Introduction
Nasopharyngeal carcinoma (NPC) is a common
malignancy in Southeast Asia, particularly in the south of China
(1). Radiotherapy is the primary
standard radical treatment for NPC. However, radiation affects
normal tissues such as the temporal lobe, salivary gland and
cochlea, and accounts for various severe delayed complications and
sequelae, including radiation encephalopathy, salivary xerostomia
and hearing impairment (2,3). Radiation encephalopathy, which was first
described in 1930 by Fischer and Holfelder (4), is one of the complications of NPC
patients previously treated with radiation. The 3- and 5-year
incidence of radiation encephalopathy have been reported to be 10.8
and 34.9%, respectively, following two-dimensional radiotherapy
(2D-RT) (5). In Hong Kong, radiation
encephalopathy in the temporal lobe accounts for 65% of all
mortalities due to radiation-induced complications in patients with
NPC (6). While NPC patients have a
long-term survival following chemoradiotherapy, radiation
encephalopathy is becoming an important factor affecting NPC
patients' quality of life (7).
Therefore, it is vital that radiation encephalopathy is correctly
identified to avoid unnecessary additional investigations or even
inappropriate treatment. Radiation encephalopathy is generally
regarded as a progressive and irreversible process (8). Autopsy findings have shown that
histological features of radiation encephalopathy include reactive
white matter edema, rarefaction of myelin or even demyelination,
fibrinoid changes in the blood vessels, coagulative necrosis and
cysts with reactive gliosis in the walls (9,10).
Pathological examination is the gold-standard evaluation. However,
brain biopsy is an invasive method, and cannot be used to evaluate
the whole lesion or to follow-up the evolution of radiation
encephalopathy. Magnetic resonance imaging (MRI) has been
demonstrated to be a useful and noninvasive method to evaluate
radiation encephalopathy and its evolution (11,12),
although the natural course of radiation encephalopathy remains
poorly understood.
At present, intensity-modulated radiotherapy (IMRT)
is widely employed in the management of NPC, and a highly conformal
dose could be delivered to the planned target volume, which enables
significantly better organ sparing compared with 2D-RT (5). However, radiation encephalopathy was
detected in ~5% of patients following IMRT (13). Therefore, it is still of clinical
interest to analyze the MRI characteristics of radiation
encephalopathy.
In the present study, a series of follow-up MRI
examinations from 68 NPC patients with radiation encephalopathy in
the temporal lobes were analyzed retrospectively. All the patients
had been previously treated with radical radiotherapy for NPC. The
objective of the present study was to provide an improved
understanding of the MRI characteristics and evolution of radiation
encephalopathy, which may help to diagnose and treat radiation
encephalopathy as early as possible.
Materials and methods
Clinical data
A total of 68 radiation encephalopathy patients were
recruited for the present study. All of them had been previously
treated with radical radiotherapy for NPC. The patient cohort
consisted of 42 men and 26 women, with a mean age of 50.3 years
(range, 22–70 years). Approval for the present retrospective
analysis of the patients' data was obtained from the Ethics
Committee of the Second Affiliated Hospital, Zhejiang University
School of Medicine (Hangzhou, China). Informed consent was obtained
when the patients were treated. All patients had pathologically
confirmed NPC. Of these, 67 patients received a radical 2D-RT
regimen with a dose of 70 Gy, while 1 patient had a first radical
2D-RT course with a dose of 70 Gy, followed by a second radiation
course with a dose of 56 Gy for NPC recurrence 13 years after the
first radiotherapy.
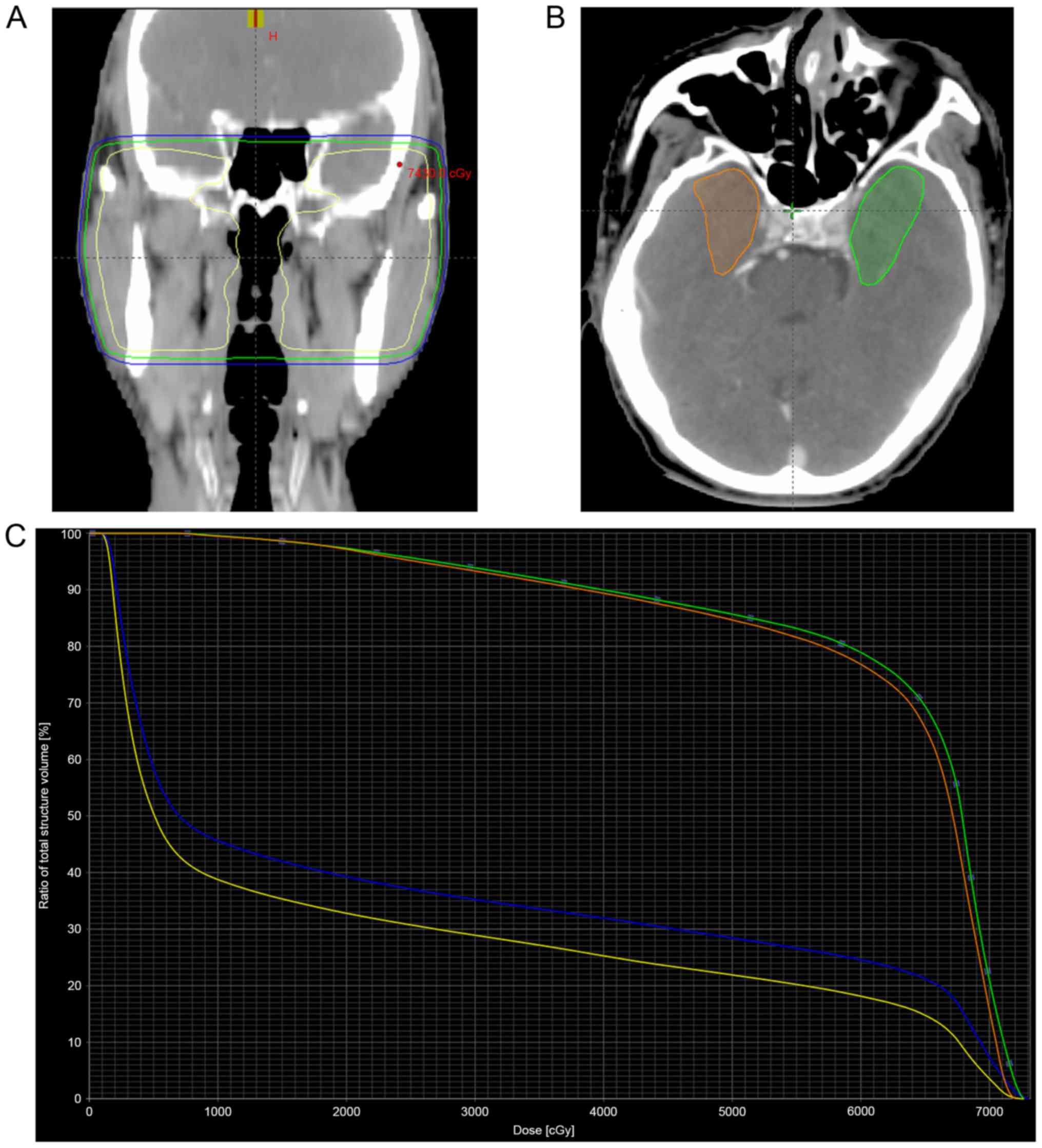
Regarding the 2D-RT data, the exact radiation dose
delivered to the temporal lobes was not available. In order to
estimate the approximate volume and dose delivered to the temporal
lobes, the dose distribution and dose-volume histogram of a patient
treated with 2D-RT were reconstructed (Fig. 1). For this purpose, target volume and
organs at risk were contoured by planning computed tomography. The
dosimetric parameters V50, V60 and V70, represent the temporal lobe
volume that received radiation dose greater than 50, 60 and 70 Gy,
respectively. The inferior-medial aspect of the temporal lobe
received the highest radiation dose, as the V50, V60, V70 and mean
dose of the inferior-medial aspect were remarkably higher than
those of the whole temporal lobe (Table
I). The dose to 0.5 ml of the temporal lobe volume of the
bilateral temporal lobes and their inferior-medial aspects were
both higher than the dose tolerance of 69 Gy suggested by Sun et
al (14).
 | Table I.Dosimetric parameters of bilateral
temporal lobes, and their inferior and medial aspects, in the
patient of Fig. 1, who was treated
with 70 Gy two-dimensional radiotherapy. |
Table I.
Dosimetric parameters of bilateral
temporal lobes, and their inferior and medial aspects, in the
patient of Fig. 1, who was treated
with 70 Gy two-dimensional radiotherapy.
| Parameter | Left temporal
lobe | Right temporal
lobe | Inferior and medial
aspects of the left temporal lobe | Inferior and medial
aspects of the right temporal lobe |
|---|
| V50 | 16.3
cm3 | 10.5
cm3 | 9.3
cm3 | 6.7
cm3 |
| V60 | 13.9
cm3 | 8.4
cm3 | 8.5
cm3 | 6.1
cm3 |
| V70 | 3.8
cm3 | 1.2
cm3 | 2.2
cm3 | 1.2
cm3 |
|
D0.5cc | 72.06 Gy | 70.85 Gy | 71.75 Gy | 70.83 Gy |
| Dmean | 22.34 Gy | 17.45 Gy | 62.19 Gy | 61.30 Gy |
In the Second Affiliated Hospital, Zhejiang
University School of Medicine, NPC patients are recommended to have
contrast enhanced nasopharyngeal MRI examination every 3 months in
the first 2 years, then every 6 months between 3 and 5 years, and
every year thereafter. However, the majority of patients in the
present study did not receive regular MRI examination after the
third year. Brain MRI was performed if any temporal abnormality was
detected. Patients with radiation encephalopathy were identified by
head and neck radiologists. The diagnostic standards for radiation
encephalopathy of NPC were as follows: i) Having a history of
radiotherapy for NPC; ii) having an abnormal signal intensity in
the temporal lobe of the brain, which was identified by follow-up
MRI examinations; and iii) having temporal lobe lesions, which were
detected ≥6 months after radiotherapy (12). Patients with imaging or endoscopic
evidence of tumor invading the cavernous sinus or the floor of the
middle cranial fossa adjacent to the injured temporal lobes were
excluded from the study. Patients with clinical or laboratory
evidence of brain infarction, infection or tumors were also
excluded from the study.
MRI scan technique
MRI was performed using two 1.5-Tesla systems, Signa
HDxt 1.5T (GE Healthcare Life Sciences, Chalfont, UK) and MAGNETOM
Sonata 1.5T (Siemens AG, Munich, Germany) at the Second Affiliated
Hospital of Zhejiang University School of Medicine. Two MRI
protocols were used. The first protocol was a standard follow-up
NPC MRI protocol for patients with NPC. Sequences for the first
protocol included an axial T2-weighted fat-suppressed sequence, an
axial T1-weighted spin-echo sequence and a contrast enhanced
T1-weighted spin-echo sequence in the axial, coronal and sagittal
planes following a bolus injection of 0.1 mmol gadopentetate
dimeglumine (Gd-DTPA) (Magnevist; Schering AG; Bayer Leverkusen,
Germany) per kg of body weight. The second protocol was modified to
target the brain. Sequences for the second protocol included an
axial T1-weighted spin-echo sequence and an axial T2-weighted turbo
spin-echo sequence. Post-contrast axial, sagittal and coronal
T1-weighted imaging was performed following an intravenous bolus
injection of 0.1 mmol clinical gadolinium chelate per kg of body
weight, and the imaging parameters were the same as for
pre-contrast imaging.
MRI appearance of radiation
encephalopathy
A total of 68 NPC patients underwent 162 follow-up
MRI examinations upon the occurrence of radiation encephalopathy.
For each patient, the two temporal lobes were assessed separately.
The radiation encephalopathy lesions in the gray and white matter
were assessed by MRI, and the diagnosis of each component of
radiation encephalopathy was based on the following definitions
(6): i) Contrast enhanced lesions
were defined as enhanced lesions on contrast enhanced T1-weighted
images, with or without necrosis. According to the appearance and
the characteristics of lesion enhancement, contrast enhanced
lesions were divided into four groups as follows: Solid enhanced
nodular lesions; enhanced nodular lesions with a necrotic center;
finger-like enhanced lesions; and dotted and patchy enhanced
lesions, often along with temporal lobe atrophy. Dotted and patchy
enhanced lesions usually have lower enhancement intensity compared
with that of the other enhanced lesions mentioned above. ii) White
matter lesions were defined as lesions of homogeneously high signal
intensity on T2-weighted images and low signal intensity on
T1-weighted images. White matter lesions were grouped into three
categories as follows: Local (small focal areas in the temporal
lobe), moderate (larger confluent areas in the temporal lobe) and
diffuse (large diffuse areas extending to the majority of the
temporal lobe). iii) Cysts were defined as round or oval
well-defined lesions, thin-walled, of very high signal intensity on
T2-weighted images. The cysts were evaluated for size, signal
intensity on T1-weighted images and enhancement of the cyst wall
following the administration of contrast medium. iv) Nodular or
annular hypointense lesions that were more hypointense than normal
white matter on both T1- and T2-weighted images were considered as
hemosiderin deposition. v) Gray matter lesions of radiation
encephalopathy were defined as disruption or erosion of
hyperintensity in the cortex on T2-weighted images. vi) Temporal
lobe atrophy was considered if there was a subjective decrease in
the size of the temporal lobe on MRI. In the process of review of
follow-up MRI examinations, the head and neck radiologists excluded
patients with clinical or laboratory evidence of brain tumor,
infarction, infection or NPC invading the tissue of the middle
cranial fossa.
The interval time between radiotherapy and the first
detection of any of the above lesions characteristic of radiation
encephalopathy was calculated. The median interval time between
radiotherapy and the first MRI detection of radiation
encephalopathy was 37 months (range, 12–156 months), and the mean
interval time was 46.5 months. For the purpose of evaluating the
full range and evolution of radiation encephalopathy, the
appearance of each component of radiation encephalopathy was
assessed in every MRI examination.
Evolution of individual lesions and
changes over time
For the purpose of evaluating the evolution of each
individual lesion of radiation encephalopathy, each type of lesion
was assessed over the course of 162 follow-up MRI examinations upon
radiation encephalopathy occurrence. To analyze the overall pattern
of abnormalities in radiation encephalopathy, the association
between white matter lesions and contrast enhanced lesions was
assessed for each MRI examination.
Results
Initial temporal lobe abnormalities at
the first MRI diagnosis of radiation encephalopathy
A total of 105 injured temporal lobes were
identified at the initial MRI examination in the 68 cases of
radiation encephalopathy analyzed in the present study. Unilateral
and bilateral temporal lobe lesions were detected in 31 (45.6%) and
37 (54.4%) of the 68 patients, respectively. For the cases with
unilateral lesions, 16 were identified in the left temporal lobe,
and the other 15 in the right temporal lobe.
Contrast enhanced lesions were detected in all 105
temporal lobes. Among these, 57 temporal lobes presented with solid
enhanced nodular lesions, 24 exhibited enhanced nodular lesions
with a necrotic center, 12 had finger-like enhanced lesions, and 12
had dotted and patchy enhanced lesions. White matter lesions were
detected in 98 (93.3%) of the 105 temporal lobes. Local, moderate
and diffuse white matter lesions were detected in 41, 21 and 36
temporal lobes, respectively. Gray matter lesions were observed in
94 (89.5%) of the 105 temporal lobes. Cysts and hemosiderin
deposition were noticed in 2 temporal lobes. No temporal lobe
atrophy was observed at the MRI examination when radiation
encephalopathy was first diagnosed.
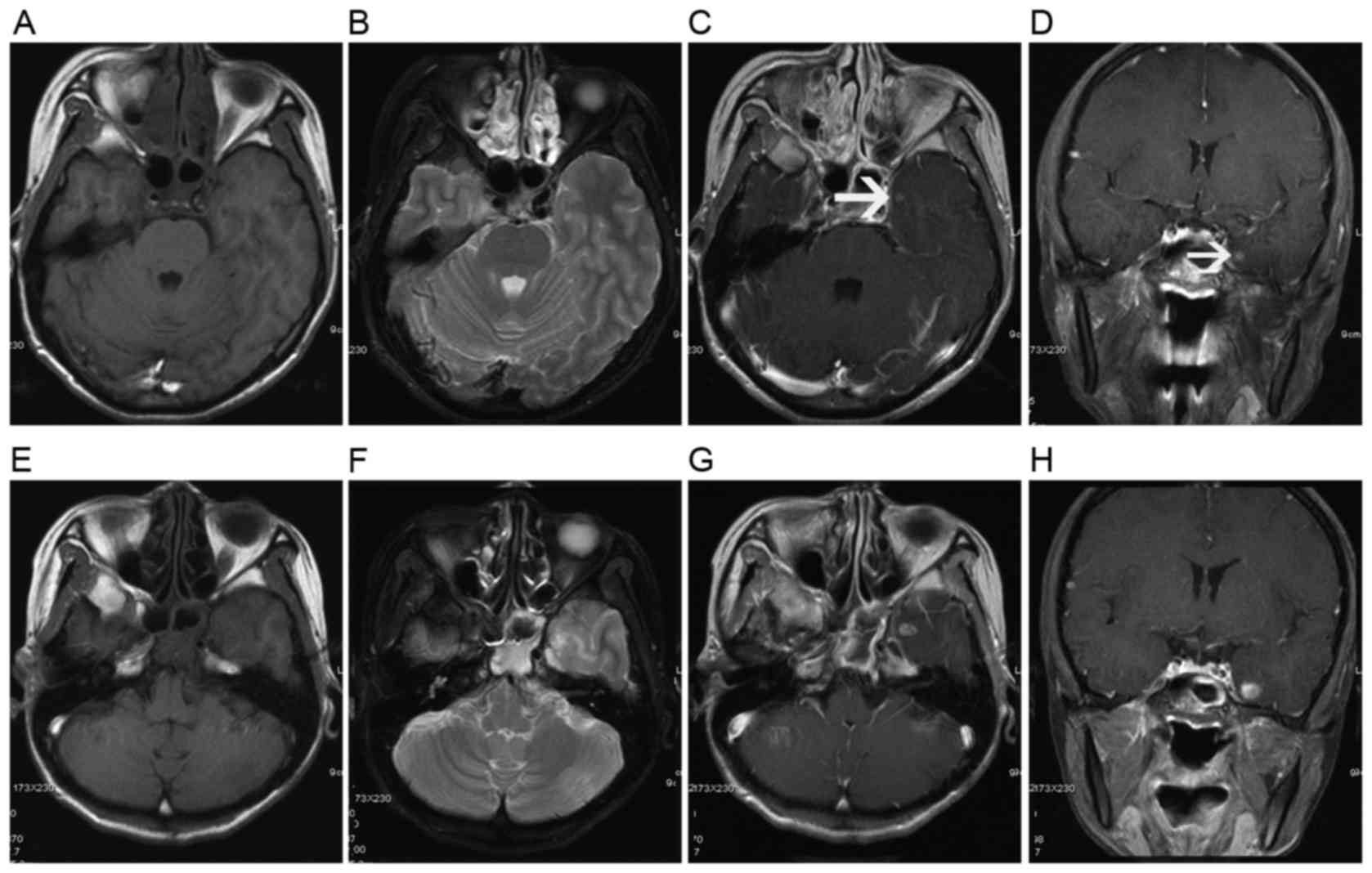
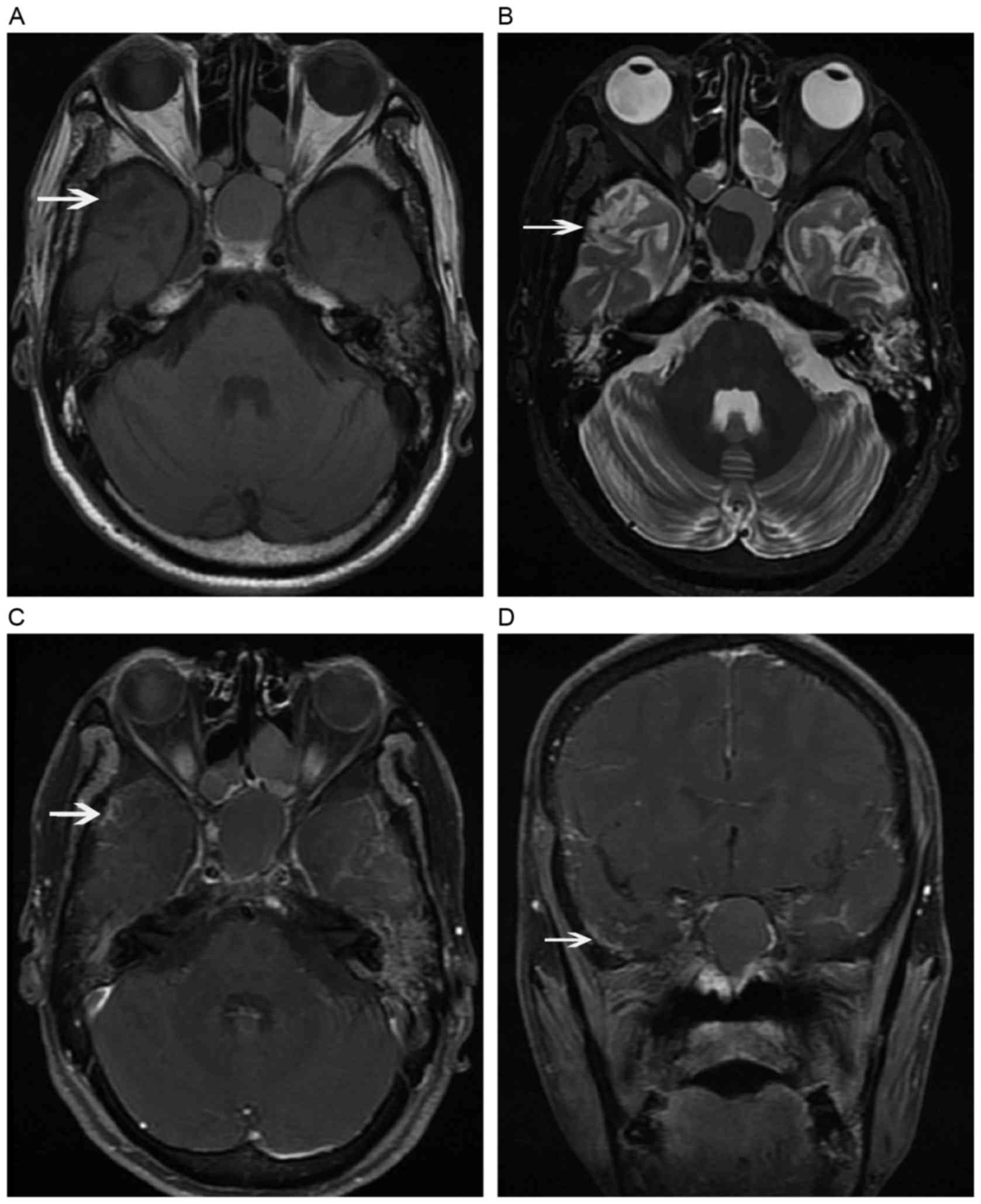
It is important to mention that, in 7 affected
temporal lobes, solid enhanced nodular lesions were presented as
the only initial abnormality (Fig.
2). For these 7 solid enhanced nodular lesions, the previous
negative MRI examinations were performed at a median time of 5.5
months prior to MRI detection of radiation encephalopathy. The
median time interval was <10.5 months (range, 2.5–24.5 months)
for patients detected with ≥2 MRI components of radiation
encephalopathy, e.g., contrast enhanced lesions, white matter
lesions, cysts, gray matter lesions or temporal lobe atrophy.
New MRI abnormalities detected during
the follow-up process of radiation encephalopathy
During the follow-up process, 12 cases originally
presented as unilateral temporal lobe lesions were observed to
exhibit new lesions in the other side of the temporal lobes. Solid
enhanced nodular lesions were initially detected as the only
abnormality in 4 temporal lobes, and contrast enhanced lesions
together with white matter lesions were detected in the other 8
temporal lobes. Regarding the enhanced patterns, solid enhanced
nodular lesions, enhanced nodular lesions with a necrotic center
and finger-like enhanced lesions were newly detected in 7, 1 and 4
temporal lobes, respectively.
New local white matter lesions were noticed in all
the 11 temporal lobes where solid enhanced nodular lesions were
initially detected as the only abnormality, and the time interval
between the detection of a solid enhanced nodular lesion and the
appearance of local white matter lesions was 3.0–24.5 months (mean,
7.8 months).
Evolution of MRI abnormalities during
the follow-up process of radiation encephalopathy
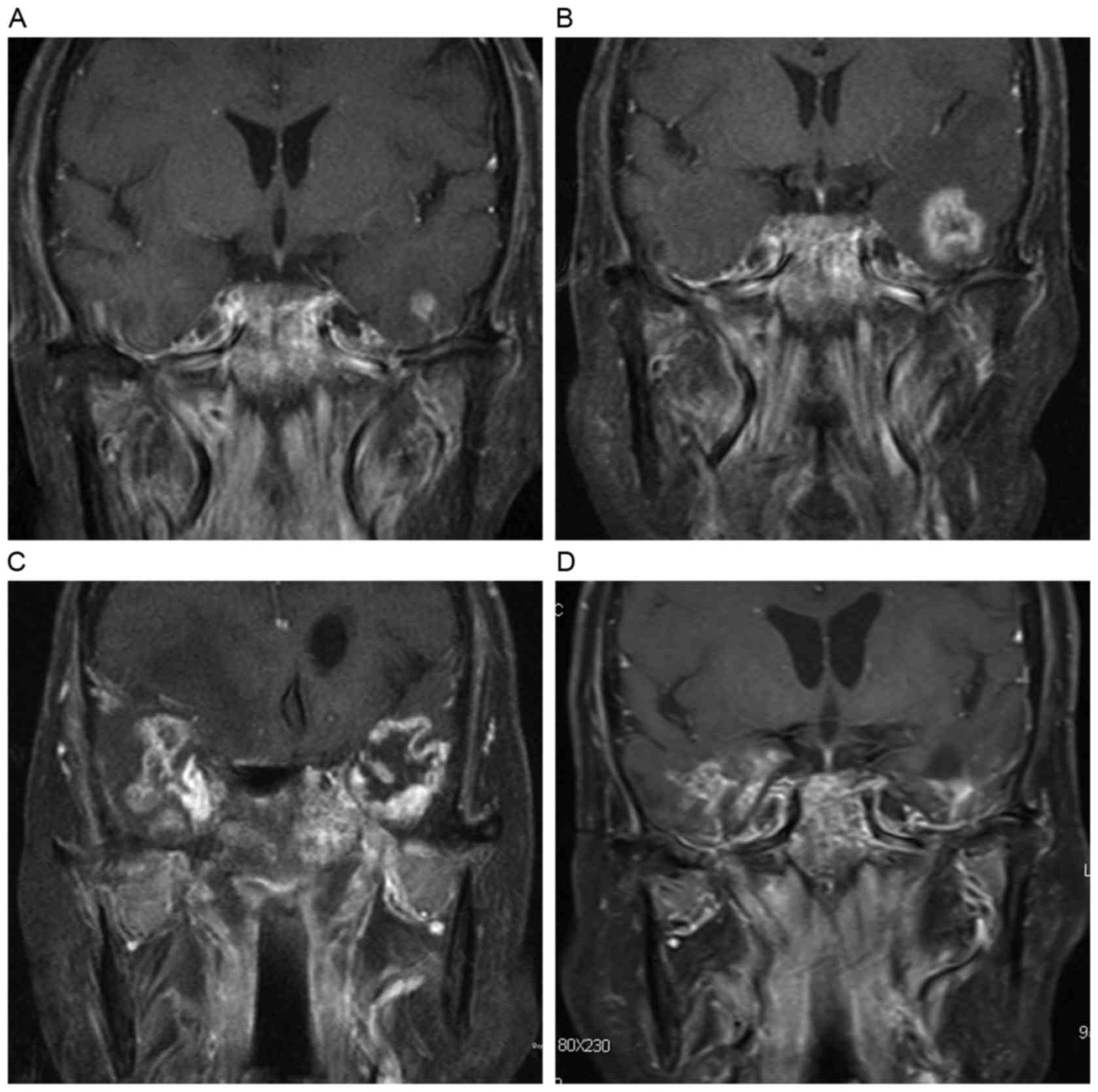
Contrast enhanced lesions usually originated from
the gray-white matter junction of the inferior-medial aspect of the
temporal lobes. Solid enhanced nodular lesions increased in size
and tended to be necrotic at a mean maximal diameter of 1.5 cm
(range, 0.8–3.0 cm). The incidence rate of a necrotic core for
enhanced nodular lesions of size <1, 1.0–1.5, 1.6–2.0 and >2
cm in diameter was 7.7, 41.5, 81.8 and 100.0%, respectively. For
those enhanced nodular lesions measuring <0.8 cm, no necrosis
could be detected. On the contrary, all the contrast enhanced
lesions that were larger than 2 cm displayed a necrotic core.
Enhanced nodular lesions with a necrotic center continued to
increase in size, extended to the gray-white matter junction of the
superior-lateral aspect of the temporal lobes and formed
finger-like enhanced lesions. Subsequently, the lesions decreased
and regressed both in size and signal intensity, as indicated by
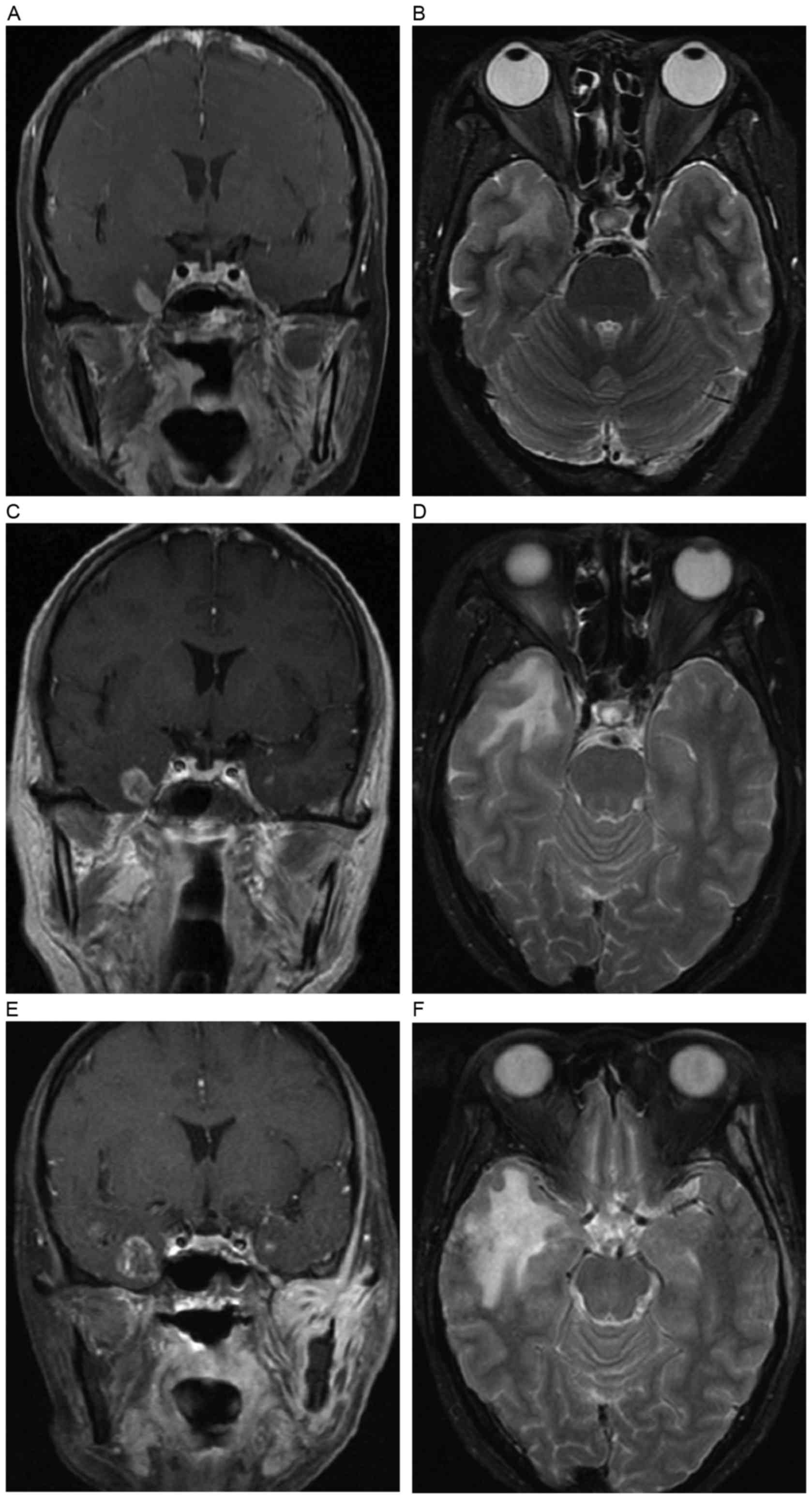
the dotted and patchy enhanced lesions shown in Fig. 3.
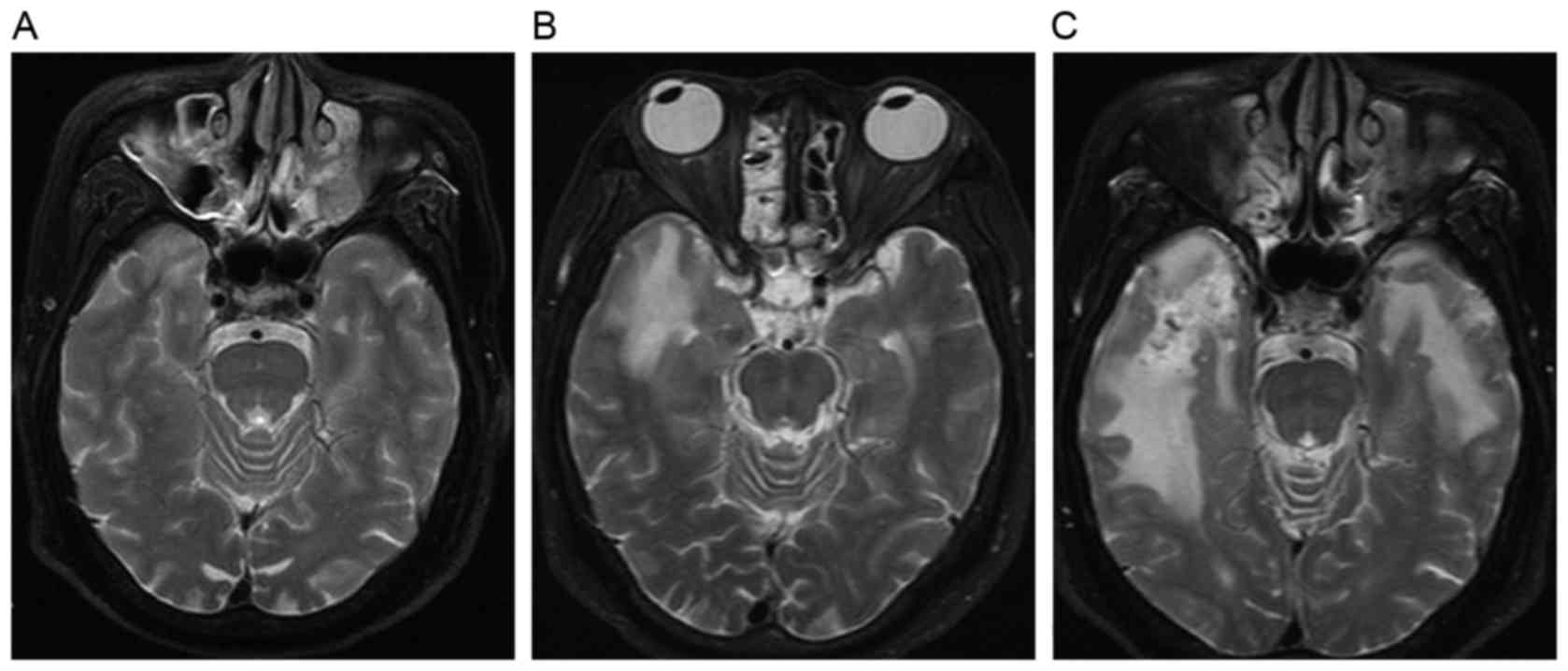
White matter lesions also originated from the
gray-white matter junction of the inferior-medial aspect of the
temporal lobes, and developed from local lesions to moderate and
diffuse white matter lesions with time (Fig. 4). Diffuse white matter lesions
decreased both in size and signal intensity with the occurrence of
temporal lobe atrophy. However, the development from diffuse white
matter lesion to local white matter lesion was not detected in the
present study.
In the current study, 77 temporal lobe lesions
underwent ≥2 follow-up MRI examinations following radiation
encephalopathy occurrence. The evolution pattern of contrast
enhanced lesions and white matter lesions could be classified as
increasing, decreasing or stable in extent or size. Contrast
enhanced lesions and white matter lesions were observed to change
with the same evolution pattern in 72 (93.5%) of 77 temporal lobes:
Increasing, decreasing, increasing followed by decreasing and
stable in 33 (42.9%), 14 (18.2%), 13 (16.9%) and 12 (15.6%) of the
77 temporal lobes, respectively (Fig.
5). The median interval time between the first MRI examination
of radiation encephalopathy and lesion increasing was 10.5 months,
while the corresponding interval time for decreasing lesions was
20.5 months. In the other 5 (6.5%) temporal lobes, different
evolution patterns were observed: White matter lesion stable and
contrast enhanced lesion increasing in 3 temporal lobes, and white
matter lesion decreasing and contrast enhanced lesion stable in 2
temporal lobes (Table II).
| Table II.Association between WMLs and CELs in
temporal lobes, and their changes over time. |
Table II.
Association between WMLs and CELs in
temporal lobes, and their changes over time.
| Lesion evolution | CEL increasing, n
(%) | CEL decreasing, n
(%) | CEL increasing
followed by decreasing, n (%) | CEL stable, n
(%) |
|---|
| WML increasing | 33
(42.9)a | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| WML decreasing | 0 (0.0) | 14 (18.2) | 0 (0.0) | 2 (2.6) |
| WML increasing
followed by decreasing | 0 (0.0) | 0 (0.0) | 13 (16.9) | 0 (0.0) |
| WML stable | 3 (3.9) | 0 (0.0) | 0 (0.0) | 12 (15.6) |
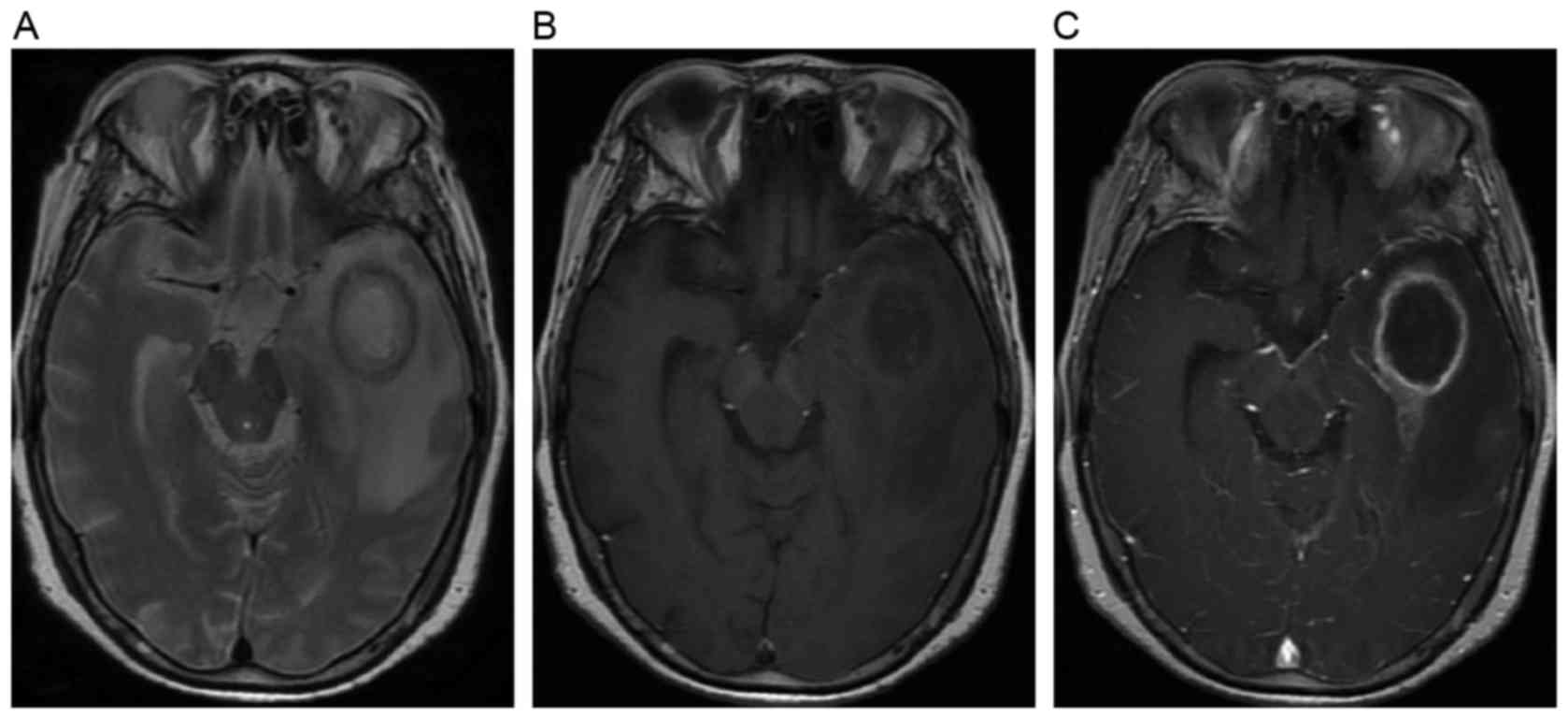
All the cysts that occurred subsequent to necrosis
presented as round or oval well-defined lesions with hypointensity
on T1-weighted images and hyperintensity on T2-weighted images.
Cyst wall enhancement could be occasionally detected on
post-contrast T1-weighted images (Fig.
6). Hemosiderin deposition was observed as hypointensity on
both T1- and T2-weighted images, accompanied by hemorrhage of
hyperintensity on both T1- and T2-weighted images in certain
cases.
Gray matter lesions arose in 89.5% of temporal lobes
at the first MRI detection of radiation encephalopathy, and reached
98.3% at the last follow-up. Gray matter lesions progressed mildly
and slowly, and presented as disruption or erosion of the cortex on
both T1- and T2-weighted images, with contrast enhancement on
post-contrast T1-weighted images (Fig.
7). Temporal lobe atrophy occurred at the late stage of
radiation encephalopathy.
The MRI abnormalities detected during the continuous
follow-up MRI examinations are presented in Table III, which indicated the dynamic
changes of the different abnormal MRI components.
| Table III.Composition of abnormal MRI components
at continuous FU MRI examinations. |
Table III.
Composition of abnormal MRI components
at continuous FU MRI examinations.
|
| Diagnostic
MRIa (n=117) | 1st MRI FU
(n=77) | 2nd MRI FU
(n=51) | 3rd MRI FU
(n=20) | 4th MRI FU (n=5) |
|---|
|
|
|
|
|
|
|
|---|
| Radiation
encephalopathy components | N | % | N | % | N | % | N | % | N | % |
|---|
| Contrast enhanced
lesions | 117 | 100.0 | 77 | 100.0 | 51 | 100.0 | 20 | 100.0 | 5 | 100.0 |
| Solid
enhanced nodular lesions | 64 | 54.7 | 20 | 26.0 | 2 | 3.9 | 0 | 0.0 | 1 | 20.0 |
|
Enhanced nodular lesions with
necrotic centers | 25 | 21.4 | 25 | 32.5 | 12 | 23.5 | 4 | 20.0 | 1 | 20.0 |
|
Finger-like enhanced
lesions | 16 | 13.7 | 21 | 27.3 | 19 | 37.3 | 6 | 30.0 | 0 | 0.0 |
| Dotted
and patchy enhanced lesions | 12 | 10.3 | 11 | 14.3 | 18 | 35.3 | 10 | 50.0 | 3 | 60.0 |
| White matter
lesions | 106 | 90.6 | 77 | 100.0 | 51 | 100.0 | 20 | 100.0 | 5 | 100.0 |
|
Local | 44 | 37.6 | 17 | 22.1 | 2 | 3.9 | 0 | 0.0 | 0 | 0.0 |
|
Moderate | 21 | 17.9 | 20 | 26.0 | 9 | 17.6 | 3 | 15.0 | 3 | 60.0 |
|
Diffuse | 41 | 35.0 | 40 | 51.9 | 40 | 78.4 | 17 | 85.0 | 2 | 40.0 |
| Cysts | 2 | 1.7 | 0 | 0.0 | 4 | 7.8 | 2 | 10.0 | 2 | 40.0 |
| Hemosiderin
deposition | 2 | 1.7 | 3 | 3.9 | 3 | 5.9 | 3 | 15.0 | 1 | 20.0 |
| Gray matter
lesions | 98 | 83.8 | 75 | 97.4 | 51 | 100.0 | 20 | 100.0 | 5 | 100.0 |
| Temporal lobe
atrophy | 0 | 0.0 | 11 | 14.3 | 8 | 15.7 | 9 | 45.0 | 4 | 80.0 |
At the end of the follow-up period, unilateral
radiation encephalopathy was noticed in 19 patients, while
bilateral radiation encephalopathy was detected in 49 patients,
with a total of 117 injured temporal lobes in all the 68 cases.
Contrast enhanced lesions and white matter lesions were detected in
all the 117 temporal lobes. At the late stage of radiation
encephalopathy, the majority of diffuse white matter lesions were
detected together with finger-like or dotted and patchy enhanced
lesions. Gray matter lesions, temporal lobe atrophy, cysts and
hemosiderin deposition were detected in 115 (98.3%), 24 (20.5%) and
6 (5.1%) of the 117 temporal lobes, respectively.
Discussion
To the best of our knowledge, the present study is
the first to describe solid enhanced nodular lesions as the
earliest MRI abnormalities of radiation encephalopathy following
NPC radiotherapy. In the present study, at the time of the initial
MRI diagnosis of radiation encephalopathy, contrast enhanced
lesions were detected in all the injured temporal lobes, while
white matter lesions were detected in 93.3% of cases, followed by
gray matter lesions, cysts and hemosiderin deposition. Importantly,
a solid enhanced nodular lesion was observed to be the first and
only MRI abnormality of radiation encephalopathy in 11 out of the
117 involved temporal lobes, and was the only imaging pattern of
MRI abnormality for several months (range, 3.0–24.5 months; mean,
7.8 months) before a second component of MRI abnormality (usually a
local white matter lesion) appeared in the MRI follow-up.
Concerning the earliest MRI abnormality, the present findings are
inconsistent with previous studies, in which contrast enhanced
lesions were reported to occur subsequently or concurrently with
white matter lesions. In the study by Wang et al (15), white matter lesions were reported to
be the only lesion to occur alone, and were detected in 100% of all
the injured temporal lobes. On the contrary, only 82.5% of the
injured temporal lobes exhibited contrast enhanced lesions in that
study. In another report, Chan et al (6) also reported white matter lesions as the
only abnormal finding of MRI, and contrast enhanced lesions were
observed in 89% of all the injured temporal lobes. The median time
interval between previous negative MRI examinations and a
subsequent MRI detections of radiation encephalopathy was 10.5
months in the present study, compared with 20.5 months in the study
by Wang et al (15). Shorter
MRI examination intervals may have the advantage of identifying
earlier MRI abnormality of radiation encephalopathy.
Although NPC patients are recommended to receive
contrast enhanced nasopharyngeal MRI examination according to the
aforementioned follow-up schedule, the majority of patients in the
present study did not receive regular MRI examination after the
third year. As patients with radiation encephalopathy are usually
asymptomatic at the early stage, the injured temporal lobes were
detected incidentally in numerous patients. Thus, the first MRI
detection of radiation encephalopathy could occur at any stage of
the disease course, from early to late stage. Therefore, there is
an obvious limitation to estimate the exact timing of the
occurrence and development of each MRI pattern of radiation
encephalopathy. Theoretically, shorter intervals between each MRI
examination may reveal more information closer to the natural
history of radiation encephalopathy. The median time interval
between a previous negative MRI examination and a subsequent MRI
detection of radiation encephalopathy was 10.5 months in the
present series, compared with 20.5 months in the study by Wang
et al (15). At the first MRI
diagnosis of radiation encephalopathy, solid enhanced nodular
lesions were detected as the only initial abnormality in 7 affected
temporal lobes. For these 7 cases with solid enhanced nodular
lesions, the time interval between the first MRI detection of
radiation encephalopathy and the previous negative MRI examination
was shorter than that for those with multiple MRI components at the
time of detection of radiation encephalopathy (5.5 vs. 10.5 months,
respectively). In the follow-up process, 12 cases that originally
presented as unilateral temporal lobe lesions were observed to
exhibit new lesions in the other side of the temporal lobes. Solid
enhanced nodular lesions were initially detected as the first and
only lesion to occur in 4 of these 12 temporal lobes. The time from
the previous negative MRI scan was 6.8 months in these 4 cases,
which was shorter than that of the other 8 cases with multiple MRI
components. Therefore, it can be proposed that solid enhanced
nodular lesions may be the earliest MRI abnormalities to occur
alone in the majority of radiation encephalopathy cases.
In the present study, contrast enhanced lesions were
detected in all the injured temporal lobes, and were the most
common component of MRI abnormalities in radiation encephalopathy.
Of all the contrast enhanced lesions, >50% were solid enhanced
nodules without necrosis on MRI, which were located in the
inferior-medial aspects of the temporal lobe, where the highest
irradiation dose was delivered. Solid enhanced nodular lesions were
usually small, and as the lesions increased in size, the lesions
tended to be necrotic; thus, they were termed enhanced nodular
lesions with necrotic centers. Taken solid enhanced nodular lesions
and enhanced nodular lesions with necrotic centers together, only
7.7% of the lesions measuring <1 cm displayed a necrotic center;
93.1% of the lesions measuring >1.5 cm exhibited necrotic
centers; and all the lesions measuring >2 cm exhibited necrotic
centers. These findings are in concordance with the study by Wang
et al (15), who reported that
all the lesions with size ≥2 cm exhibited a central necrotic core.
Enhanced nodular lesions with a necrotic center continued to
enlarge and extended to the gray-white matter junction of the
superior-lateral aspect of the temporal lobes, forming finger-like
enhanced lesions. Subsequently, the lesions decreased and regressed
both in size and signal intensity, and formed dotted and patchy
enhanced lesions.
In the present study, white matter lesions were the
second most common MRI appearance at the first MRI detection of
radiation encephalopathy, and were observed in 93.3% of all the
injured temporal lobes. Local or moderate white matter lesions were
detected in the majority of lobes, while diffuse lesions were
noticed in 1/3 of cases. Diffuse white matter lesions were always
detected together with finger-like or dotted and patchy enhanced
lesions. In addition, local white matter lesions were detected
predominantly in the inferior-medial aspects of the temporal lobe,
where the highest irradiation dose was delivered. During the
follow-up process, these white matter lesions extended to the
gray-white matter junction of the superior-lateral aspect of the
temporal lobes. At the end of the follow-up period, white matter
lesions were detected in all the injured temporal lobes, with 61.5%
of them being diffuse white matter lesions.
Gray matter lesions arose in ~80.0% of all temporal
lobes at the first MRI detection of radiation encephalopathy, and
reached 98.3% at the last follow-up. Chan et al (6) reported a similar incidence of 87.7% (50
of 57 injured temporal lobes) in a previous study. Gray matter
lesions were often presented as disruption or erosion of the cortex
in the focal region, and progressed mildly and slowly. Gray matter
may be more tolerant to radiation than white matter due to a
different microstructure (16,17). Cysts
and hemosiderin deposition often occurred following necrosis, which
is consistent with previous studies (6,13,14,18).
The median interval time between radiotherapy and
the first MRI detection of radiation encephalopathy was 37 months
in our series, which is similar to the 36 months reported by Wang
et al (15). However, longer
periods (i.e., 55.9 and 44.5 months) were reported by Norris et
al (18) and Mao et al
(13), respectively. In the present
study, bilateral temporal lobes lesions were detected in 54.4% of
patients when a diagnosis of radiation encephalopathy was
established, and this number increased to 72.1% at the last
follow-up. The incidence of bilateral radiation encephalopathy has
been reported to be 67.6% (6), 54.8%
(13) and 77.8% (15). Radiation encephalopathy in bilateral
temporal lobes appears to be more frequently observed with 2D-RT
compared with IMRT (5). This is
possibly due to the fact that parallel opposed beams were
administered to the NPC radiation field, and both temporal lobes
received approximately the same radiation dose, as demonstrated in
Fig. 1. In the era of IMRT, better
organ sparing compared with 2D-RT is possible to achieve
clinically. As a result, if the tumor is close to one side of the
temporal lobe, the other side will not receive an unnecessary high
dose of radiation (14). A low
bilateral radiation encephalopathy rate of 27.8% has been reported
for IMRT (13), and it could be
speculated that radiation encephalopathy in unilateral other than
bilateral temporal lobes will be more common in the following
years.
In conclusion, the present study is the first to
describe solid enhanced nodular lesions as the earliest MRI
abnormalities of radiation encephalopathy following NPC
radiotherapy. Contrast enhanced lesions and white matter lesions
arose from the inferior-medial aspects of temporal lobes, where the
highest irradiation dose was delivered, and extended to the
gray-white matter junction of the superior-lateral aspect of the
temporal lobes. Solid enhanced nodular lesions appeared at the
early stage of radiation encephalopathy, followed by enhanced
nodular lesions with a necrotic center and finger-like enhanced
lesions. As the lesions increased in size, dotted and patchy
enhanced lesions were detected at the late stage of radiation
encephalopathy. Local white matter lesions developed into moderate
lesions, and then diffuse white matter lesions with time. In the
majority of cases, contrast enhanced lesions and white matter
lesions were observed to change with the same evolution pattern.
Temporal lobe atrophy, cysts and hemosiderin deposition occurred at
the late stage of radiation encephalopathy. To the best of our
knowledge, the present study revealed, for the first time, solid
enhanced nodular lesions as the earliest MRI abnormalities of
radiation encephalopathy following NPC radiotherapy. These results
may help to the early diagnosis of radiation encephalopathy.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant nos. 81071823 and
81201811) and Zhejiang University Research Foundation (grant no.
11-491020-311).
References
|
1
|
Cao SM, Simons MJ and Qian CN: The
prevalence and prevention of nasopharyngeal carcinoma in China.
Chin J Cancer. 30:114–119. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lee AW, Ng WT, Hung WM, Choi CW, Tung R,
Ling YH, Cheng PT, Yau TK, Chang AT, Leung SK, et al: Major late
toxicities after conformal radiotherapy for nasopharyngeal
carcinoma-patient-and treatment-related risk factors. Int J Radiat
Oncol Biol Phys. 73:1121–1128. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jen YM, Shih R, Lin YS, Su WF, Ku CH,
Chang CS, Shueng PW, Hwang JM, Liu DW, Chao HL, et al: Parotid
gland-sparing 3-dimensional conformal radiotherapy results in less
severe dry mouth in nasopharyngeal cancer patients: A dosimetric
and clinical comparison with conventional radiotherapy. Radiother
Oncol. 75:204–209. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fischer AW and Holfelder H: Lokales
amyloid in gehirn. Dtsch Zchir. 227:475–483. 1930. View Article : Google Scholar
|
|
5
|
Zhou GQ, Yu XL, Chen M, Guo R, Lei Y, Sun
Y, Mao YP, Liu LZ, Li L, Lin AH and Ma J: Radiation-induced
temporal lobe injury for nasopharyngeal carcinoma: A comparison of
intensity-modulated radiotherapy and conventional two-dimensional
radiotherapy. PLoS One. 8:e674882013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chan YL, Leung SF, King AD, Choi PH and
Metreweli C: Late radiation injury to the temporal lobes:
Morphorlogic evaluation at MR imaging. Radiology. 213:800–807.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee AW, Ng SH, Ho JH, Tse VK, Poon YF, Tse
CC, Au GK, O SK, Lau WH and Foo WW: Clinical diagnosis of late
temporal lobe necrosis following radiation therapy for
nasopharyngeal carcinoma. Cancer. 61:1535–1542. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Valk PE and Dillon WP: Radiation injury of
the brain. AJNR Am J Neuroradiol. 12:45–62. 1991.PubMed/NCBI
|
|
9
|
Husain MM and Garcia JH: Cerebral
‘radiation necrosis’: Vascular and glial features. Acta
Neuropathol. 36:381–385. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Okeda R and Shibata T: Radiation
encephalopathy-an autopsy case and some comments on the
pathogenesis of delayed radionecrosis of central nervous system.
Acta Pathol Jpn. 23:867–883. 1973.PubMed/NCBI
|
|
11
|
Chan KC, Khong PL, Cheung MM, Wang S, Cai
KX and Wu EX: MRI of late microstructural and metabolic alterations
in radiation-induced brain injuries. J Magn Reson Imaging.
29:1013–1020. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Greene-Schloesser D, Robbins ME, Peiffer
AM, Shaw EG, Wheeler KT and Chan MD: Radiation-induced brain
injury: A review. Front Oncol. 2:732012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mao YP, Zhou GQ, Liu LZ, Guo R, Sun Y, Li
L, Lin AH, Zeng MS, Kang TB, Jia WH, et al: Comparison of
radiological and clinical features of temporal lobe necrosis in
nasopharyngeal carcinoma patients treated with 2D radiotherapy or
intensity-modulated radiotherapy. Br J Cancer. 110:2633–2639. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sun Y, Zhou GQ, Qi ZY, Zhang L, Huang SM,
Liu LZ, Li L, Lin AH and Ma J: Radiation-induced temporal lobe
injury after intensity modulated radiotherapy in nasopharyngeal
carcinoma patients: A dose-volume-outcome analysis. BMC Cancer.
13:3972013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang YX, King AD, Zhou H, Leung SF, Abrigo
J, Chan YL, Hu CW, Yeung DK and Ahuja AT: Evolution of
radiation-induced brain injury: MR imaging-based study. Radiology.
254:210–218. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Medin PM, Foster RD, van der Kogel AJ,
Sayre JW, McBride WH and Solberg TD: Spinal cord tolerance to
single-fraction partial-volume irradiation: A swine model. Int J
Radiat Oncol Biol Phys. 79:226–232. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Medin PM, Foster RD, van der Kogel AJ,
Sayre JW, McBride WH and Solberg TD: Spinal cord tolerance to
reirradiation with single-fraction radiosurgery: A swine model. Int
J Radiat Oncol Biol Phys. 83:1031–1037. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Norris AM, Carrington BM and Slevin NJ:
Late radiation change in the CNS: MR imaging following gadolinium
enhancement. Clin Radiol. 52:356–362. 1997. View Article : Google Scholar : PubMed/NCBI
|