Introduction
Brain metastases (BMs) are common in patients with
cancer, with a rate of occurrence of 20–40% (1). The prognosis concerning the survival of
patients with BMs is poor, with a 3–5-month median survival time,
even when various types of treatments are attempted (2–4). Whole
brain radiotherapy (WBRT) has been regarded as the standard
treatment for BMs. One of the aims of WBRT has been to prevent the
mortality of the patient from BMs, and to achieve longer overall
survival (OS) (5); however, numerous
studies have suggested that WBRT does not prolong the OS of
patients with BMs (6–8). Advances in chemotherapy and
molecular-targeted drugs have improved patient survival following
the appearance of distant metastasis, including brain metastasis
(9). For certain patients with brain
metastases and good prognosis, stereotactic radiosurgery (SRS) and
stereotactic radiotherapy (SRT) that have improved local control
compared with WBRT have been recommended (10–18), and
the primary objective of the WBRT has been increasingly to palliate
neurological symptoms and to improve or maintain the patients'
quality of life (QOL) (19) BMs cause
headaches in 49% of patients, focal weakness in 30%, mental
disturbances in 32%, gait ataxia in 21%, seizures in 18% and other
symptoms, leading to a lower QOL (8).
Therefore, the control of BMs is necessary even in patients with
poor survival times.
Regarding the prognostic factors for OS, A number of
studies have been conducted in patients with BMs who received WBRT.
The following parameters have been demonstrated to be prognostic
factors: Karinofsky performance status (KPS); age; treatment
history; extracranial metastases; systemic tumor activity; lactic
dehydrogenase (LDH) level (20–27).
Gaspar et al (1) suggested the
recursive partitioning analysis (RPA) score as prognostic factors
for clinical use, which includes following 3 factors; KPS; age; and
the presence of extracranial metastases (1).
However, no predictive factors regarding the
response to WBRT in reducing the size of BMs have been identified
in previous studies. The aim of the present study was to identify
predictive factors for the local control of WBRT.
Materials and methods
Ethical approval
The Teikyo University School of Medicine (Tokyo,
Japan) ethics committee approved the present study. Written
informed consent was waived due to the retrospective nature of the
study. Patient information was anonymized prior to analysis.
Patient selection
A total of 94 patients with BMs from primary lung
cancer were treated with WBRT using a palliative radiation dose
(30–40 Gy) at Teikyo University School of Medicine between
September 2010 and April 2013. The study was limited to patients
who had undergone contrast-enhanced magnetic resonance imaging
(MRI) within 1 month prior to WBRT, and brain imaging
(contrast-enhanced computed tomography/MRI) using the same imaging
modality prior and subsequent to WBRT. A total of 32 patients who
had not undergone sufficient brain imaging were excluded. The
remaining 62 patients (mean age, 67 years; age range, 50–85 years)
were evaluated.
Patient diagnoses
Patient outcomes were determined using medical
records. The following parameters were evaluated: Performance
status (PS); LDH level; pathology [small cell lung cancer (SCLC)
vs. non-small cell lung cancer (NSCLC)]; extracranial metastases
(yes vs. no); activity of extracranial disease (stable vs.
progressive); chemo-history (yes vs. no); chest radiotherapy
history (yes vs. no); treatment term [the interval between tumor
diagnosis and WBRT (months)]; and use of γ-knife radiotherapy (yes
vs. no).
The largest metastatic tumor was evaluated,
excluding tumors with a history of previous γ-knife therapy. The
following parameters were evaluated using patient imaging data
prior and subsequent to WBRT: Tumor diameter; extent of edema, E/T
ratio and diffusion weighted image (DWI) signal intensity.
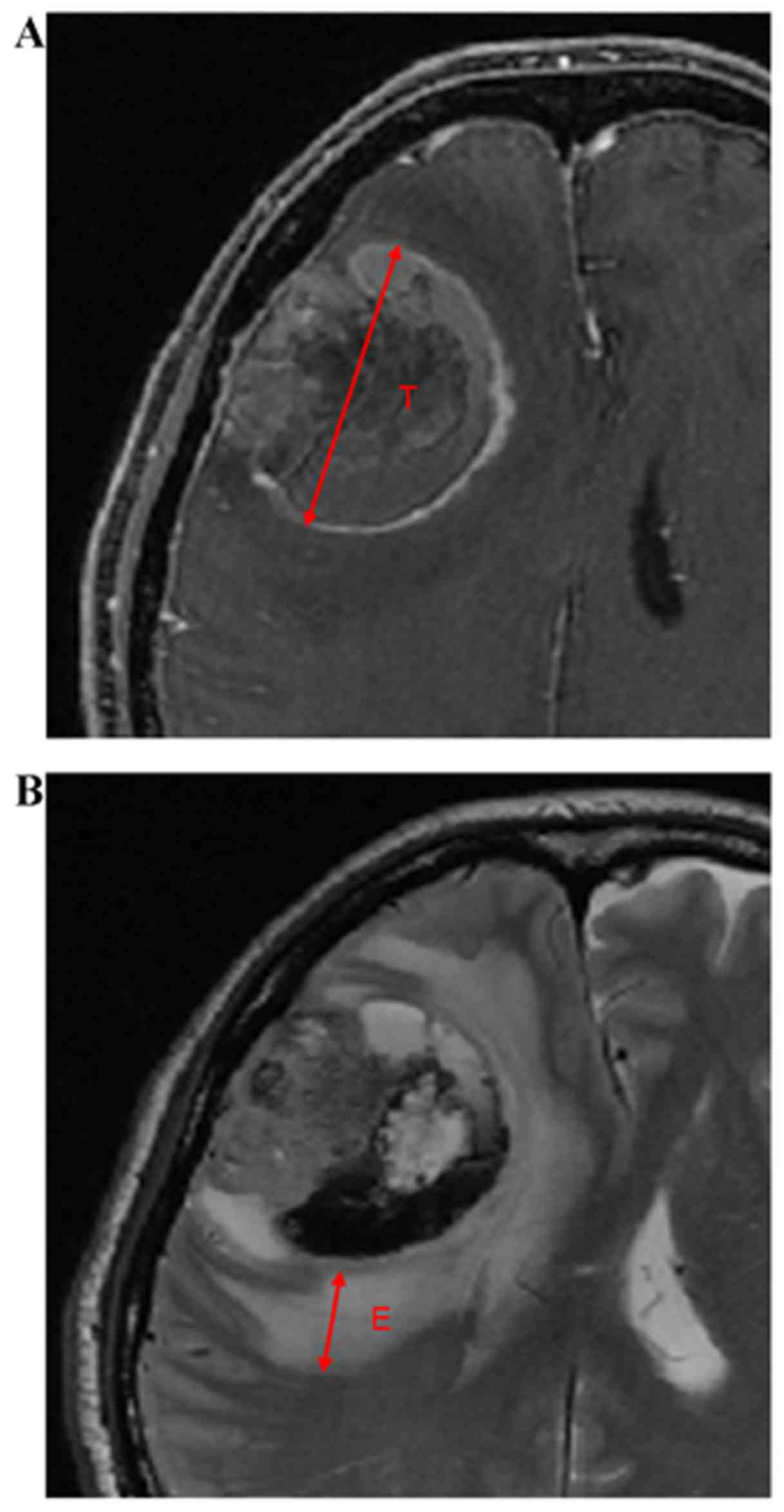
The tumor diameter was the maximum diameter (mm)
detected as an enhanced lesion on the axial contrast enhanced
T1-weighted images (WI). The extent of edema was expressed as the
maximum length between the margin of the edema and that of the
tumor on the axial T2-WI (Fig. 1).
The extent of edema (E) was divided by the tumor diameter (T) and
the association with RR was examined.
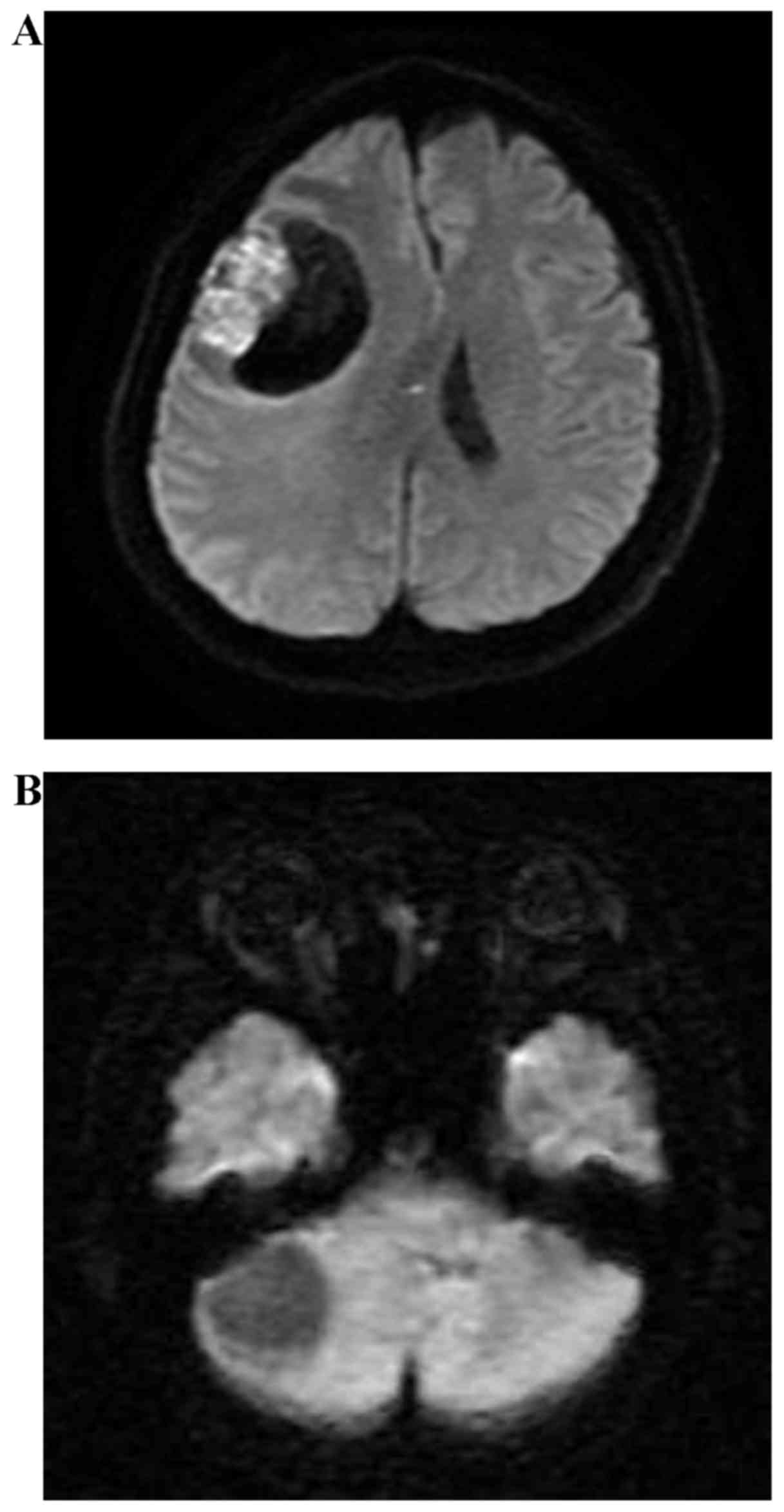
The DWI signal intensity was evaluated in the solid
portion of the tumor in five stages as follows: 5, higher compared
with the cortex; 4, iso to the cortex; 3, higher compared with the
white matter; 2, iso to the white matter; and 1, lower compared
with the white matter (Fig. 2). Image
analysis was conducted by two radiology specialists by consensus
(T.K. and S.A., with 11 and 5 years of experience, respectively),
who were blinded to the clinical data. In clinical practice, the
treatment effect is evaluated in accordance with Response
Evaluation Criteria in Solid Tumors version 4.0 (RECIST v4.0),
short-term efficacy was classified into 4 groups: complete response
(CR); partial response (PR); stable disease (SD); and progressive
disease (PD). In the current study, the patients were divided into
two groups, response group (CR+PR) and non-response group
(SD+PD).
Statistical analysis
Univariate and multivariate analyses were performed
to identify significant prognostic factors. Logistic regression
analysis with backward elimination was used to evaluate the
association between treatment effectiveness and the following
factors: Age; sex; PS; LDH; pathology; extracranial metastases;
extent of extracranial disease; chemo-history; chest radiotherapy
history; treatment term; use of γ-knife radiotherapy; DWI signal
intensity; tumor diameter; extent of edema; and the E/T ratio. All
statistical analyses were performed using software (PASW
Statistics, v.21.0: IBM SPSS, Armonk, NY, USA), P<0.05 was
considered to indicate a statistically significant difference.
Results
The patient characteristics are summarized in
Table I. A total of 35 (57%) patients
exhibited a PS ≥2, 20 (32%) exhibited SCLC, 35 (57%) exhibited
extracranial metastases, 37 (60%) suffered from progressive
extracranial disease, 37 (60%) demonstrated a chemo-history, 7
(11%) exhibited a history of chest radiotherapy, and 9 (15%)
demonstrated history of γ-knife radiotherapy. An E/T ratio ≥1.5 was
revealed in 11 (18%) patients.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Parameters | No. (range) | % |
|---|
| Age, years | 67 |
|
| Sex |
|
|
| Male | 46 | 74.2 |
|
Female | 16 | 25.8 |
| Performance
status |
|
|
| 0 | 4 | 6.5 |
| 1 | 23 | 37.1 |
| 2 | 12 | 19.4 |
| 3 | 17 | 27.4 |
| 4 | 6 | 9.7 |
| Histological
type |
|
|
|
NSCLC | 42 | 67.7 |
|
Adenocarcinoma | 34 | 54.8 |
|
Squamous cell carcinoma | 2 | 3.2 |
|
Others | 6 | 9.7 |
|
SCLC | 20 | 32.3 |
| Extracranial
metastases |
|
|
|
Yes | 35 | 56.5 |
| No | 27 | 43.5 |
| Activity of
extracranial tumor |
|
|
|
Stable | 25 | 40.3 |
|
Progressive | 37 | 59.7 |
| Treatment term from
diagnosisa | 67 (0–118) |
|
| Chemotherapy
regimen |
|
|
| 0 | 24 | 38.7 |
| 1 | 8 | 12.9 |
| 2 | 15 | 24.2 |
| 3 | 7 | 11.3 |
| 4 | 8 | 12.8 |
| Chest radiotherapy
history |
|
|
|
Yes | 7 | 11.3 |
| No | 55 | 88.7 |
| Tumor diameter,
mma | 17.6
(2–76) |
|
| Edema diameter,
mma | 13.4
(0–52) |
|
| Edema/tumor
ratio | 0.89 (0–3) |
|
| DWI Intensity |
|
|
|
1–4 | 26 | 41.9 |
| 5 | 36 | 58.1 |
| Response |
|
|
|
CR+PR | 34 | 54.8 |
|
SD+PD | 28 | 45.2 |
The overall response ratio (RR) of the cohort was
54.8%. In the univariate analyses, the response of tumors to WBRT
was associated with the presence of small cell lung carcinoma
(SCLC; P=0.0007), E/T ratio ≥1.5 (P=0.048), and median tumor
diameter of <20 mm (P=0.014). The result of univariate analysis
is described in Table II. In the
multivariate analysis, the following 3 factors, presence of SCLC
[P=0.001; odds ratio (OR), 17.152], an E/T ratio ≥1.5 (P=0.019; OR,
9.526); and presence of extracranial metastases (P=0.031; OR,
4.875) were revealed to be independent prognostic parameters for
treatment effects (Table III).
| Table II.Result of univariate analysis. |
Table II.
Result of univariate analysis.
| Parameters | Mean | Standard
deviation | P-value |
|---|
| Sex |
|
| 0.658 |
|
Male | 0.5 | 0.516 |
|
|
Female | 0.565 | 0.501 |
|
| Performance
status |
|
| 0.922 |
|
0–1 | 0.556 | 0.506 |
|
|
2–4 | 0.543 | 0.505 |
|
| Symptom |
|
| 0.217 |
|
Yes | 0.625 | 0.492 |
|
| No | 0.467 | 0.507 |
|
| Histological
type |
|
| 0.0007 |
|
Non-small cell lung
cancer | 0.405 | 0.5 |
|
| Small
cell lung cancer | 0.85 | 0.366 |
|
| Extracranial
metastases |
|
| 0.882 |
|
Yes | 0.541 | 0.505 |
|
| No | 0.56 | 0.507 |
|
| Activity of
extracranial tumor |
|
| 0.154 |
|
Stable | 0.444 | 0.506 |
|
|
Progressive | 0.629 | 0.49 |
|
| Treatment term from
diagnosis |
|
| 0.361 |
|
≤10 | 0.6 | 0.497 |
|
|
>10 | 0.481 | 0.509 |
|
| Chest radiotherapy
history |
|
| 0.899 |
|
Yes | 0.545 | 0.503 |
|
| No | 0.571 | 0.535 |
|
| γ-knife |
|
| 0.166 |
|
Yes | 0.585 | 0.497 |
|
| No | 0.333 | 0.5 |
|
| Chemotherapy
history |
|
| 0.841 |
|
With | 0.538 | 0.505 |
|
|
Without | 0.565 | 0.507 |
|
| Lactate
dehydrogenase |
|
| 0.402 |
|
<250 | 0.59 | 0.498 |
|
|
≥250 | 0.478 | 0.511 |
|
| Diffusion weighted
image intensity |
|
| 0.25 |
|
1–4 | 0.462 | 0.508 |
|
| 5 | 0.611 | 0.494 |
|
| Tumor diameter,
mm |
|
| 0.0144 |
|
≥20 | 0.659 | 0.48 |
|
|
<20 | 0.333 | 0.483 |
|
| Edema diameter,
mm |
|
| 0.361 |
|
≤10 | 0.6 | 0.497 |
|
|
>10 | 0.481 | 0.509 |
|
| Edema/tumor
ratio |
|
| 0.0484 |
|
≤1.5 | 0.49 | 0.504 |
|
|
>1.5 | 0.818 | 0.404 |
|
| Table III.Results of logistic regression
analysis. |
Table III.
Results of logistic regression
analysis.
|
| 95% confidence
interval |
|---|
|
|
|
|---|
| Parameter | Odds ratio | Lower | Upper | P-value |
|---|
| Pathology | 17.152 | 3.242 | 90.758 | 0.001 |
| Extracranial
metastases |
4.875 | 1.156 | 20.549 | 0.031 |
| Edema/tumor ratio
>1.5 |
9.526 | 1.453 | 62.459 | 0.019 |
Discussion
Data from 62 lung cancer patients with BMs who
underwent WBRT were retrospectively reviewed; the overall RR was
54.8%, which was similar to previous studies (4,28). In WBRT
for BMs from lung cancer, BMs with the following characteristics
are expected to have a higher RR: From SCLC compared with NSCLC
(OR, 17.152); an E/T ratio of ≥1.5 rather opposed to <1.5 (OR,
9.526); and an absence rather than a presence of extracranial
metastases (OR, 4.875).
Patients with SCLC exhibited an improved RR compared
with patients with NSCLC. It is widely known that SCLC exhibits
high radiosensitivity (29–31). In addition, it has been suggested that
BMs also demonstrate high radiosensitivity, similar to that
observed in the primary tumor (32).
The data of the present study agree with those from previous
studies.
In the current study, BMs with an E/T ratio of ≥1.5
are expected to exhibit a higher RR rather than BMs with an E/T
ratio of <1.5. Peritumoral edema is caused by disturbed vascular
permeability that enables an indiscriminate escape of plasma
proteins from the blood into BMs or the peritumoral regions of the
brain (33). The present study was
not able to explain the immediate reason why BMs with relatively
extensive edema (E/T ratio ≥1.5) exhibited an improved response to
WBRT. However, E/T ratios may provide useful information for
predicting therapeutic efficacy.
DWI produces a signal intensity that reflects the
cell density of a tumor and correlates with its histopathological
image; therefore, it is believed to be useful in predicting the
treatment effectiveness for esophageal, pharyngeal and cervical
cancer (34–37). DWI is also considered to be useful in
predicting the efficacy of g-knife therapy for BMs (38). However, no statistically significant
difference in RR has been observed for BMs derived from lung cancer
with different DWI signal intensities; these BMs are occasionally
accompanied by hemorrhage, necrosis and mucous production that
present with various signal intensities (39). Therefore, it has been concluded that
DWI would not predict the therapeutic effect for BMs from lung
cancer.
The presence of extracranial metastases also
correlated with an improved RR. Notably, it is a rather reverse
result to the studies concerning OS (17,24). The
RR results are explained as follows, low differentiated tumors
often cause distant metastasis and exhibit high radiosensitivity,
and this factor may have affected the results of the present
study.
There are numerous studies that have identified
prognostic factors focused on OS in patients with BM who underwent
WBRT. For example, the RPA score proposed by Gaspar et al
(1), which is widely used in clinical
settings, includes KPS, age and the presence of an active
extracranial lesion. Other factors including sex, symptom and
response to steroid treatment have been indicated as predictive
factors (Table IV). These factors
are not equal with the result of the present study focused on local
control.
| Table IV.Previous studies examining predictive
factors for the patients with BMs who underwent WBRT. |
Table IV.
Previous studies examining predictive
factors for the patients with BMs who underwent WBRT.
| Author (publication
year) | Predicting factors
for vital prognosis | (Refs.) |
|---|
| Gaspar et
al, 1997 | KPS, age,
extracranial metastases | (1) |
| Lagerwaard et
al, 1999 | PS, response to
steroid treatment, systemic tumor activity, LDH site of primary
tumor, age, number of BM, sex | (2) |
| Partl et al,
2016 | KPS/LDH index | (20) |
| Windsor et
al, 2013 | Age, sex, primary
cancer, time to WBRT from the primary cancer diagnosis | (21) |
| Rades et al,
2013 | Sex, KPS,
extracranial metastases | (22) |
| Zimm et al,
1981 | PS, age, symptom of
headache/visual disturbance/impaired consciousness | (23) |
| Sperduto et
al, 2008 | KPS, age,
extracranial metastases, number of BMs | (24) |
| Komatsu et
al, 2013 | Histological type,
EGFR mutation (use of EGFR-TKI) | (25) |
| Mayahara et
al, 2012 | KPS, sex, activity
of extracranial disease, time to develop BM, use of chemotherapy
following WBRT | (26) |
| Zhu et al,
2014 | Plasma
fibrinogen | (27) |
The majority of patients who receive WBRT
demonstrate poor health; 51% of these patients exhibit an RPA class
3 score, which is equivalent to a KPS <70 (19). Thus, a number of the factors that are
useful for prognosis of WBRT regarding OS reflect the general
condition of the patients and their general disease status, rather
than reflecting the response to WBRT. This may be one reason why
the factors useful for predicting vital prognosis do not
necessarily coincide with the response to WBRT. Therefore, it is
considered that the vital prognosis of patients and the response of
tumors to WBRT should have separate predictive factors, and it
would be useful to employ these in combination, to make decisions
concerning the treatment of the patients.
In cases with poor response to WBRT expected, the
course of treatment for each patient should potentially be
reconsidered, according to their vital prognosis. That is, for
patients with predicted poor responses to WBRT and poor vital
prognosis, palliative care without WBRT should be considered to
improve QOL (40). For patients with
expected poor response to WBRT but good vital prognosis, additional
radical treatment for BMs should be considered, such as SRS or SRT
(3,4,10).
Recently, the novel hypothesis of oligometastases
has been proposed, define as patients with a limited number of
metastases (oligometastases), may benefit of survival from curative
local therapy for metastases (11–13). In
addition, Niibe et al (12,14)
defined oligo-recurrence and this is similar to oligometastases,
but the primary lesion is also controlled (12,14).
A number of studies are have investigated the use of
curative radiotherapy for oligometastases or oligo-reccurence and
particularly in oligo-recurrence, it was demonstrated to be a
favorable factor for OS and relapse-free survival, and it was also
associated with improved local control of the metastases (12,15,16). This
is also true for SRS/SRT for BMs (17,18).
In the present study about WBRT, almost all patients
exhibited uncontrolled primary lesions, multi-organ metastases or
numerous BMs. Thus, it was not possible to neither examine enough
oligo-recurrence cases nor indicate the immediate association
between the response of BMs and the state of oligo-recurrence.
However, further clinical studies examining the association between
the local control of patients with BMs undergoing WBRT and the
state of oligo-recurrence, may lead to the identification of an
important predictive factor for appropriate treatment
decisions.
The present study had several limitations. The
number of patients studied was 64, which is a small sample size. In
addition, the study was retrospective. The majority of the data
used were extracted from previous medical records, which made it
difficult to evaluate the association between the improvement of
the symptom of BMs and the response of tumor to WBRT. It was not
possible to examine the EGFR mutation status of the patients, or
other genomic information. Regarding the evaluation of the DWI
signal intensity, an evaluation using an apparent diffusion
coefficient (ADC) map was not performed. The use of an ADC map is
considered preferable for more effective evaluation of the nature
of tumors. However, DWI signal intensity, which is clinically
convenient, was used in the present study. It will be necessary to
validate these data by studying more patients, or by performing a
prospective study, prior to their application in an actual clinical
setting.
In conclusion, predictive factors for the response
of BMs to WBRT for patients with lung cancer were investigated. The
following three factors were significantly associated to the
response to WBRT: The presence of SCLC, an E/T ratio ≥1.5 and the
presence of extracranial metastases. The identification of
predictive factors concerning the response to WBRT may provide
useful information to facilitate the selection of adequate
individual treatments for patients with lung cancer with BM prior
to WBRT.
References
|
1
|
Gaspar L, Scott C, Rotman M, Asbell S,
Phillips T, Wasserman T, McKenna WG and Byhardt R: Recursive
partitioning analysis (RPA) of prognostic factors in three
Radiation therapy oncology group (RTOG) brain metastases trials.
Int J Radiat Oncol Biol Phys. 37:745–751. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lagerwaard FJ, Levendag PC, Nowak PJ,
Eijkenboom WM, Hanssens PE and Schmitz PI: Identification of
prognostic factors in patients with brain metastases: A review of
1292 patients. Int J Radiat Oncol Biol Phys. 43:795–803. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gaspar LE, Mehta MP, Patchell RA, Burri
SH, Robinson PD, Morris RE, Ammirati M, Andrews DW, Asher AL, Cobbs
CS, et al: The role of whole brain radiation therapy in the
management of newly diagnosed brain metastases: A systematic review
and evidence-based clinical practice guideline. J Neurooncol.
96:17–32. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Postmus PE, Haaxma-Reiche H, Gregor A,
Groen HJ, Lewinski T and Scolard T: Brain-only metastases of small
cell lung cancer; efficacy of whole brain radiotherapy. An EORTC
phase II study. Radiother Oncol. 46:29–32. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gao Y, Gao F, Ma JL and Zhao DL:
Palliative whole-brain radiotherapy and health-related quality of
life for patients with brain metastasis in cancer. Neuropsychiatr
Dis Treat. 11:2185–2190. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chao JH, Phillips R and Nickson JJ:
Roentgen-ray therapy of cerebral metastases. Cancer. 7:682–689.
1954. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Order SE, Hellman S, Von Essen CF and
Kligerman MM: Improvement in quality of survival following
whole-brain irradiation for brain metastases. Radiology.
91:149–153. 1968. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tsao MN, Lloyd NS, Wong RK, Rakovitch E,
Chow E and Laperriere N: Supportive Care Guidelines Group of Cancer
Care Ontario's Program in Evidence-based Care: Radiotherapeutic
management of brain metastases: A systematic review and
meta-analysis. Cancer Treat Rev. 31:256–273. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zimmermann S, Dziadziuszko R and Peters S:
Indications and limitations of chemotherapy and targeted agents in
non-small cell lung cancer brain metastases. Cancer Treat Rev.
40:716–722. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Niibe Y, Karasawa K, Nakamura O, Shinoura
N, Okamoto K, Yamada R, Fukino K and Tanaka Y: Survival benefit of
stereotactic radiosurgery for metastatic brain tumors in patients
with controlled primary lesions and no other distant metastases.
Anticancer Res. 23:4157–4159. 2003.PubMed/NCBI
|
|
11
|
Hellman S and Weichselbaum RR:
Oligometastases. J Clin Oncol. 13:8–10. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Niibe Y and Hayakawa K: Oligometastases
and oligo-recurrence: The new era of cancer therapy. Jpn J Clin
Oncol. 40:107–111. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Niibe Y and Chang JY: Novel insights of
oligometastases and oligo-recurrence and review of the literature.
Pulm Med. 2012:2610962012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Niibe Y, Chang JY, Onishi H, Salama J,
Hiraki T and Yamashita H: Oligometastases/Oligo-recurrence of lung
cancer. Pulm Med. 2013:4382362013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yamashita H, Niibe Y, Yamamoto T, Katsui
K, Jingu K, Kanazawa S, Terahara A and Nakagawa K: Lung
stereotactic radiotherapy for oligometastases: Comparison of
oligo-recurrence and sync oligometastases. Jpn J Clin Oncol.
46:687–791. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Won YK, Lee JY, Kang YN, Jang JS, Kang JH,
Jung SL, Sung SY, Jo IY, Park HH, Lee DS, et al: Stereotactic
radiosurgery for brain metastasis in non-small cell lung cancer.
Radiat Oncol J. 33:207–216. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang TJ, Saad S, Qureshi YH, Jani A,
Isaacson SR, Sisti MB, Bruce JN, McKhann GM II, Lesser J, Cheng SK,
et al: Outcomes of gamma knife radiosurgery, bi-modality &
tri-modality treatment regimens for patients with one or multiple
brain metastases: The Columbia University Medical Center
experience. J Neurooncol. 122:399–408. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Niibe Y, Nishimura T, Inoue T, Karasawa
KY, Jingu K and Shirato H: Oligo-recurrence predicts favorable
prognosis of brain-only oligometastases in patients with non-small
cell lung cancer treated with stereotactic radiosurgery or
stereotactic radiotherapy: A multi-institutional study of 61
subjects. BMC Cancer. 16:6592016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mulvenna PM: The management of brain
metastases in patients with non-small cell lung cancer-is it time
to go back to the drawing board? Clin Oncol (R Coll Radiol).
22:365–373. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Partl R, Fastner G, Kaiser J, Kronhuber E,
Cetin-Strohmer K, Steffal C, Böhmer-Breitfelder B, Mayer J, Avian A
and Berghold A: KPS/LDH index: A simple tool for identifying
patients with metastatic melanoma who are unlikely to benefit from
palliative whole brain radiotherapy. Support Care Cancer.
24:523–528. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Windsor AA, Koh ES, Allen S, Gabriel GS,
Yeo AE, Allison R, van der Linden YM and Barton MB: Poor outcomes
after whole brain radiotherapy in patients with brain metastases:
Results from an international multicentre cohort study. Clin Oncol
(R Coll Radiol). 25:674–680. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rades D, Dziggel L, Nagy V, Segedin B,
Lohynska R, Veninga T, Khoa MT, Trang NT and Schild SE: A new
survival score for patients with brain metastases who received
whole-brain radiotherapy (WBRT) alone. Radiother Oncol.
108:123–127. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zimm S, Wampler GL, Stablein D, Hazra T
and Young HF: Intracerebral metastases in solid-tumor patients:
Natural history and results of treatment. Cancer. 48:384–394. 1981.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sperduto PW, Berkey B, Gaspar LE, Mehta M
and Curran W: A new prognostic index and comparison to three other
indices for patients with brain metastases: An analysis of 1,960
patients in the RTOG database. Int J Radiat Oncol Biol Phys.
70:510–514. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Komatsu T, Kunieda E, Oizumi Y, Tamai Y
and Akiba T: Clinical characteristics of brain metastases from lung
cancer according to histological type: Pretreatment evaluation and
survival following whole-brain radiotherapy. Mol Clin Oncol.
1:692–698. 2013.PubMed/NCBI
|
|
26
|
Mayahara H, Sumi M, Ito Y, Sekii S,
Takahashi K, Inaba K, Kuroda Y, Murakami N, Morota M and Itami J:
Effect of chemotherapy on survival after whole brain radiation
therapy for brain metastases: A single-center retrospective
analysis. J Cancer Res Clin Oncol. 138:1239–1247. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhu JF, Cai L, Zhang XW, Wen YS, Su XD,
Rong TH and Zhang LJ: High plasma fibrinogen concentration and
platelet count unfavorably impact survival in non-small cell lung
cancer patients with brain metastases. Chin J Cancer. 33:96–104.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Barnes EA, Chow E, Tsao MN, Bradley NM,
Doyle M, Li K, Lam K and Danjoux C: Physician expectations of
treatment outcomes for patients with brain metastases referred for
whole brain radiotherapy. Int J Radiat Oncol Biol Phys. 76:187–192.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kuremsky JG, Urbanic JJ, Petty WJ, Lovato
JF, Bourland JD, Tatter SB, Ellis TL, McMullen KP, Shaw EG and Chan
MD: Tumor histology predicts patterns of failure and survival in
patients with brain metastases from lung cancer treated with gamma
knife radiosurgery. Neurosurgery. 73:641–647. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Seute T, Leffers P, Wilmink JT, ten Velde
GP and Twijnstra A: Response of asymptomatic brain metastases from
small-cell lung cancer to systemic first-line chemotherapy. J Clin
Oncol. 24:2079–2083. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bohlen G, Meyners T, Kieckebusch S,
Lohynska R, Veninga T, Stalpers LJ, Schild SE and Rades D:
Short-course whole-brain radiotherapy (WBRT) for brain metastases
due to small-cell lung cancer (SCLC). Clin Neurol Neurosurg.
112:183–187. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Schuette W: Treatment of brain metastases
from lung cancer: Chemotherapy. Lung Cancer. 45 Suppl 2:S253–S257.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang M and Olsson Y: Hematogenous
metastases of the human brain-characteristics of peritumoral brain
changes: A review. J Neurooncol. 35:81–89. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wang L, Han C, Zhu S, Shi G, Wang Q, Tian
H, Kong J and Zhang A: Investigation of using diffusion-weighted
magnetic resonance imaging to evaluate the therapeutic effect of
esophageal carcinoma treatment. Oncol Res Treat. 37:112–116. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chen Y, Liu X, Zheng D, Xu L, Hong L, Xu Y
and Pan J: Diffusion-weighted magnetic resonance imaging for early
response assessment of chemoradiotherapy in patients with
nasopharyngeal carcinoma. Magn Reson Imaging. 32:630–637. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hong J, Yao Y, Zhang Y, Tang T, Zhang H,
Bao D, Chen Y and Pan J: Value of magnetic resonance
diffusion-weighted imaging for the prediction of radiosensitivity
in nasopharyngeal carcinoma. Otolaryngol Head Neck Surg.
149:707–713. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mardor Y, Roth Y, Ochershvilli A,
Spiegelmann R, Tichler T, Daniels D, Maier SE, Nissim O, Ram Z,
Baram J, et al: Pretreatment prediction of brain tumors' response
to radiation therapy using high b-value diffusion-weighted MRI.
Neoplasia. 6:136–142. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lee CC, Wintermark M, Xu Z, Yen CP,
Schlesinger D and Sheehan JP: Application of diffusion-weighted
magnetic resonance imaging to predict the intracranial metastatic
tumor response to gamma knife radiosurgery. J Neurooncol.
118:351–361. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Osborn AG: Osborn's Brain: Imaging,
Pathology and Anatomy. Lippincott Williams & Wilkins;
Philadelphia, PA: 2012
|
|
40
|
Tsao MN, Rades D, Wirth A, Lo SS,
Danielson BL, Gaspar LE, Sperduto PW, Vogelbaum MA, Radawski JD,
Wang JZ, et al: Radiotherapeutic and surgical management for newly
diagnosed brain metastasis(es): An American Society for Radiation
Oncology evidence-based guideline. Pract Radiat Oncol. 2:210–225.
2012. View Article : Google Scholar : PubMed/NCBI
|