Introduction
Nodular fasciitis is a benign soft tissue tumor that
is characterized by the proliferation of fibroblasts and
myofibroblasts in the deep subcutaneous layer, as well as the
muscular fascia (1). Its occurrence
is common in the upper extremities of young to middle aged adults
and is equal in distribution among men and women. Its risk factors
remain unknown and it is often mistaken for soft tissue malignancy
or metastasis (2,3). Complete excision is currently the gold
standard for diagnosis and treatment. Nodular fasciitis exhibits
good prognosis with a low recurrence rate and thus, is considered
benign (3). There are few case
reports on the clinical implications of nodular fasciitis using
18F-fluorodeoxyglucose positron emission
tomography/computed tomography (18F-FDG PET/CT), in
which 18F-FDG uptake was distributed to areas of rich
cellularity and high mitotic activity (4,5). The
present study exhibits a case of nodular fasciitis incidentally
detected on 18F-FDG PET/CT in a patient followed up for
papillary thyroid cancer (PTC).
Case report
A 47-year-old woman was diagnosed with PTC and was
admitted to Ulsan University Hospital (Ulsan, Republic of Korea) in
March 2013 for a total thyroidectomy. The final pathological stage
was T3N1b in accordance with the American Joint Committee on Cancer
staging system (6), with a size of
0.9×0.9×0.8 cm extending to the perithyroidal soft tissue with a
clear resection margin and no lymphovascular invasion, and 9 lymph
node metastases in the left cervical levels II–IV. Radioactive
iodine therapy of 150 mCi was performed.
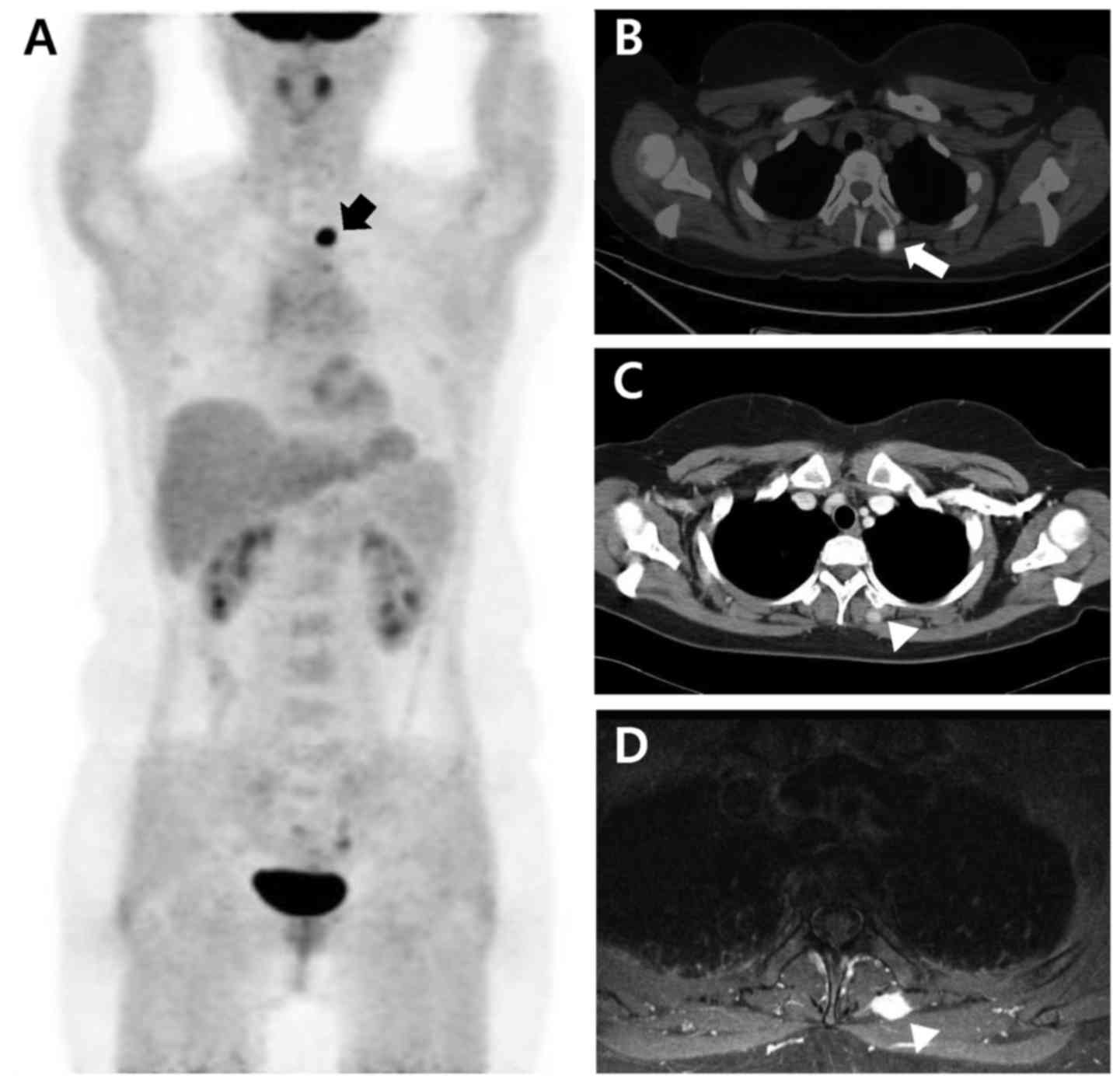
A 12-month follow-up using 18F-FDG PET/CT
revealed an unexpected focal 18F-FDG-avid lesion
(SUVmax, 9.8) in the left paraspinal muscle at the T3
level (Fig. 1A and B). Enhanced chest
CT and magnetic resonance imaging (MRI) were performed to evaluate
the possibility of metastasis. The two modalities showed a
well-enhanced nodule of 9 mm, indicative of metastasis (Fig. 1C and D). No abnormalities were
observed in the laboratory findings at that time. The levels of
thyroid stimulating hormone, thyroglobulin (Tg), thyroxine (T4) and
anti-Tg antibodies measured using chemiluminescence immunoassays
were 0.017 µIU/ml, <0.1 ng/ml, 1.85 ng/dl and <20 IU/ml,
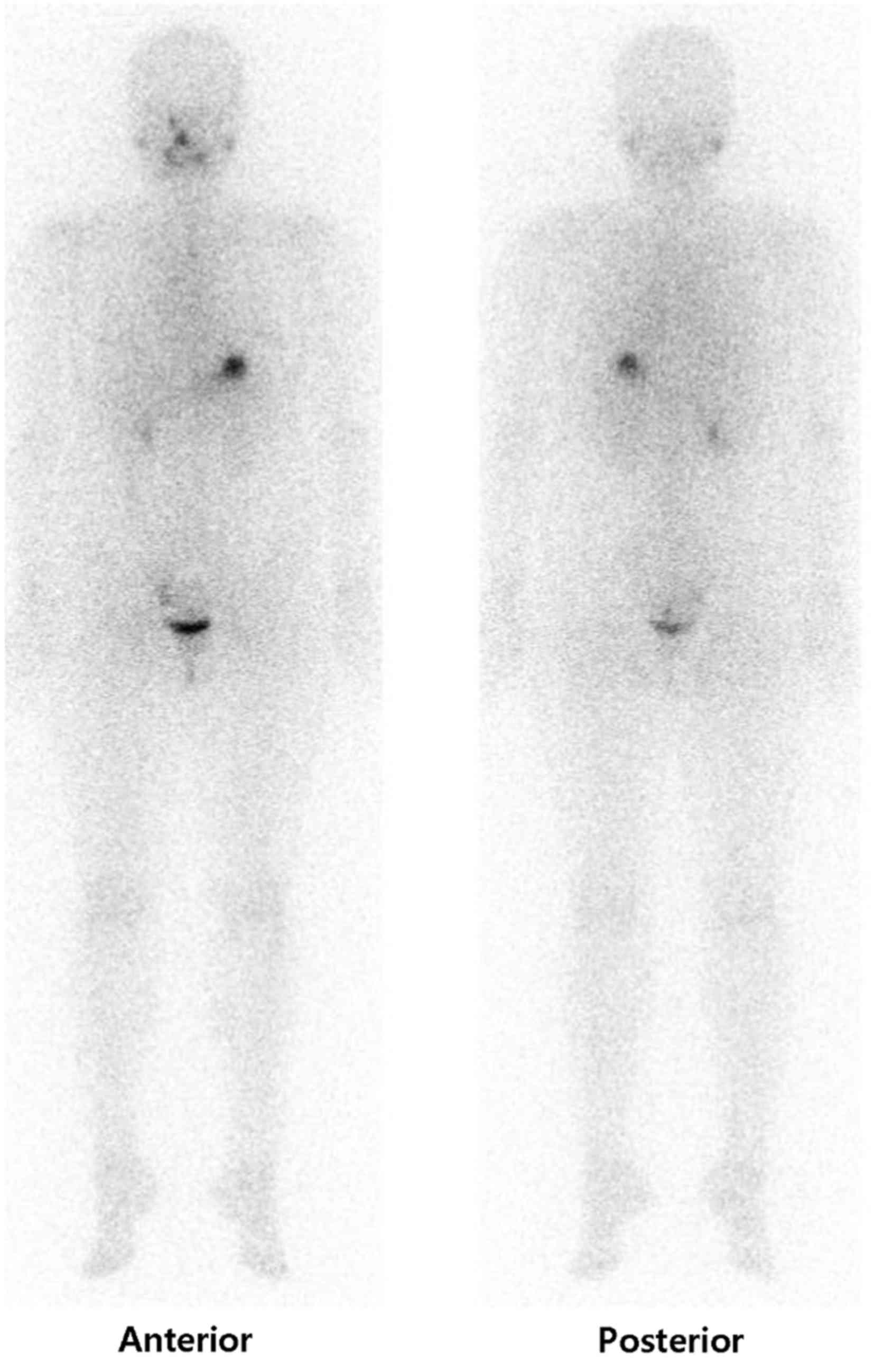
respectively. An 123I diagnostic whole body scan, which
was performed to exclude metastasis from thyroid cancer, showed no
abnormal iodine uptake in the left upper back (Fig. 2). These findings favored a benign
condition over metastasis. The level of stimulated Tg at this time
was 0.89 ng/ml.
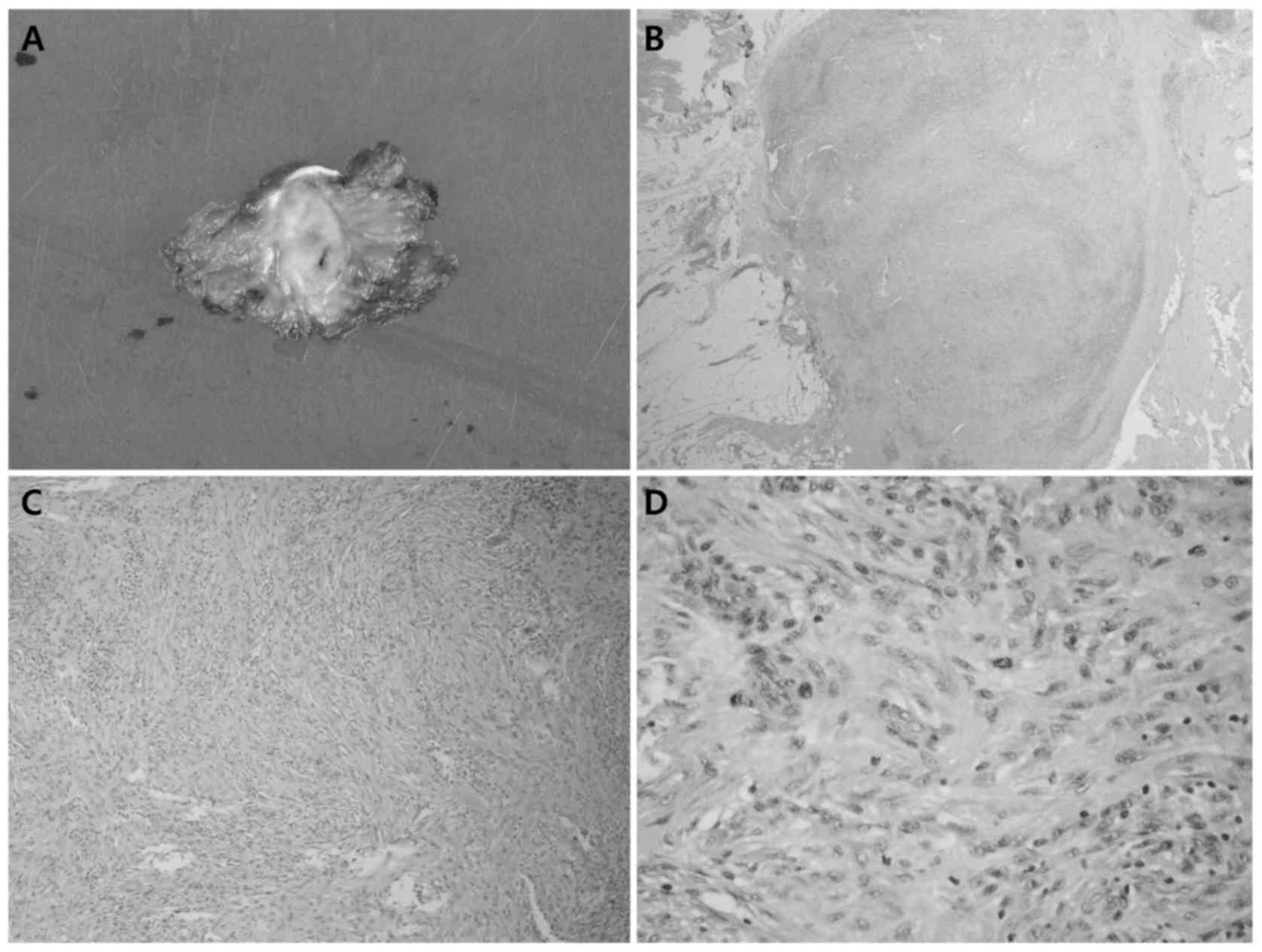
Surgical excision was performed and the pathological
diagnosis was nodular fasciitis. The gross pathological specimen
was a 1.7×1.1 cm well demarcated firm mass (Fig. 3). Following hematoxylin and eosin
staining, the specimen was observed under a light microscope
(Olympus BX51; Olympus Corporation, Tokyo, Japan). Spindle cells
were identified to be arranged in storiform fascicles and normal
mitotic figures were present (Fig.
3). Immunohistochemical analysis for CD68 (cat. no. M0876;
dilution, 1:200; Dako; Agilent Technologies, Inc., Santa Clara, CA,
USA), smooth muscle actin (cat. no. 18-0106; dilution, 1:250;
Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA), CD34
(cat. no. MS-363-P; dilution, 1:1,000; Thermo Fisher Scientific,
Inc.) and S-100 protein (cat. no. LCL-L-S100P; dilution, 1:1,000;
Novocastra; Leica Biosystems GmbH, Wetzlar, Germany) were performed
on formalin-fixed paraffin-embedded 4 µm-thick tissue sections
using Bond-Max with a Bond Polymer Refine Detection kit (Leica
Biosystems GmbH) according to the manufacturers protocol. All
antigen vs. antibody reactions were performed with a Bond Polymer
Refine Detection kit (Leica Biosystems GmbH), and non-specific
binding was blocked by the hydrogen peroxide in the kit according
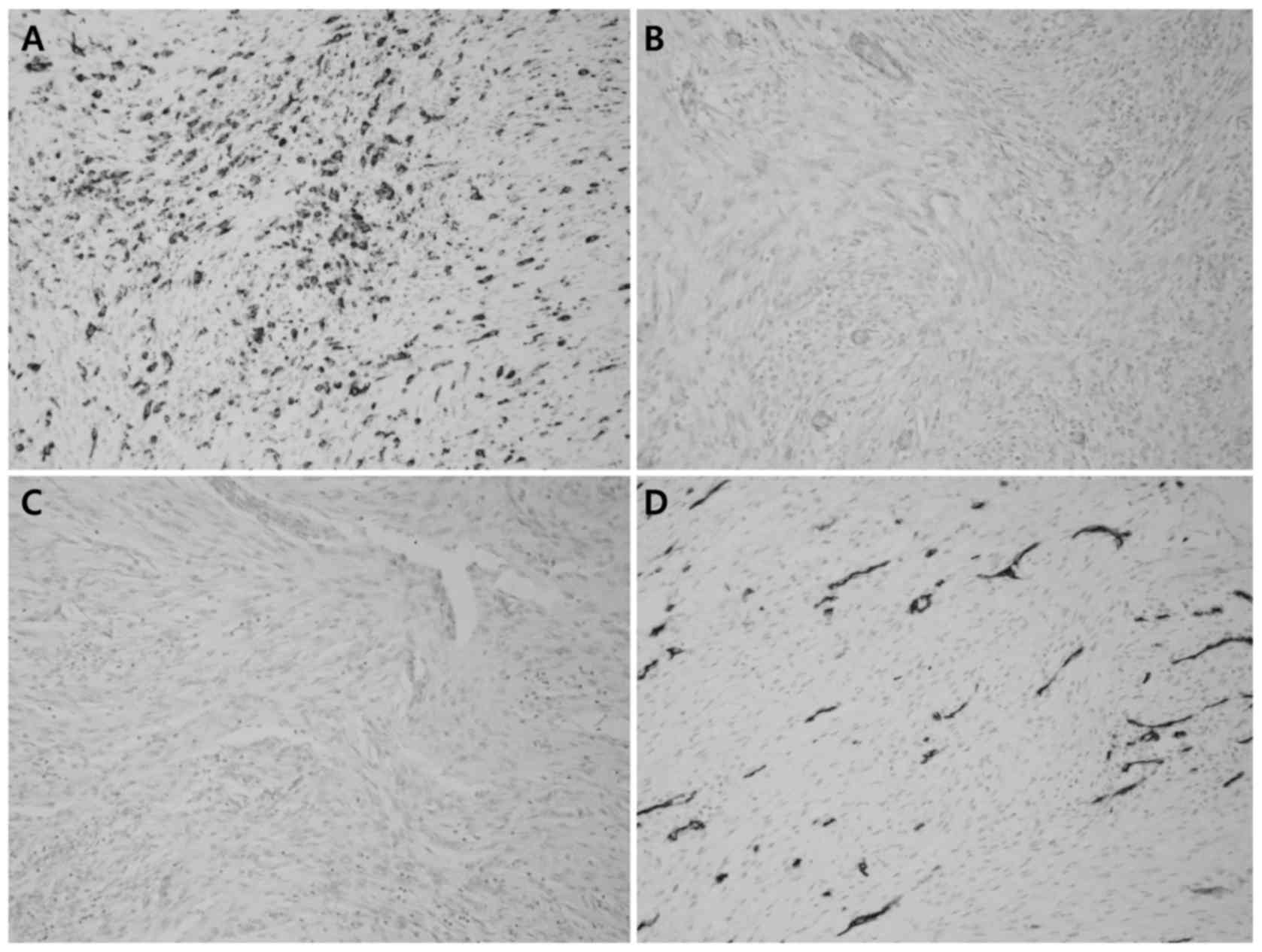
to the protocol of the manufacturer. The specimen exhibited
positive expression levels of CD68 (Fig.
4A) and smooth muscle actin (Fig.
4B), while CD34 (Fig. 4C) and
S-100 (Fig. 4D) proteins were not
expressed (Fig. 4).
No additional treatment was performed. At a 9-month
follow-up post-excision, the patient was disease-free, with an
unstimulated Tg level of <0.01 ng/ml.
Discussion
This is a case of nodular fasciitis, which was
mistaken for muscle metastasis, in a patient being followed up for
PTC.
The majority of thyroid cancers are localized at the
time of diagnosis with only a small proportion (10–35%), depending
on the histology, presenting with distant metastasis (7,8). This
proportion is only 4–15% in the case of differentiated thyroid
cancers (7,8). Common sites of metastasis include the
lungs and bones (8–11), while soft tissue metastasis is
reportedly extremely rare (12–14).
Although distant metastasis in patients with thyroid cancer is not
as grave as that in other cancers, it significantly affects
survival; therefore, a thorough work-up including
18F-FDG PET/CT is required (9,15,16).
18F-FDG PET/CT visualizes glucose
metabolism and is widely used to differentiate between benign and
malignant lesions, as well as to stage/restage various malignances
(17–22). In a number of cases, the intensity of
FDG accumulation is used to differentiate between malignant and
benign lesions (23–26). However, numerous other benign
conditions, including abscess, pulmonary granuloma, tuberculosis
and sarcoidosis, may also present with increased 18F-FDG
uptake (23,27–32). Thus,
there is a high chance of encountering false-positive conditions in
a clinical setting.
The patient in the present case showed a focal
18F-FDG avid lesion that did not show abnormal iodine
uptake, and the patient exhibited a low stimulated Tg level. The
differential diagnosis in this case includes primary (such as
schwannoma, dermatofibroma and sarcoma) and metastatic (from
dedifferentiated thyroid cancer or other malignancies) tumors
(33,34). The 18F-FDG avid lesion in
the current patient turned out to be nodular fasciitis.
Nodular fasciitis is a benign condition, which shows
proliferating fibroblasts in the deep subcutaneous layer or the
muscular fascia (35). Nodular
fasciitis is occasionally clinically mistaken for soft tissue
sarcoma. If there is infiltration of mitotically active spindle
cell lesions in the connective tissue (35), pathological diagnosis is difficult.
The lesion commonly occurs in the first 3 decades of life, with the
upper extremities and the trunk being the most commonly affected
anatomical sites (36,37). Lesions usually present as oval nodules
with poorly- or well-defined margins, and occasionally
microlobulation on CT, MRI and ultrasonography (US) (1,38,39). Lesions show mixed but overall
hypoechoic echogenicity on US, as well as variable but typically
diffuse contrast enhancement on MRI (1,38,39). Although surgical excision is curative,
it usually shows spontaneous involution and is self-limiting
(40).
The present case is in agreement with other case
reports that describe 18F-FDG-avid nodular fasciitis
(4,5,33). The
high 18F-FDG uptake in nodular fasciitis may be due to
its histological characteristics that are also present in
malignancy. These include rapid growth, rich cellularity and high
mitotic activity (4,5). Thus, nodular fasciitis is hard to
diagnose and the high 18F-FDG uptake may be a limitation
of 18F-FDG PET/CT as it mimics malignancy, as in other
radiological and pathological modalities as above mentioned
(2,3,34–37). To the best of our knowledge, there are
no studies on nodular fasciitis mimicking metastasis in PTC.
However, since nodular fasciitis exhibited high FDG avidity in the
present case, metastasis of PTC could not be excluded and
additional diagnostic work-up was necessary. The present
histological findings were similar to those aforementioned.
In the present case, the 18F-FDG-avid
paraspinal lesion was excised, since the imaging modalities showed
findings indicative of soft tissue metastasis. When the lesion was
retrospectively reviewed, it had an increased probability of being
a primary soft tissue lesion compared with metastasis from thyroid
cancer, partly as the patient had a relatively low level of
stimulated Tg (0.89 ng/ml) and the 123I whole body scan
showed negative iodine uptake. Although these findings may also be
shown in the case of a poorly-differentiated metastatic lesion,
soft tissue metastasis from thyroid cancer, which is considered a
manifestation of a terminal stage, is rare and is usually
accompanied by multiple metastases in other sites.
In summary, the present study reported a case of
nodular fasciitis with FDG avidity in a patient with thyroid
cancer. Nodular fasciitis may be included in the differential
diagnosis of an 18F-FDG-avid and iodine non-avid
paraspinal soft tissue lesion, when clinical probability of distant
metastasis is low. In such circumstances of patients with thyroid
cancer, unnecessary surgical procedures may be prevented using a
123I whole body scan as a part of non-invasive
work-up.
References
|
1
|
Kim ST, Kim HJ, Park SW, Baek CH, Byun HS
and Kim YM: Nodular fasciitis in the head and neck: CT and MR
imaging findings. AJNR Am J Neuroradiol. 26:2617–2623.
2005.PubMed/NCBI
|
|
2
|
Rhee SJ, Ryu JK, Kim JH and Lim SJ:
Nodular fasciitis of the breast: Two cases with a review of imaging
findings. Clin Imaging. 38:730–733. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kessels LW, Simsek S, van Hattum AH, Stam
F and Comans EF: Nodular fasciitis: An unexpected finding on
computed tomography and positron emission tomography. Eur J Intern
Med. 15:183–185. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim JY, Park J, Choi YY, Lee S and Paik
SS: Nodular fasciitis mimicking soft tissue metastasis on 18F-FDG
PET/CT during surveillance. Clin Nucl Med. 40:172–174. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang KB, Tsai SC and Chen YC: A possible
musculoskeletal pitfall in 18F-FDG PET: Nodular fasciitis. Ann Nucl
Med Sci. 23:165–168. 2010.
|
|
6
|
Edge SB and Compton CC: The American joint
committee on cancer: The 7th edition of the ajcc cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shaha AR, Ferlito A and Rinaldo A: Distant
metastases from thyroid and parathyroid cancer. ORL J
Otorhinolaryngol Relat Spec. 63:243–249. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Song HJ, Xue YL, Xu YH, Qiu ZL and Luo QY:
Rare metastases of differentiated thyroid carcinoma: Pictorial
review. Endocr Relat Cancer. 18:R165–R174. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Clark JR, Lai P, Hall F, Borglund A, Eski
S and Freeman JL: Variables predicting distant metastases in
thyroid cancer. Laryngoscope. 115:661–667. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schlumberger M, Tubiana M, De Vathaire F,
Hill C, Gardet P, Travagli JP, Fragu P, Lumbroso J, Caillou B and
Parmentier C: Long-term results of treatment of 283 patients with
lung and bone metastases from differentiated thyroid carcinoma. J
Clin Endocrinol Metab. 63:960–967. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ruegemer JJ, Hay ID, Bergstralh EJ, Ryan
JJ, Offord KP and Gorman CA: Distant metastases in differentiated
thyroid carcinoma: A multivariate analysis of prognostic variables.
J Clin Endocrinol Metab. 67:501–508. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sevinc A, Buyukberber S, Sari R, Baysal T
and Mizrak B: Follicular thyroid cancer presenting initially with
soft tissue metastasis. Jpn J Clin Oncol. 30:27–29. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Califano I, Quildrian S, Coduti M, Bilbao
E Rojas, Otero J and Califano L: Soft tissue metastases from
differentiated thyroid cancer diagnosed by 18F FDG PET-CT. Arq Bras
Endocrinol Metabol. 57:317–321. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rodrigues G and Ghosh A: Synchronous bony
and soft tissue metastases from follicular carcinoma of the
thyroid. J Korean Med Sci. 18:914–916. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Shaha AR, Shah JP and Loree TR:
Differentiated thyroid cancer presenting initially with distant
metastasis. Am J Surg. 174:474–476. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Durante C, Haddy N, Baudin E, Leboulleux
S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De
Vathaire F and Schlumberger M: Long-term outcome of 444 patients
with distant metastases from papillary and follicular thyroid
carcinoma: Benefits and limits of radioiodine therapy. J Clin
Endocrinol Metab. 91:2892–2899. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Asagi A, Ohta K, Nasu J, Tanada M, Nadano
S, Nishimura R, Teramoto N, Yamamoto K, Inoue T and Iguchi H:
Utility of contrast-enhanced FDG-PET/CT in the clinical management
of pancreatic cancer: Impact on diagnosis, staging, evaluation of
treatment response and detection of recurrence. Pancreas. 42:11–19.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Groheux D, Hindié E, Marty M, Espié M,
Rubello D, Vercellino L, Bousquet G, Ohnona J, Toubert ME, Merlet P
and Misset JL: 18F-FDG-PET/CT in staging, restaging, and treatment
response assessment of male breast cancer. Eur J Radiol.
83:1925–1933. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cayvarli H, Bekis R, Akman T and Altun D:
The role of 18F-FDG PET/CT in the evaluation of gastric cancer
recurrence. Mol Imaging Radionucl Ther. 23:76–83. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
de Geus-Oei LF, Vriens D, van Laarhoven
HW, van der Graaf WT and Oyen WJ: Monitoring and predicting
response to therapy with 18F-FDG PET in colorectal cancer: A
systematic review. J Nucl Med. 50 Suppl 1:43S–54S. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bestic JM, Peterson JJ and Bancroft LW:
Pediatric FDG PET/CT: Physiologic uptake, normal variants, and
benign conditions (corrected). Radiographics. 29:1487–1500. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wahl RL: Current status of PET in breast
cancer imaging, staging, and therapy. Semin Roentgenol. 36:250–260.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aoki J, Watanabe H, Shinozaki T, Takagishi
K, Ishijima H, Oya N, Sato N, Inoue T and Endo K: FDG PET of
primary benign and malignant bone tumors: Standardized uptake value
in 52 lesions. Radiology. 219:774–777. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Keyes JW Jr: SUV: Standard uptake or silly
useless value? J Nucl Med. 36:1836–1839. 1995.PubMed/NCBI
|
|
25
|
Visser EP, Boerman OC and Oyen WJ: SUV:
From silly useless value to smart uptake value. J Nucl Med.
51:173–175. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hu SL, Yang ZY, Zhou ZR, Yu XJ, Ping B and
Zhang YJ: Role of SUV(max) obtained by 18F-FDG PET/CT in patients
with a solitary pancreatic lesion: Predicting malignant potential
and proliferation. Nucl Med Commun. 34:533–539. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Park SA, Lee KM, Choi U, Kim HS, Kim HW
and Song JH: Normal physiologic and benign foci with F-18 FDG
avidity on PET/CT in patients with breast cancer. Nucl Med Mol
Imaging. 44:282–289. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Tahara T, Ichiya Y, Kuwabara Y, Otsuka M,
Miyake Y, Gunasekera R and Masuda K: High [18F]-fluorodeoxyglucose
uptake in abdominal abscesses: A PET study. J Comput Assist Tomogr.
13:829–831. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Meyer MA, Frey KA and Schwaiger M:
Discordance between F-18 fluorodeoxyglucose uptake and contrast
enhancement in a brain abscess. Clin Nucl Med. 18:682–684. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Slosman DO, Spiliopoulos A, Keller A,
Lemoine R, Besse F, Couson F, Townsend D and Rochat T: Quantitative
metabolic PET imaging of a plasma cell granuloma. J Thorac Imaging.
9:116–119. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Patz EF Jr, Lowe VJ, Hoffman JM, Paine SS,
Burrowes P, Coleman RE and Goodman PC: Focal pulmonary
abnormalities: Evaluation with F-18 fluorodeoxyglucose PET
scanning. Radiology. 188:487–490. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lewis PJ and Salama A: Uptake of
fluorine-18-fluorodeoxyglucose in sarcoidosis. J Nucl Med.
35:1647–1649. 1994.PubMed/NCBI
|
|
33
|
Demir MK, Ozdemir H, Gençhallaç H, Altaner
S and Kartal O: Dermatofibroma mimicking malignancy on integrated
F-18 fluorodeoxyglucose PET-CT. Diagn Interv Radiol. 15:61–63.
2009.PubMed/NCBI
|
|
34
|
de Waele M, Carp L, Lauwers P, Hendriks J,
De Maeseneer M, Van Schil P and Blockx P: Paravertebral schwannoma
with high uptake of fluorodeoxyglucose on positron emission
tomography. Acta Chir Belg. 105:537–538. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zuber TJ and Finley JL: Nodular fasciitis.
South Med J. 87:842–844. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Konwaler BE, Keasbey L and Kaplan L:
Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin
Pathol. 25:241–252. 1955. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Pandian TK, Zeidan MM, Ibrahim KA, Moir
CR, Ishitani MB and Zarroug AE: Nodular fasciitis in the pediatric
population: A single center experience. J Pediatr Surg.
48:1486–1489. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Khuu A, Yablon CM, Jacobson JA, Inyang A,
Lucas DR and Biermann JS: Nodular fasciitis: Characteristic imaging
features on sonography and magnetic resonance imaging. J Ultrasound
Med. 33:565–573. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Dinauer PA, Brixey CJ, Moncur JT,
Fanburg-Smith JC and Murphey MD: Pathologic and MR imaging features
of benign fibrous soft-tissue tumors in adults. Radiographics.
27:173–187. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kong CS and Cha I: Nodular fasciitis:
Diagnosis by fine needle aspiration biopsy. Acta Cytol. 48:473–477.
2004. View Article : Google Scholar : PubMed/NCBI
|