Introduction
Myeloproliferative neoplasms (MPNs) are cancers that
originate from hematopoietic stem cells and are characterized by
proliferation of myeloid cells. The classic Philadelphia
chromosome-negative MPNs (Ph−MPNs) include polycythaemia
vera (PV), essential thrombocythaemia (ET) and primary
myelofibrosis (PMF) (1). MPN patients
usually exhibit elevated blood cells and splenomegaly. The
JAK2V617F mutation is a diagnostic marker for MPN and it also plays
an important role in patient treatment since inhibition of
JAK2-associated proliferative pathways has the potential to inhibit
cell proliferation in MPNs (2). This
mutation is present in ~95% of PV patients and 50% of ET or PMF
patients (3,4). Thrombosis and haemostasis are major
complications that affect the life expectancy of patients with MPN.
The incidence of thrombosis ranges between 12 and 39% in PV
patients, ranges between 11 and 25% in ET patients (5), and is ~9.5% in PMF patients (6). Several studies have shown that
JAK2V617F+ patients experience a significantly increased
frequency of thrombosis complications compared with
JAK2V617F− patients, and that the thrombosis
complications are associated with the JAK2V617F+ mutant
allele burden (7,8).
Circulating microparticles (MPs) are small membrane
vesicles that are shed from activated and/or apoptotic cells, such
as platelets, endothelial cells and red blood cells. MPs express
specific antigens that are present on the surface of their mother
cells. MPs are considered to be biomarkers indicating the
procoagulant state associated with a host of clinical diseases,
including cancer, cardiovascular disease, sepsis and diabetes.
Numerous studies have shown that the levels of circulating MPs are
elevated in cancer patients, and that MPs contribute to the
development of thrombosis-associated complications (9–11). MPs
trigger blood coagulation and are expressed by numerous types of
cancer cells (8). It has been
suggested that the majority of MPs in cancer patients are derived
from tumour cells (12,13). At present, the effect of the
Ph− state on MPs has not yet been fully elucidated.
Therefore, the levels of MPs originating from platelets (PMPs), red
blood cell (RMPs), endothelial cells (EMPs) and tissue
factor-positive MPs (TF + MPs) were measured in patients with PV,
ET and PMF.
Materials and methods
Patients
Characteristics of the MPN patients included in the
present study are listed in Table I.
A total of 92 patients with MPN who were treated at the First
Affiliated Hospital of Soochow University were enrolled. Patients
with Ph−MPN were diagnosed according to the 2008 World
Health Organization (WHO) criteria. The present study included 60
patients with ET, 20 with PV and 12 with PMF. The MPN patients were
divided into two groups, a JAK2V617F mutation-positive group (n=55)
and a JAK2V617F mutation-negative group (n=37). Healthy volunteers
(n=30), with no history of thrombosis or cancer and no drug use
over the previous 2 weeks, were used as age- and sex-matched
controls. The present study was approved by the First Affiliated
Hospital of Soochow University Ethical Committee (Suzhou, China)
and patient consent was also obtained.
 | Table I.Clinical characteristics of patients
with myeloprolife-rative neoplasms. |
Table I.
Clinical characteristics of patients
with myeloprolife-rative neoplasms.
|
Characteristics | ET | PV | PMF |
|---|
| Cases, n | 60 | 20 | 12 |
| Sex, n |
|
|
|
|
Male | 26 | 8 | 6 |
|
Female | 34 | 12 | 6 |
| Median age,
years | 50 | 61 | 58 |
| Median WBC,
×109/1 | 10 | 12 | 12 |
| Median Hb, g/l | 128 | 186 | 74 |
| Median PLT,
×109/1 | 667 | 358 | 116 |
| Thrombosis, n |
|
|
|
|
Yes | 16 | 5 | 2 |
| No | 44 | 15 | 10 |
| Splenomegaly,
n |
|
|
|
|
Yes | 30 | 10 | 10 |
| No | 30 | 10 | 2 |
| JAK2V617F mutation,
n |
|
|
|
|
Yes | 32 | 17 | 6 |
| No | 28 | 3 | 6 |
Materials
Monoclonal CD235a-phycoerythrin (PE) (cat. no.
A07792), CD61-PE (cat. no. IM3605), CD142-PE (cat. no. 550312) and
CD62E-PE (cat. no. IM1243 U) antibodies (all dilutions, 1:100;
Beckman Coulter, Inc., Brea, CA, USA) were used for the detection
of RMPs, PMPs, EMPs, and TF + MPs. Flow-Count™ fluorescent
microspheres (diameter, 10 µm; density, 992/µl; Beckman Coulter)
were used for the calibration of the flow cytometry instrument, and
the Flow Cytometer FC500 instrument was obtained from Beckman
Coulter.
Sample collection and preparation
Samples of peripheral venous blood (3 ml) were
collected from patients with MPN and healthy control individuals
into 3.2% sodium citrate tubes (containing 300 nM PGE1).
Platelet-poor plasma (PPP) was obtained by centrifugation at 1,900
× g twice for 15 min and then stored at −80°C until use. Samples
were processed within 2 h of collection.
Detection of MPs by flow
cytometry
After thawing, PPP was diluted in PBS (dilution,
1:10), with 5 µl of the aforementioned monoclonal CD235a-PE,
CD61-PE, CD142-PE and CD62E-PE antibodies. Samples were incubated
with the antibodies for 30 min in the dark at room temperature.
Subsequently, 10 µl Flow-Count fluorescent microspheres was added
to all tubes as a calibration for the calculation of the absolute
concentration of MPs in PPP. MPs were resuspended and mixed in PBS
prior to loading for flow cytometry. Rat anti-human IgG-PE
(dilution, 1:100; cat. no. PA129628; Thermo Fisher Scientific,
Inc., Waltham, MA, USA) was used as a negative control. Forward
scatter was calibrated using fluorescent microspheres of 0.8 µm.
Standard fluorescent microbeads (0–0.8 µm) in diameter were used to
set the MP gate. The flow cytometer analysed 20,000 particles, and
the number of MPs and fluorescent microspheres were presented in
the upper right quadrant of the flow cytometric graph. All flow
cytometry data were analysed using BD CellQuest Pro 5.1 software
(BD Biosciences, San Jose, CA, USA). MP analyses were performed
using the flow cytometer as previously described (14). The absolute number of MPs was
calculated using the following formula: (992x number of MPs)/(4x
number of Flow-Count fluorescent microspheres).
JAK2V617F mutation detection
Total genomic DNA was extracted from
EDTA-anticoagulated peripheral blood samples using the UNlQ-10
Column Clinical Sample DNA Isolation kit (cat. no. B511341; Sangon
Biotech Co., Ltd., Shanghai, China) according to the manufacturer's
protocol. The JAK2V617F mutation was detected using allele-specific
PCR, as previously described (15). A
sample of 80 ng of each patient's DNA was PCR amplified in the ABI
9600 machine (Applied Biosystems, Foster City, CA) using the
specific forward primer (0.5 µmol/l),
5′AGCATTTGGTTTTAAATTATGGAGTATATT 3′, the internal control primer
(0.5 µmol/l), 5′ATCTATAGTCATGCTGAAAGTAGGAGAAAG3′ and the reverse
primer (1 µmol/l) 5′CTGAATAGTCCTACAGTGTTTTCAGTTTCA3′. The
thermocycler parameters were 36 cycles of 30 sec at 94°C, 58°C for
30 sec and 72°C for 45 sec Subsequently, LDR products were analyzed
with a DNA sequencer (model 377; Applied Biosystems; Thermo Fisher
Scientific, Inc.). All assays were conducted without the knowledge
of case or control status.
Statistical analysis
Statistical analysis was performed using SPSS 17.0
software (SPSS, Inc., Chicago, IL, USA). Data were expressed as the
mean ± standard deviation. Two-tailed unpaired Student's t-tests
were used for comparison between two groups. One-way analysis of
variance with Dunnett's multiple comparisons test was used to
compare the differences amongst groups (n≥3). Spearman's rank
correlation coefficient was used for correlation analysis.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Alteration of MP level in patients
with MPN
The abundance of the four types of MPs was increased
in patients with Ph−MPN compared with healthy control
individuals [RMPs (24.4±20.2/µl), PMPs (95.2±55.8/µl) and EMPs
(193.1±127.1/µl), all P<0.01; TF + MPs (193.1±127.1/µl),
P<0.05]. It was also found that the abundance of the four types
of MPs in patients with PMF was increased compared with patients
with PV (P<0.05). No evident difference was identified between
the MP levels in PV and ET groups, with the exception of EMPs
(Fig. 1).
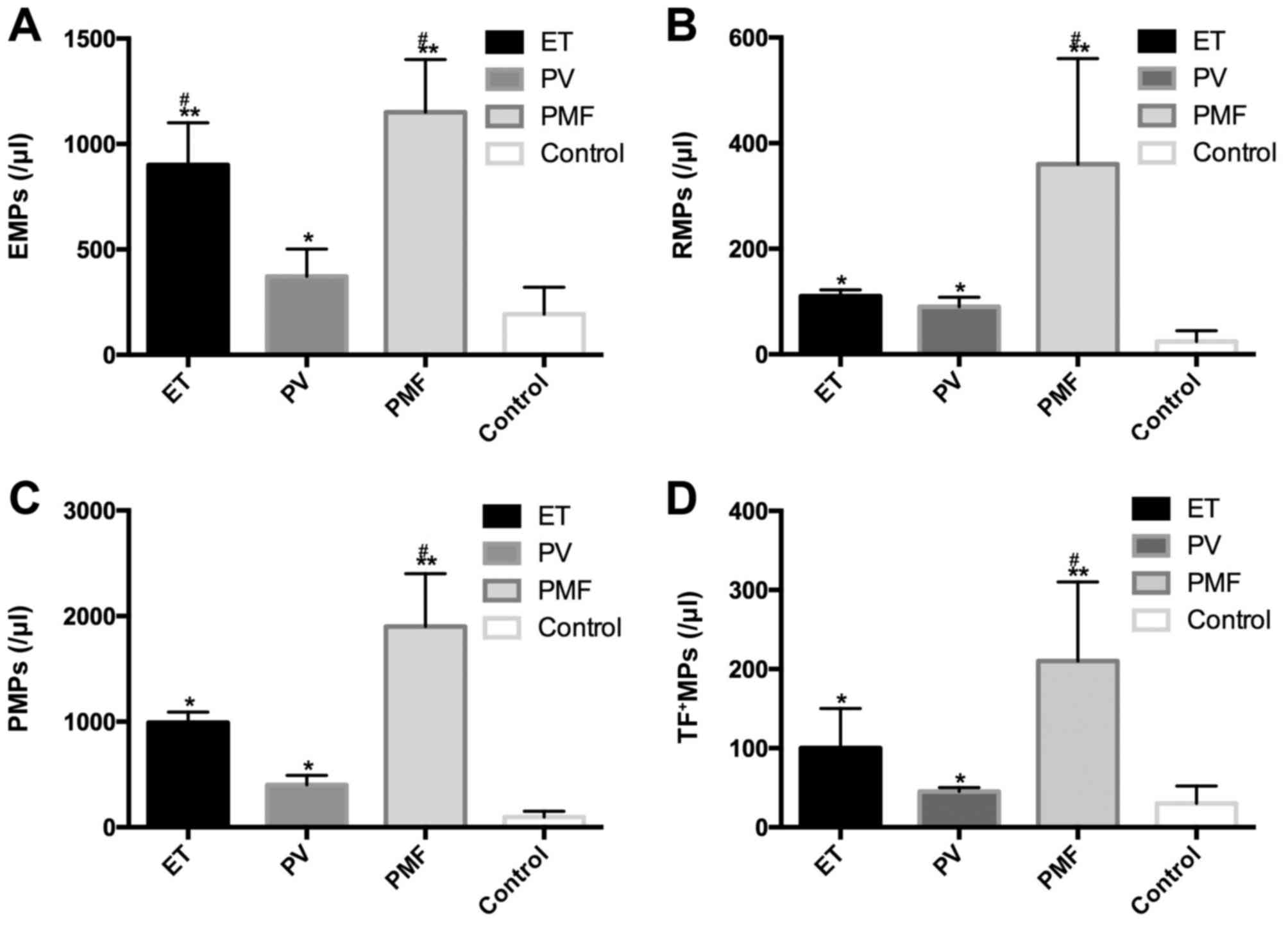 | Figure 1.Comparison of MP abundance in patients
with different subtypes of Ph−MPN. The level of all four
types of MPs was increased in patients with MPN compared with the
control group. (A) EMP abundance in patients with ET and PMF was
increased compared with patients with PV. (B) RMP abundance in
patients with PMF was increased compared with patients with PV. (C)
PMP abundance in patients with PMF was increased compared with
patients with PV. (D) TF + MP abundance in patients with PMF
increased compared with patients with PV. *P<0.05, **P<0.01
vs. Control. #P<0.05 vs. PV. Ph−MPN,
Philadelphia chromosome-negative myeloproliferative neoplasms; ET,
essential thrombocythaemia; PV, polycythaemia vera; PMF, primary
myelofibrosis; MPs, microparticles; EMPs, endothelial MPs; PMPs,
platelet-derived MPs; RMPs, red blood cell MPs; TF+MPs, tissue
factor-positive MPs. |
MPs and MPN-associated thrombotic
complications and splenomegaly
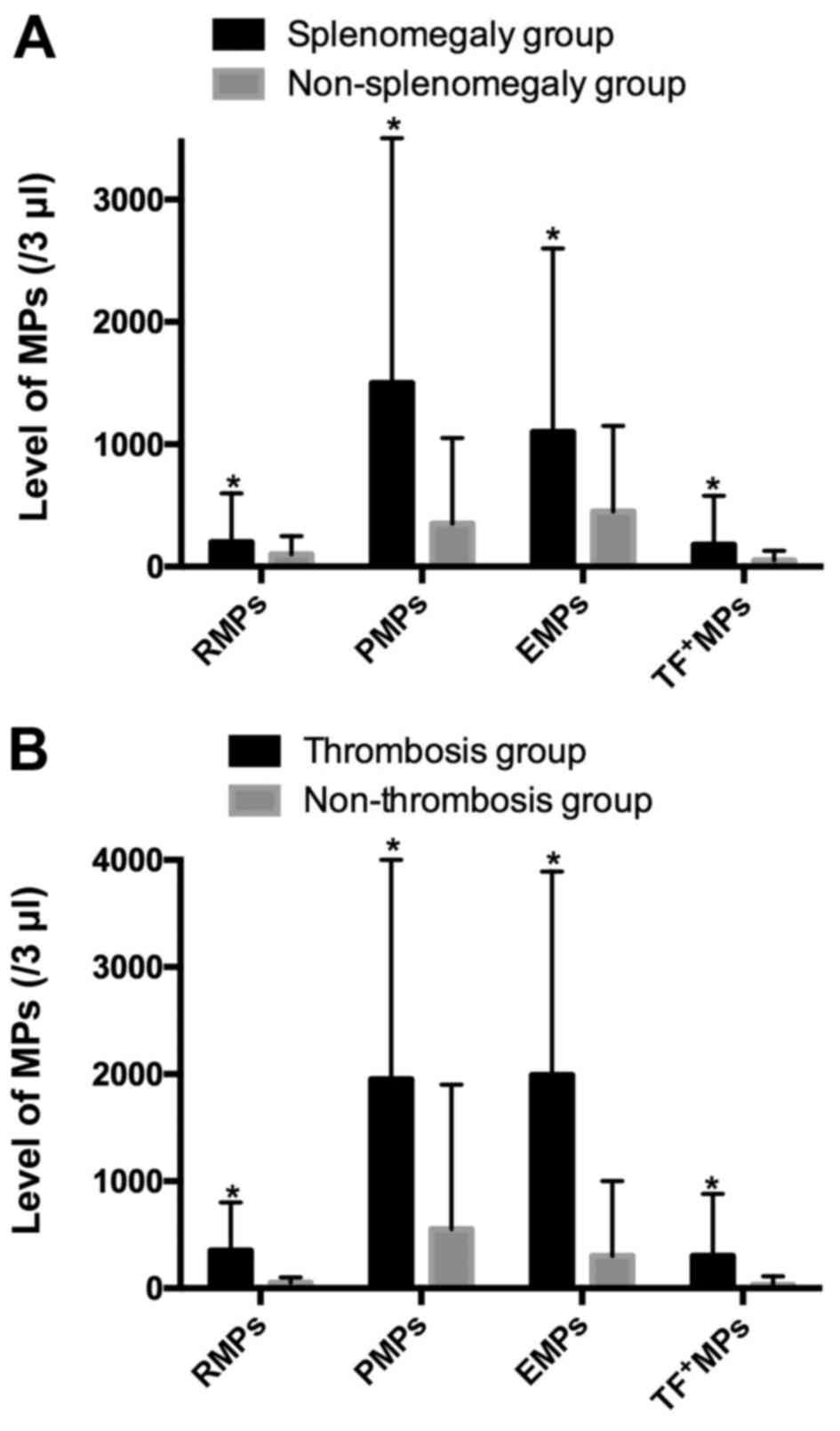
In the present sample, 50 patients were diagnosed
with splenomegaly and 42 patients were not diagnosed with
splenomegaly. The mean concentration of RMPs, PMPs, EMPs and TF +
MPs in the splenomegaly group was 189.9+370.9, 1,447.5+1,873.1,
1,092.1+1,518.9 and 157.9+403.4/µl, respectively, and these values
were significantly increased compared with those in the
non-splenomegaly group, which were 69.9±127.2, 381.1±656.8,
471.6±682.3 and 37.9±45.3/µl (P<0.05), respectively, as shown in
Fig. 2A.
Among the 92 MPN patients, there were 23 patients
with thrombosis complications and 69 without thrombosis. The mean
concentration of RMPs, PMPs, EMPs, and TF + MPs in thrombosis group
was 375.9+504.5, 1989.7+2,023.7, 2000.5±1,851.7 and 268.0+566.0/µl,
respectively. These counts were significantly increased compared
with the non-thrombosis group, which were 54.9+72.6, 617.7+1,169.5,
411.6+568.2 and 48.2+86.5/µl (P<0.05), as shown in Fig. 2B.
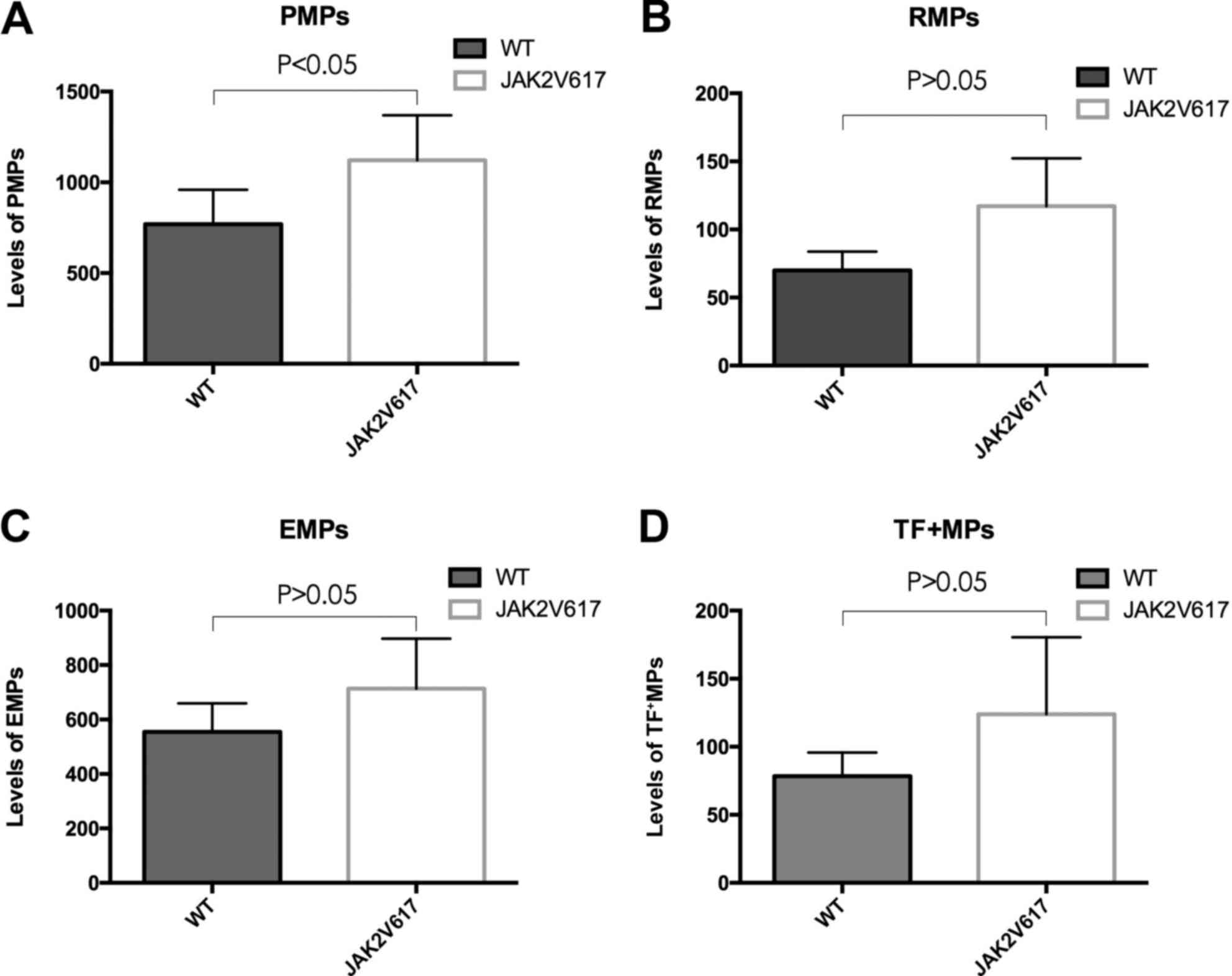
Association between MPs and the
JAK2V617F mutation
The MPN patients were divided into
JAK2V617F+ (n=50) and JAK2V617F− (n=42)
groups. PMP levels in the JAK2V617F+ group were found to
be increased compared with the JAK2V617F− group
(Fig. 3A). No statistically
significant differe-nces were observed between the levels of the
three remaining MPs in the two groups (Fig. 3B-D).
Discussion
MPs are small membrane vesicles that are secreted by
almost all types of cells during activation, apoptosis or injury.
Increased levels of procoagulant MPs in the blood may result in
thrombogenesis (16). Several animal
studies have investigated and confirmed the function of MPs in
cancer models. Yu et al (17)
showed that mice with colorectal tumours showed increased levels of
tumour-derived MPs, and the levels of circulating MPs were
associated with tumour progression. Circulating MPs were also shown
by Davila et al (18) to be
associated with the activation of coagulation in mice with
pancreatic tumours. A study by Thomas et al (19) showed that MPs enhance the development
of thrombosis in mice.
MPs are potentially procoagulant and they have a
crucial role in thrombosis and haemostasis. Scott syndrome is a
bleeding disorder that is characterised by the diminished excretion
of phosphatidylserine to the cell surface of activated platelets
(20). A large number of studies have
detected elevated circulating MPs in cancer patients, and observed
that the composition of MPs in cancer patients was different from
that of healthy controls. Hron et al (21) found that patients with advanced
colorectal cancer exhibited increased levels of MPs, which were
almost exclusively derived from platelets (21). A previous study found increased levels
of MPs in patients with pancreatic and metastatic breast cancer
compared to controls (22). The MPs
that are found in patients with acute promyelocytic leukaemia are
mainly TF + MPs that are derived from promyelocytic cells, with low
levels of PMPs, which may be the result of decreased platelet
counts, as reported by Ma et al (23). In addition, patients with venous
thromboembolism (VTE) exhibit an increased level of MPs compared
with patients without VTE (24). At
present, there has been little research into the role of MPs in
Ph−MPN patients. Trappenburg et al (25) reported that ET patients have elevated
levels of PMPs, EMPs and TF + MPs, with the exception of RMPs.
However, to the best of our knowledge, no previous study has
considered the variation in level of MPs in PV and PMF patients. As
Trappenburg et al (25)
described, ET patients have been observed to show increased von
Willebrand factor, which is synthesized by endothelial cells and
has an important role in platelet thrombus formation, accompanied
by elevated MPs.
The plasma levels of four types of MPs (RMPs, PMPs,
EMPs and TF + MPs) were evaluated in 92 Ph−MPN patients
by flow cytometry. The present study reveals an increased number of
MPs in MPN patients compared with controls. Additionally, it was
found that RMPs were elevated in Ph−MPN patients and
that MPs are elevated in patients with PV or PMF. No correlation
between PMPs and platelet counts was identified, which may be due
to the frequently abnormal platelet function of MPN patients. The
increasing number of EMPs that was observed is indicative of
endothelial cell activation.
The ET-associated result is consistent with the
previous findings of Trappenburg et al (25). Increased numbers of MPs were observed
in PMF patients compared with ET and PV patients, and the prognosis
of PMF patients is less favourable than that of other MPN patients.
Due to the limitation of a small number of patients in the present
study, the impact of MPs on different phenotypes requires
additional study.
Thrombosis and splenomegaly are common complications
in MPN patients, and the former varies from mild microcirculatory
disturbances to severe and potentially fatal complications, such as
ischemic stroke and acute myocardial infarction. A previous study
by Duchemin et al (26)
documented increased thrombin generation in MPN patients. This
result is compatible with previous observations in patients with
other cancers (27). Splenomegaly,
resulting from extramedullary haematopoiesis, is present in almost
all PMF patients and a subset of ET and PV patients at diagnosis.
It is associated with systemic symptoms that have a negative impact
on the quality of life and life expectancy (28). Increased MPs may promote thrombosis in
MPN patients with splenomegaly.
Among the patients in the present study, 23 patients
showed various thrombotic complications and 69 cases did not show
evidence of thrombosis, while 50 showed splenomegaly and 42 did
not. The present results show that the levels of MPs in the group
of patients with thrombosis were increased compared with those in
the non-thrombosis group. The levels of MPs in the patients with
splenomegaly were increased compared with those in the patients
without splenomegaly. To the best of our knowledge, the present
study is the first to describe the association between MPs,
thrombosis and splenomegaly complications in Chinese patients with
MPN.
The JAK2V617F mutation often occurs in patients with
Ph−MPN. It has been reported that the JAK2V617F mutation
is associated with the increased occurrence of thrombosis in MPN
patients (29–31). Marchetti et al (32) showed that ET patients with the
JAK2V617F mutation were more procoagulant than patients without the
mutation, and that JAK2V617F was the major determinant that
contributes to increased thrombin generation. However, to the best
of our knowledge, no previous study has addressed the association
between the JAK2V617F mutation, MPs and thrombosis.
To evaluate the potential association between the
JAK2V617F mutation and MPs, JAK2V617F mutation screening was
performed by allele-specific polymerase chain reaction. A total of
17 PV patients (85.0%), 32 ET patients (53.3%) and 6 PMF patients
(50.0%) were positive for the JAK2V617F mutation. The present study
found that the concentration of PMPs in the JAK2V617F+
group is increased compared with the group lacking the mutation.
The increased level of PMPs observed in MPN patients with the
JAK2V617F mutation indicates that the JAK2V617F mutation may
enhance a hypercoagulable state.
In summary, the present study observed elevated
levels of MPs (RMPs, PMPs, EMPs and TF + MPs) in patients with MPN.
Increased values were present in patients with thrombosis or
splenomegaly. In addition, increased MPs were also observed in
JAK2V617F-positive patients, compared with JAK2V617F-negative
patients. Therefore, MPs may be useful as a new biomarker for the
development of thrombotic events in MPN patients. Additional
prospective studies are required to better understand the relevance
of MPs in different subtypes of MPN, and to explore their potential
roles in the diagnosis and prognosis of MPN patients.
Acknowledgements
The authors thank San Francisco Edit for their
assistance in editing this manuscript. This study was supported by
grants from the Jiangsu Province of China (grant nos. BK20131167,
RC2011105 and ZX201102), National Nature Science Foundation of
China (grant nos. 81270591 and 81670132), National Key Basic
Research Program of China (grant no. 2012CB526600), Jiangsu
Provincial Special Program of Social Development (grant no.
SBE2016740635), Jiangsu Provincial Special Program of Medical
Science (grant no. BL2012005), and the Priority Academic Program
Development of Jiangsu Higher Education Institutions.
References
|
1
|
Tefferi A and Vardiman JW: Classification
and diagnosis of myeloproliferative neoplasms: The 2008 World
Health Organization criteria and point-of-care diagnostic
algorithms. Leukemia. 22:14–22. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Barrio S, Gallardo M, Arenas A, Ayala R,
Rapado I, Rueda D, Jimenez A, Albizua E, Burgaleta C, Gilsanz F and
Martinez-Lopez J: Inhibition of related JAK/STAT pathways with
molecular targeted drugs shows strong synergy with ruxolitinib in
chronic myeloproliferative neoplasm. Br J Haematol. 161:667–676.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Levine RL, Wadleigh M, Cools J, Ebert BL,
Wernig G, Huntly BJ, Boggon TJ, Wlodarska I, Clark JJ, Moore S, et
al: Activating mutation in the tyrosine kinase JAK2 in polycythemia
vera, essential thrombocythemia, and myeloid metaplasia with
myelofibrosis. Cancer Cell. 7:387–397. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Baxter EJ, Scott LM, Campbell PJ, East C,
Fourouclas N, Swanton S, Vassiliou GS, Bench AJ, Boyd EM, Curtin N,
et al: Acquired mutation of the tyrosine kinase JAK2 in human
myeloproliferative disorders. Lancet. 365:1054–1061. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tefferi A: Polycythemi a vera and
essential thrombocythemia: 2012 update on diagnosis, risk
stratification, and management. Am J Hematol. 87:285–293. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Barbui T, Carobbio A, Cervantes F,
Vannucchi AM, Guglielmelli P, Antonioli E, Alvarez-Larrán A,
Rambaldi A, Finazzi G and Barosi G: Thrombosis in primary
myelofibrosis: Incidence and risk factors. Blood. 115:778–782.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cheung B, Radia D, Pantelidis P,
Yadegarfar G and Harrison C: The presence of the JAK2 V617F
mutation is associated with a higher haemoglobin and increased risk
of thrombosis in essential thrombocythemia. Br J Haematol.
132:244–245. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Finazzi G, Rambaldi A, Guerini V, Carobbo
A and Barbui T: Risk of thrombosis in patients with essential
thrombocythemia and polycythemia vera according to JAK2 V617F
mutation status. Haematologica. 92:135–136. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Willms A, Müller C, Julich H, Klein N,
Schwab R, Güsgen C, Richardsen I, Schaaf S, Krawczyk M, Krawczyk M,
et al: Tumour-associated circulating microparticles: A novel liquid
biopsy tool for screening and therapy monitoring of colorectal
carcinoma and other epithelial neoplasia. Oncotarget.
7:30867–30875. 2016.PubMed/NCBI
|
|
10
|
Tseng CC, Wang CC, Hsiao CC, Lu HI, Leu S,
Chang HC, Huang KT, Fang WF, Chen YM, Liu SF, et al: Time courses
and value of circulating microparticles in patients with operable
stage non-small cell lung cancer undergoing surgical intervention.
Tumour Biol. 37:11873–11882. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Campello E, Zanetto A, Spiezia L, Radu CM,
Gavasso S, Ferrarese A, Farinati F, Senzolo M and Simioni P:
Hypercoagulability detected by circulating microparticles in
patients with hepatocellular carcinoma and cirrhosis. Thromb Res.
143:118–121. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Owens AP III and Mackman N: Microparticles
in hemostasis and thrombosis. Circ Res. 108:1284–1297. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zwicker JI, Liebman HA, Neuberg D, Lacroix
R, Bauer KA, Furie BC and Furie B: Tumor-derived tissue
factor-bearing microparticles are associated with venous
thromboembolic events in malignancy. Clin Cancer Res. 15:6830–6840.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Morel O, Luca F, Grunebaum L, Jesel L,
Meyer N, Desprez D, Robert S, Dignat-George F, Toti F, Simon C and
Goichot B: Short-term very low-calorie diet in obese females
improves the haemostatic balance through the reduction of leptin
levels, PAI-1 concentrations and a diminished release of platelet
and leukocyte-derived microparticles. Int J Obes (Lond).
35:1479–1486. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Baxter EJ, Scott LM, Campbell PJ, East C,
Fourouclas N, Swanton S, Vassiliou GS, Bench AJ, Boyd EM, Curtin N,
et al: Acquired mutation of the tyrosine kinase JAK2 in human
myeloproliferative disorders. Lancet. 365:1054–1061. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Boulanger CM, Amabile N and Tedgui A:
Circulating microparticles: A potential prognostic marker for
atherosclerotic vascular disease. Hypertension. 48:180–186. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yu JL, May L, Lhotak V, Shahrzad S,
Shirasawa S, Weitz JI, Coomber BL, Mackman N and Rak JW: Oncogenic
events regulate tissue factor expression in colorectal cancer
cells: Implications for tumor progression and angiogenesis. Blood.
105:1734–1741. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Davila M, Amirkhosravi A, Coll E, Desai H,
Robles L, Colon J, Baker CH and Francis JL: Tissue factor-bearing
microparticles derived from tumor cells: Impact on coagulation
activation. J Thromb Haemost. 6:1517–1524. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Thomas GM, Panicot-Dubois L, Lacroix R,
Dignat-George F, Lombardo D and Dubois C: Cancer cell-derived
microparticles bearing P-selectin glycoprotein ligand 1 accelerate
thrombus formation in vivo. J Exp Med. 206:1913–1927. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Weiss HJ: Scott syndrome: A disorder of
platelet coagulant activity. Semin Hematol. 31:312–319.
1994.PubMed/NCBI
|
|
21
|
Hron G, Kollars M, Weber H, Sagaster V,
Quehenberger P, Eichinger S, Kyrle PA and Weltermann A: Tissue
factor-positive microparticles: Cellular origin and association
with coagulation activation in patients with colorectal cancer.
Thromb Haemost. 97:119–123. 2007.PubMed/NCBI
|
|
22
|
Rodriguez P Garcia, Eikenboom HC,
Tesselaar ME, Huisman MV, Nijkeuter M, Osanto S and Bertina RM:
Plasma levels of microparticle-associated tissue factor activity in
patients with clinically suspected pulmonary embolism. Thromb Res.
126:345–349. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ma G, Liu F, Lv L, Gao Y and Su Y:
Increased promyelocytic-derived microparticles: A novel potential
factor for coagulopathy in acute promyelocytic leukemia. Ann
Hematol. 92:645–652. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tesselaar ME, Romijn FP, van der Linden
IK, Prins FA, Bertina RM and Osanto S: Microparticle-associated
tissue factor activity: A link between cancer and thrombosis? J
Thromb Haemost. 5:520–527. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Trappenburg MC, van Schilfgaarde M,
Marchetti M, Spronk HM, ten Cate H, Leyte A, Terpstra WE and
Falanga A: Elevated procoagulant microparticles expressing
endothelial and platelet markers in essential thrombocythemia.
Haematologica. 94:911–918. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Duchemin J, Ugo V, Ianotto JC, Lecucq L,
Mercier B and Abgrall JF: Increased circulating procoagulant
activity and thrombin generation in patients with
myeloproliferative neoplasms. Thromb Res. 126:238–242. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Campello E, Spiezia L, Radu CM, Bulato C,
Castelli M, Gavasso S and Simioni P: Endothelial, platelet, and
tissue factor-bearing microparticles in cancer patients with and
without venous thromboembolism. Thromb Res. 127:473–477. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Randhawa J, Ostojic A, Vrhovac R, Atallah
E and Verstovsek S: Splenomegaly in myelofibrosis-new options for
therapy and the therapeutic potential of Janus kinase 2 inhibitors.
J Hematol Oncol. 5:432012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lee HS, Park LC, Lee EM, Lee SJ, Shin SH,
Im H, Do KM, Kim EJ, Ye BJ, Song MK, et al: Incidence rates and
risk factors for vascular events in patients with essential
thrombocythemia: A multicenter study from Korea. Clin Lymphoma
Myeloma Leuk. 12:70–75. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lussana F, Caberlon S, Pagani C,
Kamphuisen PW, Büller HR and Cattaneo M: Association of V617F Jak2
mutation with the risk of thrombosis among patients with essential
thrombocythaemia or idiopathic myelofibrosis: A systematic review.
Thromb Res. 124:409–417. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Antonioli E, Guglielmelli P, Poli G,
Bogani C, Pancrazzi A, Longo G, Ponziani V, Tozzi L, Pieri L and
Santini V: Influence of JAK2V617F allele burden on phenotype in
essential thrombocythemia. Haematologica. 93:41–48. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Marchetti M, Tartari CJ, Russo L,
Panova-Noeva M, Leuzzi A, Rambaldi A, Finazzi G, Woodhams B and
Falanga A: Phospholipid-dependent procoagulant activity is highly
expressed by circulating microparticles in patients with essential
thrombocythemia. Am J Hematol. 89:68–73. 2014. View Article : Google Scholar : PubMed/NCBI
|