Introduction
The female genital tract is rarely involved by
metastatic tumors. The most common anatomic locations for
metastases to the female genital tract are the ovaries and the
vagina. Among extragenital cancers metastasizing to the female
genital tract, breast is the most common primary site, followed by
the gastrointestinal tract, lung, kidney, and skin (melanoma)
(1,2).
Metastases to the uterus from extragenital cancer are less common
(3), but up to 8% of breast
carcinomas will metastasize to that organ (4). Lobular carcinoma is the most common type
of breast carcinoma that metastasizes to the uterus (5). When an extragenital tumor metastasizes
to the uterus, it is predominantly located in the myometrium; in a
minority of cases, the metastasis is confined to the endometrium
(1,2).
In this article, we present a case of concurrent metastatic breast
carcinoma to an endometrial polyp, a uterine leiomyoma, and the
uterine cervix. This is the first reported case with this
combination. We also review the literature.
Case report
A 58-year-old postmenopausal Japanese woman
presented to our gynecological outpatient department with abnormal
uterine bleeding in 2015. Nine years previously, she had undergone
breast-conserving surgery for cancer of the right breast.
Histopathologic examination of that mass revealed a stage IIIc
invasive ductal carcinoma in the breast, with large groups of
lobular cancer cells and very small groups of ductal cancer cells
found in the lymph nodes. After surgery of the breast cancer, the
patient had been received adjuvant chemotherapy (doxifluridine 5
years, cyclophosphamide 3 years and docetaxel 1 years) radiotherapy
(60 Gy to the right breast) and hormone therapy (goserelin acetate
6 years, tamoxifen 4 months, toremifene citrate 3 years).
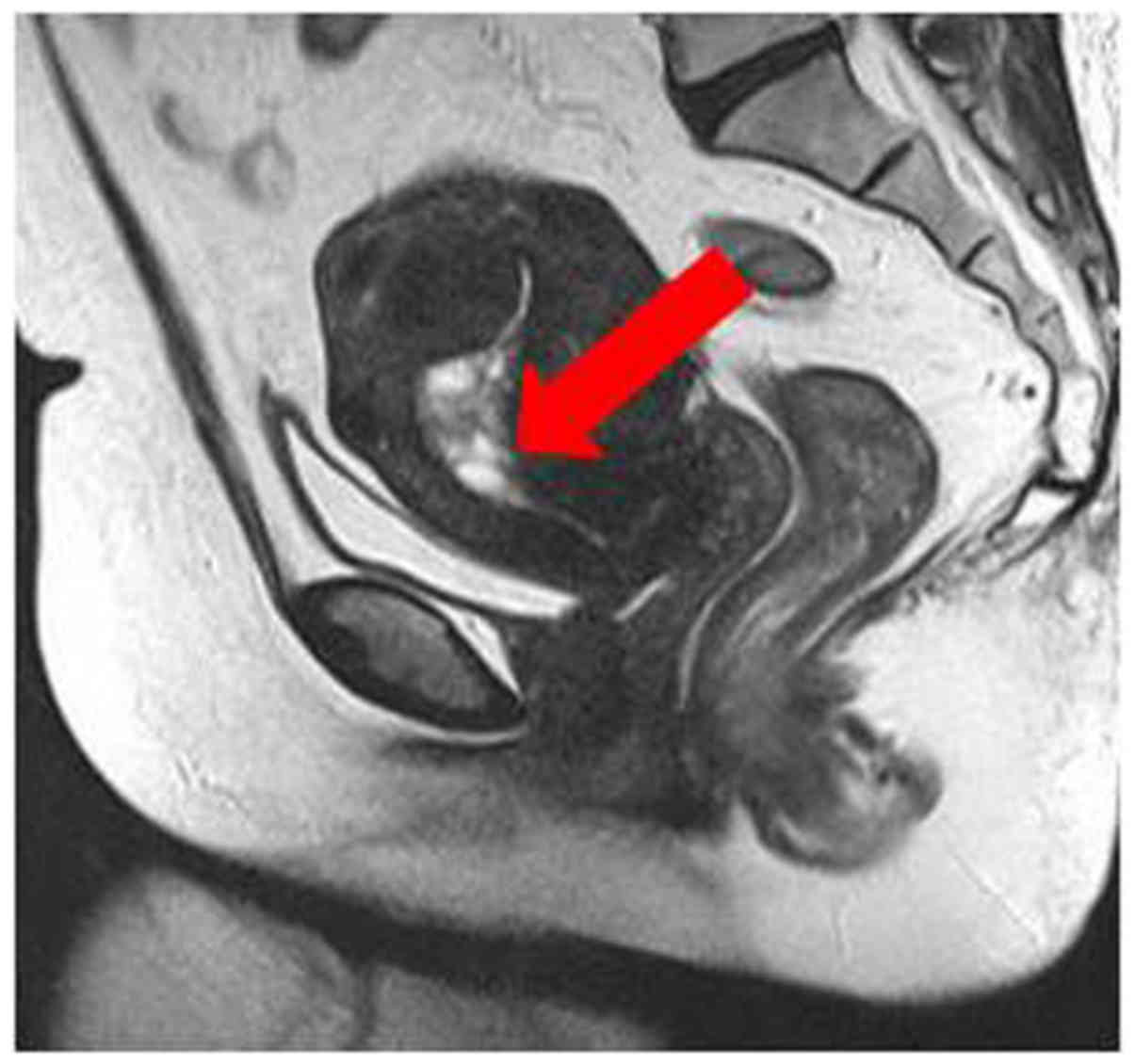
A diagnostic work-up was initiated to detect
possible causes of vaginal bleeding. She underwent transvaginal
ultrasound, which revealed endometrial thickening (9 mm). Magnetic
resonance imaging (MRI) revealed a thickened endometrial myometrium
(16×32 mm) with multicystic tumors (Fig.
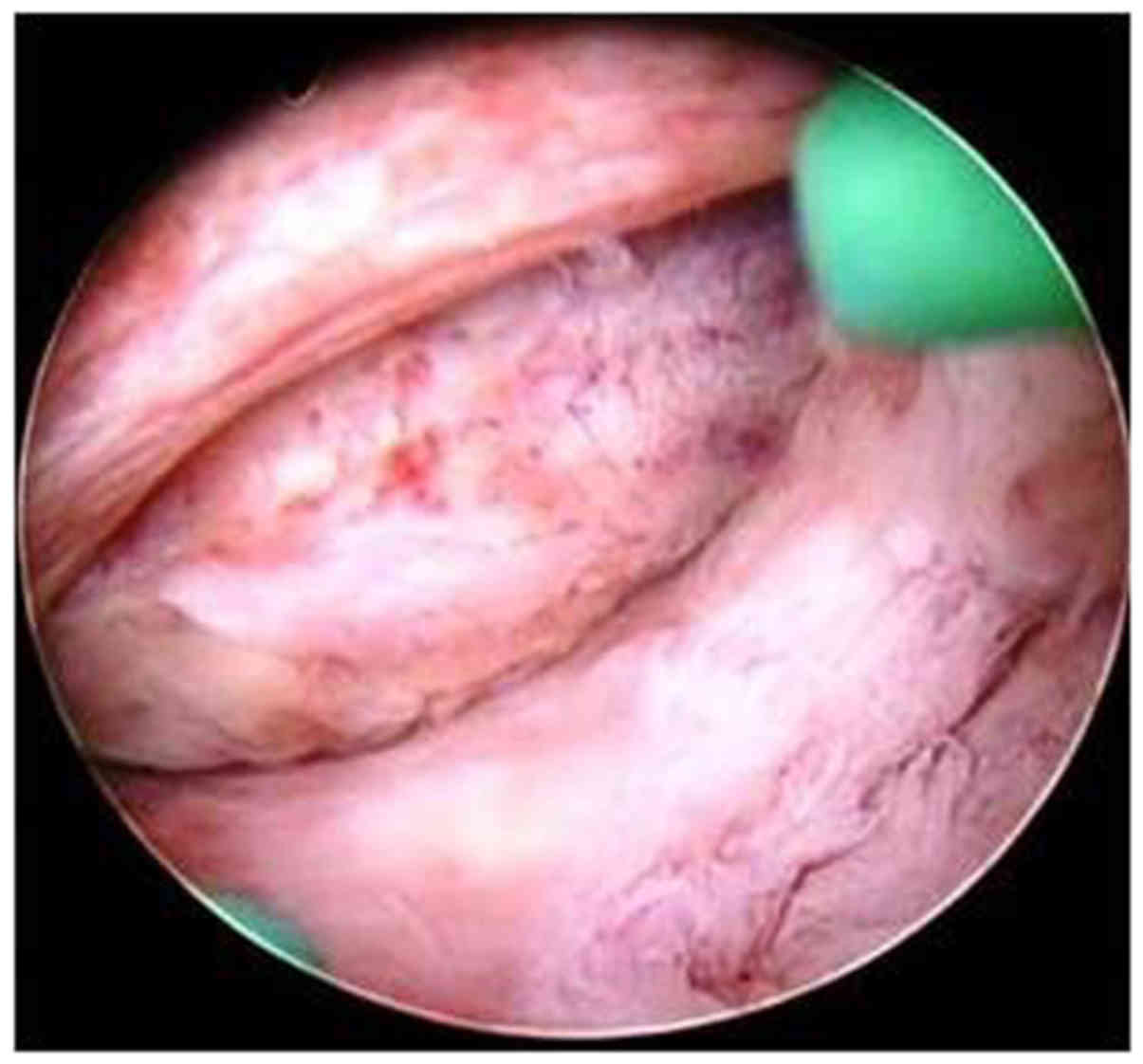
1). A hysteroscopic examination revealed an endometrial polyp
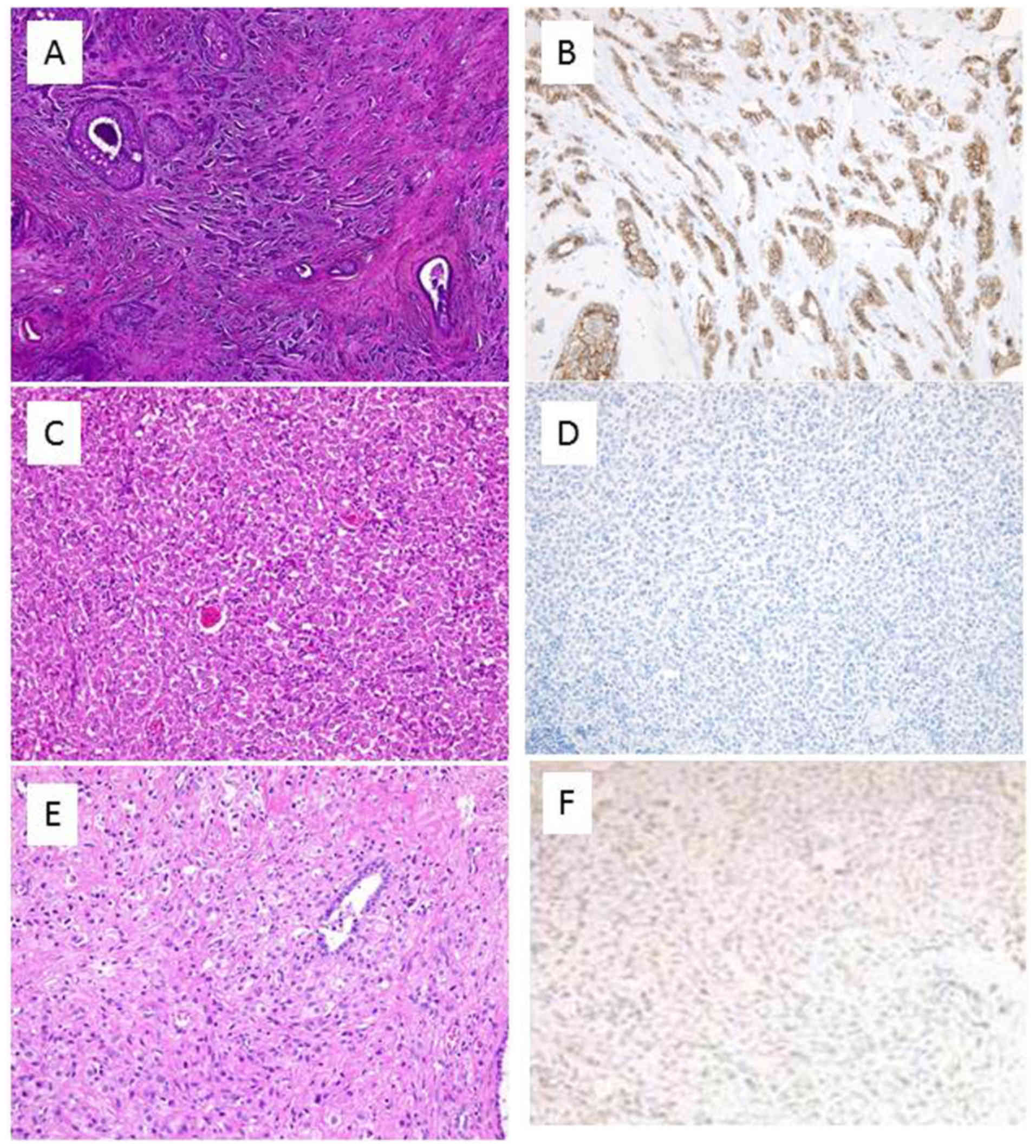
in the uterine cavity, which was resected (Fig. 2). A pathological examination,
including hematoxylin-eosin staining and immunohistochemical
staining, was performed (Fig. 3). The
acquisition of tumor tissues of the patients was approved by the
Shimane University Institutional Review Board. Hematoxylin and
eosin revealed the absence of solid, alveolar, papillary, or
gland-forming units. The tumor cells were arranged in slender
linear strands, one to two cells in thickness. The tumor cells may
have been dispersed in an irregular fashion in a densely fibrotic
stroma. Results of immunohistochemical staining for estrogen
receptor, progesterone receptor, and HER2 were positive, whereas
those for E-cadherin were negative. The morphology, along with the
immunohistochemical findings and the clinical history, supported
the diagnosis of lobular breast carcinoma metastatic to the
endometrial polyp.
A positron emission tomography/computed tomography
(PET-CT) examination showed slightly increased uptake in the myoma.
The standardized uptake value (SUV) on the PET was 9 in the early
phase and 11 in the late phage. Multiple reports suggest that mild
or moderate uptake of 18F-fludeoxyglucose is often
observed in benign uterine leiomyoma and should not be confused
with malignant accumulation, and our experience is consistent with
this observation. Therefore, the tumor was assumed to be benign,
and a laparoscopic hysterectomy was planned. However, because of
the large size of the uterus and copious adhesions between the
ovary, uterus, and rectum, the procedure was changed to an
abdominal hysterectomy. The patient underwent total abdominal
hysterectomy, bilateral salpingo-oophorectomy, and partial
colectomy. Interestingly, the uterine leiomyoma and cervix shared
the same histopathologic features as the primary lobular carcinoma
of the breast, indicating that metastatic tumor arose from the
original breast carcinoma after a 9-year interval. At the time of
this report, the patient is alive and receiving aromatase inhibitor
therapy.
Discussion
Metastases to the female genital tract from
extragenital cancers are less common than metastases from genital
tract cancers and most often affect the ovaries, with the breast
and gastrointestinal tract being the most common sites of the
primary tumor (2). The ovaries are
often first in the path of spread of malignant cells. They provide
an optimal environment for implantation of malignant cells, because
they are very vascular with a well-developed lymph network.
Additionally, the stroma of ovaries has a favorable pH and oxygen
pressure (6). On the other hand, the
other female genital tract organs, including the uterus, seem
resistant to metastasis. Mazur et al (1) reported that, among 149 metastatic tumors
to the female genital tract from extragenital primaries, the ovary
and vagina were the most frequent locations of metastases (75.8 and
13.4%, respectively), while only 8.1% were to the uterus (4.7% to
the endometrium, 3.4% to the cervix). Breast was the second-most
common primary site after gastrointestinal tumors; of 52 breast
cancer cases metastatic to the gynecologic organs, ovaries were
affected in 88.5% cases, vagina in 5.8%, endometrium in 3.8%, vulva
in 1.9% and none to the cervix (1).
Metastases to the uterus from extragenital cancers
are significantly rarer than metastases to the ovaries. Piura et
al (7) reported 198 cases of
extragenital metastases to the uterus, 112 of which originated from
primary breast carcinoma. However, reports of breast cancer
metastasis to uterine leiomyoma were limited. Leiomyoma of the
uterus is the most common benign tumor in women, and it can be
found in 20% of women at autopsy (8).
The low incidence of cancer metastatic to uterine leiomyoma may be
explained by the lack of routine autopsy. Kondo et al
(9) described presenting signs and
symptoms that may result from metastasis to a uterine leiomyoma in
13 cases, including abnormal bleeding in 6 cases (6/13, 46.2%),
enlargement of the uterus in 4 cases, and no symptoms in 3 cases.
In view of these observations, abnormal uterine bleeding may be a
characteristic of a patient with metastasis to a uterine leiomyoma.
Our review of the literature regarding metastasis of a carcinoma to
a uterine leiomyoma is summarized in Table I. Reviewing the histological types of
breast cancer in these reports, ductal carcinoma comprised 61.55%
(8/13) and lobular carcinoma comprised 38.4% (5/13) of metastases
to uterine leiomyoma. In our case, the patient was diagnosed with
both ductal and lobular breast carcinoma, but only lobular
carcinoma metastasized to the uterine leiomyoma, and abnormal
uterine bleeding was the first sign of metastasis.
 | Table I.Cases of resected breast cancer
metastases to uterine leiomyoma. |
Table I.
Cases of resected breast cancer
metastases to uterine leiomyoma.
| Case no. | Author's | Primary
histology | Residual
metastasis | Hormonal
receptor | Postoperative
therapy | Prognosis | (Refs.) |
|---|
| 1 | Di Bonito et
al | Lobular
carcinoma | Ovary and bone | Unknown | Unknown | Died, 5 months | (5) |
| 2 | Sugiyama et
al | Ductal carcinoma | AxLN and bone | Unknown | Unknown | Died, 14 months | (8) |
| 3 | Charvolin et
al | Ductal carcinoma | Nil | ER(+), PR(−) | C and E | Alive, 2 years | (16) |
| 4 | Uner et
al | Ductal carcinoma | AxLN and bone | ER(+), PR(−) | Unknown | Died, 4 months | (17) |
| 5 | Liebmann et
al | Lobular
carcinoma | Unknown | Unknown | Unknown | Unknown | (18) |
| 6 | Minelli et
al | Ductal
carcinoma | Bone and brain | ER(+), PR(+) | C and R | Died, 1 year | (19) |
| 7 | Afriat et
al | Lobular
carcinoma | AxLN | Unknown | C and E | Alive, 4 years | (20) |
| 8 | Beattie et
al | Ductal
carcinoma | AxLN and bone | Unknown | C | Unknown | (21) |
| 9 | Spiro | Ductal
carcinoma | AxLN and
pleura | Unknown | Unknown | Unknown | (22) |
| 10 | Spiro | Lobular
carcinoma | Liver | Unknown | C | Died, 1 year | (22) |
| 11 | Banooni et
al | Lobular
carcinoma | AxLN and bone | Unknown | None | Unknown | (23) |
| 12 | Birdsall et
al | Ductal
carcinoma | AxLN | Unknown | None | Alive, 10
months | (24) |
| 13 | Weingold et
al | Ductal
carcinoma | Bone | Unknown | Unknown | Unknown | (25) |
| 14 | Current case | Ductal and lobular
carcinoma | lymph node | ER(+), PR(+)
HER2(2+) | C, R, and E | Alive |
|
Most extragenital metastases to the cervix arise
from primary tumors of the gastrointestinal tract (1). Other primary sites include the lung,
pancreas, melanoma, urethra, and breast. Breast cancer often
metastasizes to the ovary, but rarely to the cervix. Possible
explanations for this rarity include the small size of the cervix,
its reduced blood flow and distal circulation, and the presence of
abundant fibrous tissue, which make the uterine cervix unfavorable
for the propagation of malignant cells (10). Yazigi et al (11) summarized the first 24 cases in the
literature of breast metastasis to the uterine cervix from his
series and previous authors in 1988. Two subsequent cases were
reported by Piura et al (7),
and Kennebeck and Alagoz (12).
Yazigi drew some general conclusions of the patients reviewed. More
than two-thirds had vaginal bleeding as a presenting symptom, and
greater than 60% had no evidence of disease on examination. Thus,
the metastasis would have been missed if complete evaluations had
not been performed, including Pap smear, colposcopy, and biopsy. In
our case, the patient had irregular vaginal bleeding, and her
cervical Pap smear was normal. In most cases, cervical metastasis
of breast cancer is a manifestation of widespread disease. In
67–89% of the reported cases, distant metastases of other sites
were present at diagnosis of cervical metastasis (12,13). The
response of the cervix to metastatic disease is fibrous
proliferation and an inflammatory cellular reaction, which may
explain the clinical finding of an expanded, indurated cervix
(2). After reviewing the literature,
8 cases (including our case) of metastatic breast carcinoma to the
cervix are presented in Table II. Of
these 8 cases, 3 (37.5%) had ductal carcinoma and 5 (62.5%) had
lobular carcinoma.
| Table II.Reported cases of breast cancer with
synchronous metastasis to the uterine cervix. |
Table II.
Reported cases of breast cancer with
synchronous metastasis to the uterine cervix.
| Case no. | Author's | Patient no. | Age (yr) | Clinical
presentation | Pap | Initial
impression | Primary
histology | Treatment | Survival | (Refs.) |
|---|
| 1 | Hepp et
al | 1 | 55 | Abdominal pain | NP | Cervical tumor | Lobular
carcinoma | Mastectomy
chemotherapy loop excision of cervical tumor | NM | (13) |
| 2 | Song | 2 | 45 | AVB | + | Cervical
cancer | Ductal
carcinoma | Radiation | AAR (6 months) | (26) |
|
|
| 3 | 49 | AVB | − | Cervical
cancer | Ductal
carcinoma | None | AAR (4 months) |
|
| 3 | Limoine et
al | 4 | 39 | AVB | NP | Cervical
cancer | Ductal
carcinoma | NM | 6 months | (27) |
| 4 | Fiorella et
al | 5 | 54 | AVB | + | Endometrial
cancer | Signet ring
cell | None | 6 months | (28) |
| 5 | Bogliolo et
al | 6 | 78 | none | − | Cervical
cancer | Lobular
carcinoma | Quadrantectomy
radiation (breast) chemotherapy | AAR (2.5
years) | (29) |
| 6 | D'souza et
al | 7 | 44 | AVB | + | Cervical
cancer | Lobular
carcinoma | NM | NM | (30) |
| 7 | Horikawa et
al | 8 | 52 | Abdominal
discomfort | − | Leiomyoma | Lobular
carcinoma | Hysterectomy
mastectomy chemotherapy | AAR (7 years) | (31) |
| 8 | Current case | 9 | 58 | AVB | − | Endometrial
polyp | Ductal and lobular
carcinoma | Radiation
chemotherapy hormone therapy | Alive |
|
Endometrial metastasis from a breast cancer is also
uncommon. Kumar and Hart (2) found 2
of 63 cases (3.8%) and Mazur et al (1) found 7 of 149 cases (4.7%) with
metastases to the endometrium. Polyps are the most common benign
lesion in the endometrium, and metastasis to a polyp is
exceptional. Abrams et al (4)
described 15 cases of breast cancer metastatic to endometrial
polyps. Of them, 7 patients had lobular breast cancer, 7 had ductal
adenocarcinoma, and 1 had an apocrine type. Ductal carcinoma
accounts for approximately 70–75% of all breast cancers, while
lobular carcinoma only accounts for 5–20%. Despite its lower
incidence among breast cancers, lobular carcinoma is the most
frequent histologic type that metastasizes to the female genital
tract, being found in more than 80% of all cases. In our case, the
patient was diagnosed invasive ductal carcinoma in the breast;
lobular and ductal carcinoma both were found together in the lymph
node, but histological examination of the endometrial polyp
identified only metastatic lobular carcinoma. Thus, our study
supports the observation that the metastatic potential of lobular
carcinoma for gynecologic organs is higher than that of ductal
carcinoma. After analyzing 261 cases of breast cancer, Lamovec and
Bracko concluded that lobular carcinoma spreads more frequently to
gynecologic organs than ductal carcinoma does (15). This may be explained by the more
frequent loss of the adhesive molecule E-cadherin in lobular
carcinoma. We believe that a similar phenomenon might have taken
place in our patient. A summary of all reported cases to date with
metastatic carcinoma to an endometrial polyp is presented in
Table III.
| Table III.Summary of reported cases of breast
cancer metastases to endometrial polyp. |
Table III.
Summary of reported cases of breast
cancer metastases to endometrial polyp.
| Case no. | Author's | Age | Histologic type
primary tumor | Lymph node
metastasis | Clinical
symptom | Maximal diameter
polyp (cm) | Treatment
procedure | (Refs.) |
|---|
| 1 | Kennebeck et
al | 71 | Ductal | Yes | No | NM | Palliative
RT/CT | (12) |
| 2 | Hooker et
al | 83 | Lobular | Yes | Vaginal
bleeding | 3.5 | Polyp
resection | (14) |
| 3 | Sullivan et
al | 83 | Ductal | Yes | No | 11.5 | TAH+BSO | (32) |
| 4 | Corley et
al | 58 | Ductal | Yes | Vaginal
bleeding | NM | TAH+BSO | (33) |
| 5 | Aranda et
al | 76 | Lobular | No | No | 9 | TAH+BSO | (34) |
| 6 | Martinez et
al | 78 | Lobular | Yes | Vaginal
bleeding | 3.3 | TAH+BSO | (35) |
| 7 | Martinez et
al | 58 | Ductal | Yes | Vaginal
bleeding | NM | TAH+BSO | (35) |
| 8 | Lambot et
al | 70 | Apocrine | Yes | Vaginal
bleeding | 1.5 | TAH+BSO | (36) |
| 9 | Horn et
al | 73 | Ductal | No | No | 8 | TAH+BSO | (37) |
| 10 | Alvarez et
al | 69 | Lobular | Yes | Vaginal
bleeding | 1.5 | None d | (38) |
| 11 | Houghton et
al | 62 | Lobular | Yes | Vaginal
bleeding | 3 | Polyp
resection | (39) |
| 12 | Houghton et
al | 92 | Lobular | Unknown | Vaginal
bleeding | 3 | Polyp
resection | (39) |
| 13 | Al-brahim et
al | 53 | Lobular | Yes | Vaginal
bleeding | 7 | Polyp
resection | (40) |
| 14 | Acikalin et
al | 58 | Ductal | Yes | No | 5 | TAH+BSO | (41) |
| 15 | Manipadam et
al | 70 | Lobular | Yes | Vaginal
bleeding | 3 | Polyp
resection | (42) |
| 16 | Aydin et
al | 60 | Ductal | Unknown | Vaginal
bleeding | 6.5 | CT, ANA | (43) |
| 17 | Current case | 58 | Ductal and
lobular | Yes | Vaginal
bleeding | 3.2 | Polyp
resection |
|
Uterine metastases from extragenital cancers are
significantly rarer than metastases to the ovary, and when they
occur, they are usually secondary to lymphatic spread from
preceding ovarian metastases. Metastases restricted to the uterus,
without involvement of the ovaries, are indeed very rare and can be
explained by hematogenous spread.
In our case, lobular breast carcinoma metastasized
to a uterine leiomyoma, the cervix, and an endometrial polyp
concurrently, which is exceedingly rare. Although the ovary and
vagina are the most common locations of metastasis, the entire
organ system is at risk for metastatic disease. Therefore, abnormal
uterine bleeding in patients with a history of breast carcinoma
should always alert the physician to consider the diagnosis of
metastatic spread to the genital tract. Gynecologists who are
planning a laparoscopic operation for the patient with a history of
lobular breast cancer should consider abdominal dissection rather
than laparoscopy, even if the tumor is thought to be benign. If
lobular carcinoma remains dormant in the myoma or other
gynecological organs, as our case, and the surgeon misses any
tissue during the operation, residual disease may spread elsewhere
in the peritoneal cavity. Before surgery, the use of PET-CT may be
beneficial for identifying an unanticipated mass.
References
|
1
|
Mazur MT, Hsuesh S and Gersell DJ:
Metastases to the female genital tract. Analysis of 325 cases.
Cancer. 53:1978–1984. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kumar NB and Hart WR: Metastases to the
uterine corpus from extragenital cancer. A clinicopathological
study of 63 cases. Cancer. 50:2163–2169. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Charache H: Metastatic carcinoma in the
uterus. AM J Surg. 53:152–157. 1941. View Article : Google Scholar
|
|
4
|
Abrams HL, Spiro R and Goldstein N:
Metastases in carcinoma: Analysis of 1000 autopside cases. Cancer.
3:74–85. 1950. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Di Bonito L, Patriarca S and Alberico S:
Breast carcinoma metastasizing to the uterus. Eur J Gynaecol Oncol.
6:211–217. 1985.PubMed/NCBI
|
|
6
|
Perisić D, Jancić S, Kalinović D and
Cekerevac M: Metastasis of lobular breast carcinoma to the cervix.
J Obstet Gynaecol Res. 33:578–580. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Piura B, Yanai-Inbar I, Rabinovich A,
Zalmanov S and Goldstein J: Abnormal uterine bleeding as a
presenting sign of metastases to the uterine corpus, cervix and
vagina in a breast cancer patient on tamoxifen therapy. Eur J
Obstet Gynecol Reprod Biol. 83:57–61. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sugiyama T, Toyoda N, Nose J, Kihira N,
Ando Y and Ishihara A: Breast cancer metastatic to uterine
leiomyoma: A case report. J Obstet Gynaecol (Tokyo 1995).
21:349–355. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kondo NI, Yoshida S, Kajiyama H, Nagasaka
T and Uematsu T: Metastasis of breast cancer to a uterine
leiomyoma. Breast Cancer. 16:157–161. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pérez-Montiel D, Serrano-Olvera A, Salazar
LC, Cetina-Pérez L, Candelaria M, Coronel J, Montalvo LA and de
León DC: Adenocarcinoma metastatic to the uterine cervix: A case
series. J Obstet Gynaecol Res. 38:541–549. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yazigi R, Sandstad R and Munoz A: Breast
cancer metastasizing to the uterine cervix. Cancer. 61:2558–2560.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kennebeck C and Alagoz T: Signet ring
breast carcinoma metastases limited to the endometrium and cervix.
Gynecol Oncol. 71:461–464. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hepp HH, Hoos A, Leppien G and Wallwiener
D: Breast cancer metastatic to the uterine cervix: Analysis of a
rare event. Cancer Invest. 17:468–473. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hooker AB, Radder CM, van de Wiel B and
Geenen MM: Metastasis from breast cancer to an endometrial polyp;
treatment options and follow-up. Report of a case and review of the
literature. Eur J Gynaec Oncol. 32:228–230. 2011.
|
|
15
|
Lamovec J and Bracko M: Metastatic pattern
of infiltrating lobular carcinoma of the breast: An autopsy study.
J Surg Oncol. 48:28–33. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Charvolin JY, Salmon RJ, Pecking A and
Mareschal V: Positron emission tomography detection of breast
cancer metastasis to the uterus. Obstet Gynecol. 99:915–917. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Uner A, Tiras MB, Kilic D, Dursun A and
Dilek U: Uterine lipoleiomyoma containing metastatic breast
carcinoma: A case with two unusual pathologies. Eur J Obstet
Gynecol Reprod Biol. 106:76–78. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liebmann RD, Jones KD, Hamid R and Lapsley
M: Fortuitous diagnosis in a uterine leiomyoma of metastatic
lobular carcinoma of the breast. Histopathology. 32:577–578. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Minelli L, Romagnolo C, Giambanco L and
Bongiorno E: Uterine leiomyoma metastasis as a first sign of breast
cancer. J Am Assoc Gynecol Laparosc. 5:213–215. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Afriat R, Lenain H, Vuagnat C, Michenet P,
Luthier F, Maitre F and Grossetti D: Metastasis of breast cancer to
a uterine leiomyoma. J Gynecol Obstet Biol Rep (Paris). 22:243–244.
1993.(In French).
|
|
21
|
Beattie GJ, Duncan AJ, Paterson AJ,
Williams AR and Geirsson RT: Breast carcinoma metastatic to uterine
leiomyoma. Gynecol Oncol. 51:255–257. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Spiro RK: Breast cancer metastatic to
uterine leiomyoma. J Med Soc N J. 76:285–287. 1979.PubMed/NCBI
|
|
23
|
Banooni F, Labes J and Goodman PA: Uterine
leiomyoma containing metastatic breast carcinoma. Am J Obstet
Gynecol. 111:427–430. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Birdsall CJ, Dockerty MB and Pratt JH:
Mammary carcinoma metastasis to uterine myoma. Obstet Gynecol.
23:229–231. 1964.PubMed/NCBI
|
|
25
|
Weingold AB and Boltuch SM: Extragenital
metastases to the uterus. Am J Obstet Gynecol. 82:1267–1272. 1961.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Song J: Metastatic carcinoma of the
uterine cervix from primary breast cancer. JAMA. 184:498–500. 1963.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Limoine NR and Hall PA: Epithelial tumors
metastatic to the uterine cervix. A study of 33 cases and review of
the literature. Cancer. 57:2002–2005. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fiorella RM, Beckwith LG, Miller LK and
Kragel PJ: Metastatic signet ring carcinoma of the breast as a
source of positive cervicovaginal cytology. A case report. Acta
Cytol. 37:948–952. 1993.PubMed/NCBI
|
|
29
|
Bogliolo S, Morotti M, Menada Valenzano M,
Fulcheri E, Musizzano Y and Casabona F: Breast cancer with
synchronous massive metastasis in the uterine cervix: A case report
and review of the literature. Arch Gynecol Obstet. 281:769–773.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
D'souza MM, Sharma RS, Tripathi M, Saw SK,
Anad A, Singh D and Mondal A: Cervical and uterine metastasis from
carcinoma of breast diagnosed by PET/CT. An unusual presentation.
Clin Nucl Med. 35:820–823. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Horikawa M, Mori Y, Nagai S, Tanaka S,
Saito S and Okamoto T: Metastatic breast cancer to the uterine
cervix mimicking a giant cervical leiomyoma. J Med Sci. 74:347–351.
2012.
|
|
32
|
Sullivan LG, Sullivan JL and Fairey WF:
Breast carcinoma metastatic to endometrial polyps. Gynecol Oncol.
39:96–98. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Corley D, Rowe J, Curtis MT, Hogan WM,
Noumoff JS and Livolsi VA: Postmenopausal bleeding from unusual
endometrial polyps in women on chronic tamoxifen therapy. Obstet
Gynecol. 79:111–116. 1992.PubMed/NCBI
|
|
34
|
Aranda FI, Laforga JB and Martinez MA:
Metastasis from breast lobular carcinoma to an endometrial polyps:
Reports of a case with immunohistochemical study. Acta Obstet
Gynecol Scand. 72:585–587. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Martinez-Montero I, Dominguez-Cunchillos
F, Muruzabal JC, de Míguel C, Recari E and Ezcurdia M: Uterine
metastases from breast cancer. Acta Obstet Gynecol Scand.
78:165–167. 1999.PubMed/NCBI
|
|
36
|
Lambot MA, Eddafali B, Simon P, Fayt I and
Noël JC: Metastasis from apocrine carcinoma of the breast to an
endometrial polyp. Virchows Arch. 438:517–518. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Horn LC, Einenkel J and Baier D:
Endometrial metastasis from breast cancer in a patient receiving
tamoxifen therapy. Gynecol Obstet Invest. 50:136–138. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Alvarez C, Ortiz-Rey JA, Estévez F,
Estevez F and de la Fuente A: Metastatic lobular breast carcinoma
to an endometrial polyps diagnosed by hysteroscopic biopsy. Obstet
Gynecol. 102:1149–1151. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Houghton JP, Ioffe OB, Silverberg SG,
McGrady B and McCluggaga WG: Metastatic breast lobular carcinoma
involving tamoxifen-associated endometrial polyps: Report of two
cases and review of tamoxifen-associated polypoid uterine lesions.
Mod Pathol. 16:395–398. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Al-brahim N and Elavathil LJ: Metastatic
breast lobular carcinoma to tamoxifen-associated endometrial polyp:
Case report and literature review. Ann Diagn Pathol. 9:166–168.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Acikalin MF, Oner U, Tekin B, Yakuz E and
Cengiz O: Metastastasis from breast carcinoma to a
tamoxifen-related endometrial polyp. Gynecol Oncol. 97:946–948.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Manipadam MT, Walter NM and Selvamnani B:
Lobular carcinoma metastasis to endometrial polyp unrelated to
tamoxifen. Report of a case and review of the literature. APMIS.
116:538–540. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Aydin O, Bagic P, Akyildiz EU, Ozguroglu M
and Ilvan S: Metastasis from breast carcinoma to endometrial polyp.
Eur J Gynaecol Oncol. 29:666–668. 2008.PubMed/NCBI
|