Introduction
According to the current estimates of the American
Cancer Society, laryngeal cancer is one of the most common types of
cancer of the upper aerodigestive tract (1). It was estimated that ~13,360 incident
cases of laryngeal cancer and 3,660 mortalities would occur by 2017
in the United States (2). Changes in
diagnostic and therapeutic approaches have increased the rates of
larynx preservation and survival (3).
However, the 5-year survival rate of patients with advanced-stage
laryngeal cancer, particularly stage IV patients, remains low
globally, including China (4,5). In addition, patients undergoing
aggressive treatments experience a significant reduction in quality
of life, including speech, eating, social disruption and aesthetics
(4). Therefore, prognostic evaluation
and treatment decisions based on clinical pathological features
should be implemented according to novel risk stratification, which
is based on novel markers for patients with laryngeal cancer,
including inflammation-based prognostic scores including the
Glasgow Prognostic Score, neutrophil-to-lymphocyte ratio (NLR) and
Prognostic Nutritional Index (6).
The inflammatory response serves a vital role in the
development and progression of a number of solid tumors.
Neutrophils and platelets supply the required bioactive molecules,
including angiogenic, epithelial, and stromal growth factors and
matrix-remodeling enzymes, for neoplastic progression (7,8). In
addition, conditions that induce compromised cell-mediated
immunity, such as lymphocytopenia and an impaired T-lymphocytic
response, reflect imbalances in the innate and adaptive immune
systems, which compromises effective host-tumor immune responses
(9,10). Therefore, the combination of
neutrophils, platelets and lymphocytes, as markers of host
inflammation, has been identified to be an independent prognostic
factor in different malignancies (11,12). An
increased NLR or platelet-to-lymphocyte ratio (PLR) is associated
with poor outcomes in various tumors, including colorectal, primary
liver, lung, urinary, cervical, oropharyngeal squamous cell or
advanced esophageal cancer (13–15).
Furthermore, serum albumin has been identified to be a sensitive
and reliable marker of systemic inflammation in patients with
cancer (16). However, the
application and credibility of albumin level as a marker is limited
owing to its interference by numerous factors, including the
peritoneal burden of vascular endothelial growth factor (17). The albumin-to-globulin ratio (AGR),
which takes into account the level of albumin and globulin,
reflects the body nutritional status (18,19). AGR
was also identified to be an effective prognostic factor for
advanced malignancies, including non-small cell lung cancer
(20). Risk stratification based on
these factors and clinical pathological features may underlie the
optimal treatment decision-making and prognostic evaluation.
However, limited data are available on the
prognostic role of these indices in patients with laryngeal
squamous cancer (21,22). Rassouli et al (21) demonstrated that systemic inflammatory
markers NLR and PLR were independent prognostic factors of head and
neck squamous cell carcinoma. However, this was a heterogeneous
study that included only a small number of patients with laryngeal
cancer. Kum et al (22)
indicated that the mean NLR of patients with precancerous laryngeal
lesion and laryngeal squamous cell carcinoma was significantly
increased compared with patients with benign laryngeal lesion and
without prognostic evaluation. At present, there is a lack of data
on the evaluation of prognosis with these readily available and
inexpensive biomarkers for patients with laryngeal squamous cancer.
The present study evaluated the association between these indices
and survival outcomes of patients with laryngeal squamous cell
cancer.
Materials and methods
Patients and data collection
Patients identified with laryngeal cancer confirmed
by pathological diagnosis at the West China Hospital (Chengdu,
China) between September 2008 and September 2013 were enrolled in
the retrospective study. All the cases were scheduled for regular
follow-up visits (1, 2, 3, 6, 12, 24, 36 and 60 months
post-operation) at an outpatient department in West China Hospital
(Chengdu, China). Patients absent from regular follow-up visits
received follow-up by telephone, and the end-point of these
patients were collected by the Disease Surveillance Point System in
the Sichuan Province Center for Disease Control and Prevention. The
current status (succumbed, recurrent or in remission), date of
recurrence, date of mortality, and associated cause of recurrence
or mortality were recorded.
The inclusion criteria were as follows: i)
Pathological diagnosis of squamous cell cancer; and ii) routine
complete blood counts (CBCs) tests with differential counting and
serum biochemical analysis. The exclusion criteria were: i)
Presence of infection, connective tissue diseases or any other
disease affecting blood cells; ii) patients who discontinued
treatment or were treated outside of West China Hospital; iii)
absence of CBC and serum biochemical analysis prior to treatment;
iv) patients who succumbed prior to discharge from hospital
following initial treatment; v) presence of symptoms and signs of
hepatic function damage that may affect AGR; and vi) and presence
of other tumors. The present study was approved by the
Institutional Ethics Committee of the West China Hospital, Sichuan
University (Chengdu, China), and written informed consent were
obtained.
A total of 654 patients were enrolled for the
present study, and 85 patients were enrolled for cytokine testing
in tumor tissues. Patient characteristics such as age, sex,
American Joint Committee on Cancer histologic grade (23), pathological diagnosis [including Tumor
Node Metastasis (TNM) Classification of Malignant Tumors staging]
(23), tumor location, date of
diagnosis and treatment were recorded from the electronic hospital
information system (HIS). In addition, hospital examination
included CBC with differential counting, and several biochemical
indices such as globulin and albumin were also recorded from HIS at
the West China Hospital.
Freshly obtained laryngeal cancer tissue specimens,
obtained during the operation, were processed and assayed for
interleukin (IL)-6 and IL-8 levels. Briefly, the samples were
homogenized and centrifuged at 3,000 × g for 10 min at 4°C, and the
supernatants were stored at −80°C until analysis. The samples were
assayed for IL-6 (cat. no. D6050; R&D Systems China Co., Ltd.,
Shanghai, China) and IL-8 (cat. no. D8000C; R&D Systems China
Co., Ltd.) using commercially available ELISA kits (R&D Systems
China Co., Ltd.), according to the manufacturer's protocol.
NLR and PLR ratio
NLR was calculated by dividing the number of
neutrophils by the number of lymphocytes obtained from the CBCs.
PLR was calculated by dividing the number of platelets by the
number of lymphocytes, and AGR was calculated by dividing the level
of albumin by the level of globulin obtained from biochemical
analysis of the blood. All three ratios were obtained from the CBCs
prior to the initiation of treatment. Progression-free survival
(PFS) and overall survival (OS) are presented in months.
A review of the literature revealed heterogeneity in
the NLR, PLR and AGR cutoff points used in various malignances
(14,24), including head and neck squamous cancer
(21,22). Patients were grouped according to the
cut-off points for NLR, PLR, AGR and age. The classification and
regression tree (CART) algorithm was used to produce predictive
rules and improve the accuracy of survival prediction (25–27).
Statistical analysis
All parameters including CBCs with differential
counting, biochemical indices, and NLR, PLR and AGR were compared
among different clinical characteristics by Kruskal-Wallis test.
CART analysis was performed in SPSS (version no. 17.0; SPSS, Inc.,
Chicago, IL, USA) to generate predictive rules and optimal cutoff
points. Survival outcomes were compared using Kaplan-Meier analyses
with log-rank tests. All the clinical pathological features and NLR
were included in the univariate analysis, and then factors with
significance values of P<0.10 in a univariate analysis were
included in the multivariable analyses using Cox's proportional
hazards model to determine the hazard ratio of survival. The
differences in the level of cytokines between groups with different
NLR values were compared using the Mann-Whitney test, and the
correlation between cytokines with NLR was analyzed using Pearson's
correlation test. For statistical analysis, Statistical Package for
Social Sciences (version 18.0; SPSS, Inc.) was used. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patient characteristics
Of the total 654 patients enrolled in the present
study, 70 patients (70/654; 10.7%) were not followed up for overall
survival (median follow-up, 36 months; interquartile range (IQR),
28–46 months). A total of 49 patients (7.5%) failed to receive
follow-up for PFS at a median follow-up of 33 months (IQR, 18–41
months). Overall, 200 patients (200/654; 30.6%) exhibited disease
progression, and 128 patients (128/654; 19.6%) succumbed to cancer.
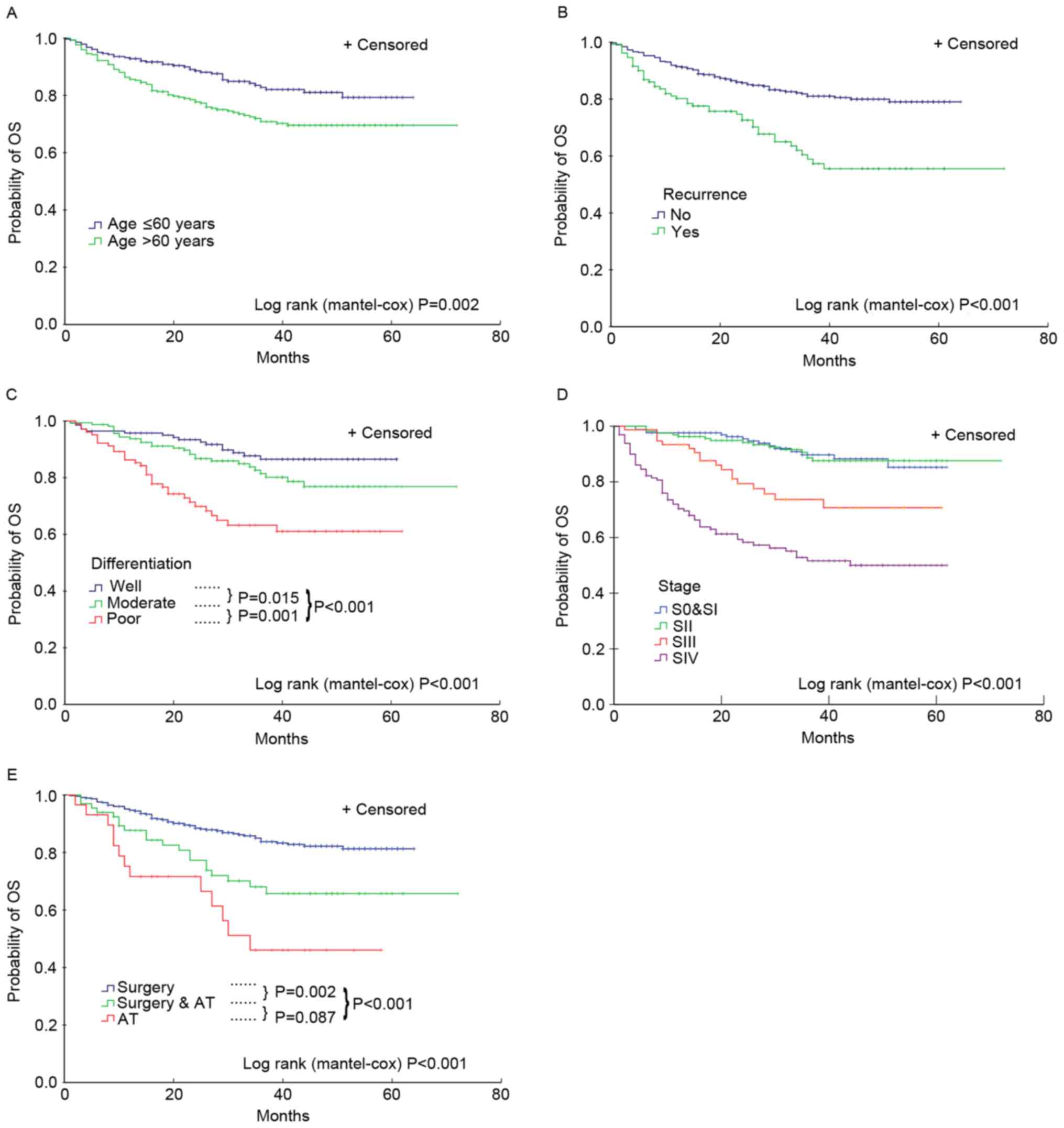
The 5-year survival rates were 85, 81, 70 and 51% for patients with
laryngeal cancer at TNM stages I, II, III and IV, respectively.
Additionally, the 3-year survival rate was 87%, and the survival
rate of glottic carcinoma was increased significantly compared with
other types of cancer in the larynx, which were 87 and 53%
(P<0.05), respectively. Finally, factors, including age >60
years, non-glottic carcinoma, high histologic grade, high staging,
extensive treatment and recurrence were associated with increased
probability of overall mortality (Fig.
1) and disease progression (data not shown).
Association of blood and biochemical
parameters with clinical characteristics of patients with laryngeal
cancer
There were no differences observed among the
histologic grades for the median of whole white blood cell (WBC)
and various differential counts from CBC analysis, including
hemoglobin, globulin and albumin levels, and NLR, PLR and AGR. All
increased parameters (including WBC count and various differential
counts from CBC analysis, including hemoglobin, globulin and
albumin levels, and NLR, PLR and AGR) were associated with the
higher T classification and TNM stage (P<0.01). All increased
parameters, with the exception of WBC, lymphocyte and monocyte
counts, were associated with higher N classifications (P<0.01;
Table I).
 | Table I.Blood and biochemical parameters of
patients with laryngeal squamous cell cancer. |
Table I.
Blood and biochemical parameters of
patients with laryngeal squamous cell cancer.
| Parameters
(IQR) | WBC
(×109/l) (IQR) | Neutrophil
(×109/l) (IQR) | Lymphocyte
(×109/l) (IQR) | Monocyte
(×109/l) (IQR) | Platelet
(×109/l) (IQR) | Hb (g/l) (IQR) | Globulin level
(g/l) (IQR) | Albumin level (g/l)
(IQR) | NLR (IQR) | PLR (IQR) | GAR (IQR) |
|---|
| Total (n=654) | 6.31
(5.39–7.46) | 3.89
(3.13–4.86) | 1.75
(1.39–2.19) | 0.37
(0.29–0.47) | 162 (127–207) | 145 (135–154) | 26.6
(24.1–29.5) | 43.6 (41–45.6) | 2.18
(1.58–3.10) | 92.4
(67.9–122.8) | 0.48
(0.38–0.63) |
| Histologic
grade |
|
|
|
|
|
|
|
|
|
|
|
| Well
(n=149) | 6.35
(5.38–7.26) | 3.81
(3.08–4.61) | 1.77
(1.45–2.22) | 1.77
(1.45–2.22) | 164 (130–208) | 147 (136–155) | 27.1 (24.1–30) | 43.9
(41.2–46.2) | 2 (1.55–2.81) | 94.1
(72.3–113.6) | 0.61
(0.56–0.68) |
|
Moderately (n=224) | 6.34
(5.43–7.44) | 3.83
(3.05–4.92) | 1.74
(1.39–2.19) | 1.74
(1.39–2.19) | 176 (135–220) | 145 (137–153) | 26.1
(23.5–28.9) | 43.7 (41–45.4) | 2.18
(1.57–3.18) | 101
(70.8–127.1) | 0.61
(0.53–0.68) |
| Poorly
(n=143) | 6.22
(5.23–7.67) | 3.89
(3.15–4.88) | 3.89
(3.15–4.88) | 1.72
(1.35–2.05) | 162 (124–212) | 145 (135–154) | 27 (24.8–29.7) | 42.9
(40.5–45.1) | 2.34
(1.71–3.18) | 93.5
(67.8–129.7) | 0.62
(0.57–0.7) |
|
P-value | 0.916 | 0.754 | 0.346 | 0.519 | 0.246 | 0.37 | 0.061 | 0.121 | 0.128 | 0.154 | 0.143 |
| T stage |
|
|
|
|
|
|
|
|
|
|
|
| T1
(n=186) | 6.21
(5.16–7.05) | 3.65
(2.93–4.42) | 1.81
(1.46–2.31) | 0.36
(0.29–0.44) | 149 (119–183) | 147 (136–155) | 26.4
(23.7–28.7) | 44.3 (41.7–46) | 1.96
(1.43–2.64) | 80.5
(60.7–109.9) | 0.6
(0.53–0.67) |
| T2
(n=213) | 6.11
(5.33–7.04) | 3.69
(2.99–4.33) | 1.82
(1.49–2.18) | 0.35
(0.28–0.46) | 164 (128–204) | 149 (139–156) | 26.1
(23.8–28.4) | 44 (41.7–46) | 1.94
(1.51–2.61) | 88.4
(66.1–115.8) | 0.6
(0.54–0.67) |
| T3
(n=103) | 6.34
(5.43–7.73) | 3.92
(3.24–4.88) | 1.8
(1.38–2.15) | 0.38
(0.29–0.47) | 167 (126–211) | 146 (138–153) | 27.2
(24.6–29.7) | 44.4
(42.2–45.7) | 2.18
(1.75–2.88) | 94.7
(69.3–125.2) | 0.61
(0.55–0.7) |
| T4
(n=136) | 6.97
(5.5–8.62) | 4.53
(3.41–6.22) | 1.57
(1.24–1.99) | 0.42
(0.32–0.55) | 176 (135–226) | 140 (131–150) | 27.9
(24.5–30.5) | 41.9
(39.3–44.3) | 3.01
(1.98–4.29) | 108.5
(80.6–159.1) | 0.66
(0.58–0.75) |
|
P-value | 0.001 | <0.001 | <0.001 | 0.002 | 0.002 | <0.000 | 0.005 | <0.001 | <0.001 | <0.001 | <0.001 |
| N stage |
|
|
|
|
|
|
|
|
|
|
|
| N0
(n=535) | 6.22
(5.38–7.32) | 3.81
(3.05–4.63) | 1.78
(1.43–2.21) | 0.37
(0.3–0.47) | 158 (126–200) | 147 (137–155) | 26.5
(23.8–28.9) | 44 (41.5–45.9) | 2.09
(1.55–2.88) | 88.4
(65.4–117.6) | 0.61
(0.54–0.68) |
| N1
(n=57) | 6.49
(5.07–7.46) | 3.95
(3.07–5.19) | 1.63 (1.3–2) | 0.34
(0.29–0.47) | 189 (141–226) | 140 (130–152) | 27.8
(25.8–30.1) | 41.8
(38.9–44.5) | 2.19
(1.66–3.15) | 104.7
(83.6–139) | 0.66
(0.59–0.73) |
| N2 and
N3 (n=55) | 7.13
(5.47–8.25) | 4.3
(3.52–5.91) | 1.79
(1.32–2.13) | 0.42
(0.33–0.54) | 184 (128–252) | 140 (134–150) | 28.1
(25.3–30.9) | 42.2
(39.5–44.8) | 2.58
(1.82–3.83) | 101.5
(68.3–169) | 0.5
(0.42–0.65) |
|
P-value | 0.056 | 0.011 | 0.092 | 0.061 | 0.003 | 0.004 | 0.001 | <0.001 | 0.006 | <0.001 | <0.001 |
| TNM stage |
|
|
|
|
|
|
|
|
|
|
|
| 0 and I
(n=182) | 6.21
(5.13–7.05) | 3.66
(2.90–4.42) | 1.80
(1.46–2.31) | 0.36
(0.29–0.44) | 149 (119–183) | 147 (137–155) | 26.4
(23.7–28.7) | 44.3
(41.7–46.0) | 1.96
(1.43–2.64) | 81.3
(60.7–109.9) | 0.60
(0.53–0.67) |
| S II
(n=199) | 6.11
(5.34–7.06) | 3.66
(2.99–4.35) | 1.82
(1.49–2.19) | 0.36
(0.30–0.46) | 160 (127–203) | 149 (139–156) | 26.0
(23.8–28.5) | 44.0
(41.9–46.0) | 1.95
(1.51–2.63) | 87.2
(64.2–115.0) | 0.60
(0.54–0.67) |
| S III
(n=104) | 6.22
(5.33–7.31) | 3.83
(3.12–4.64) | 1.80
(1.47–2.14) | 0.37
(0.28–0.47) | 168 (132–217) | 146 (137–152) | 27.0
(24.7–29.4) | 44.1
(41.0–45.5) | 2.16
(1.73–2.70) | 95.2
(70.0–120.5) | 0.62
(0.55–0.70) |
| S IV
(n=164) | 7.11
(5.69–8.62) | 4.65
(3.52–6.25) | 1.58
(1.23–2.06) | 0.42
(0.32–0.54) | 180 (135–227) | 140 (130–150) | 28.0
(14.7–30.5) | 42.0
(39.3–44.5) | 2.94
(1.92–4.37) | 106.5
(79.4–159.4) | 0.66
(0.58–0.76) |
|
P-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
NLR value categorizes patients into
groups with different survival and clinical features
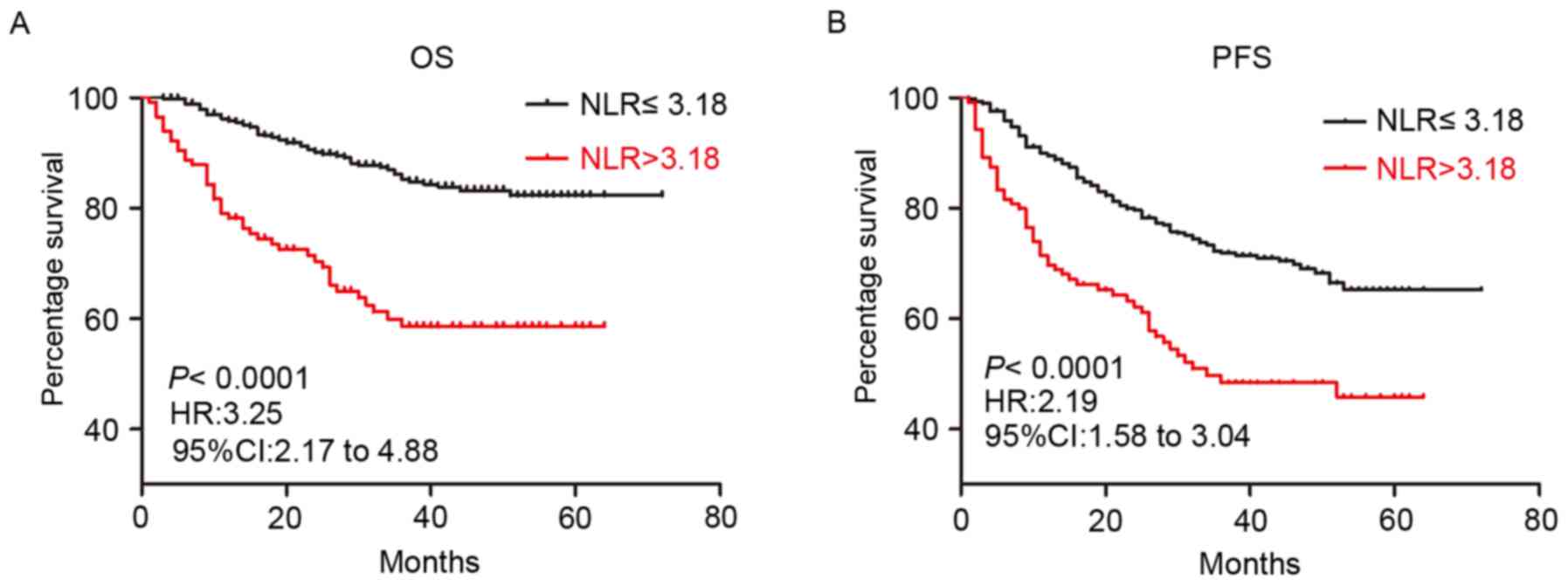
Using the recursive partitioning statistical
approach, with OS status as a dependent variable, while age, NLR,
PLR and AGR were independent variables, only one node with a NLR
value of 3.18 divided patients into different groups. Patients with
a NLR >3.18 exhibited significantly decreased OS and PFS
compared with patients with ≤3.18, as demonstrated by the
Kaplan-Meier survival curve (Fig. 2).
Patients with NLR ≤3.18 exhibited lower probability of overall
mortality compared with patients with NLR >3.18 (3-year OS for
NLR ≤3.18 vs. >3.18, 84.36 vs. 58.58%; log-rank, P<0.001;
Fig. 2A) and disease progression
(3-year PFS for NLR ≤3.18 vs. >3.18, 71.87 vs. 48.41%; log-rank,
P<0.001; Fig. 2B).
There was no significant difference in median age
and histologic grade between patients with NLR below and above the
cutoff value (Table II). The NLR
cutoff value subdivided patients into different proportion of T and
N classification and TNM stage (P<0.001; Table II). Patients with a NLR >3.18
experienced significantly more invasive procedures including
surgery (P<0.001) and neck dissection (P=0.012) (Table II).
| Table II.Patient characteristics. |
Table II.
Patient characteristics.
| A, Patient
characteristics |
|---|
|
|---|
|
|
| NLR |
|---|
|
|
|
|
|---|
|
| Total, (n=654) | ≤3.18 | >3.18 | P-value |
|---|
| Age |
|
|
|
|
|
Median | 61 (54–67) | 60 (54–67) | 62
(54–68) | 0.184 |
| ≤60, n
(%) | 324 (49.5) | 207 (52.1) | 117 (45.5) | 0.098 |
| >60,
n (%) | 330 (50.5) | 210 (47.9) | 141 (54.7) |
|
| Sex |
|
|
|
|
| Female,
n (%) | 17 (2.6) | 8 (1.8) | 9
(3.5) | 0.159 |
| Male, n
(%) | 637 (97.4) | 436 (98.2) | 248 (96.5) |
|
|
| B, Disease
characteristics |
|
|
|
| NLR |
|
|
|
|
|
| Total,
(n=654) | ≤3.18 |
>3.18 | P-value |
| Region, n (%) |
|
|
|
|
| Glottic laryngeal
cancer | 478 (73.1) | 332 (81.9) | 144 (57.8) | <0.001 |
| Histologic
grade |
|
|
|
|
|
Well-differentiated | 149 (28.9) | 105 (32.1) | 44 (23.7) | 0.100 |
|
Moderately differentiated | 224 (43.4) | 138 (42.2) | 83 (44.6) |
|
| Poorly
differentiated | 143 (27.7) | 84 (25.7) | 59 (31.7) |
|
| T stage, n (%) |
|
|
|
|
| pT0,
T1 | 186 (29.2) | 136 (32.9) | 49 (22.4) | <0.001 |
|
pT2 | 213 (33.4) | 159 (38.5) | 54 (24.7) |
|
|
pT3 | 103 (16.1) | 68 (16.5) | 35 (16) |
|
|
pT4 | 136 (21.3) | 50 (12.1) | 81 (37) |
|
| N stage, n (%) |
|
|
|
|
|
pN0 | 535 (82.7) | 357 (85.5) | 176 (78.2) | 0.011 |
|
pN1 | 57 (8.8) | 33 (7.9) | 22 (9.8) |
|
|
pN2 | 49 (7.6) | 24 (5.8) | 24 (10.7) |
|
|
pN3 | 6 (0.9) | 2 (0.5) | 3 (1.3) |
|
| Stage, n (%) |
|
|
|
|
| Early
0 | 31 (4.8) | 20 (4.8) | 11 (4.7) | <0.001 |
| I | 151 (23.3) | 114 (27.3) | 37 (15.9) |
|
| II | 199 (30.7) | 146 (35) | 53 (22.8) |
|
| Late
III | 104 (16) | 71 (10.9) | 33 (14.2) |
|
| IV | 164 (25.3) | 66 (15.8) | 98 (42.2) |
|
|
Recurrence, n (%) | 157 (24) | 81 (20.4) | 76 (29.5) | 0.008 |
|
| C, Treatment
characteristics |
|
|
|
| NLR |
|
|
|
|
|
| Total,
(n=654) | ≤3.18 |
>3.18 | P-value |
|
| Surgery, n (%) |
|
|
|
|
|
Larynscopy | 227 (32.3) | 170 (41) | 66 (28.1) | <0.001 |
| Partial
laryngectomy | 253 (36) | 180 (43.4) | 73 (31.1) |
|
| Total
laryngectomy | 164 (23.3) | 65 (15.7) | 96 (40.9) |
|
| Neck dissection, n
(%) |
|
|
|
|
|
None | 515 (78.7) | 310 (74.9) | 159 (66.2) | 0.012 |
|
Unilateral | 117 (16.6) | 71 (17.1) | 45 (18.8) |
|
|
Bilateral | 71 (10.1) | 33 (8.0) | 36 (15.0) |
|
| Chemotherapy, n
(%) |
|
|
|
|
|
Yes | 96 (14.7) | 62 (14.4) | 34 (18.0) | 0.253 |
| Radiotherapy, n
(%) |
|
|
|
|
|
Yes | 59 (9.0) | 32 (7.9) | 27 (10.8) | 0.212 |
Univariate and multivariable analysis
indicates that NLR is a risk factor for OS and PFS
All the factors analyzed in univariate analysis with
Cox's proportional hazards model were identified to be associated
with an increased risk of mortality and disease progression,
including histologic grade, pathological diagnosis, TNM staging,
tumor location, recurrence, treatment and NLR (P<0.05; Tables III and IV). When adjusted in multivariable Cox's
models, non-glottic cancer, poor cancer cell differentiation, late
stage, recurrence and NLR >3.18 were identified to be associated
with an increased risk of mortality [NLR HR, 1.901; 95% confidence
interval (CI), 1.153–3.135; P=0.012; Table III]. Furthermore, NLR >3.18 was
also identified to be associated with increased risk of disease
progression (NLR HR, 1.621; 95% CI, 1.094–2.404; P=0.016; Table IV).
| Table III.Univariate and multivariable analyses
of hazard ratio for overall survival. |
Table III.
Univariate and multivariable analyses
of hazard ratio for overall survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| NLR |
|
|
|
|
|
>3.18 vs. ≤3.18 | 3.254
(2.171–4.877) | <0.0001 | 1.901
(1.153–3.135) | 0.012 |
| Age, years |
|
|
|
|
| >60
vs. ≤60 | 1.720
(1.153–2.567) | 0.008 |
| 0.077 |
| Tumor location |
|
|
|
|
| Glottic
vs. non-glottic | 4.833
(3.260–7.163) | <0.001 | 1.858
(1.071–3.223) | 0.028 |
| Histologic
grade |
|
| 1.528
(1.036–2.254) | 0.032 |
|
Moderately vs. well
differentiated | 2.822
(1.281–6.220) | 0.010 |
|
|
| Poorly
vs. well differentiated | 5.662
(2.552–12.565) | <0.001 |
|
|
| TNM stage |
|
| 1.582
(1.208–2.072) | 0.001 |
| II vs.
I | 1.163
(0.538–2.515) | 0.701 |
|
|
| III vs.
I | 3.464
(1.654–7.255) | 0.001 |
|
|
| IV vs.
I | 6.654
(3.524–12.566) | <0.001 |
|
|
| Recurrence |
|
|
|
|
| Yes vs.
no | 2.610
(1.745–3.904) | <0.001 | 1.884
(1.122–3.163) | 0.017 |
| Surgery |
|
|
| 0.842 |
| Total
LE vs. partial LE | 3.669
(2.397–5.616) | <0.001 |
|
|
|
Non-surgery vs. Partial
LE | 6.968
(3.975–12.217) | <0.001 |
|
|
| Neck
dissection |
|
|
|
|
| Yes vs.
no | 3.391
(2.224–5.168) | <0.001 |
| 0.075 |
| Chemotherapy |
|
|
|
|
| Yes vs.
no | 2.396
(1.422–4.037) | 0.001 |
| 0.402 |
| Radiotherapy |
|
|
|
|
| Yes vs.
no | 2.474
(1.608–3.808) | <0.001 |
| 0.239 |
| Table IV.Univariate and multivariable analyses
of hazard ratio for progression-free survival. |
Table IV.
Univariate and multivariable analyses
of hazard ratio for progression-free survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
|
| HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| NLR |
|
|
|
|
|
>3.18 vs. ≤3.18 | 2.191
(1.582–3.035) | <0.001 | 1.621
(1.094–2.404) | 0.016 |
| Age |
|
|
|
|
| >60
vs. ≤60 |
| 0.081 |
| 0.609 |
| Tumor location |
|
|
|
|
|
Non-glottic vs. glottic | 2.518
(1.867–3.398) | <0.001 | 1.604
(1.062–2.422) | 0.025 |
| Histologic
grade |
|
| 1.485
(1.139–1.938) | 0.004 |
|
Moderately vs. well
differentiated | 1.576
(0.978–2.539) | 0.061 |
|
|
| Poorly
vs. well differentiated | 2.821
(1.731–4.598) | <0.001 |
|
|
| TNM stage |
|
|
| 0.692 |
| II vs.
I | 0.839
(0.530–1.329) | 0.454 |
|
|
| III vs.
I | 1.609
(0.985–2.629) | 0.058 |
|
|
| IV vs.
I | 2.548
(1.702–3.814) | <0.001 |
|
|
| Surgery |
|
| 1.445
(0.967–2.159) | 0.073 |
| Total
LE vs. partial LE | 2.158
(1.560–2.986) | <0.001 |
|
|
|
Non-surgery vs. partial
LE | 3.323
(2.009–5.494) | <0.001 |
|
|
| Neck
dissection |
|
|
|
|
| Yes vs.
no | 1.665
(1.207–2.298) | 0.002 |
| 0.596 |
| Chemotherapy |
|
|
|
|
| Yes vs.
no | 1.999
(1.298–3.079) | 0.002 |
| 0.063 |
| Radiotherapy |
|
|
|
|
| Yes vs.
no | 1.755
(1.224–2.516) | 0.002 |
| 0.221 |
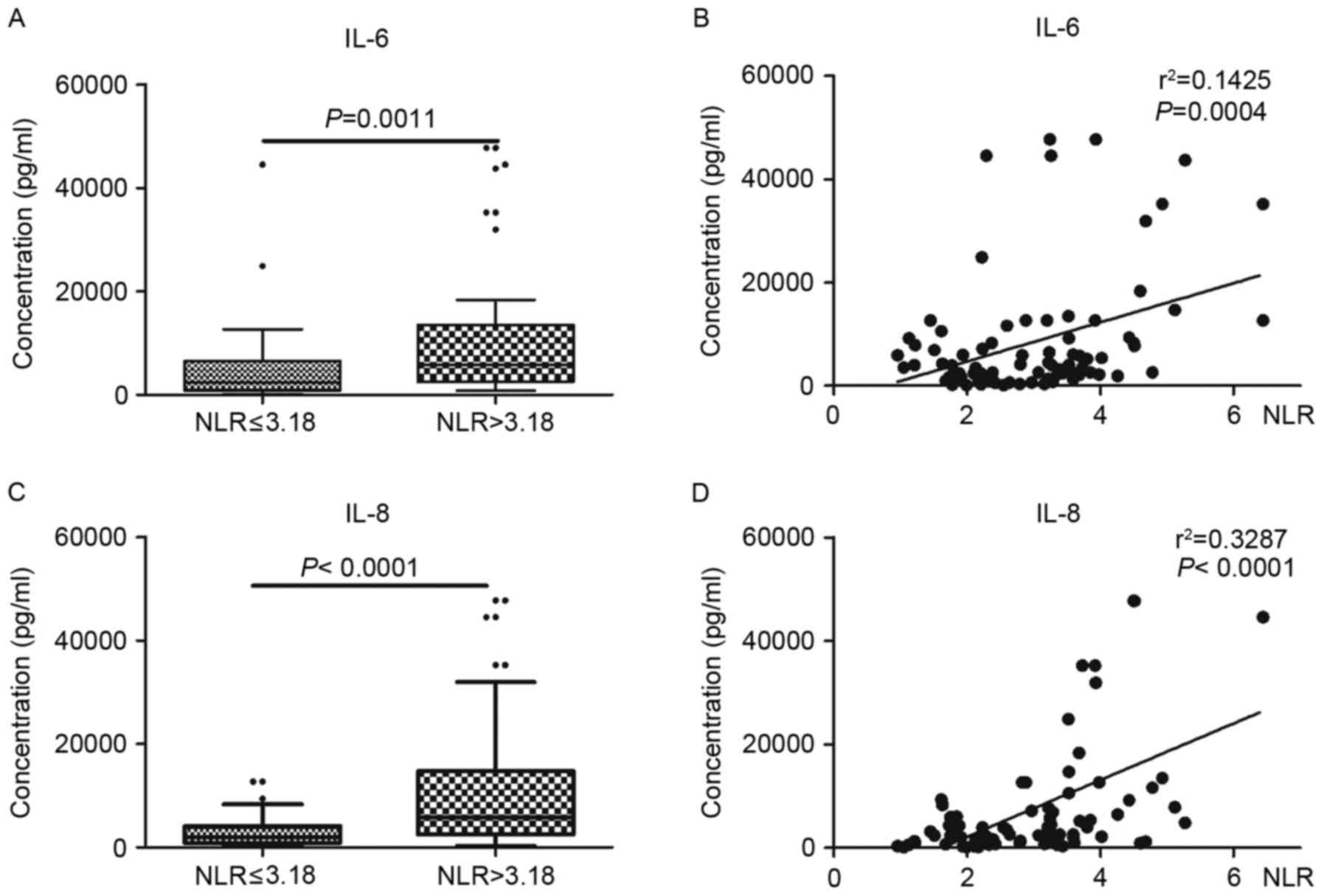
NLR is associated with the levels of
IL-6 and IL-8
To confirm the association between NLR and the level
of cytokines in tumor tissues, the levels of inflammatory mediators
in laryngeal cancer tissues were examined. As indicated in Fig. 3, the levels of IL-6 and IL-8 were
significantly increased in tumor tissues with higher NLR values
(NLR >3.18) compared with lower NLR values (NLR ≤3.18)
(P<0.01). Additionally, there was a significant association
between the levels of cytokines and NLR value (P<0.001).
Discussion
Association of systemic inflammation with
adverse outcomes in malignancies
Systemic hematological markers that represent the
inflammatory response of the body, including neutrophils,
lymphocytes and platelet counts, either alone or expressed as
ratios, have been used as prognostic factors associated with
malignancies (28). The prognostic
role of these markers is attributed to the infiltration of the
immune cells such as neutrophils and lymphocytes in solid tumors
and inflammation at the majority of cancer stages (28). Previously, studies on different
malignancies have demonstrated that higher NLR and PLR values were
associated with poorer prognoses in terms of mortality and
recurrence (24,29). Serum albumin and globulin belong to a
separate class of biochemical markers included in clinical routine
blood examinations. These are also used as prognostic factors in
various types of cancer. Serum albumin generally reflects the
severity of disease and the nutritional status of the body
(30). In addition, it is also used
to assess the progression and prognosis of certain malignancies
such as operable colorectal cancer, advanced non-small cell lung
cancer and ovarian cancer (16,27,28).
Concurrently, globulin was identified to be associated with certain
types of hormone-associated cancer with poor survival outcomes
(19,31,32), and
AGR (serum chemistry indexes for globulin and albumin levels
together) has been identified to function as an effective
prognostic factor for patients with cancer (20). In the present study, the levels of
cytokines (IL-6 and IL-8) were examined in tumor tissues, and it
was identified that the level of NLR was associated with the levels
of IL-6 and IL-8 in tumor tissues. As previously reported (33), cytokines may be secreted into blood as
chemokines of neutrophils to elevate neutrophil levels.
Association of NLR, PLR and AGR with the
severity of laryngeal cancer
The results of the present study indicated that the
medians of NLR, PLR and AGR were significantly increased with
increased T and N classifications as well as TNM stage,
respectively. Additionally, patients with NLR above the cutoff
values (NLR >3.18) demonstrated higher proportions of higher T,
N and clinical stage tumors. However, NLR was not associated with
histologic grades. The findings of the present study were different
from the results by Rassouli et al (21), where NLR and PLR values were analysed
in head and neck squamous cell carcinoma. Rassouli et al
(21) demonstrated that there was no
significant increase in NLR values with high T and N
classifications, and TNM stage. It was also demonstrated that a
higher NLR was associated with an increased proportion of higher T
classification in patients with other types of cancer (21), which was consistent with the data of
the present study.
Identification of optimal cutoff with
minimum bias with CART analysis
CART analysis has been used to estimate the survival
probability of individual patients with tumor (breast, head and
neck tumor) and to select immune markers for tumor diagnosis
(25–27). CART analysis also has been used in the
study of unknown primary carcinoma to estimate the survival
probability of individual patients and additionally in the analysis
of recurrence in breast cancer following radiation and chemotherapy
(24,25). A number of previous studies have
revealed the heterogeneity of NLR (cut-off, 1.9–7.2) (29) and PLR (cut-off, 100–300) (24) when predicting prognostic outcomes
(23,28). This may be attributed to the use of
different approaches in determining cutoff values in different
populations. In a study on head and neck squamous cell carcinoma by
Rassouli et al (21), a
recursive partitioning statistical approach was used to determine
the cut-off points of NLR (cut-off value, 3) and PLR (cut-off
value, 170).
However, in other studies investigating cancer, mean
(22), median (34) and ROC curve (20) were used to determine the cut-off
points, which may have led to heterogeneity in data. These cut-off
values may differ from the optimal original values for adverse
outcomes. The present study used a CART algorithm to produce the
predictive rules. Age, NLR, PLR and AGR were entered into the
analysis as independent variables, while overall survival status
was considered as a dependent variable, and only one node with NLR
at 3.18 divided patients into different groups. PLR, AGR and age
were excluded. Therefore, in the present study, the optimal cutoff
for NLR was identified as 3.18.
NLR predicts prognosis in patients with
laryngeal cancer
To the best of our knowledge, the present study
investigated the largest sample size for the prognostic ability of
NLR as an independent factor in patients with laryngeal squamous
cell cancer. NLR, at the determined cutoff points (NLR ≤3.18 and
>3.18), was able to differentiate the patients into two groups
with significantly different prognoses for OS and PFS. The groups
above the cutoff value (NLR >3.18) exhibited poorer prognoses in
the survival analysis. This result is consistent with previous
studies in a number of other malignancies (24,29).
Furthermore, NLR above the cutoff points was also associated with
an increased risk of mortality and disease progression in the
univariate analysis with Cox's regression model. Subsequent to
adjustment for age, pathological grade, TNM stage, treatment and
recurrence, a higher HR for OS was demonstrated for NLR values
above the cutoff point (NLR >3.18).
Previous studies with large patient populations have
also indicated the prognostic role of NLR in various malignancies
(29). Therefore, the authors of the
present study hypothesized that with a large sample size,
collection of more detailed information and reduction in the loss
of follow-up, consistent or more accurate results may be obtained.
The results of the present study indicate that NLR, as an index of
the systemic inflammatory response, may predict prognosis in
patients with laryngeal cancer.
In conclusion, the results of the present study have
demonstrated that pretreatment NLR, PLR and serum AGR may be
associated with the severity of laryngeal cancer, and NLR may serve
as a useful prognostic predictor for patients with laryngeal
cancer. With these readily available and inexpensive biomarkers,
prognostic factors may be established for clinical decisions,
including stringent follow-up and additional adjunctive therapy, to
improve the stratification of patients with laryngeal cancer.
Acknowledgements
The authors would like to thank Professor Yajia Lan
(School of Public Health, West China Medical Center, Sichuan
University, Chengdu, China) for his assistance in statistical
analysis, and Xiaofang Chen (Sichuan Province Center for Disease
Control and Prevention, Chengdu, China) for her assistance in
investigating the survival status of patients using the Disease
Surveillance Point System. The authors would also like to thank
Professor Hengyi Xiao (Laboratory for Aging Research, Center for
Medical Stem Cell Biology, State Key Laboratory of Biotherapy, West
China Hospital, China) for her assistance in reviewing the
manuscript.
Glossary
Abbreviations
Abbreviations:
|
NLR
|
neutrophil-to-lymphocyte ratio
|
|
IL-6
|
interleukin-6
|
|
IL-8
|
interleukin-8
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
CART
|
classification and regression tree
|
References
|
1
|
Cahlon O, Lee N, Le QT, Kaplan MJ and
Colevas AD: Cancer of the larynx. https://clinicalgate.com/cancer-of-the-larynx/April
9–2015
|
|
2
|
American Cancer Society, . What are the
key statistics about laryngeal and hypopharyngeal cancers.
https://www.cancer.org/cancer/laryngeal-and-hypopharyngeal-cancer/about/key-statistics.htmlJanuary
5–2017
|
|
3
|
Barzan L, Talamini R, Franchin G, Vaccher
E, Politi D, Minatel E and Gobitti C: Changes in presentation and
survival of head and neck carcinomas in Northeastern Italy,
1975–1998. Cancer. 95:540–552. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Woodard TD, Oplatek A and Petruzzelli GJ:
Life after total laryngectomy: A measure of long-term survival,
function, and quality of life. Arch Otolaryngol Head Neck Surg.
133:526–532. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ji W, Guan C and Pan Z: Analysis of
curative effects on laryngeal carcinoma patients in the northeast
region of China. Acta Otolaryngol. 128:574–577. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hermanns T, Bhindi B, Wei Y, Yu J, Noon
AP, Richard PO, Bhatt JR, Almatar A, Jewett MA, Fleshner NE, et al:
Pre-treatment neutrophil-to-lymphocyte ratio as predictor of
adverse outcomes in patients undergoing radical cystectomy for
urothelial carcinoma of the bladder. Br J Cancer. 111:444–451.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Grivennikov SI, Greten FR and Karin M:
Immunity, inflammation, and cancer. Cell. 140:883–899. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Canna K, McArdle PA, McMillan DC, McNicol
AM, Smith GW, McKee RF and McArdle CS: The relationship between
tumour T-lymphocyte infiltration, the systemic inflammatory
response and survival in patients undergoing curative resection for
colorectal cancer. Br J Cancer. 92:651–654. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Roxburgh CS, Salmond JM, Horgan PG, Oien
KA and McMillan DC: Comparison of the prognostic value of
inflammation-based pathologic and biochemical criteria in patients
undergoing potentially curative resection for colorectal cancer.
Ann Surg. 249:788–793. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Guthrie GJ, Charles KA, Roxburgh CS,
Horgan PG, McMillan DC and Clarke SJ: The systemic
inflammation-based neutrophil-lymphocyte ratio: Experience in
patients with cancer. Crit Rev Oncol Hematol. 88:218–230. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Smith RA, Bosonnet L, Ghaneh P, Sutton R,
Evans J, Healey P, Garvey C, Hughes M, Raraty M, Campbell F and
Neoptolemos JP: The platelet-lymphocyte ratio improves the
predictive value of serum CA19-9 levels in determining patient
selection for staging laparoscopy in suspected periampullary
cancer. Surgery. 143:658–666. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ying HQ, Deng QW, He BS, Pan YQ, Wang F,
Sun HL, Chen J, Liu X and Wang SK: The prognostic value of
preoperative NLR, d-NLR, PLR and LMR for predicting clinical
outcome in surgical colorectal cancer patients. Med Oncol.
31:3052014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xue TC, Zhang L, Xie XY, Ge NL, Li LX,
Zhang BH, Ye SL and Ren ZG: Prognostic significance of the
neutrophil-to-lymphocyte ratio in primary liver cancer: A
meta-analysis. PLoS One. 9:e960722014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wei Y, Jiang YZ and Qian WH: Prognostic
role of NLR in urinary cancers: A meta-analysis. PLoS One.
9:e920792014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Roxburgh CS and McMillan DC: Role of
systemic inflammatory response in predicting survival in patients
with primary operable cancer. Future Oncol. 6:149–163. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bizzo SM, Meira DD, Lima JM, Mororó Jda S,
Moreira FC, Casali-da-Rocha JC and Ornellas MH: Serum albumin and
vascular endothelial growth factor in epithelial ovarian cancer:
Looking at adnexal tumor drainage. Arch Gynecol Obstet.
283:855–859. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fujii T, Sutoh T, Morita H, Katoh T,
Yajima R, Tsutsumi S, Asao T and Kuwano H: Serum albumin is
superior to prealbumin for predicting short-term recurrence in
patients with operable colorectal cancer. Nutr Cancer.
64:1169–1173. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Adly L, Hill D, Sherman ME, Sturgeon SR,
Fears T, Mies C, Ziegler RG, Hoover RN and Schairer C: Serum
concentrations of estrogens, sex hormone-binding globulin, and
androgens and risk of breast cancer in postmenopausal women. Int J
Cancer. 119:2402–2407. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yao Y, Zhao M, Yuan D, Gu X, Liu H and
Song Y: Elevated pretreatment serum globulin albumin ratio predicts
poor prognosis for advanced non-small cell lung cancer patients. J
Thorac Dis. 6:1261–1270. 2014.PubMed/NCBI
|
|
21
|
Rassouli A, Saliba J, Castano R, Hier M
and Zeitouni AG: Systemic inflammatory markers as independent
prognosticators of head and neck squamous cell carcinoma. Head
Neck. 37:103–110. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kum RO, Ozcan M, Baklaci D, Kum NY, Yilmaz
YF, Gungor V and Unal A: Elevated neutrophil-to-lymphocyte ratio in
squamous cell carcinoma of larynx compared to benign and
precancerous laryngeal lesions. Asian Pac J Cancer Prev.
15:7351–7355. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
American Joint Committee on Cancer, .
LarynxAJCC Cancer Staging Manual. 7th. Springer; New York, NY: pp.
57–62. 2010
|
|
24
|
Zhou X, Du Y, Huang Z, Xu J, Qiu T, Wang
J, Wang T, Zhu W and Liu P: Prognostic value of PLR in various
cancers: A meta-analysis. PLoS One. 9:e1011192014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Freedman GM, Hanlon AL, Fowble BL,
Anderson PR and Nicolaou N: Recursive partitioning identifies
patients at high and low risk for ipsilateral tumor recurrence
after breast-conserving surgery and radiation. J Clin Oncol.
20:4015–4021. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hess KR, Abbruzzese MC, Lenzi R, Raber MN
and Abbruzzese JL: Classification and regression tree analysis of
1000 consecutive patients with unknown primary carcinoma. Clin
Cancer Res. 5:3403–3410. 1999.PubMed/NCBI
|
|
27
|
Rassouli A, Saliba J, Castano R, Hier M
and Zeitouni AG: Systemic inflammatory markers as independent
prognosticators of head and neck squamous cell carcinoma. Head
Neck. 37:103–110. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Grivennikov SI and Karin M: Inflammation
and oncogenesis: A vicious connection. Curr Opin Genet Dev.
20:65–71. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Templeton AJ, McNamara MG, Šeruga B,
Vera-Badillo FE, Aneja P, Ocaña A, Leibowitz-Amit R, Sonpavde G,
Knox JJ, Tran B, et al: Prognostic role of neutrophil-to-lymphocyte
ratio in solid tumors: A systematic review and meta-analysis. J
Natl Cancer Inst. 106:dju1242014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Arrieta O, Michel Ortega RM,
Villanueva-Rodríguez G, Serna-Thomé MG, Flores-Estrada D,
Diaz-Romero C, Rodríguez CM, Martínez L and Sánchez-Lara K:
Association of nutritional status and serum albumin levels with
development of toxicity in patients with advanced non-small cell
lung cancer treated with paclitaxel-cisplatin chemotherapy: A
prospective study. BMC cancer. 10:502010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Asher V, Lee J and Bali A: Preoperative
serum albumin is an independent prognostic predictor of survival in
ovarian cancer. Med Oncol. 29:2005–2009. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kristal AR, Schenk JM, Song Y, Arnold KB,
Neuhouser ML, Goodman PJ, Lin DW, Stanczyk FZ and Thompson IM:
Serum steroid and sex hormone-binding globulin concentrations and
the risk of incident benign prostatic hyperplasia: Results from the
prostate cancer prevention trial. Am J Epidemiol. 168:1416–1424.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chen ZY, Raghav K, Lieu CH, Jiang ZQ, Eng
C, Vauthey JN, Chang GJ, Qiao W, Morris J, Hong D, et al: Cytokine
profile and prognostic significance of high neutrophil-lymphocyte
ratio in colorectal cancer. Br J Cancer. 112:1088–1097. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhang Y, Wang L, Liu Y, Wang S, Shang P,
Gao Y and Chen X: Preoperative neutrophil-lymphocyte ratio before
platelet-lymphocyte ratio predicts clinical outcome in patients
with cervical cancer treated with initial radical surgery. Int J
Gynecol Cancer. 24:1319–1325. 2014. View Article : Google Scholar : PubMed/NCBI
|