Introduction
Natural killer (NK)/T-cell lymphoma, an aggressive
malignancy, is a unique type of non-Hodgkin's lymphoma (NHL)
(1). It primarily occurs in the
nasal/nasopharyngeal region, accounting for ~75% of cases, with 4%
occurring in the skin and 6% in the gastrointestinal tract
(2). However, primary lymphoma
located within the esophagus is markedly rare, with an incidence of
<1% of all patients with lymphoma (3) and the majority of such cases are NHL.
Furthermore, to the best of our knowledge, only 6 cases of primary
NK/T-cell lymphoma of the esophagus have been identified (4–8). Owing to
the poorly defined early clinical and radiological signs, cases of
primary esophageal NK/T-cell lymphoma present difficulties to
physicians; therefore, appropriate preoperative diagnosis and
operative planning may be delayed.
In the present study discussed the case report of a
52-year-old male patient with esophageal NK/T-cell lymphoma who
presented with a 2-year history of postprandial fullness and
difficulty swallowing solid food, and was treated accordingly.
Primary esophageal NK/T-cell lymphoma is a markedly rare tumor and
is considered during the differential diagnosis of patients
presenting with a fungal or viral infection; however, only few
studies have reported cases of this cancer type. In the present
study, the imaging characteristics and clinical features of a rare
case of primary esophageal NK/T-cell lymphoma were analyzed, in
addition, the results of previous studies regarding this cancer
were reviewed.
Case report
A 52-year-old male presented to the First Affiliated
Hospital of Zhengzhou University (Zhengzhou, China) with a 2-year
history of postprandial fullness and difficulty swallowing solid
food. The patient did not complain of nausea, vomiting, fever,
weight loss or night sweats, and the physical examination and
laboratory blood tests were normal. In addition, the results of
coagulation studies, electrolyte level tests and tests of renal and
liver function were all within the normal limits. Increased levels
of tumor markers including cancer antigen (CA)125, CA199 and
carcinoembryonic antigen were not observed. A bone marrow biopsy
was negative for lymphoma.
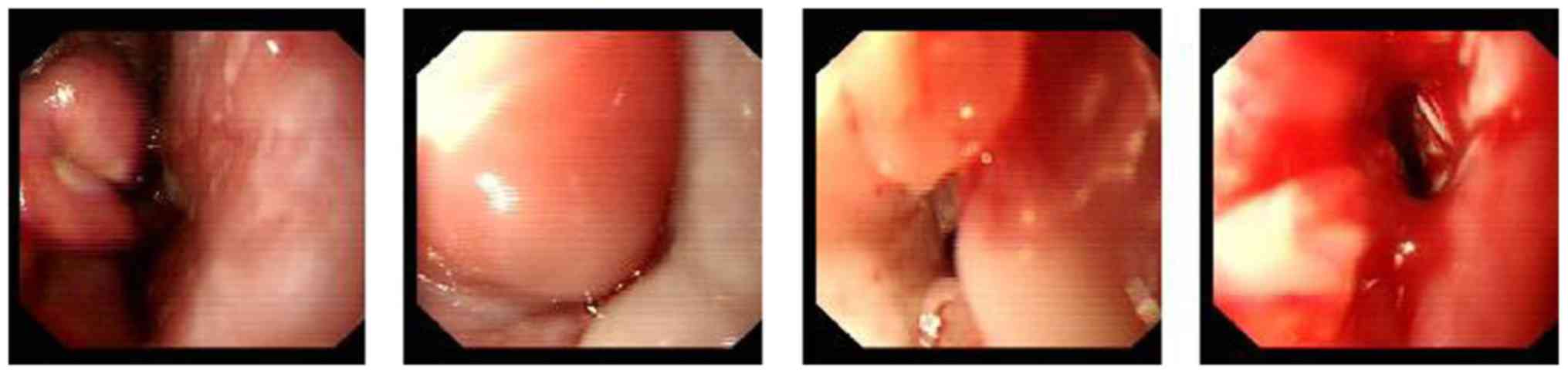
An esophagogastroduodenoscopy (Fig. 1) revealed diffuse mucous membrane
congestion and edema located along the entire length of the
esophagus. Additionally, multiple ovoid lesions with intact normal
mucosa were identified within 20 cm of the incisor teeth. The
remaining esophagus was irregular and stenotic which prevented the
esophagogastroduodenoscope from passing through. Biopsy specimens
from six esophageal sites of endoscopic mucosal resection were
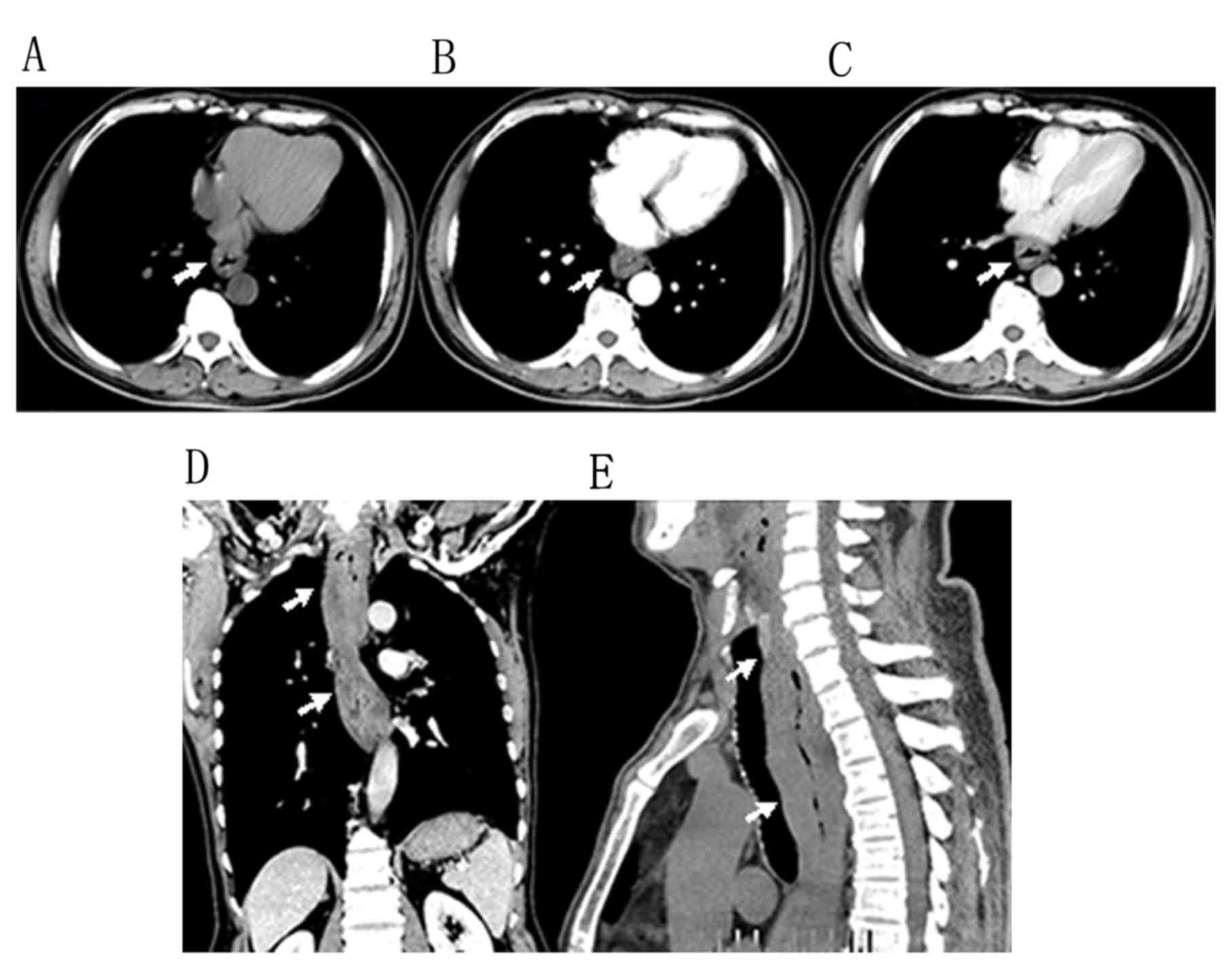
obtained for pathological evaluation. A chest computed tomography
(CT) scan (Fig. 2A-E) disclosed
diffuse thickening of the esophageal wall, with apparent stenosis
of the esophagus. A dynamic chest CT identified a well-defined
poorly enhanced mass in the abnormal esophagus (Fig. 2B and C). No enlarged lymph nodes were
detected in the centrilobular or paraseptal regions.
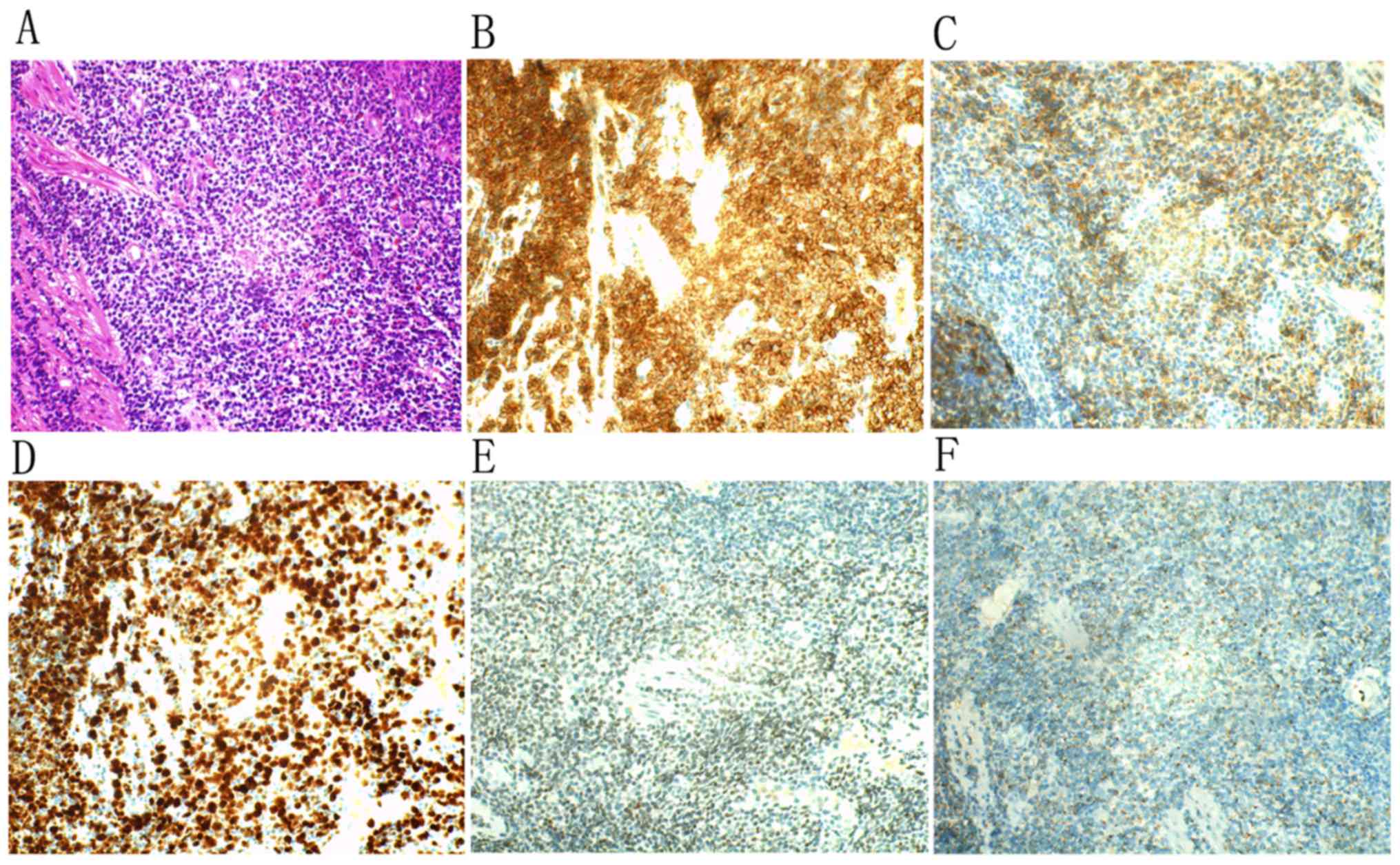
Histopathological examination of the biopsies of the
esophagus revealed moderate pleomorphic atypical lymphoid cells
disseminated in the lesions, with irregular nuclei and a pale
cytoplasm (Fig. 3A).
Immunohistochemistry was performed on formalin-fixed
paraffin-embedded tissue sections using the streptavidin biotin
peroxidase method (9).
Immunohistochemical staining of the biopsies were positive for
cluster of differentiation (CD)3 (Fig.
3B), CD56 (Fig. 3C) and Ki-67
(90%; Fig. 3D); weakly positive for
granzyme B (Fig. 3E) and cytotoxic
granule-associated RNA-binding protein (TIA-1) (Fig. 3F). However, biopsies were negative for
CD20 and cytokeratin. The results of the present study suggested
the diagnosis of NK/T-cell lymphoma.
The patient was staged as IIA, according to the Ann
Arbor system (7), and treated with 5
cycles of a cisplatine [50 mg day (d)1; 60 mg d2 d3], etoposide
VP-16 (180 mg d1-d3), ifosfamide (2 g d1-d3), dexamethasone (40 mg
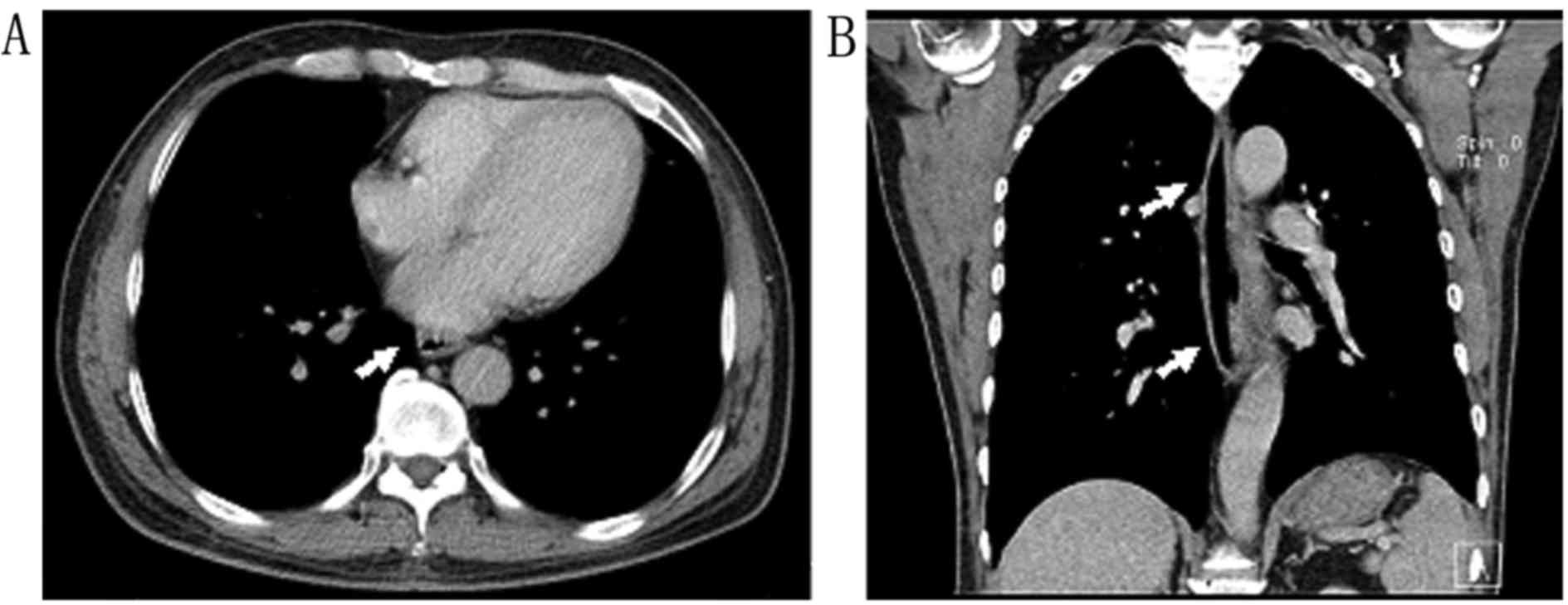
d1-d4) and mesna (0.4 g d1-d3) therapy regimen. Chest CT studies
following chemotherapy revealed prompt and marked shrinkage of the
tumor (Fig. 4). The patient remained
in remission until the last follow-up evaluation in July 2014. At
the time of writing, the patient has survived for 24 months with a
good quality of life without postprandial fullness or difficulty
swallowing solid food. Informed consent was obtained from the
patient for the present case report.
Literature review
The present study searched Pubmed, Medline, Google
Scholar, Chinese Biomedicine Database and the China Journal Full
Text Database for articles published in English and Chinese. The
search term used was: Lymphoma, Extranodal NK-T-Cell (MeSH).
Initially, five relevant items were identified using PubMed,
Medline, Google Scholar, Chinese Biomedicine Database and China
Journal Full Text Database. Publication dates ranged between June
1997 and June 2015. Each publication was reviewed and,
subsequently, five original studies were selected. The
characteristics of 6 patients with primary NK/T-cell lymphoma of
the esophagus is presented in Table
I.
 | Table I.Characteristics of 6 patients with
primary NK/T-cell lymphoma of the esophagus. |
Table I.
Characteristics of 6 patients with
primary NK/T-cell lymphoma of the esophagus.
| Author/(Refs.),
year | Complaint | Age, years | Sex | Site | Ulcers | EBV | Therapy | Survival time |
|---|
| Lee et al
(5), 2010 | Intermittent
retrosternal soreness | 45 | M | From the
gastroesophageal junction to the upper esophagus | + | + | Chemo | 495 days,
deceased |
| Fujihara et al
(6), 2014 | Dysphagia with throat
pain | 53 | M | Entire length of the
esophagus | + |
| Chemo and R | 4 months,
deceased |
| Zhang et al
(4), 2008 | Retrosternal
soreness | 45 | M | At 30 cm from the
incisor teeth | + | + | R | 9 months,
deceased |
| Zhang et al
(4), 2008 | Progressive
dysphagia | 61 | M | Mid and distal
esophagus | + |
| Chemo and R | 5 months,
deceased |
| Song et al
(7), 2014 | Dysphagia for solids
and liquids | 52 | M | Distal esophagus | + |
| Chemo |
|
| Tang and Li (8), 2014 | Dysphagia for solids
and liquids | 40 | F | Between the distal
esophagus and the gastric fundus | + |
|
|
|
Discussion
Extranodal NHL primarily occurs in the
gastrointestinal tract, with between 48 and 50% occurring in the
stomach, between 30 and 37% in the intestine, and between 12 and
13% in the ileocecal region (2). The
total number of patients with primary esophageal lymphoma was
<35 cases and the least common type is diffuse large B-cell type
NHL. According to a published study, Taal et al (10) identified only 2 cases of primary NHL
out of a total of 37 cases of esophageal NHL. NK/T-cell lymphoma is
a distinct subgroup of diffuse large B-cell type NHL with a diverse
spectrum of morphologies (11) and
accounts for between 2 and 8% of NHL in Asia, and <2% in Europe
(12). Primary esophageal NK/T cell
lymphoma is rare: In a review of published studies between 1997 and
June 2015 (Pubmed, Medline, Google Scholar, Chinese Biomedicine
Database and the China Journal Full Text Database), only 6 cases
were identified (4–8). Between May 2010 and July 2014, 346
patients with extranodal NHL confirmed by surgery and pathology
were retrospectively reviewed, and only 2 cases were esophageal
(0.6%); an indication that the lymphoid tissue present in a
particular segment has an association with the incidence of
lymphoma in the gastrointestinal tract (13).
Esophageal NK/T-cell lymphoma typically arises in
adult patients aged between 40 and 61 years, with the mean age of
49 years (almost 50% of described cases occurred in patients over
the age of 49). Esophageal NK/T-cell lymphoma is primarily in male
patients, with a male to female ratio of 5:1 (4–8). Patients
with esophageal lymphoma may present with dysphagia (3), odynophagia (14) and weight loss (9). Additional clinical features include
fever, night sweats (15), pharyngeal
pain (16) and epigastric pain
(17), and generalized weakness and
dizziness (18) may also be present.
Dysphagia symptoms are common due to the increased thickening of
the esophageal wall. However, a patient with esophageal NHL without
any clinical symptoms has been previously reported (19). Previous studies have demonstrated that
Epstein-Barr virus (EBV) infection has been determined in virtually
all patients with gastrointestinal NK/T cell lymphoma (20,21).
Although the association between EBV and esophageal NK/T cell
lymphoma is well-understood through previous clinical studies
(5,22), it is typically controversial. Kim
et al (20) identified that
the frequency of EBV-positivity is decreased in the esophagus due
to the limited number of EBV RNA tests available and the inclusion
of CD3ε+CD56− EBV. However, Lee et al
(5) revealed that viral esophagitis
may serve a role in the origin and development of NK/T cell
lymphoma, and noted benign conditions that mimic viral
esophagitis.
The criteria for primary extranodal lymphoma include
the following: i) Superficial lymph node involvement is absent; ii)
the initial symptoms are confined to the primary site; iii) the
tumor is limited to the primary region with an absence of adjacent
lymphoma or lymphoblastic leukemia; and iv) the possibility of
secondary lymphomas is excluded by test results. In the present
study, the patient presented to hospital with a 2-year history of
postprandial fullness and difficulty swallowing solid food. The
immunohistochemical staining suggested that the tumor meets the
diagnostic criteria for NK/T-cell lymphoma. Although biopsies,
obtained through esophagogastroduodenoscopy, are useful when making
a definitive diagnosis of esophageal NK/T-cell lymphoma,
misdiagnosis is often observed. This diagnostic delay is due to the
character of vascular invasion, which is a strong factor of
inflammatory cell infiltration, and the result of large-scale
necrosis is the main cause of misdiagnosing esophageal NK/T cell
lymphoma. Esophageal NK/T cell lymphoma is diagnosed by
immunophenotyping (5,6,11,12). The typical phenotype is the expression
of NK cell markers (including CD56), T cell-associated antigens
(including CD3 and CD2) and expression of cytotoxic markers
(including TIA-1, perforin and granzyme B), with negative results
for CD20 and CD23 (5,6,11,12). The present case demonstrated the
immune characteristics of tumor cells are typical of NK/T cell
lymphoma: CD3+, CD56+, TIA-1+ and
granzyme B+. Radiographic characteristics of esophageal
lymphoma have revealed a variety of abnormalities which are similar
to lymphoma in other gastrointestinal locations (10). Additionally, Crook and Robinson
(23) identified negative biopsy
results in a patient with a history of esophageal large B-cell
lymphoma, which suggests that analysis of cytological specimens may
be required to diagnose lymphoma. According to a previous study
which analyzed clinical and pathological results (9), primary esophageal lymphomas typically
arise in the lower esophagus. In the present study, the esophageal
wall, extending from the upper to the lower portion, was
extensively thickened. A previous study (24) suggested that ulceration, or tumors
which are ulceroinfiltrative, was a feature of esophageal NK/T cell
lymphomas (24). However, owing to
the limited number of distinguishing symptoms, including
ulcerations from other types of esophageal inflammation, it was not
possible to achieve a definitive diagnosis from the
esophagogastroduodenoscopy (24).
The clinical diagnosis of esophageal NK/T-cell
lymphoma is rare since it is difficult to make a correct
differential diagnosis on the basis of esophageal symptoms in
patients presenting with a fungal or viral infection,
therapy-related mucositis or reflux esophagitis (25). The diagnosis of esophageal NK/T-cell
lymphoma is often overlooked as it can present as dysphagia,
odynophagia or pharyngeal pain. Since esophageal NK/T-cell lymphoma
presents with the lack of specific clinical symptoms and signs, the
early diagnosis and appropriate treatment of this lymphoma may be
delayed. Patients with human immunodeficiency virus infection and
acquired immune deficiency syndrome may have an increased risk of
developing esophageal lymphoma; however, this is rare.
Immunohistochemical analysis of esophageal node and intestinal
polyp biopsies may assist in identifying patients with esophageal
NK/T-cell lymphoma. Since esophageal NK/T-cell lymphoma is a
relatively rare type of tumor arising from the esophageal
submucosa, the primary reasons for misdiagnosis are inadequate
analysis and improper biopsy. Examination by brush cytology may
assist in diagnosing this type of tumor.
Despite the diagnosis of esophageal NK/T-cell
lymphoma being clear, the disease was incurable (11). Primary gastrointestinal lymphoma is an
aggressive malignancy with vascular destruction, tissue necrosis
and a poor prognosis, with overall 5-year and 5-year disease-free
survival rates of 47 and 40%, respectively (11). A total of 79% of patients with primary
gastrointestinal lymphoma succumbed within 1 year of diagnosis
(11). It has been established that
prognostic factors include stage of the disease, extent of surgical
resection, response to treatment, serosal involvement,
multimodality treatment, and performance status of the patient
(11). Therefore, clinically
suspected malignant lymphoma requires early diagnosis and treatment
for the best outcome for the patient; however, an effective
standard treatment for this type of tumor remains unknown. Fujihara
et al (6) and Zhang et
al (4) have suggested that
systemic chemotherapy combined with concurrent radiotherapy may be
an effective treatment for esophageal NK/T-cell lymphoma. Lee et
al (5) identified a 45-year-old
male with esophageal NK/T-cell lymphoma who was treated by salvage
SMILE chemotherapy (dexamethasone, methotrexate, ifosfamide,
L-asparaginase and etoposide). Primary NK/T cell lymphoma of the
esophagus is rare; however, pathological and immunohistochemical
examinations of biopsy specimens may be useful in making an early
diagnosis.
Glossary
Abbreviations
Abbreviations:
|
NK/T-cell lymphoma
|
natural killer T cell lymphoma
|
|
NHL
|
non-Hodgkin's lymphoma
|
|
CT
|
computed tomography
|
|
EBV
|
Epstein-Barr virus
|
References
|
1
|
Wu X, Li P, Zhao J, Yang X, Wang F, Yang
YQ, Fang F, Xu Y, Zhang H, Wang WY and Yi C: A clinical study of
115 patients with extranodal natural killer/T-cell lymphoma, nasal
type. Clin Oncol (R Coll Radiol). 20:619–625. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ghimire P, Wu GY and Zhu L: Primary
esophageal lymphoma in immunocompetent patients: Two case reports
and literature review. World J Radiol. 2:334–338. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mori T, Komeno T and Ohtani H: Mantle cell
lymphoma-like solitary polypoid tumor of the esophagus: A case
report. Cases J. 2:66462009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang S, Wang H and Leng DN:
Clinicopathological observation on 2 cases of nasal-type NK/T-cell
lymphoma in the esophagus. Zhonghua Zhong Liu Za Zhi. 30:767–769.
2008.(In Chinese). PubMed/NCBI
|
|
5
|
Lee SR, Park EK, Won NH and Kim BS:
Esophageal involvement by extranodal natural killer T cell
lymphoma, nasal type, mimicking Epstein Barr viral esophagitis in a
tonsillar lymphoma patient undergoing chemoradiation therapy. Asia
Pac J Clin Oncol. 6:149–154. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fujihara S, Mori H, Kobara H, Nishiyama N,
Kobayashi M and Masaki T: Esophageal natural killer (NK)/T cell
lymphoma of true natural killer cell origin. Endoscopy. 46 Suppl 1
UCTN:E77–E78. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Song Y, Huang Y, Hu Y and He C: Primary
NK/T cell lymphoma of the esophagus: A case report. Chin J Oncol.
400:2014.(In Chinese).
|
|
8
|
Tang J and Li D: Primary extranodal NK/T
cell lymphoma, nasal type of the esophagus-gastric cardia: A case
report. Chin J Diffic Compl Cas. 645–66. 2014.(In Chinese).
|
|
9
|
Hosaka S, Nakamura N, Akamatsu T, Fujisawa
T, Ogiwara Y, Kiyosawa K, Hidaka E, Ota H, Katsuyama T and Inagaki
H: A case of primary low grade mucosa associated lymphoid tissue
(MALT) lymphoma of the oesophagus. Gut. 51:281–284. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Taal BG, Van Heerde P and Somers R:
Isolated primary oesophageal involvement by lymphoma: A rare cause
of dysphagia: Two case histories and a review of other published
data. Gut. 34:994–998. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li JZ, Tao J, Ruan DY, Yang YD, Zhan YS,
Wang X, Chen Y, Kuang SC, Shao CK and Wu B: Primary duodenal
NK/T-cell lymphoma with massive bleeding: A case report. World J
Clin Oncol. 3:92–97. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zheng S, Ouyang Q, Li G, Xu H, Jiang M,
Cui D, Xue L and Li J: Primary intestinal NK/T cell lymphoma: A
clinicopathologic study of 25 Chinese cases. Arch Iran Med.
15:36–42. 2012.PubMed/NCBI
|
|
13
|
Bandyopadhyay SK, Moulick A and Dutta A:
Primary duodenal lymphoma producing obstructive jaundice. J Assoc
Physicians India. 55:76–77. 2007.PubMed/NCBI
|
|
14
|
Coppens E, El Nakadi I, Nagy N and Zalcman
M: Primary Hodgkin's lymphoma of the esophagus. AJR Am J
Roentgenol. 180:1335–1337. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Radin DR: Primary esophageal lymphoma in
AIDS. Abdom Imaging. 18:223–224. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Doki T, Hamada S, Murayama H, Suenaga H
and Sannohe Y: Primary malignant lymphoma of the esophagus. A case
report. Endoscopy. 16:189–192. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kalogeropoulos IV, Chalazonitis AN,
Tsolaki S, Laspas F, Ptohis N, Neofytou I and Rontogianni D: A case
of primary isolated non-Hodgkin's lymphoma of the esophagus in an
immunocompetent patient. World J Gastroenterol. 15:1901–1903. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lin CC, Lai HW, Tsai MC, Chen TH, Tseng
SW, Chang H and Chen TY: Extranodal marginal zone B-cell lymphoma
of the gastrointestinal tract sparing only the esophagus: A case
report. Turk J Gastroenterol. 23:58–62. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kurihara K, Fukui A and Kumano S:
Malignant lymphoma of the esophagus associated with
macroglobulinemia: Report of a case. Pathol Int. 44:712–715. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kim TM, Lee SY, Jeon YK, Ryoo BY, Cho GJ,
Hong YS, Kim HJ, Kim SY, Kim CS, Kim S, et al: Clinical
heterogeneity of extranodal NK/T-cell lymphoma, nasal type: A
national survey of the Korean cancer study group. Ann Oncol.
19:1477–1484. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bautista-Quach MA, Ake CD, Chen M and Wang
J: Gastrointestinal lymphomas: Morphology, immunophenotype and
molecular features. J Gastrointest Oncol. 3:209–225.
2012.PubMed/NCBI
|
|
22
|
Jaffe ES, Chan JK, Su IJ, Frizzera G, Mori
S, Feller AC and Ho FC: Report of the workshop on nasal and related
extranodal angiocentric T/Natural killer cell lymphomas.
definitions, differential diagnosis and epidemiology. Am J Surg
Pathol. 20:103–111. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Crook TW and Robinson RA: Dysphagia in a
patient with a history of large B-cell lymphoma: Esophageal disease
with negative biopsy findings. Diagn Cytopathol. 26:167–169. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim JH, Lee JH, Lee J, Oh SO, Chang DK,
Rhee PL, Kim JJ, Rhee JC, Lee J, Kim WS and Ko YH: Primary
NK-/T-cell lymphoma of the gastrointestinal tract: Clinical
characteristics and endoscopic findings. Endoscopy. 39:156–160.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Santra G: Oesophageal involvement in
mantle cell lymphoma. Singapore Med J. 51:e201–e203.
2010.PubMed/NCBI
|