Introduction
Patients with colorectal cancer (CRC) often have
metastases at initial presentation or during follow-up (1,2). The liver
is one of the most frequent sites of metastasis (1,2). Newly
developed chemotherapeutic agents, including targeted therapies,
have improved the progression-free and overall survival times of
patients with metastatic CRC (3,4). There is
also evidence supporting the benefit of surgery to treat metastases
from CRCs, with surgery improving overall survival time (5–7). The
prolonged survival times of patients have highlighted the
importance of local therapy for CRC and limited metastatic disease.
In patients who are unfit for surgery, alternative local
therapeutic approaches, including radiofrequency ablation (RFA),
are available to treat liver metastases; these approaches are
minimally invasive and can achieve good local control (8,9). However,
their indication is currently limited to relatively small tumors
that are located far away from critical structures (8,9).
Modern radiotherapeutic techniques, including
intensity-modulated radiation therapy (IMRT) and stereotactic body
radiation therapy (SBRT), have recently become more frequently
utilized to curatively treat limited metastatic tumors (10–14). SBRT,
also termed stereotactic ablative radiation therapy, is a proven
curative treatment for medically inoperable small tumors in the
lung and liver; it delivers highly conformal radiation in a limited
number of high-dose fractions, providing excellent primary tumor
control with minimal toxicity (12–21).
Radiotherapy in alternatively fractionated regimens with a greater
number of fractions may be required to reduce the biologically
effective doses (BEDs) to normal tissues when treating liver tumors
located in the hepatic portal regions. In those cases, IMRT may be
considered a more conventional schedule (22). However, there are limited data that
compare SBRT with conventionally fractionated radiotherapy of
curative intent.
The present study aimed to evaluate the optimal
radiotherapy regimen for liver metastases from CRC.
Materials and methods
Patients
The present study was conducted according to the
principles of the Declaration of Helsinki. The institutional review
board of Miyakojima IGRT Clinic (Osaka, Japan) approved data
collection and analysis (approval no. 9). A total of 39 liver
tumors in 24 patients who received definitive radiotherapy at
Miyakojima IGRT Clinic between November 2007 and December 2014 were
analyzed. All eligible patients were histologically diagnosed with
primary colorectal adenocarcinoma and radiographically diagnosed
with liver metastases using computed tomography (CT) or magnetic
resonance imaging (MRI). Tumors from patients who were followed up
for <6 months without any failures were excluded. Written
informed consent for radiotherapy was obtained from all patients.
Patient characteristics are shown in Table I.
 | Table I.Characteristics of the patients
(n=24) and tumors (n=39). |
Table I.
Characteristics of the patients
(n=24) and tumors (n=39).
|
Characteristics | n (%) | Median (range) |
|---|
| Gender |
|
|
|
Male | 14 (58.3) | – |
|
Female | 10 (41.7) | – |
| Age, years | – | 64 (43–84) |
| Performance
status |
|
|
| 0 | 14 (58.3) | – |
| 1 | 10 (41.7) | – |
| Primary tumor
location |
|
|
|
Right-sided colon | 4
(16.7) | – |
|
Left-sided colon | 14 (58.3) | – |
|
Rectum | 6
(25.0) | – |
| Interval between
the initial treatment and radiotherapy, months | – | 34 (5–145) |
| Number of liver
metastasis at the initial radiotherapy |
|
|
| 1 | 18 (75.0) | – |
| 2 | 4
(16.7) | – |
| 3 | 2 (8.3) | – |
| Usage of
chemotherapy after initial surgery to radiotherapy |
|
|
|
Yes | 21 (87.5) | – |
| No | 3
(12.5) | – |
| Presence of
metastasis at the initial diagnosis |
|
|
|
Yes | 8
(33.3) | – |
| No | 16 (66.7) | – |
| History of local
therapya for
metastasis |
|
|
|
Yes | 16 (66.7) | – |
| No | 8
(33.3) | – |
| History of
chemotherapy |
|
|
|
Yes | 21 (87.5) | – |
| No | 3 (12.5) | – |
| History of
radiotherapy |
|
|
|
Yes | 4
(16.7) | – |
| No | 20 (83.3) | – |
| Presence of extra
diseases outside the field of radiotherapy |
|
|
|
Yes | 5
(20.8) | – |
| No | 19 (79.2) | – |
| Primary tumor
location |
|
|
|
Right-sided colon | 7
(17.9) | – |
|
Left-sided colon | 22 (56.4) | – |
|
Rectum | 10 (25.6) | – |
| GTV, cc | – | 8.7
(0.4–134.7) |
| Size of maximum
diameter, mm |
| 35.6
(7.0–116.9) |
|
≤30 | 18 (46.2) | – |
|
30–50 | 13 (33.3) | – |
|
>50 | 8
(20.5) | – |
| PTV, cc | – | 52.8
(12.3–243.0) |
| Total dose, Gy | – | 56.0
(45.0–72.0) |
| Number of
fractions | – | 8 (4–33) |
| Fraction size,
Gy | – | 7.0 (2.0–12.0) |
| Total prescription
BED10, Gy | – | 97.5
(71.7–115.5) |
SBRT technique
Radiotherapy for liver tumors was performed as
previously described (23). Briefly,
CT and MRI scans for treatment planning were obtained using a
4-slice BrightSpeed ExcelÔ (GE Healthcare Bio-Sciences, Pittsburgh,
PA, USA) between November 2007 and June 2014, and a 64-slice
SOMATOM Definition AS Open RT Pro edition (Siemens AG, Munich,
Germany) from July 2014 onward, as well as the SIGNA EXCITE HDx
1.5T (GE Healthcare Bio-Sciences), respectively. Planning
contrast-enhanced 4-dimensional CT scans and
gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic
acid-enhanced MRI images were used to determine gross tumor volume.
Planning target volume (PTV) was created by adding a 4–8-mm margin
in all directions to the internal target volume (ITV). The
prescribed radiation doses were documented at the reference point
using conformal beams in 17 tumors, or designed to deliver the
prescribed dose to cover 95% of the PTV using IMRT in 22 tumors. A
prescribed dose equivalent to a BED10 of ~100 Gy was
administered to the liver metastases from CRC. Radiotherapy was
performed using a 6-MV linear accelerator (Novalis BrainLAB AG,
Feldkirchen, Germany).
Follow-up
Local control was defined as the absence of local
failure. Local control and survival times were defined as the
intervals between the start of radiotherapy and the date of
diagnosis of local failure or the date of mortality, respectively.
Local failures were identified by experienced physicians using CT
and MRI, and defined by any regrowth of the target tumor or the
appearance of tumor staining in the target tumor on
contrast-enhanced images. Toxicity was evaluated for the 29
treatments for 39 tumors in 24 patients. No hematological
toxicities were considered to exist in patients who exhibited
hematological abnormalities prior to radiotherapy and developed no
apparent changes from the baseline. Toxicity was evaluated using
the Common Terminology Criteria for Adverse Events version 4.0
(24).
Statistical analysis
The data are expressed as the medians, with the
ranges in parentheses, unless otherwise indicated. Cumulative local
control and survival estimates were calculated using the
Kaplan-Meier method, and statistical differences were evaluated by
the log-rank test. The Cox proportional hazards model was performed
to evaluate factors affecting local control and survival. Results
are reported as hazard ratios (HR) and corresponding 95% confidence
intervals (CI). Variables with P<0.2 by univariate analysis were
entered into the multivariate model. Multivariate analyses were
performed with a Cox regression analysis. All statistical analyses
were performed using JMP software version 12.2.0 (SAS Institute,
Cary, NC, USA). P<0.05 was considered to indicate a
statistically significant difference.
Results
Eligible patients and tumors
Of the 24 eligible patients, 14 patients received
radiotherapy for a single liver metastasis, 3 patients received
radiotherapy for two different lesions simultaneously, 3 patients
received radiotherapy for two different lesions that occurred
sequentially, and 2 patients received radiotherapy for three
different lesions simultaneously. In addition, 1 patient received
radiotherapy for one lesion and then for three lesions
simultaneously 4 months later, and 1 patient received radiotherapy
for two lesions simultaneously and then for one lesion 1 month
later. The median follow-up times were 11 months (range, 5–52
months) and 16.5 months (range, 6–64 months) for local control and
survival, respectively. Ablative SBRT, defined as BED10
≥100 Gy in ≤5 fractions, was performed for 16 tumors in 8
patients.
Grade 1 nausea and fatigue were observed in 2
patients including 1 patient who developed grade 1 alkaline
phosphatase (ALP) elevation and grade 2 γ-glutamyl transpeptidase
(GGT) elevation following radiotherapy. Furthermore, 1 patient
developed grade 1 aspartate aminotransferase (AST), alanine
aminotransferase (ALT) and ALP elevation, and grade 2 GGT elevation
following two different treatments. One patient developed grade 1
ALP elevation alone. In addition, 1 patient developed grade 1 AST,
ALT and ALP elevation and grade 3 GGT elevation due to
chemotherapy. One patient developed grade 2 AST and ALP elevation,
and grade 3 GGT and blood bilirubin elevation due to cholangitis
caused by a recurrent tumor. Furthermore, 1 patient developed a
hemorrhagic duodenal ulcer; however, there was no evident causal
association between that event and radiotherapy.
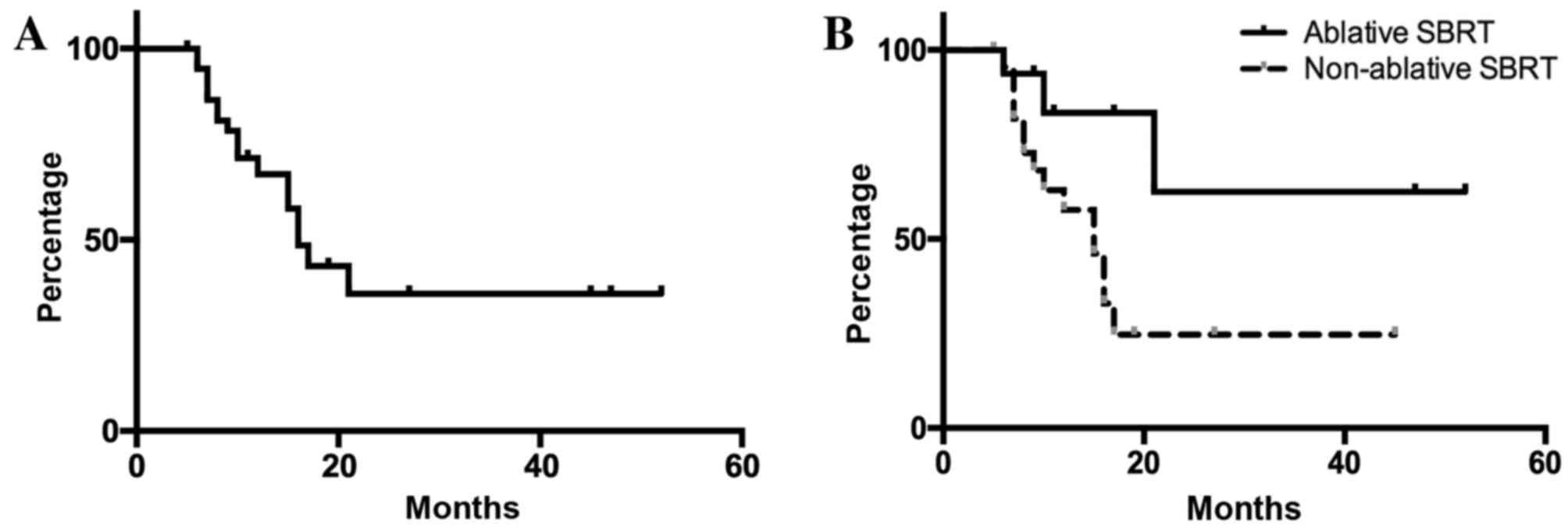
Local control
In all 39 liver metastases, the local control rates
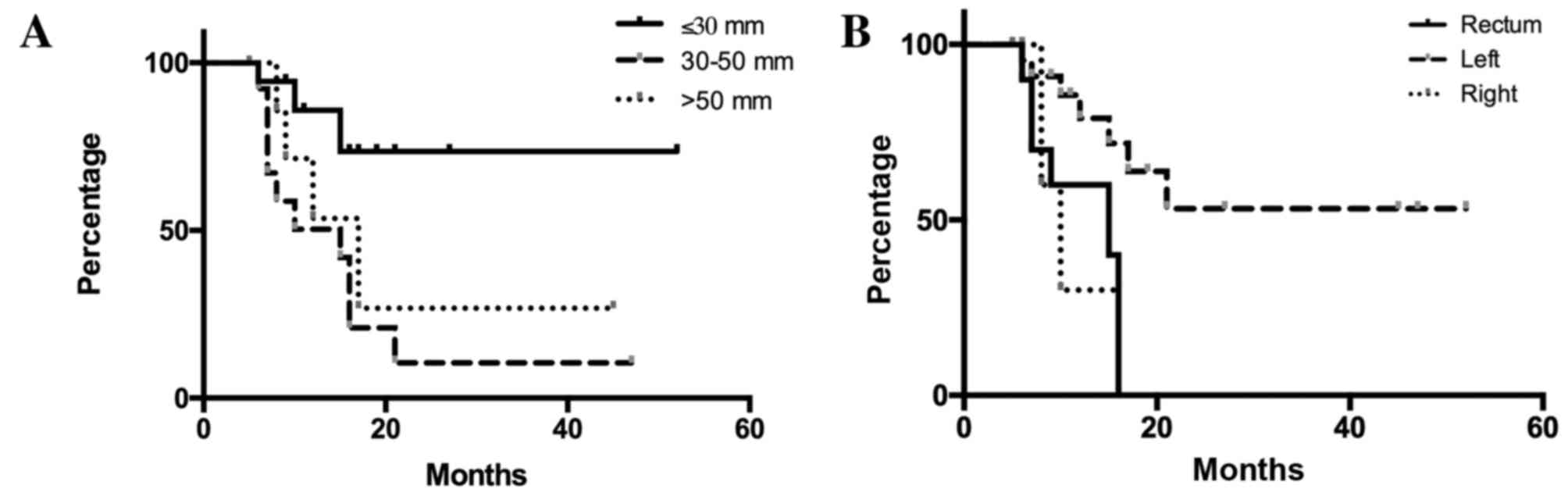
were 67.2 and 35.9% after 1 and 2 years, respectively (Fig. 1). When patients were divided into
three groups based on tumor size (maximum diameter of GTV, ≤30,
30–50 and >50 mm), patients with tumors ≤30 mm in maximum
diameter had significantly improved local control compared with the
other two groups (Fig. 2A). When
patients were stratified according to the primary tumor, defined as
right-sided colon (cecum, ascending and transverse colon),
left-sided colon (descending, sigmoid and rectosigmoidal) or rectal
cancers, liver metastases from rectal cancer were shown to be
associated with a significantly poorer local control rate compared
with those from the left-sided colon (Fig. 2B).
Univariate analyses showed that colon cancer,
left-sided location of primary tumor, the use of ablative SBRT and
tumor size ≤30 mm were significantly associated with improved local
control rates. In addition, multivariate analysis showed that tumor
size <30 mm was a significant independent predictor of local
control (Table II).
| Table II.Factors associated with local control
in 39 tumors. |
Table II.
Factors associated with local control
in 39 tumors.
|
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|---|
| Factor | n (%) | MST, months | P-value | HR (95% CI) | P-value | HR (95% CI) |
|---|
| Age, years |
|
|
|
|
|
|
|
<65 | 19 (48.7) | 16 | 0.9486 | 1.000 | – | – |
|
≥65 | 20 (51.3) | 17 |
| 0.969
(0.368–2.600) |
| – |
| Gender |
|
|
|
|
|
|
|
Male | 25 (64.1) | 16 | 0.7442 | 1.000 | – | – |
|
Female | 14 (35.9) | 21 |
| 0.839
(0.261–2.309) |
| – |
| Performance
Status |
|
|
|
|
|
|
| 0 | 25 (64.1) | 17 | 0.8508 | 1.000 | – | – |
| 1 | 14 (35.9) | 12 |
| 0.908
(0.344–2.649) |
| – |
| Primary tumor
location |
|
|
|
|
|
|
|
Left-sided colon | 22 (56.4) | N/A | 0.0058 | 1.000 | 0.1068 | 1.000 |
|
Other | 17 (43.6) | 10 |
| 4.370
(1.529–14.199) |
| 3.728
(0.766–23.295) |
| Ablative SBRT |
|
|
|
|
|
|
|
Yes | 16 (41.0) | N/A | 0.0268 | 1.000 | 0.4817 | 1.000 |
| No | 23 (59.0) | 15 |
| 3.558
(1.144–15.594) |
| 2.292
(0.205–24.041) |
| BED10,
Gy |
|
|
|
|
|
|
|
<100 | 20 (51.3) | 15 | 0.0751 | 1.000 | 0.7181 | 1.000 |
|
≥100 | 19 (48.7) | N/A |
| 0.401
(0.126–1.094) |
| 1.464
(0.148–9.748) |
| Maximum diameter of
the GTV, mm |
|
|
|
|
|
|
|
≤30 | 18 (46.2) | N/A | 0.0059 | 1.000 | 0.0314 | 1.000 |
|
>30 | 21 (53.8) | 15 |
| 4.625
(1.506–20.084) |
| 3.940
(1.121–18.692) |
| PTV margin, mm |
|
|
|
|
|
|
|
<8 | 17 (43.6) | 16 | 0.1350 | 1.000 | 0.6641 | 1.000 |
| 8 | 22 (56.4) | 21 |
| 0.478
(0.177–1.265) |
| 1.441
(0.296–9.156) |
| Interval between
the initial treatment and radiotherapy, months |
|
|
|
|
|
|
|
≥35 | 19 (48.7) | 16 | 0.5991 | 1.000 | – | – |
|
<35 | 20 (51.3) | 21 |
| 0.771
(0.284–2.051) |
| – |
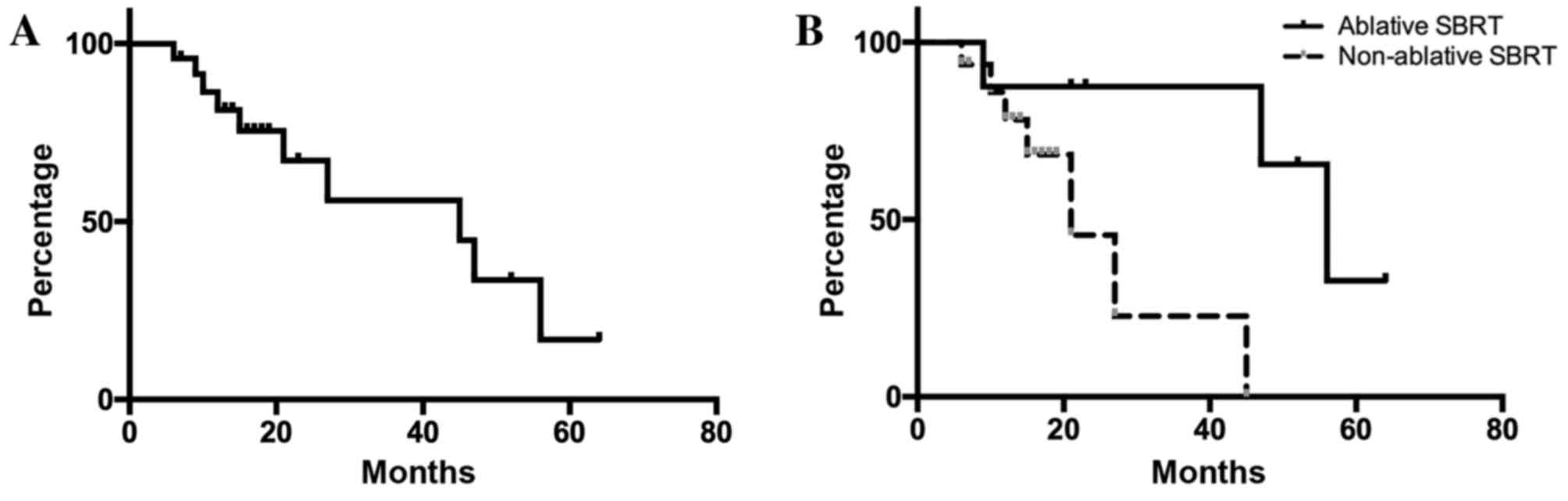
Survival times
For all 24 patients, the overall survival rates were
81.3 and 67.1% at 12 and 24 months, respectively (Fig. 3). In univariate analyses, ablative
SBRT, BED10 ≥100 Gy, an interval between the initial
surgical treatment for the primary tumor and radiotherapy ≥35
months, and presence of a single liver metastasis were
significantly associated with improved survival outcomes (Table III). No significant independent
factors were detected by multivariate analysis.
| Table III.Factors associated with overall
survival in 24 patients. |
Table III.
Factors associated with overall
survival in 24 patients.
|
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|---|
| Factor | n (%) | MST, months | P-value | HR (95% CI) | P-value | HR (95% CI) |
|---|
| Age, years |
|
|
|
|
|
|
|
<65 | 13 (54.2) | 47 | 0.3912 | 1.000 | – | – |
|
≥65 | 11 (45.8) | 27 |
| 1.964
(0.412–10.545) |
| – |
| Gender |
|
|
|
|
|
|
|
Male | 14 (58.3) | 27 | 0.7355 | 1.000 | – | – |
|
Female | 10 (41.7) | 47 |
| 0.801
(0.212–3.001) |
| – |
| Performance
Status |
|
|
|
|
|
|
| 0 | 14 (58.3) | 27 | 0.5065 | 1.000 | – | – |
| 1 | 10 (41.7) | 47 |
| 0.636
(0.151–2.398) |
| – |
| Primary tumor
location |
|
|
|
|
|
|
|
Colon | 18 (75.0) | 45 | 0.6331 | 1.000 | – | – |
|
Rectum | 6 (25.0) | 21 |
| 1.414
(0.295–5.256) |
| – |
|
Left-sided colon | 11 (45.8) | 45 | 0.5105 | 1.000 | – | – |
|
Other | 13 (54.2) | 21 |
| 1.562
(0.385–5.691) |
| – |
| Ablative SBRT |
|
|
|
|
|
|
|
Yes | 8 (33.3) | 56 | 0.0182 | 1.000 | 0.4688 | 1.000 |
| No | 16 (66.7) | 12 |
| 8.673
(1.387–169.233) |
|
1.121×10−8 (0–25.088) |
| BED10,
Gy |
|
|
|
|
|
|
|
<100 | 13 (54.2) | 21 | 0.0060 | 1.000 | 0.1802 | 1.000 |
|
≥100 | 11 (45.8) | 56 |
| 0.092
(0.005–0.544) |
|
3.133×10−9
(0–9.697×10−39) |
| Maximum diameter of
the GTV, mm |
|
|
|
|
|
|
|
≤30 | 9 (37.5) | 27 | 0.4843 | 1.000 | – | – |
|
>30 | 15 (62.5) | 45 |
| 1.715
(0.409–11.580) |
| – |
|
≤50 | 17 (70.8) | 47 | 0.3458 | 1.000 | – | – |
|
>50 | 7 (29.2) | 45 |
| 2.066
(0.416–8.634) |
| – |
| PTV margin, mm |
|
|
|
|
|
|
|
<8 | 11 (45.8) | 21 | 0.2071 | 1.000 | – | – |
| 8 | 13 (54.2) | 45 |
| 0.445
(0.113–1.573) |
| – |
| Interval between
the initial treatment and radiotherapy, months |
|
|
|
|
|
|
|
≥35 | 11 (45.8) | 21 | 0.0028 | 1.000 | 0.4246 | 1.000 |
|
<35 | 13 (54.2) | 56 |
| 0.079
(0.004–0.456) |
| 0.353 (0.010-
3.807) |
| Presence of
metastasis at the initial diagnosis |
|
|
|
|
|
|
|
Yes | 8 (33.3) | 45 | 0.3683 | 1.000 | – | – |
| No | 16 (66.7) | 27 |
| 1.984
(0.475–13.384) |
| – |
| History of local
therapya for
metastasis |
|
Yes | 16 (66.7) | 45 | 0.4530 | 1.000 | – | – |
| No | 8 (33.3) | N/A |
| 0.564
(0.084–2.313) |
| – |
| History of
chemotherapy |
|
|
|
|
|
|
|
Yes | 21 (87.5) | 45 | 0.3970 | 1.000 | – | – |
| No | 3 (12.5) | N/A |
| 2.903
(0.147–20.092) |
| – |
| History of
radiotherapy |
|
|
|
|
|
|
|
Yes | 4 (16.7) | 15 | 0.1113 | 1.000 | 0.1131 | 1.000 |
| No | 20 (83.3) | 45 |
| 0.201
(0.033–1.545) |
| 0.154
(0.013–1.629) |
| Presence of extra
diseases outside the field of radiotherapy |
|
|
|
|
|
|
|
Yes | 5 (20.8) | 56 | 0.6227 | 1.000 | – | – |
| No | 19 (79.2) | 27 |
| 1.438
(0.354–7.363) |
| – |
| Number of liver
metastases |
|
|
|
|
|
|
| 1 | 18 (75.0) | 47 | 0.0323 | 1.000 | 0.1246 | 1.000 |
|
>1 | 6 (25.0) | 21 |
| 5.294
(1.160–27.017) |
| 3.845
(0.689–30.348) |
Discussion
The recommended treatment for patients with
oligometastases in the liver is surgical resection (10,11).
However, the resection rate of hepatic metastases has been reported
to be only 0.8–22% (25). Liver
metastases are known to have different sensitivities to radiation
therapy based on the location of the primary tumor; it has been
reported that liver metastases derived from CRCs were significantly
more resistant to radiation compared with liver metastases derived
from non-colorectal cancers (15–17). Thus,
patients with CRC metastases may benefit from dose escalation. In
addition, a hypoxic cell radiosensitizer may potentially improve
local control (26).
The present data indicated that liver metastases
from rectal cancer were more resistant to radiotherapy compared
with those from colon cancer. Conversely, patients with metastases
from left-sided colon cancer showed favorable local control rates
following radiotherapy. CRC biological behavior was previously
shown to depend on tumor location, as it varies for tumors
originating from the right-sided colon, left-sided colon and rectum
(27–33). Significant overexpression of p53 that
can affect the response to radiotherapy in rectal cancer in
comparison with colon cancer has been reported (33,34).
Ayiomamitis et al (33)
reported significant overexpression of p53 in rectal cancer
compared with colon cancer tissue samples. In addition, Spitz et
al (34) reported that p53
immunohistochemical staining of pretreatment biopsy specimens
correlated with the extent of residual disease following
chemoradiation in patients with rectal cancer. To the best of our
knowledge, this is the first study to investigate the association
between the radiosensitivity of liver metastases and primary tumor
location.
Treatment with ablative SBRT, which was defined as a
prescribed BED10 ≥100 Gy in ≤5 fractions, was found to
lead to improved local control and survival rates compared with a
conventional fractionated schedule. High-dose regimens have been
described for metastatic liver tumors (16,18,19). Dose
escalation of SBRT for liver metastasis can improve local control
(18,19). However, the optimal regimen of SBRT
remains unclear. The linear-quadratic (LQ) model has been widely
used to compare differentially fractionated radiotherapeutic
regimens, despite several limitations (35). Our previous studies have described a
prescription using IMRT based on the LQ model (23,36,37).
Hypofractionated radiotherapy at higher doses per fraction may
increase radiation-induced damages due to direct cytotoxicity, and
may lead to microvascular disruption (38–41). It
was suggested that liver metastases should be treated by ablative
SBRT as often as possible, and the present data support the
findings reported in previous studies (15,16).
In the present study, adding margins >8 mm to the
ITV led to improved outcomes, although the differences were not
significant. When performing SBRT for liver tumors, no margins are
usually added to the ITV (12–14,16–21,23).
However, only a few studies have demonstrated how many GTV-to-CTV
expansions are required in order to reach the gross and microscopic
diseases in liver metastasis (41,42).
Beginning in July 2012, the PTV margin was reduced from 8 to 4–6 mm
in order to minimize focal liver damage. A possible CTV margin of
2–4 mm could therefore exist in tumors with a PTV margin of 8 mm in
the present study.
The present study had several limitations. It was a
retrospective study with a small sample size and a relatively short
follow-up period. In addition, selection bias could exist in the
present study, since tumors in the hepatic portal region were often
treated with a more conventional regimen. Although a maximum tumor
diameter ≤30 mm was the only prognostic factor for local control by
multivariate analysis, the present results were compatible with
those in previous studies (20,21).
Chemotherapy was less thoroughly described and heterogeneous in the
present study. Chemotherapy and other supportive care may
differentially affect results, since no significant differences
were observed in survival time despite primary tumor location
significantly affecting local control in the present study. In
addition, molecular biological analysis using immunohistochemistry
and gene evaluation in isolated tissues may reveal differences in
biological behavior of metastatic CRCs in future clinical
studies.
To conclude, patients with liver metastases ≤30 mm
in size from colorectal adenocarcinoma that received ablative SBRT
exhibited favorable local control. Location of the primary tumor
may affect the radiosensitivity of liver metastases.
Acknowledgements
The authors would like to thank Editage (www.editage.jp) for English language editing.
References
|
1
|
Khatri VP, Petrelli NJ and Belghiti J:
Extending the frontiers of surgical therapy for hepatic colorectal
metastases: Is there a limit? J Clin Oncol. 23:8490–8499. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Aranda E, Abad A, Carrato A, Cervantes A,
García-Foncillas J, García Alfonso P, García Carbonero R, Gómez
España A, Tabernero JM and Díaz-Rubio E: Treatment recommendations
for metastatic colorectal cancer. Clin Transl Oncol. 13:162–178.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cunningham D, Humblet Y, Siena S, Khayat
D, Bleiberg H, Santoro A, Bets D, Mueser M, Harstrick A, Verslype
C, et al: Cetuximab monotherapy and cetuximab plus irinotecan in
irinotecan-refractory metastatic colorectal cancer. N Engl J Med.
351:337–345. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Giantonio BJ, Levy DE, O'dwyer PJ, Meropol
NJ, Catalano PJ and Benson AB III; Eastern Cooperative Oncology
Group, : A phase II study of high-dose bevacizumab in combination
with irinotecan, 5-fluorouracil, leucovorin, as initial therapy for
advanced colorectal cancer: Results from the eastern cooperative
oncology group study E2200. Ann Oncol. 17:1399–1403. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rees M, Tekkis PP, Welsh FK, O'Rourke T
and John TG: Evaluation of long-term survival after hepatic
resection for metastatic colorectal cancer: A multifactorial model
of 929 patients. Ann Surg. 247:125–135. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pawlik TM, Scoggins CR, Zorzi D, Abdalla
EK, Andres A, Eng C, Curley SA, Loyer EM, Muratore A, Mentha G, et
al: Effect of surgical margin status on survival and site of
recurrence after hepatic resection for colorectal metastases. Ann
Surg. 241:715–724. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nordlinger B, Guiguet M, Vaillant JC,
Balladur P, Boudjema K, Bachellier P and Jaeck D: Surgical
resection of colorectal carcinoma metastases to the liver. A
prognostic scoring system to improve case selection, based on 1568
patients. Association Française de Chirurgie. Cancer. 77:1254–1262.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cirocchi R, Trastulli S, Boselli C,
Montedori A, Cavaliere D, Parisi A, Noya G and Abraha I:
Radiofrequency ablation in the treatment of liver metastases from
colorectal cancer. Cochrane Database Syst Rev. 13:CD0063172012.
|
|
9
|
Minami Y and Kudo M: Radiofrequency
ablation of liver metastases from colorectal cancer: A literature
review. Gut Liver. 7:1–6. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
National Comprehensive Cancer Network, .
Guidelines version 2.2016 updates colon cancer. https://www.nccn.org/professionals/physician_gls/pdf/colon.pdfJune
12–2016
|
|
11
|
National Comprehensive Cancer Network:
Guidelines version 2.2016 rectal cancer. https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdfJune
12–2016
|
|
12
|
Rieber J, Streblow J, Uhlmann L, Flentje
M, Duma M, Ernst I, Blanck O, Wittig A, Boda-Heggemann J, Krempien
R, et al: Stereotactic body radiotherapy (SBRT) for medically
inoperable lung metastases-A pooled analysis of the German working
group ‘stereotactic radiotherapy’. Lung Cancer. 97:51–58. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hanna GG and Landau D: Stereotactic body
radiotherapy for oligometastatic disease. Clin Oncol (R Coll
Radiol). 27:290–297. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Takeda A, Sanuki N and Kunieda E: Role of
stereotactic body radiotherapy for oligometastasis from colorectal
cancer. World J Gastroenterol. 20:4220–4229. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Binkley MS, Trakul N, Jacobs LR, von Eyben
R, Le QT, Maxim PG, Loo BW Jr, Shultz DB and Diehn M: Colorectal
histology is associated with an increased risk of local failure in
lung metastases treated with stereotactic ablative radiation
therapy. Int J Radiat Oncol Biol Phys. 92:1044–1052. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Takeda A, Sanuki N, Tsurugai Y, Oku Y and
Aoki Y: Stereotactic body radiotherapy for patients with
oligometastases from colorectal cancer: Risk-adapted dose
prescription with a maximum dose of 83–100 Gy in five fractions. J
Radiat Res. 57:400–405. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ahmed KA, Caudell JJ, El-Haddad G,
Berglund AE, Welsh EA, Yue B, Hoffe SE, Naghavi AO, Abuodeh YA,
Frakes JM, et al: Radiosensitivity differences between liver
metastases based on primary histology suggest implications for
clinical outcomes after stereotactic body radiation therapy. Int J
Radiat Oncol Biol Phys. 95:1399–1404. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vautravers-Dewas C, Dewas S, Bonodeau F,
Adenis A, Lacornerie T, Penel N, Lartigau E and Mirabel X:
Image-guided robotic stereotactic body radiation therapy for liver
metastases: Is there a dose response relationship? Int J Radiat
Oncol Biol Phys. 81:e39–e47. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wulf J, Guckenberger M, Haedinger U,
Oppitz U, Mueller G, Baier K and Flentje M: Stereotactic
radiotherapy of primary liver cancer and hepatic metastases. Acta
Oncol. 45:838–847. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yamashita H, Onishi H, Matsumoto Y,
Murakami N, Matsuo Y, Nomiya T and Nakagawa K; Japanese
Radiological Society multi-institutional SBRT study group
(JRS-SBRTSG), : Local effect of stereotactic body radiotherapy for
primary and metastatic liver tumors in 130 Japanese patients.
Radiat Oncol. 9:1122014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rusthoven KE, Kavanagh BD, Cardenes H,
Stieber VW, Burri SH, Feigenberg SJ, Chidel MA, Pugh TJ, Franklin
W, Kane M, et al: Multi-institutional phase I/II trial of
stereotactic body radiation therapy for liver metastases. J Clin
Oncol. 27:1572–1578. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Engels B, Gevaert T, Everaert H, De
Coninck P, Sermeus A, Christian N, Storme G, Verellen D and De
Ridder M: Phase II study of helical tomotherapy in the
multidisciplinary treatment of oligometastatic colorectal cancer.
Radiat Oncol. 7:342012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Doi H, Shiomi H, Masai N, Tatsumi D, Igura
T, Imai Y and Oh RJ: Threshold doses and prediction of visually
apparent liver dysfunction after stereotactic body radiation
therapy in cirrhotic and normal livers using magnetic resonance
imaging. J Radiat Res. 57:294–300. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Common terminology criteria for adverse
events version 4.0. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdfApril
3–2017
|
|
25
|
Folprecht G, Grothey A, Alberts S, Raab HR
and Köhne CH: Neoadjuvant treatment of unresectable colorectal
liver metastases: Correlation between tumour response and resection
rates. Ann Oncol. 16:1311–1319. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Brown JM, Diehn M and Loo BW Jr:
Stereotactic ablative radiotherapy should be combined with a
hypoxic cell radiosensitizer. Int J Radiat Oncol Biol Phys.
78:323–327. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Loupakis F, Yang D, Yau L, Feng S,
Cremolini C, Zhang W, Maus MK, Antoniotti C, Langer C, Scherer SJ,
et al: Primary tumor location as a prognostic factor in metastatic
colorectal cancer. J Natl Cancer Inst. 107:pii:dju4272015.
View Article : Google Scholar
|
|
28
|
Tran B, Kopetz S, Tie J, Gibbs P, Jiang
ZQ, Lieu CH, Agarwal A, Maru DM, Sieber O and Desai J: Impact of
BRAF mutation and microsatellite instability on the pattern of
metastatic spread and prognosis in metastatic colorectal cancer.
Cancer. 117:4623–4632. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Distler P and Holt PR: Are right- and
left-sided colon neoplasms distinct tumors? Dig Dis. 15:302–311.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Iacopetta B: Are there two sides to
colorectal cancer? Int J Cancer. 101:403–408. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hutchins G, Southward K, Handley K, Magill
L, Beaumont C, Stahlschmidt J, Richman S, Chambers P, Seymour M,
Kerr D, et al: Value of mismatch repair, KRAS, and BRAF mutations
in predicting recurrence and benefits from chemotherapy in
colorectal cancer. J Clin Oncol. 29:1261–1270. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Loupakis F, Ruzzo A, Cremolini C, Vincenzi
B, Salvatore L, Santini D, Masi G, Stasi I, Canestrari E, Rulli E,
et al: KRAS codon 61, 146 and BRAF mutations predict resistance to
cetuximab plus irinotecan in KRAS codon 12 and 13 wild-type
metastatic colorectal cancer. Br J Cancer. 101:715–721. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ayiomamitis GD, Notas G, Zaravinos A,
Zizi-Sermpetzoglou A, Georgiadou M, Sfakianaki O and Kouroumallis
E: Differences in telomerase activity between colon and rectal
cancer. Can J Surg. 57:199–208. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Spitz FR, Giacco GG, Hess K, Larry L, Rich
TA, Janjan N, Cleary KR and Skibber JM: p53 immunohistochemical
staining predicts residual disease after chemoradiation in patients
with high-risk rectal cancer. Clin Cancer Res. 3:1685–1690.
1997.PubMed/NCBI
|
|
35
|
Hall EJ and Giaccia AJ: Radiobiology for
the radiologist. 7th. Philadelphia: Lippincott Williams &
Wilkins; 2011
|
|
36
|
Doi H, Oh RJ, Miura H, Masai N, Shiomi H
and Inoue T: Outcomes and toxicity of radiotherapy for refractory
bone and soft tissue sarcomas. Mol Clin Oncol. 4:83–88.
2016.PubMed/NCBI
|
|
37
|
Miura H, Masai N, Oh RJ, Shiomi H, Sasaki
J and Inoue T: Approach to dose definition to the gross tumor
volume for lung cancer with respiratory tumor motion. J Radiat Res.
54:140–145. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Thames HD and Suit HD: Tumor
radioresponsiveness versus fractionation sensitivity. Int J Radiat
Oncol Biol Phys. 12:687–691. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Park HJ, Griffin RJ, Hui S, Levitt SH and
Song CW: Radiation-induced vascular damage in tumors: Implications
of vascular damage in ablative hypofractionated radiotherapy (SBRT
and SRS). Radiat Res. 177:311–327. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Brown JM, Carlson DJ and Brenner DJ: The
tumor radiobiology of SRS and SBRT: Are more than the 5 Rs
involved? Int J Radiat Oncol Biol Phys. 88:254–262. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Qian Y, Zeng ZC, Ji Y and Xiao YP:
Microinvasion of liver metastases from colorectal cancer:
Predictive factors and application for determining clinical target
volume. Radiat Oncol. 10:1252015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Welter S, Theeqarten D, Trarbach T,
Maletzki F, Stamatis G and Tötsch M: Safety distance in the
resection of colorectal lung metastases: A prospective evaluation
of satellite tumor cells with immunohistochemistry. J Thorac
Cardiovasc Surg. 141:1218–1222. 2011. View Article : Google Scholar : PubMed/NCBI
|