Introduction
Differentiated thyroid carcinoma (DTC) constitutes
~95% of thyroid carcinomas and generally is associated with a
favorable long-term survival; however, the prognosis is worse for
patients developing distant metastases (DMs) (1,2).
Radioactive iodine (RAI) therapy is the main treatment modality for
DMs with 131I uptake, but 2/3 of patients with
metastatic DTC become RAI refractory (3). In the majority of cases, progression is
likely to occur in metastases without radioactive iodine uptake (in
particular when 18F-FDG uptake is present) and RAI
treatment will not be beneficial (3).
Additional therapy involves external radiation, surgery or other
local ablative procedures (4).
Systemic therapies with the tyrosine kinase inhibitors (TKIs)
sorafenib and lenvatinib have been recently approved (2–5). Sorafenib
(Nexavar®), was the first drug employed in RAI-refractory DTC, and
its inhibitory effect has been explored in an international,
multicentric, phase 3 study (DECISION trial) (5). The present study demonstrates that the
progression-free survival (PFS) of naïve patients receiving this
drug was longer compared with the placebo group (10.8 vs. 5.8
months; P<0.0001). The positive results in terms of the safety
and efficacy of sorafenib allowed for the approval of this drug by
the FDA in 2013, and by the EMA in 2014. In addition, another TKI
drug (lenvatinib, Lenvima®), was investigated for the treatment of
RAI-refractory DTC, and the results were published in a phase 3,
multicenter randomized, placebo controlled study (SELECT trial)
(6). In the SELECT trial, PFS was
longer in naïve and second line patients treated with
lenvatinibthan compared with the placebo group. Although TKIs are
promising in the treatment of RAI-refractory DTC, the main
limitation of them is the fact that following a variable period of
time from the beginning of treatment, an indefinite number of
cancer cells begin to grow again, possibly due to the development
of an escape mechanism (7).
Case report
A 65-year-old male underwent total thyroidectomy
(TT) for pre-toxic multinodular goiter in February 2005.
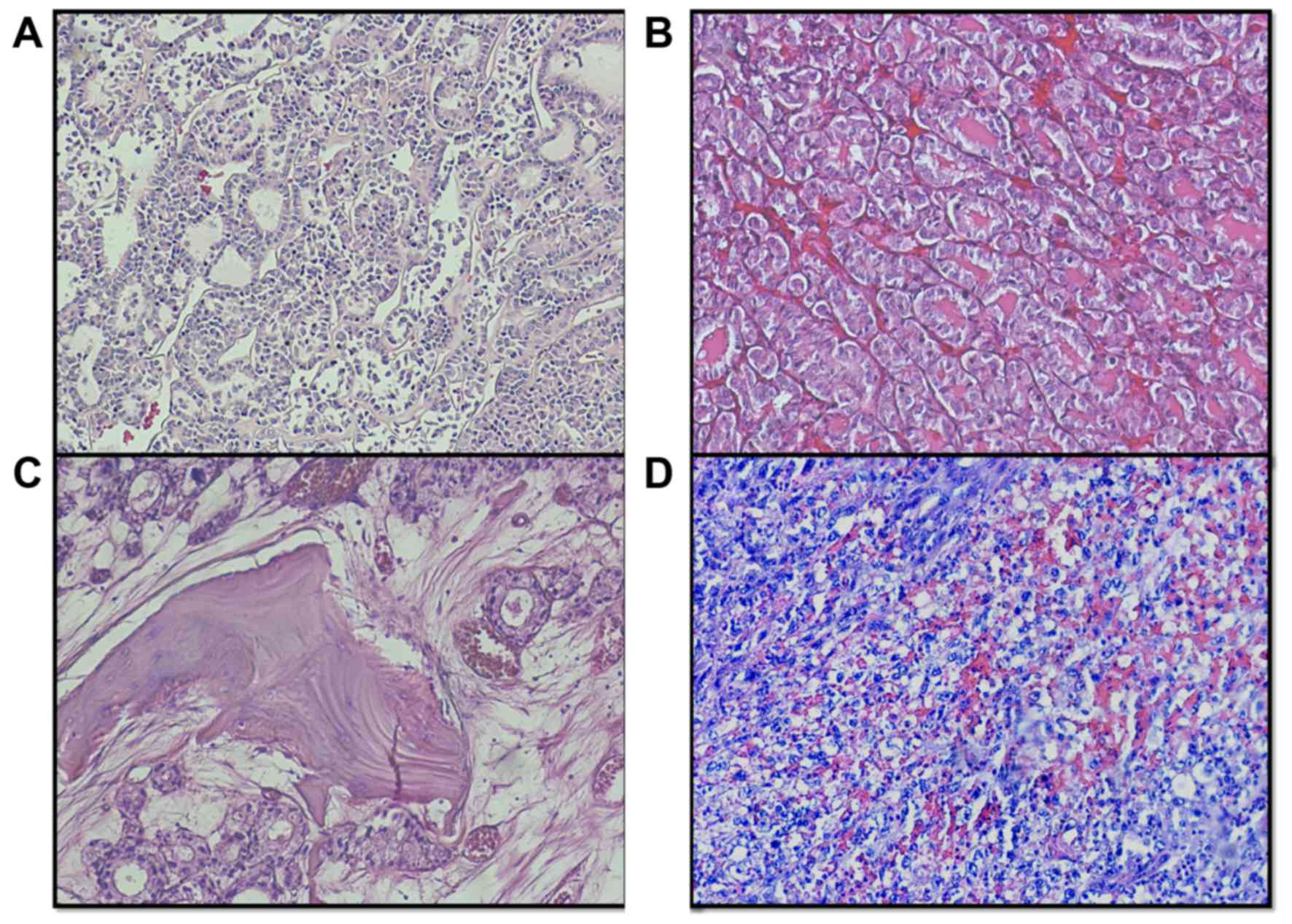
Histological examination revealed a 4-cm follicular thyroid
carcinoma (FTC), Hürthle cell variant, with capsular invasion and
vascular emboli (Fig. 1A). During the
subsequent 5 years, the patient received four 131I
administrations (cumulative dose, 612 mCi) for increasing serum
thyroglobulin (Tg) levels (from 9 to 144 ng/ml) on fully
suppressive L-thyroxine therapy and faint lung uptake at
131I whole body scan (WBS), in the absence of any
radiological [computed tomography (CT)] evidence of lung
metastases. Bone scintigraphy was negative 3 years after TT. No
relevant RAI uptake was detected at WBS performed following the
last RAI dose (200 mCi), which was administered 5 years after TT,
despite the further increase in serum Tg levels (≥800 ng/ml)
obtained with fully suppressed TSH. At that time, a new bone
scintigraphy detected an osteolytic lesion in the left humerus
neck, which was treated by embolization, electrochemotherapy and
partial resection. Histology confirmed an FTC (metastatic lesion)
which was strongly positive for Tg at immunohistochemistry
(Tg++). Nine months later, a chest CT revealed a new
osteolytic lesion at the fifth left rib, which was surgically
removed in October 2011. Histology confirmed a Tg++ FTC
(metastatic lesion). In 2012, an infusion cyclic-therapy with
zolendronic acid (Zometa®, 4 mg at monthly intervals) was performed
for 12 months. In April 2013, positron emission tomography (PET)/CT
displayed a skull bone lesion, which was confirmed by total body CT
(TBCT). TBCT also demonstrated a synchronous PET-negative adrenal
left metastasis. Both lesions were surgically resected and were
histologically confirmed to be FTC metastases expressing Tg and
thyroid transcription factor 1 (TTF1). (Fig. 1B and C). A further TBCT performed 6
months later documented progression of bone metastatic lesions and
new appearance of lung metastases. According to the Response
Evaluation Criteria In Solid Tumors (8), in March 2014, the patient started a
first-line treatment with sorafenib (2,4) with a
full daily oral dose of 800 mg. At that time, the patient was
asymptomatic and in good general condition, but one month later,
the patient developed a severe hand-foot skin reaction, requiring
reduction of sorafenib to 400 mg/day. Six months after the
initiation of the therapy, a new TBCT demonstrated stable disease,
although the progressive increase in serum Tg levels suggested
biochemical progression.
Four months later, sorafenib was stopped to allow
urgent prostatectomy for acute urinary retention due to prostatic
hyperplasia. Three days after the surgery, the patient suddenly
reported an intense pain in the sacral region, and a TBCT performed
two weeks later identified a markedly large (9 cm) necrotic right
gluteus muscle lesion, alongside the appearance of additional lung
metastatic lesions. A review of the TBCT scan performed four months
earlier confirmed the absence at the time of any detectable mass in
the gluteus. Since the precise nature of the gluteal lesion was
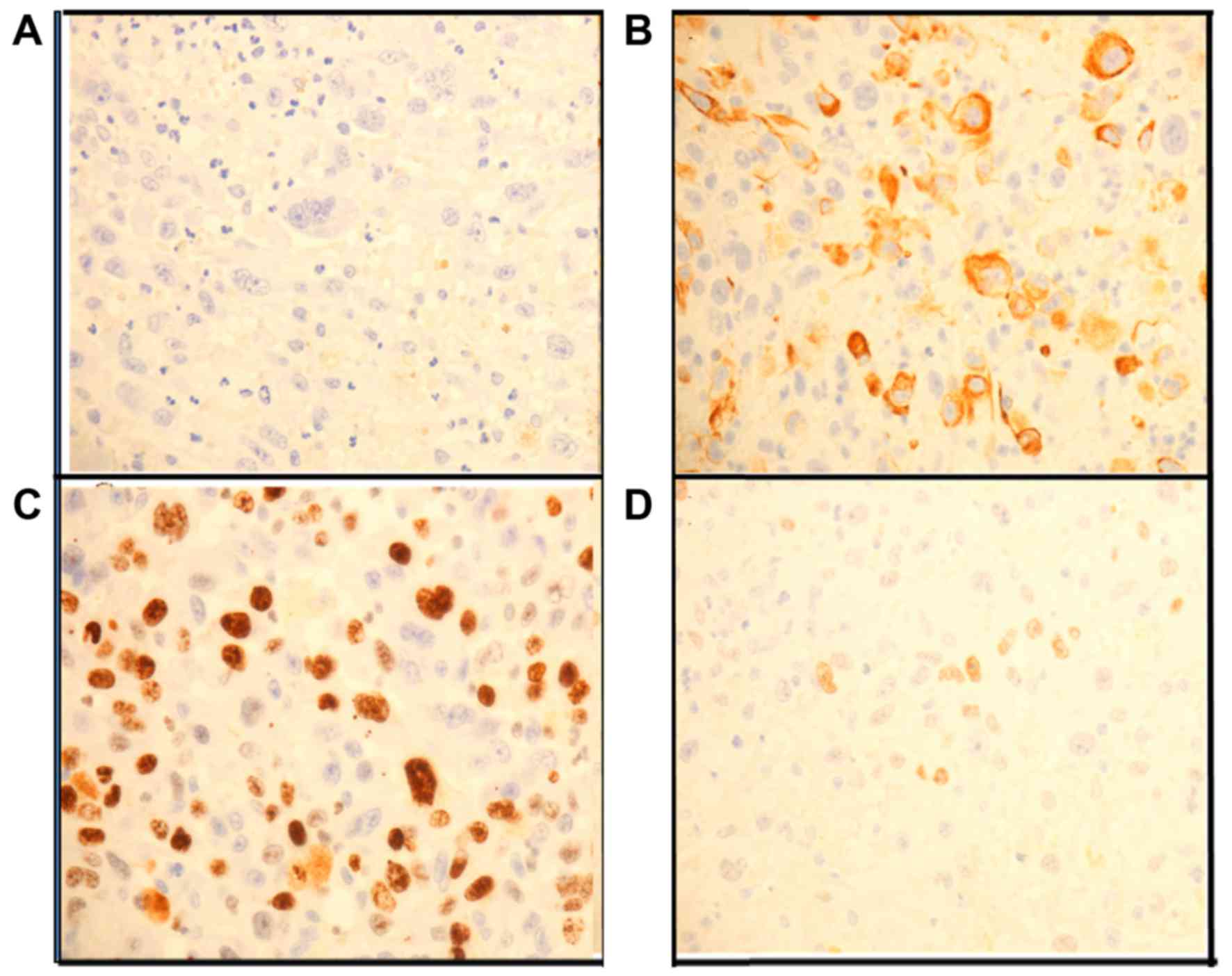
unclear, a diagnostic biopsy was performed. Histology (Fig. 1D) revealed an extensively necrotic
undifferentiated neoplasia, with rhabdoid aspects, Tg negativity at
immunohistochemistry, and positivity for cytokeratin 7, Ki-67 (40%)
and TTF1 (Fig. 2A-D). All
immunohistochemistry assays have been performed using the same
platform (Ventana Medical Systems, Inc., Tucson, AZ, -USA); all
antibodies were ready-to-use: Thyroglobulin, mouse monoclonal
antibody-clone 2H11+6E1 (cat. no., 760-2671); TTF1, mouse
monoclonal antibody, clone 8G7G3/1 (cat. no., 790-4462); Ki-67,
rabbit monoclonal antibody, clone 30-9 (cat. no., 760-2542)
(Ventana Medical Systems, Inc.). Two weeks after the biopsy, the
clinical conditions rapidly worsened. Thus, the patient was
admitted to a local hospital for severe anemia and succumbed few
hours later.
The patient had signed an informed consent form
stating that all the clinical examinations required for an accurate
diagnosis could be performed. The ethics committee or head of the
University Hospital of Cagliari (Cagliari, Italy) reviewed and
approved the study protocol. No autopsy was performed. The
histological and immunohistochemical features of the primary tumor
and all the available metastatic tissues, together with the serum
Tg concentrations prior and subsequent to the removal of each
metastatic lesion are reported in Table
I.
 | Table I.Comparison of histological and
immunoistochemical features of the primary neoplasia and metastatic
lesions. |
Table I.
Comparison of histological and
immunoistochemical features of the primary neoplasia and metastatic
lesions.
|
|
|
|
Immunohystochemistry | Serum Tg (ng/ml) |
|---|
| Lesion site | Surgical removal
date | Histology | TTF1 | CK7 | Ki67 (%) | Prior to surgery | Following
surgery |
|---|
| Thyroid gland | Feb 2005 | Differentiated | ++ | ++ | ND | ND | ND |
9 |
| Humerus | Aug 2010 | Differentiated | ++ | ND | ND | ND | 800 | 144 |
| Rib | Oct 2011 | Differentiated | ++ | ND | ND | ND | 672 |
31 |
| Skull | May 2013 | Differentiated | ++ | ND | ND | ND | 168 | 159 |
| Adrenal gland | July 2013 | Differentiated | ++ | ++ | ND | ND | 168 | 159 |
| Gluteus | Feb 2015 | Undifferentiated | + | ++ | ++ | ++ | 1,484 | 1,784 |
Several oncogenes involved in thyroid tumorigenesis
were evaluated in all the available tissues (Table II). All tumor samples were formalin
fixed and paraffin embedded. For each case, the most representative
paraffin block was selected, and three 10-µm unstained sections
were prepared for DNA purification. The DNA from the primary tumor
and that from the adrenal and gluteal metastatic lesions were
adequate for molecular analysis. However, bone-derived DNA is known
to contain high levels of polymerase chain reaction (PCR)
inhibitors (9). In consequence, the
cranial metastatic lesion DNA resulted unsuitable for downstream
analyses. An extensive molecular analysis was performed using a
mass spectrometry platform (MassARRAY System, Agena Bioscience, San
Diego, CA, USA) and the Myriapod Colon Status kit (Diatech
Pharmacogenetics SRL, Jesi, Italy), which allowed the
identification of 216 cancer-associated hotspot mutations in the
KRAS, BRAF, NRAS and phosphatidylinositol-4,5-bisphosphate
3-kinase, catalytic subunit alpha oncogenes. All lesions had the
same point mutation in NRAS codon 61 (p.Q61R, c.182C>G), while a
wildtype result was obtained for the other oncogenes. These data
are in agreement with a previous study reporting that NRAS-mutant
thyroid carcinoma exhibit a high risk with respect to develop bone
metastases (10). Further molecular
analyses were carried out by PCR, followed by direct Sanger
sequencing (AbiPrism 3130 Genetic Anayzer, Applied Biosystem,
Foster City, CA, USA) in order to assess the presence of mutations
in the exons 4–9 of the p53 gene and in the promoter region of the
telomerase (TERT) gene, which are known to be associated with
clinicopathological features of aggressiveness in DTC (11). Sequencing of p53 was carried out
following the protocol provided by the IARC TP53 Mutation Database
(available on the website: p53.iarc.fr), and analysis of TERT
promoter was performed as described previously (12). The analysis revealed the presence of
the C228T TERT promoter mutation in the primary thyroid tumor and
in all other metastatic lesions samples. A p53 non-synonymous
polymorphism was also identified in the undifferentiated gluteal
metastatic lesion [p.P72R, c.215C>G (rs 1042522)], while no p53
amplification reaction was observed with the other samples (primary
tumor and differentiated MLs), probably due to high DNA
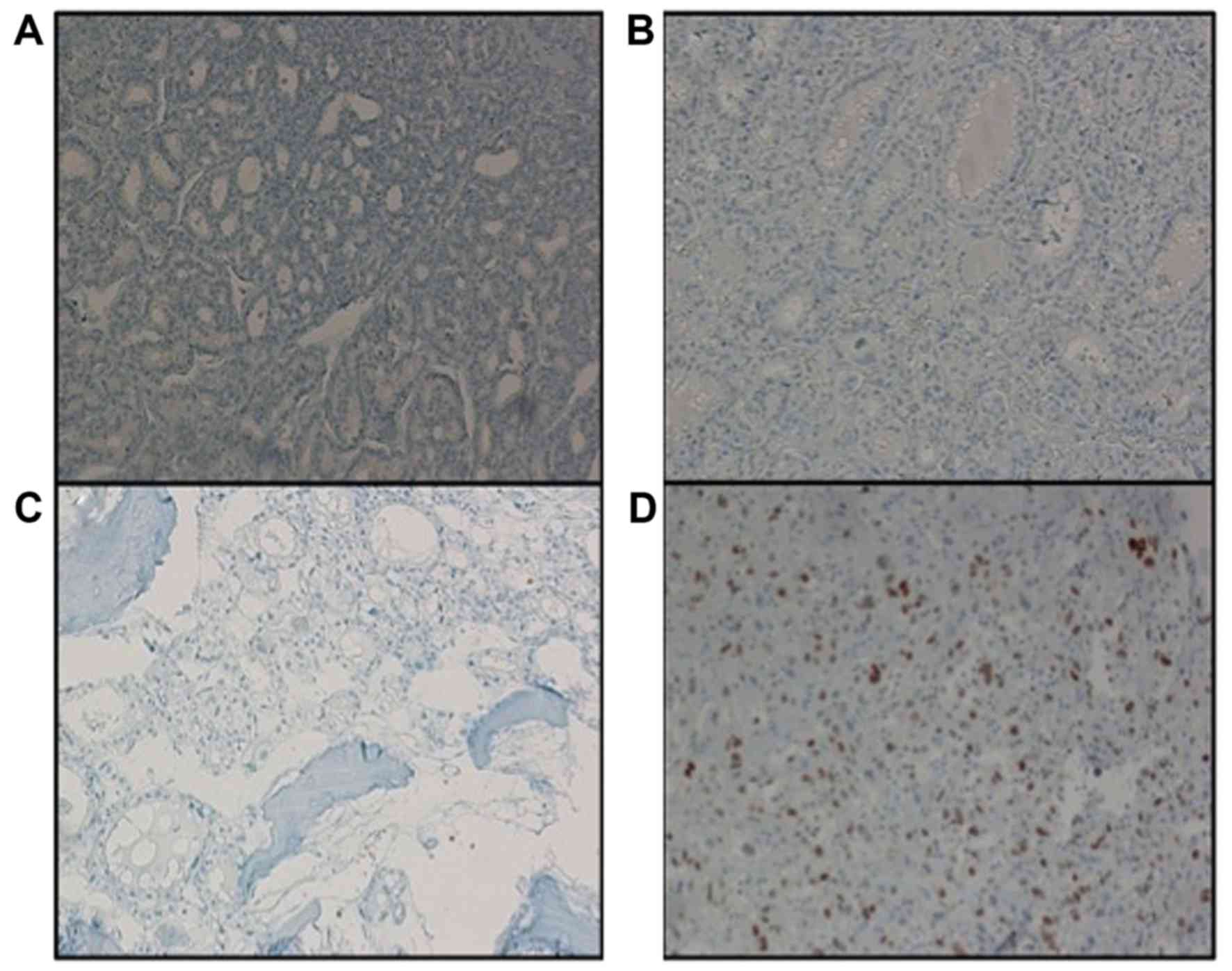
fragmentation and excessive amplicon length (13). Thus, p53 protein expression was
assessed by immunohistochemistry [mouse monoclonal antibody, clone
Bp53-11 (cat. no., 760-2542)] and only the gluteal undifferentiated
metastatic lesion resulted positive for p53 (Fig. 3A-D).
| Table II.Mutational status of oncogenes in
primary tumor and metastatic lesions. |
Table II.
Mutational status of oncogenes in
primary tumor and metastatic lesions.
|
| Oncogenes |
|---|
|
|
|
|---|
|
| p53 |
|---|
|
|
|
|---|
| Tumor tissue | BRAF | NRAS | KRAS | PIK3CA | TERT | PCR | IHC |
|---|
| Thyroid
(primary) | WT | p.Q61R | WT | WT | C228T | Unassessable | − |
| Adrenal gland
(metastasis) | WT | p.Q61R | WT | WT | C228T | Unassessable | − |
| Skull
(metastasis) | Ins | Ins | Ins | Ins | C228T | Unassessable | − |
| Gluteus
(metastasis) | WT | p.Q61R | WT | WT | C228T | p.P72R,
c.215C>G | ++ |
Discussion
Sudden rapid progression of tumors subsequent to
sorafenib discontinuation (known as ‘flare-up’) is considered to be
a rather common event, but it has been reported only in a limited
number of patients with solid tumors, including a single case of
papillary thyroid carcinoma (14–16). The
mechanisms involved in this phenomenon are unknown, although the
emergence of aggressive clones responsive to TKI and a vascular
rebound following the withdrawal of angiogenesis inhibition are the
most probable explanations (14).
The present case report provides a detailed
description of a flare-up phenomenon observed in a patient with
metastatic FTC few days following the interruption of sorafenib
administration. The availability of formalin-embedded specimens
from the primary tumor and several metastases allowed the
morphological, biochemical and molecular comparative analyses of
all tissues. The primary tumor displayed double oncogenic mutations
(RAS and TERT promoter), which are known to be associated with
aggressive behavior (11,12). Accordingly, the patient developed in
the last 5 years of life a large number of metastases (bone,
adrenal and lung metastases), which remained well differentiated
with a rather slow disease progression. The same two mutations were
detected in all the MLs available for analysis, including the
undifferentiated gluteal metastases, thus confirming the common
origin of both differentiated and undifferentiated MLs. A p53
non-synonymous polymorphism was clearly detectable by Sanger
sequencing in the undifferentiated lesion, but no conclusive data
were obtained in the primary tumor or in the other metastatic
lesions, probably due to high DNA fragmentation and PCR failure.
However, immunohistochemical analysis of p53 protein expression
indicated that p53 was strongly expressed only in the
undifferentiated metastasis. Although the above mutations are
typical of different DTC histotypes, the peculiarity of the present
case is represented by the documentation of a chronological
sequence of the oncogenic mutations from the primary tumor to the
last undifferentiated metastasis. Taken together, the present
findings suggest that, in the current case, the main pathogenic
explanation was the rapid proliferation of p53-mutated neoplastic
clones whose growth was previously controlled by sorafenib, which
retrospectively appeared to be effective in the patient.
In conclusion, the present case confirms that
remarkable flare-ups should be always considered prior to sorafenib
withdrawal in all patients with metastatic tumors. In addition, the
present case offered a unique opportunity to document the
‘molecular history’ of an aggressive form of FTC, from the primary
tumor to the last undifferentiated metastasis.
Acknowledgements
The authors sincerely thank Dr Antonio Maccioni
(Surgical Pathology SS Trinità Hospital Cagliari, Italy), Dr
Giuseppe Salvatore Porcu (Surgical Pathology, Businco Hospital,
Cagliari) and Dr Giuseppe Bianchi (Surgical Pathology, Rizzoli
Bologna Hospital, Bologna, Italy) for providing paraffin-embedded
tissue samples of the surgically removed primary tumor and
metastatic lesions.
References
|
1
|
DeGroot LJ, Kaplan EL, McCormick M and
Straus FH: Natural history, treatment, and course of papillary
thyroid carcinoma. J Clin Endocrinol Metab. 71:414–424. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Haugen BR, Alexander EK, Bible KC, Doherty
GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM,
Schlumberger M, et al: American thyroid association management
guidelines for adult patients with thyroid nodules and
differentiated thyroid cancer: The American Thyroid Association
Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid
Cancer. Thyroid. 26:1–133. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Durante C, Haddy N, Baudin E, Leboulleux
S, Harti D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De
Vathaire F and Schlumberger M: Long-term outcome of 444 patients
with distant metastases from papillary and follicular thyroid
carcinoma: Benefits and limits of radioiodine therapy. J Clin
Endocrinol Metab. 91:2892–2899. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Smit JW, Vielvoye GJ and Goslings BM:
Embolization for vertebral metastases of follicular thyroid
carcinoma. J Clin Endocrinol Metab. 85:989–994. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Brose MS, Nutting CM, Jarzab B, Elisei R,
Siena S, Bastholt L, de la Fouchardiere C, Pacini F, Paschke R,
Shong YK, et al: Sorafenib in radioactive iodine-refractory,
locally advanced or metastatic differentiated thyroid cancer: A
randomised, double-blind, phase 3 trial. Lancet. 384:319–328. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schulmberger M, Tahara M, Wirth LJ,
Robinson B, Brose MS, Elisei R, Habra MA, Newbold K, Shah MH, Hoff
AO, et al: Lenvatinib versus placebo in radioiodine-refractory
thyroid cancer. N Engl J Med. 372:621–630. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang S, Pashtan I, Tsutsumi S, Xu W and
Neckers L: Cancer cells harboring MET gene amplification activate
alternative signaling pathways to escape MET inhibition but remain
sensitive to Hsp90 inhibitors. Cell Cycle. 8:2050–2056. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ruan M, Shen Y, Chen L and Li M: RECIST
1.1 and serum thyroglobulin measurements in the evaluation of
responses to sorafenib in patients with radioactive
iodine-refractory differentiated thyroid carcinoma. Oncol Lett.
6:480–486. 2013.PubMed/NCBI
|
|
9
|
Eilert KD and Foran DR: Polymerase
resistance to polymerase chain reaction inhibitors in bone. J
Forensic Sci. 54:1001–1007. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Basolo F, Pisaturo E, Pollina LE,
Fontanini G, Elisei R, Molinaro E, Iacconi P, Miccoli P and Pacini
F: N-ras mutation in poorly differentiated thyroid carcinomas:
Correlation with bone metastases and inverse correlation to
thyroglobulin expression. Thyroid. 10:19–23. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Melo M, da Rocha AG, Vinagre J, Batista R,
Peixoto J, Tavares C, Celestino R, Almeida A, Salgado C, Eloy C, et
al: TERT promoter mutations are a major indicator of poor outcome
in differentiated thyroid carcinoma. J Clin Endocrinol Metab.
99:E754–E765. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Landa I, Ganly I, Chan TA, Mitsutake N,
Matsuse M, Ibrahimpasic T, Ghossein RA and Fagin JA: Frequent
somatic TERT promoter mutations in thyroid cancer: Higher
prevalence in advanced forms of the disease. J Clin Endocrinol
Metab. 9:E1562–E1566. 2013. View Article : Google Scholar
|
|
13
|
Dobashi Y, Sugimura H, Sakamoto A, Mernyei
M, Mori M, Oyama T and Machinami R: Stepwise participation of p53
gene mutation during dedifferentiation of human thyroid carcinomas.
Diagn Mol Pathol. 3:9–14. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wolter P, Beuselinck B, Pans S and
Schöffski P: Flare-up: An often un reported phenomenon nevertheless
familiar to oncologists prescribing tyrosine kinase inhibitors.
Acta Oncol. 48:621–624. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Desar IM, Mulder SF, Stillebroer AB, van
Spronsen DJ, van der Graaf WT, Mulders PF and van Herpen CM: The
reverse side of the victory: Flare up of symptoms after
discontinuation of sunitinib or sorafenib in renal cell cancer
patients. A report of three cases. Acta Oncol. 48:927–931. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yun KJ, Kim W, Kim EH, Kim MH, Lim DJ,
Kang MI and Cha BY: Accelerated disease progression after
discontinuation of sorafenib in a patient with metastatic papillary
thyroid cancer. Endocrinol Metab (Seoul). 29:388–393. 2014.
View Article : Google Scholar : PubMed/NCBI
|