
Chongqing Medical University for technical support and assistance.
The present study was supported by the National Natural Science
Foundation of China to Dr Ke Zheng (grant no. 81202090).
References
|
1
|
Siegel R, Ma J, Zou Z and Jemal A: Cancer
statistics, 2014. CA Cancer J Clin. 64:9–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fan L, Strasser-Weippl K, Li JJ, St Louis
J, Finkelstein DM, Yu KD, Chen WQ, Shao ZM and Goss PE: Breast
cancer in China. Lancet Oncol. 15:e279–e289. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Weigelt B, Peterse JL and van't Veer LJ:
Breast cancer metastasis: Markers and models. Nat Rev Cancer.
5:591–602. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Espaillat MP, Shamseddine AA, Adada MM,
Hannun YA and Obeid LM: Ceramide and sphingosine-1-phosphate in
cancer, two faces of the sphinx. Transl Cancer Res. 4:484–499.
2015.
|
|
5
|
Wymann MP and Schneiter R: Lipid
signalling in disease. Nat Rev Mol Cell Biol. 9:162–176. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xia P, Gamble JR, Wang L, Pitson SM,
Moretti PA, Wattenberg BW, D'Andrea RJ and Vadas MA: An oncogenic
role of sphingosine kinase. Curr Biol. 10:1527–1530. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Limaye V, Li X, Hahn C, Xia P, Berndt MC,
Vadas MA and Gamble JR: Sphingosine kinase-1 enhances endothelial
cell survival through a PECAM-1-dependent activation of PI-3K/Akt
and regulation of Bcl-2 family members. Blood. 105:3169–3177. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Maceyka M, Sankala H, Hait NC, Le Stunff
H, Liu H, Toman R, Collier C, Zhang M, Satin LS, Merrill AH Jr, et
al: SphK1 and SphK2, sphingosine kinase isoenzymes with opposing
functions in sphingolipid metabolism. J Biol Chem. 280:37118–37129.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Igarashi N, Okada T, Hayashi S, Fujita T,
Jahangeer S and Nakamura S: Sphingosine kinase 2 is a nuclear
protein and inhibits DNA synthesis. J Biol Chem. 278:46832–46839.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liu H, Toman RE, Goparaju SK, Maceyka M,
Nava VE, Sankala H, Payne SG, Bektas M, Ishii I, Chun J, et al:
Sphingosine kinase type 2 is a putative BH3-only protein that
induces apoptosis. J Biol Chem. 278:40330–40336. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang Q, Li J, Li G, Li Y, Xu C, Li M, Xu G
and Fu S: Prognostic significance of sphingosine kinase 2
expression in non-small cell lung cancer. Tumor Biol. 35:363–368.
2014. View Article : Google Scholar
|
|
12
|
French KJ, Schrecengost RS, Lee BD, Zhuang
Y, Smith SN, Eberly JL, Yun JK and Smith CD: Discovery and
evaluation of inhibitors of human sphingosine kinase. Cancer Res.
63:5962–5969. 2003.PubMed/NCBI
|
|
13
|
Malavaud B, Pchejetski D, Mazerolles C, De
Paiva GR, Calvet C, Doumerc N, Pitson S, Rischmann P and Cuvillier
O: Sphingosine kinase-1 activity and expression in human prostate
cancer resection specimens. Eur J Cancer. 46:3417–3424. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li W, Yu CP, Xia JT, Zhang L, Weng GX,
Zheng HQ, Kong QL, Hu LJ, Zeng MS, Zeng YX, et al: Sphingosine
kinase 1 is associated with gastric cancer progression and poor
survival of patients. Clin Cancer Res. 15:1393–1399. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
van Brocklyn JR, Jackson CA, Pearl DK,
Kotur MS, Snyder PJ and Prior TW: Sphingosine kinase-1 expression
correlates with poor survival of patients with glioblastoma
multiforme: Roles of sphingosine kinase isoforms in growth of
glioblastoma cell lines. J Neuropathol Exp Neurol. 64:695–705.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kohno M, Momoi M, Oo ML, Paik JH, Lee YM,
Venkataraman K, Ai Y, Ristimaki AP, Fyrst H, Sano H, et al:
Intracellular role for sphingosine kinase 1 in intestinal adenoma
cell proliferation. Mol Cell Biol. 26:7211–7223. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Le Scolan E, Pchejetski D, Banno Y, Denis
N, Mayeux P, Vainchenker W, Levade T and Moreau-Gachelin F:
Overexpression of sphingosine kinase 1 is an oncogenic event in
erythroleukemic progression. Blood. 106:1808–1816. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu SQ, Su YJ, Qin MB, Mao YB, Huang JA
and Tang GD: Sphingosine kinase 1 promotes tumor progression and
confers malignancy phenotypes of colon cancer by regulating the
focal adhesion kinase pathway and adhesion molecules. Int J Oncol.
42:617–626. 2013.PubMed/NCBI
|
|
19
|
Liu G, Zheng H, Zhang Z, Wu Z, Xiong H, Li
J and Song L: Overexpression of sphingosine kinase 1 is associated
with salivary gland carcinoma progression and might be a novel
predictive marker for adjuvant therapy. BMC Cancer. 10:4952010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Guan H, Song L, Cai J, Huang Y, Wu J, Yuan
J, Li J and Li M: Sphingosine kinase 1 regulates the Akt/FOXO3a/Bim
pathway and contributes to apoptosis resistance in glioma cells.
PLoS One. 6:e199462011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Akao Y, Banno Y, Nakagawa Y, Hasegawa N,
Kim TJ, Murate T, Igarashi Y and Nozawa Y: High expression of
sphingosine kinase 1 and S1P receptors in chemotherapy-resistant
prostate cancer PC3 cells and their camptothecin-induced
up-regulation. Biochem Biophys Res Commun. 342:1284–1290. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kawamori T, Osta W, Johnson KR, Pettus BJ,
Bielawski J, Tanaka T, Wargovich MJ, Reddy BS, Hannun YA, Obeid LM
and Zhou D: Sphingosine kinase 1 is up-regulated in colon
carcinogenesis. FASEB J. 20:386–388. 2006.PubMed/NCBI
|
|
23
|
Pchejetski D, Golzio M, Bonhoure E, Calvet
C, Doumerc N, Garcia V, Mazerolles C, Rischmann P, Teissié J,
Malavaud B and Cuvillier O: Sphingosine kinase-1 as a chemotherapy
sensor in prostate adenocarcinoma cell and mouse models. Cancer
Res. 65:11667–11675. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sarkar S, Maceyka M, Hait NC, Paugh SW,
Sankala H, Milstien S and Spiegel S: Sphingosine kinase 1 is
required for migration, proliferation and survival of MCF-7 human
breast cancer cells. FEBS Lett. 579:5313–5317. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Datta A, Loo SY, Huang B, Wong L, Tan SS,
Tan TZ, Lee SC, Thiery JP, Lim YC, Yong WP, et al: SPHK1 regulates
proliferation and survival responses in triple-negative breast
cancer. Oncotarget. 5:5920–5933. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Luo HJ, Chen X, Tu G, Wang J, Wu CY and
Yang GL: Therapeutic application of ultrasound-guided 8-gauge
mammotome system in presumed benign breast lesions. Breast J.
17:490–497. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pan X, Zhou T, Tai YH, Wang C, Zhao J, Cao
Y, Chen Y, Zhang PJ, Yu M, Zhen C, et al: Elevated expression of
CUEDC2 protein confers endocrine resistance in breast cancer. Nat
Med. 17:708–714. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Goldhirsch A, Wood W, Coates A, Gelber R,
Thürlimann B and Senn HJ: Panel members: Strategies for
subtypes-dealing with the diversity of breast cancer: Highlights of
the St. Gallen International Expert Consensus on the Primary
Therapy of Early Breast Cancer 2011. Ann Oncol. 22:1736–1747. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Paget S: The distribution of secondary
growths in cancer of the breast. Cancer Metastasis Rev. 8:98–101.
1889.
|
|
31
|
Fidler IJ: The pathogenesis of cancer
metastasis: The ‘seed and soil’ hypothesis revisited. Nat Rev
Cancer. 3:453–458. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
32
|
Rakha EA, El-Sayed ME, Green AR, Lee AH,
Robertson JF and Ellis IO: Prognostic markers in triple-negative
breast cancer. Cancer. 109:25–32. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang W, Goswami S, Sahai E, Wyckoff JB,
Segall JE and Condeelis JS: Tumor cells caught in the act of
invading: Their strategy for enhanced cell motility. Trends Cell
Biol. 15:138–145. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yao G, He P, Chen L, Hu X, Gu F and Ye C:
MT1-MMP in breast cancer: Induction of VEGF-C correlates with
metastasis and poor prognosis. Cancer Cell Int. 13:982013.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yan LX, Huang XF, Shao Q, Huang MY, Deng
L, Wu QL, Zeng YX and Shao JY: MicroRNA miR-21 overexpression in
human breast cancer is associated with advanced clinical stage,
lymph node metastasis and patient poor prognosis. RNA.
14:2348–2360. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Skobe M, Hawighorst T, Jackson DG, Prevo
R, Janes L, Velasco P, Riccardi L, Alitalo K, Claffey K and Detmar
M: Induction of tumor lymphangiogenesis by VEGF-C promotes breast
cancer metastasis. Nat Med. 7:192–198. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kim HS, Yoon G, Ryu JY, Cho YJ, Choi JJ,
Lee YY, Kim TJ, Choi CH, Song SY, Kim BG, et al: Sphingosine kinase
1 is a reliable prognostic factor and a novel therapeutic target
for uterine cervical cancer. Oncotarget. 6:26746–26756. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Shu X, Wu W, Mosteller RD and Broek D:
Sphingosine kinase mediates vascular endothelial growth
factor-induced activation of ras and mitogen-activated protein
kinases. Mol Cell Biol. 22:7758–7768. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ruckhäberle E, Rody A, Engels K, Gaetje R,
von Minckwitz G, Schiffmann S, Grösch S, Geisslinger G, Holtrich U,
Karn T and Kaufmann M: Microarray analysis of altered sphingolipid
metabolism reveals prognostic significance of sphingosine kinase 1
in breast cancer. Breast Cancer Res Treat. 112:41–52. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hait NC, Sarkar S, Le Stunff H, Mikami A,
Maceyka M, Milstien S and Spiegel S: Role of sphingosine kinase 2
in cell migration toward epidermal growth factor. J Biol Chem.
280:29462–29469. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yamanaka M, Shegogue D, Pei H, Bu S,
Bielawska A, Bielawski J, Pettus B, Hannun YA, Obeid L and
Trojanowska M: Sphingosine kinase 1 (SPHK1) is induced by
transforming growth factor-beta and mediates TIMP-1 up-regulation.
J Biol Chem. 279:53994–54001. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Donati C, Cencetti F, De Palma C, Rapizzi
E, Brunelli S, Cossu G, Clementi E and Bruni P: TGFbeta protects
mesoangioblasts from apoptosis via sphingosine kinase-1 regulation.
Cell Signal. 21:228–236. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Stayrook KR, Mack JK, Cerabona D, Edwards
DF, Bui HH, Niewolna M, Fournier PG, Mohammad KS, Waning DL and
Guise TA: TGFβ-mediated induction of SphK1 as a potential
determinant in human MDA-MB-231 breast cancer cell bone metastasis.
Bonekey Rep. 4:7192015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Li J, Guan HY, Gong LY, Song LB, Zhang N,
Wu J, Yuan J, Zheng YJ, Huang ZS and Li M: Clinical significance of
sphingosine kinase-1 expression in human astrocytomas progression
and overall patient survival. Clin Cancer Res. 14:6996–7003. 2008.
View Article : Google Scholar : PubMed/NCBI
|