Introduction
Intrahepatic cholangiocarcinoma (ICC) arises from
the bile epithelial cells of the intrahepatic second-degree bile
tracts (1). ICC is the second most
common primary liver cancer following hepatocellular carcinoma
(HCC) and accounts for 10–15% of all primary liver cancer cases
(2). In recent decades, the incidence
rate for ICC has increased worldwide (3,4). Despite
the existence of diverse treatment strategies, including curative
surgical resection, pre-operative portal vein embolization,
trans-arterial chemoembolization and liver transplantation, the
prognosis for patients with ICC remains unsatisfactory (5,6). Frequent
recurrence and aggressive metastasis limit the success of
postoperative therapies and the overall prognosis (7). Therefore, a better comprehension of the
potential molecular mechanisms behind ICC is urgently required in
order to investigate potential prognostic factors and to improve
the overall survival (OS) rate.
The B-cell lymphoma 2 gene (Bcl-2) (8) is part of a family of proteins whose main
function is their involvement in the initiation phase of the
intrinsic pathways of apoptosis (9).
Bcl-2 has been demonstrated to be associated with apoptosis
(10), which can be induced via
various stimuli, including lipid peroxidation, glucose deprivation
and growth factor deprivation (8).
High expression of Bcl-2 has been indicated to protect against
apoptosis (11). A number of clinical
studies suggested that the overexpression of Bcl-2 was associated
with a relatively poor prognosis in a number of malignant tumors
types, including breast cancer and pancreatic carcinoma (12,13).
Bcl-2-like protein 4 (Bax), a pro-apoptotic protein of the Bcl-2
family of proteins, has been demonstrated to be directly regulated
by the tumor suppressor cellular antigen p53 (p53) (14). Multiple studies have demonstrated that
Bax could strongly facilitate mitochondrial membrane
permeabilization and the activation of nucleases and caspases. This
can result in irreversible damage to the mitochondria and
accelerated programmed cell death (15,16).
Mortalin (also known as glucose-regulated protein
75) is a member of the heat shock protein 70 family, which was
originally identified in the cytoplasm of mouse embryonic
fibroblasts (17). Research suggests
that the expression of mortalin is associated with a number of
biological processes, including intracellular trafficking, cell
proliferation and apoptosis, protein localization, antigen
processing, muscle activity and regulation of p53 (18,19).
Previous studies have demonstrated that mortalin interacts directly
with Bcl-2 and can indirectly regulate Bax via p53 (20,21).
Recent studies have demonstrated that mortalin is overexpressed in
numerous types of cancerous tumors, and is involved in a multitude
of pathological processes that promote tumor carcinogenesis and
progression (22–24).
The aim of the present study was to investigate the
expression of mortalin, Bcl-2 and Bax in ICC, and the association
between these 3 markers and the clinicopathological features of
patients with ICC. The associations between the expression of these
markers was analyzed, and finally, the prognostic significance of
mortalin, Bcl-2 and Bax in patients with ICC was statistically
evaluated.
Materials and methods
Patients and follow-up
Fresh ICC tumor tissues and their corresponding
peritumoral tissues were obtained from 116 consecutive patients
(mean age, 59.38; range 30–81) who underwent curative resection
between February 1998 and December 2006 at the Liver Cancer
Institute (Zhongshan Hospital, Shanghai, China). Curative resection
was defined as per Huang et al (25). Liver function was evaluated according
to the Child-Pugh scoring system (26). ICC diagnosis was based on the criteria
outlined by the World Health Organization (27). Tumor differentiation was based on the
classification proposed by Edmondson and Steiner (27). The clinical classification of tumors
was performed according to the 7th edition of the
tumor-node-metastasis (TNM) classification system of the
International Union Against Cancer (28). The detailed clinicopathological
features recorded are provided in Table
I. The following patient exclusion criteria were applied:
Failure of important organs, including the heart, lungs, kidneys
and brain, intolerance to surgery, distant organ metastasis, lymph
node involvement beyond the hepatoduodenal ligament, hilar or caval
lymph nodes, preoperative chemotherapy or radiotherapy and
preoperative liver treatment (arterial chemoembolization,
radiofrequency ablation or percutaneous ethanol injection). Ethical
approval was obtained from the Zhongshan Hospital Research Ethics
Committee and each patient provided written informed consent. All
incorporated ICC patients had undergone regular follow-ups and full
clinicopathological data was available for prognostic analysis.
During follow-up, abdominal Doppler ultrasonography, a physical
examination and serological tests were performed every 1–2 months
postoperatively during the first 2 years, then every 3–4 months
from years 2–5 and every 6 months thereafter. For patients with
suspected recurrence of ICC, computed tomography or magnetic
resonance was used for confirmation. Patients with recurrence were
treated by arterial chemoembolization, radiofrequency ablation and
percutaneous ethanol injection or a second liver resection
depending on the tumor number, location and size, the number of
affected lymph nodes and the extent of distant metastasis. OS time
was defined as the time between the date of original surgery until
the end of follow-up (December 31, 2016) or the event of mortality
from any cause. The recurrence time was defined as the duration
between the date of original surgery to the time of recurrence. The
median follow-up time was 31.5 months (range, 4–120 months).
 | Table I.Association of mortalin, Bax or Bcl-2
expression with clinicopathological characteristics in 116 patients
with intrahepatic cholangiocarcinoma. |
Table I.
Association of mortalin, Bax or Bcl-2
expression with clinicopathological characteristics in 116 patients
with intrahepatic cholangiocarcinoma.
| Variable | Number | Mortalin staining
(% total area) | P-value | Bcl-2 staining (%
total area) | P-value | Bax staining (%
total area) | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
|
≥53 | 60 | 47.7±23.9 | NS | 53.4±22.9 | 0.029 | 21.1±14.5 | NS |
|
<53 | 56 | 48.4±22.8 |
| 44.9±20.7 |
| 21.7±16.4 |
|
| Sex |
|
|
|
|
|
|
|
|
Male | 50 | 51.2±24.5 | NS | 51.7±21.9 | NS | 20.6±12.2 | NS |
|
Female | 66 | 45.3±22.3 |
| 47.4±22.7 |
| 22.5±17.6 |
|
| GGT, U/l |
|
|
|
|
|
|
|
|
≥37 | 60 | 47.5±23.2 | NS | 49.9±22.4 | NS | 22.0±15.9 | NS |
|
<37 | 56 | 48.6±23.6 |
| 47.9±22.6 |
| 21.4±15.2 |
|
| CEA, ng/ml |
|
|
|
|
|
|
|
| ≥5 | 71 | 52.5±21.4 | NS | 49.9±22.3 | NS | 22.0±15.9 | NS |
|
<5 | 45 | 45.2±24.2 |
| 48.5±22.6 |
| 21.4±15.2 |
|
| CA19-9, ng/ml |
|
|
|
|
|
|
|
|
>75 | 70 | 47.2±23.9 | NS | 47.9±22.7 | NS | 19.3±14.5 | 0.039 |
|
≤75 | 46 | 49.4±22.5 |
| 50.6±22.1 |
| 25.3±16.2 |
|
| Liver
cirrhosis |
|
|
|
|
|
|
|
|
Yes | 47 | 52.2±22.8 | 0.018 | 50.2±22.6 | NS | 22.8±17.5 | NS |
| No | 69 | 41.9±22.9 |
| 47.3±22.3 |
| 20.8±13.9 |
|
| Tumor
encapsulation |
|
|
|
|
|
|
|
| No | 96 | 49.1±22.6 | NS | 49.3±22.9 | NS | 21.8±15.1 | NS |
|
Yes | 20 | 43.1±21.9 |
| 47.5±20.3 |
| 20.8±17.1 |
|
| Lymphatic
metastasis |
|
|
|
|
|
|
|
|
Yes | 28 | 54.2±22.8 | 0.009 | 52.5±22.7 | NS | 19.7±11.8 | NS |
| No | 88 | 45.1±23.1 |
| 47.3±22.2 |
| 22.4±16.8 |
|
| Tumor number |
|
|
|
|
|
|
|
|
Multiple | 10 | 62.9±20.9 | 0.034 | 67.8±17.9 | 0.005 | 20.8±15.5 | NS |
|
Solitary | 106 | 46.6±23.1 |
| 47.2±22.1 |
| 21.6±15.5 |
|
| Tumor diameter,
cm |
|
|
|
|
|
|
|
| ≥5 | 25 | 47.1±22.5 | NS | 48.9±22.7 | NS | 26.1±18.3 | 0.013 |
|
<5 | 91 | 48.3±26.7 |
| 49.5±21.5 |
| 19.5±14.5 |
|
| Tumor
differentiation |
|
|
|
|
|
|
|
| Grade
3/4 | 58 | 53.1±24.6 | 0.017 | 53.4±21.4 | 0.042 | 21.0±15.4 | NS |
| Grade
1/2 | 58 | 42.9±20.9 |
| 45.1±22.2 |
| 21.9±15.6 |
|
| TNM stage |
|
|
|
|
|
|
|
|
III/IV | 32 | 52.9±23.5 | 0.047 | 55.1±21.6 | 0.012 | 17.4±10.1 | 0.021 |
|
I/II | 84 | 44.3±22.6 |
| 44.8±21.5 |
| 24.4±17.9 |
|
Tissue microarray and
immunohistochemistry (IHC)
Tissue microarrays were constructed and IHC was
performed as described in our previous studies (25,29).
Rabbit anti-human mortalin monoclonal antibody (cat. no. 3593,
dilution 1:100; Cell Signaling Technology, Inc., Danvers, MA, USA),
mouse anti-human Bcl-2 monoclonal antibody (cat. no. ab182858,
dilution 1:400) and mouse anti-human Bax monoclonal antibody (cat.
no. ab77566; dilution 1:400) (both from Abcam, Cambridge, UK) were
used to detect the expression of mortalin, Bcl-2 and Bax in ICC
tissues, respectively. Two independent pathologists, who were
blinded to patient clinicopathological characteristics, analyzed
the IHC staining using an optical microscope. The scoring criteria
for the determination of mortalin, Bcl-2 and Bax staining
intensities were defined as follows: 3, strong (deep-brown
staining); 2, moderate (medium-brown staining); 1, weak
(light-brown staining); and 0, negative (absence of brown
staining). The mean area of positive staining was scored as
follows: 0, 0–30%; 1, 31–60%; and 2%, >60%. Total staining score
(intensity + mean area) ≥2.0 was considered to indicate high
expression, and total scores <2.0 were considered to indicate
low expression.
Statistical analysis
Statistical analysis was performed using SPSS,
version 21.0 (IBM Corp., Armonk, NY, USA). Data are presented as
the mean ± standard deviation. Continuous data were analyzed using
Student's t-tests. The correlations between mortalin, Bcl-2 and Bax
protein levels were assessed using Pearson's correlation
coefficient and multiple linear regression analysis. The
Kaplan-Meier method and the log-rank test were used to calculate
the OS and cumulative recurrence rates. Cox's proportional hazards
regression model was used to investigate potential independent
prognostic factors. All tests were two-tailed. P<0.05 was
considered to indicate a statistically significant difference.
Results
Expression of mortalin, Bcl-2 and Bax
in ICC patients
Hematoxylin and eosin staining was used to identify
primary ICC, and the expression of mortalin, Bcl-2 and Bax protein
was detected using IHC of tissues from 116 patients with ICC.
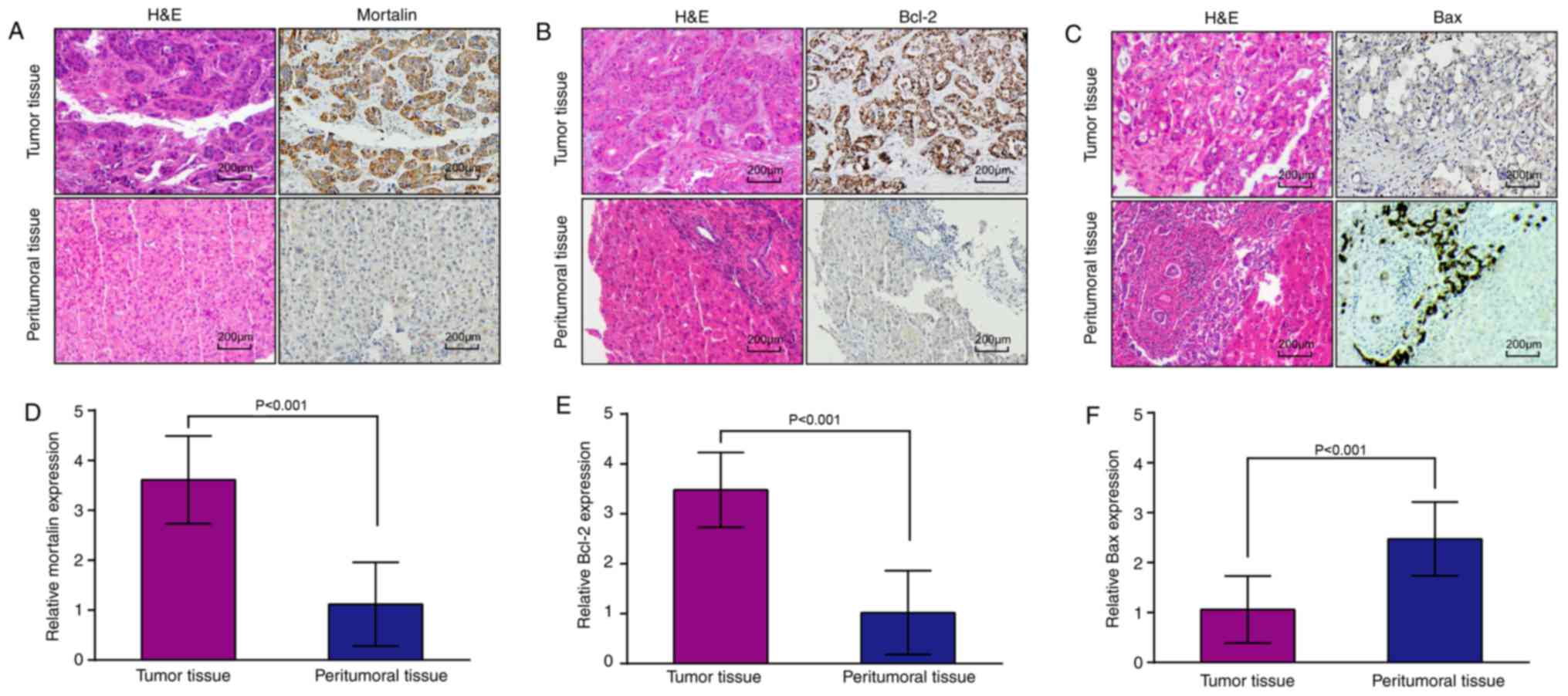
Mortalin (Fig. 1A) and Bcl-2
(Fig. 1B) expression was exhibited in
the cell cytoplasm of ICC tumor cells. However, Bax expression was
exhibited in the cell cytoplasm of peritumoral bile epithelial
cells (Fig. 1C).
A total of 60 ICC tumor tissues expressed high
levels of mortalin (51.7%). The expression of mortalin was higher
in ICC tissues than in adjacent peritumoral liver tissues
(3.61±0.88 vs. 1.12±0.84, P<0.001; Fig. 1A and D). Consistent with a previous
study (29), high expression of
mortalin was significantly associated with liver cirrhosis
(P=0.018), lymphatic metastasis (P=0.009), tumor differentiation
(P=0.017), tumor number (P=0.034) and TNM stage (P=0.047) (Table I). However, none of the other clinical
characteristics, including age, sex, serum γ-glutamyl
transpeptidase (GGT), carcinoembryonic antigen (CEA), carbohydrate
antigen 19-9 (CA19-9), tumor encapsulation or tumor diameter were
associated with mortalin expression.
High Bcl-2 expression was exhibited in 61 ICC tumor
tissues (52.6%). Higher levels of Bcl-2 expression were detected in
tumor tissues compared with the levels detected in peritumoral
tissues (3.48±0.75 vs. 1.02±0.84, P<0.001; Fig. 1B and E). Patients with high Bcl-2
expression were older (P=0.029), had multiple tumors (P=0.005), low
tumor differentiation (P=0.017) and a high TNM stage (P=0.047)
compared with patients exhibiting low Bcl-2 expression expression
(Table I).
A total of 18 ICC tissues expressed high levels of
Bax (15.5%). Expression of Bax was evidently lower in ICC tissues
compared with the peritumoral tissues (1.06±0.67 vs. 2.54±0.78,
P<0.001; Fig. 1C and F). Serum
CA19-9 was significantly associated with low Bax expression
(P=0.039), tumor diameter (P=0.013) and TNM stage (P=0.021)
(Table I).
Clinical association between the
expression of mortalin and Bcl-2 or Bax in ICC patients
A correlation analysis of mortalin, Bcl-2 and Bax
expression was performed on the basis of the IHC results. The
expression levels of mortalin and Bcl-2 protein levels were
markedly increased in ICC tissues, whereas the expression level of
Bax protein was significantly downregulated in tumor tissues. The
high expression of mortalin was positively correlated with the
expression of Bcl-2 (Fig. 2A), as
indicated in a scatter plot of mortalin and Bcl-2 expression in
Fig. 2B (r=0.398, P<0.001).
However, high mortalin expression was negatively correlated with
the expression of Bax (r=−0.238, P=0.010; Fig. 2C), and high Bcl-2 expression was also
negatively correlated with the expression of Bax (r=−0.207,
P=0.026; Fig. 2D). Furthermore,
multiple linear regression analysis also revealed that the
expression of mortalin was positively associated with that of Bcl-2
(r=0.425, P<0.001) in ICC patients (data not shown). However, no
significant association was detected for Bax (P=0.091) (data not
shown).
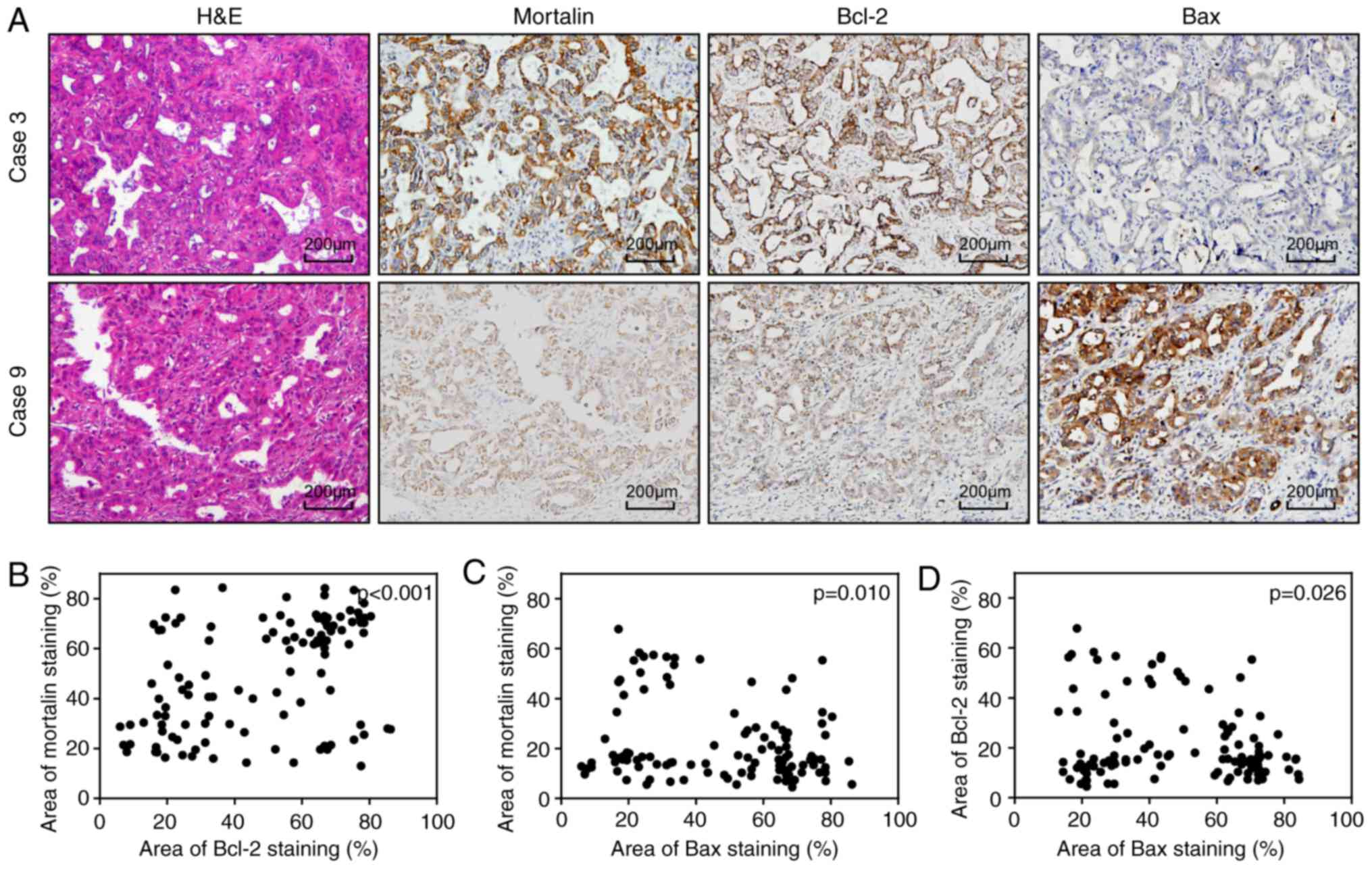 | Figure 2.Associations between mortalin, Bcl-2
and Bax expression in ICC tumor samples. (A) Representative
staining images demonstrating high moratlin and Bcl-2 expression
and low Bax expression tissue (case 3), and low mortalin and Bcl-2
expression and low Bax expression tissue (case 9) (scale bars, 200
µm). Positive correlations were detected between (B) mortalin and
Bcl-2 expression in ICC tissues (r=0.398, P<0.001); (C) between
mortalin and Bax expression (r=−0.238, P=0.010) and (D) between
Bcl-2 and Bax expression (r=−0.207, P=0.026). Bcl-2, B-cell
lymphoma 2; Bax, Bcl-2-like protein 4; ICC, intrahepatic
cholangiocarcinoma; H&E, hematoxylin and eosin. |
Combined expression of mortalin, Bcl-2
and Bax is associated with poor prognosis in patients with ICC
Over the follow-up period, 83 patients suffered from
ICC recurrence and 84 fatalities occurred. The 2- and 5-year OS
rates for patients with ICC were 69.8 and 28.3%, respectively, and
the 2- and 5-year cumulative recurrence rates were 38.7 and 72.4%,
respectively. Univariate analysis demonstrated that lymphatic
metastasis, tumor differentiation, tumor number and TNM stage were
predictors of OS and cumulative recurrence (Table II). Other clinicopathological
characteristics, such as age, sex, serum GGT, serum CEA, serum
CA9-9, liver cirrhosis, tumor encapsulation and max diameter had no
prognostic significance in terms of the OS or cumulative recurrence
rates (Table II).
| Table II.Univariate and multivariate Cox
regression analysis of factors associated with overall survival
rate and cumulative recurrence rate. |
Table II.
Univariate and multivariate Cox
regression analysis of factors associated with overall survival
rate and cumulative recurrence rate.
|
| Overall
survival | Cumulative
recurrence |
|---|
|
|
|
|
|---|
|
|
| Multivariate |
| Multivariate |
|---|
|
|
|
|
|
|
|---|
| Variable | Univariate
P-value | HR (95% CI) | P-value | Univariate
P-value | HR (95% CI) | P-value |
|---|
| Age (<53 vs. ≥53
years) | 0.401 |
| NA | 0.368 |
| NA |
| Sex (male vs.
female) | 0.791 |
| NA | 0.637 |
| NA |
| GGT (<37 vs. ≥37
U/l) | 0.602 |
| NA | 0.101 |
| NA |
| CEA (<5 vs. ≥5
ng/ml) | 0.398 |
| NA | 0.332 |
| NA |
| Serum CA19-9
(<37 vs. ≥37 ng/ml) | 0.189 |
| NA | 0.064 |
| NA |
| Liver cirrhosis (no
vs. yes) | 0.477 |
| NA | 0.280 |
| NA |
| Tumor encapsulation
(no vs. yes) | 0.191 |
| NA | 0.067 |
| NS |
| Lymphatic
metastasis (no vs. yes) | <0.001 |
| NS | <0.001 |
| NS |
| TNM stage (I/II vs.
III/IV) | <0.001 | 0.563
(0.320–0.993) | 0.047 | <0.001 | 0.524
(0.301–0.910) | 0.022 |
| Tumor number
(single vs. multiple) | <0.001 |
| NS | 0.001 |
| NS |
| Tumor diameter
(<5 vs. ≥5 cm) | 0.152 |
| NA | 0.098 |
| NA |
| Tumor
differentiation (low vs. high) | <0.001 | 0.562
(0.354–0.891) | 0.014 | <0.001 | 0.536
(0.337–0.851) | 0.008 |
| Mortalin staining
(low vs. high) | <0.001 | 3.381
(1.777–6.435) | <0.001 | <0.001 | 3.175
(1.675–6.018) | <0.001 |
| Bcl-2 staining (low
vs. high) | 0.001 | 2.909
(1.550–5.459) | 0.001 | <0.001 | 2.636
(1.351–4.732) | 0.004 |
| Bax staining (low
vs. high) | 0.009 |
| NS | 0.010 |
| NS |
| Combination of
mortalin, Bcl-2 and | 0.002 | 3.277
(1.459–7.358) | 0.004 | 0.002 | 2.808
(1.257–6.271) | 0.012 |
| Bax (group I vs.
groups II/III)a |
|
|
|
|
|
|
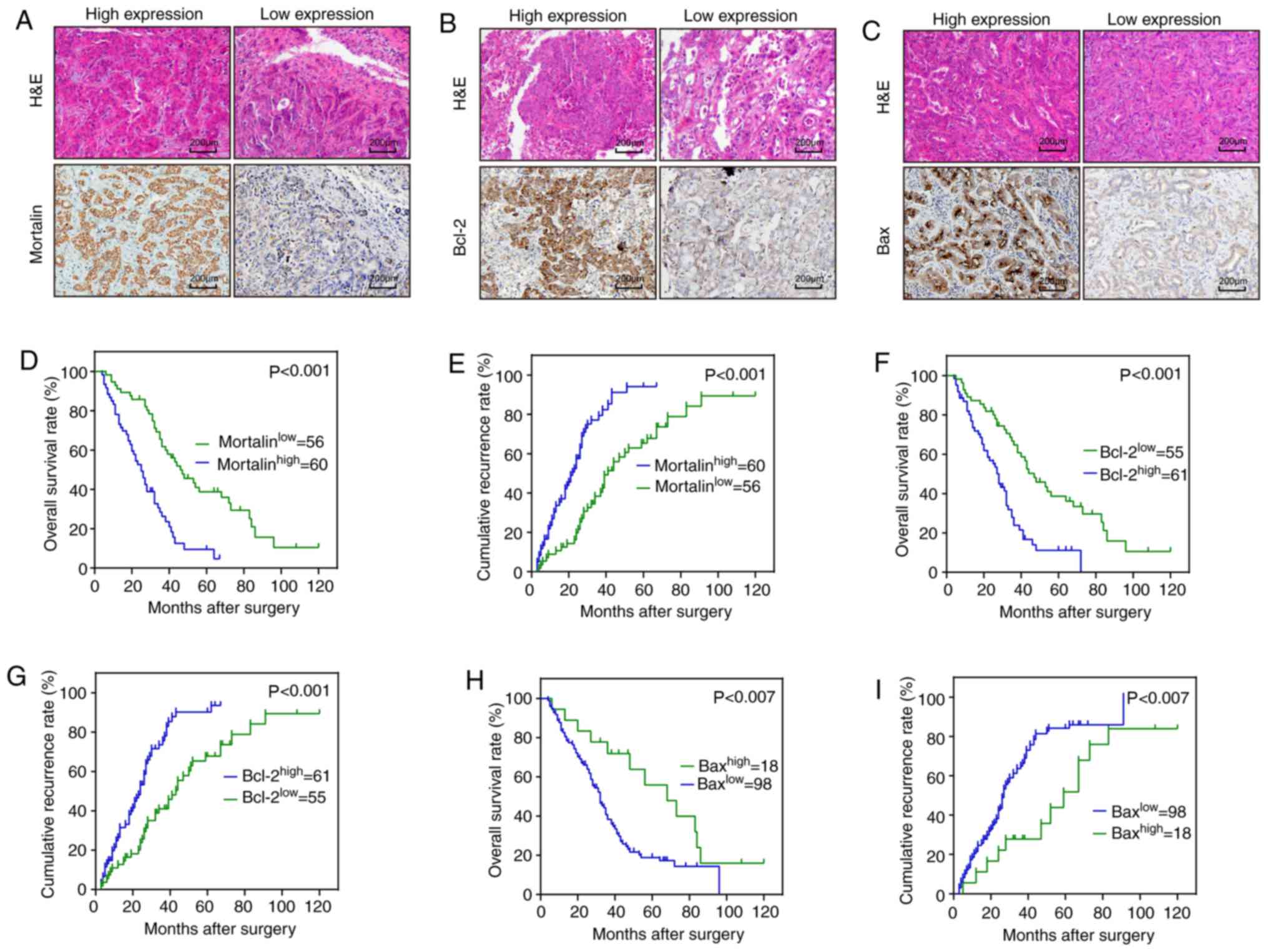
The expression of mortalin, Bcl-2 and Bax was also
associated with OS and cumulative recurrence rates. As illustrated
in Fig. 3A-C, the expression of the
three proteins in the ICC tumor tissues demonstrated considerable
heterogeneity. The 2- and 5-year OS rates in the high mortalin
expression group were significantly lower than those in the low
mortalin expression group (51.0 vs. 85.7% and 18.3 vs. 41.1%,
respectively; Fig. 3D). The
corresponding cumulative recurrence rates in the high mortalin
expression group were significantly higher than those in the low
mortalin expression group (53.3 vs. 21.4% and 85.0 vs. 62.5%,
respectively; Fig. 3E). The 2- and
5-year OS rates in the high Bcl-2 expression group were
significantly lower compared with those in the low Bcl-2 expression
group (55.7 vs. 80.0% and 18.1 vs. 43.6%, respectively; Fig. 3F). The 2- and 5-year cumulative
recurrence rates in the high Bcl-2 expression group were
significantly higher than those in the low Bcl-2 expression group
(52.5 vs. 23.6% and 81.9 vs. 61.8%, respectively; Fig. 3G). The postoperative 2- and 5-year OS
rates for ICC patients were lower in the low Bax expression group
than those in the high Bax expression group (66.3 vs. 88.3% and
17.3 vs. 44.4%, respectively; Fig.
3H), and the postoperative 2- and 5-year cumulative recurrence
rates in the high Bax expression group were significantly higher
than those in the low Bax expression group (22.2 vs. 41.8% and 55.6
vs. 84.7%, respectively; Fig.
3I).
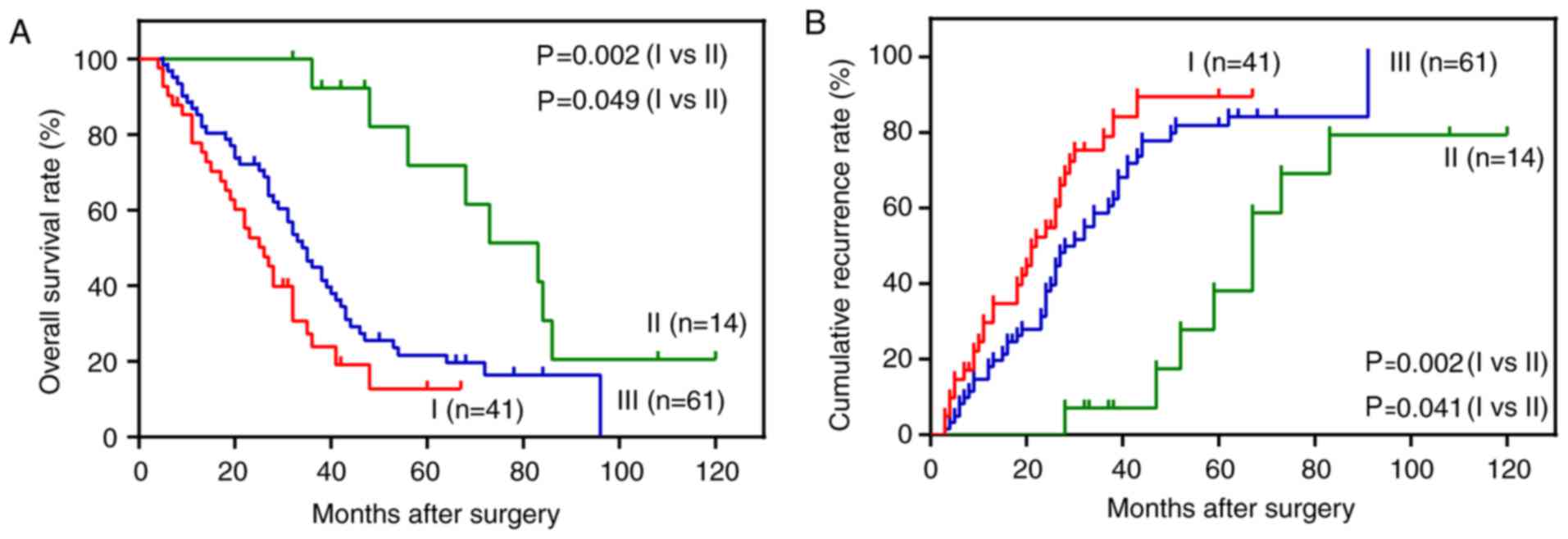
To investigate the combined effect of the expression
of mortalin, Bcl-2 and Bax on the prognosis of patients with ICC,
patient samples were divided into 3 subgroups: Group I (n=41)
exhibited low expression of Bax and high expression of mortalin and
Bcl-2; group II (n=14) exhibited high expression of Bax and low
expression of mortalin and Bcl-2; and group III (n=61) consisted of
all remaining possible combinations of expression of the 3
proteins, including high expression of all 3 markers; low
expression of all 3 markers; low expression of Bcl-2, and high
expression of mortalin and Bax; high expression of mortalin, and
low expression of Bcl-2 and Bax; high expression of Bcl-2, and low
expression of mortalin and Bax; low expression of mortalin, and
high expression of Bcl-2 and Bax. Kaplan-Meier analysis
demonstrated that the 2- and 5-year OS rates in group I were
significantly lower than those in groups II and III (P<0.05;
Fig. 4A). The 2- and 5-year
cumulative recurrence rates in group I were significantly higher
than those for groups II and III (P<0.05; Fig. 4B). The multivariate Cox proportional
hazards model analysis demonstrated that mortalin, Bcl-2, tumor
differentiation and TNM stage were independent prognostic
indicators for OS rate and cumulative recurrence of ICC (Table II). Furthermore, the combination of
overexpression of mortalin and Bcl-2 and low expression of Bax was
also an independent prognostic indicator for OS rate and cumulative
recurrence (Table II).
Discussion
Mortalin was first reported by Wadhwa et al
(17); it is encoded by the gene of
heat shock protein family A (Hsp70) member 9 and is involved in
multiple mitochondrial processes, including maintenance of
mitochondrial protein integrity, biogenesis, energy metabolism and
translocation of cytosolic protein (20). Overexpression of mortalin has been
detected in numerous types of malignant tumor (22–24). In
the present study, it was confirmed that the expression of mortalin
was significantly increased in ICC tissues compared with
corresponding peritumoral tissues. Recent studies have demonstrated
that high levels of mortalin expression are associated with a
relatively poor prognosis in pancreatic cancer (23), non-small cell lung cancer (24) and hepatocellular carcinoma (30). The present study demonstrated that the
expression of mortalin was an independent predictor of OS rate and
cumulative recurrence in patients with ICC, which is consistent
with previous research (29).
Mortalin has been suggested to be a more efficient index than lymph
node metastasis for evaluating the prognosis of gastric cancer
patients (31). Previous studies have
indicated that mortalin may interact with apoptosis-associated
proteins, including p53, cyclin-dependent kinase 11p60,
Bcl-2, Bcl-xL and p66Shc, to inhibit apoptosis in various types of
tumors (20,21). Mortalin binds to p53 to form a complex
that insulates p53 in the cytoplasm and prevents its
transcriptional activation (32).
Furthermore, a previous study demonstrated that the downregulation
of mortalin expression markedly promoted apoptosis in ICC cell
lines (29). This was supported by
fact that malignant histopathological features, including lymphatic
metastasis, multiple tumors, poor differentiation and high TNM
stage, were more frequently observed in high mortalin expression
ICC tissues compared with those in low mortalin expression tissues.
In view of these results, it is concluded that high expression of
mortalin is associated with tumor progression and malignant ICC
phenotypes, and may be a prognostic indicator for ICC patients.
In the present study, Bcl-2 expression was markedly
increased in ICC tissues compared with adjacent peritumoral
tissues. The expression of Bax was significantly decreased in ICC
tissues. Furthermore, the expression of mortalin in ICC patients
was positively correlated with the expression of Bcl-2 and
negatively correlated with the expression of Bax. Multiple linear
regression analysis also indicated a close association between
mortalin and Bcl-2 expression in ICC patient tissues. High
expression of Bcl-2 and low expression of Bax were demonstrated to
be associated with malignant phenotypes, which may be due to the
role of Bcl-2 and Bax in the intrinsic apoptotic pathway. It has
been previously indicated that the interaction of Bcl-2 and Bcl-xL
with mortalin interferes with mortalin-p53 interaction,
inactivating p53 function and inducing cancer cell apoptosis
(21). Activation of p53 can trigger
the activation of pro-apoptotic genes, including Bax (33), and allows mitochondrial proteins, such
as Bcl-2, to regulate apoptosis (34). The overexpression of mortalin directly
abrogates the transcriptional activation of p53 (35). Further investigation regarding the
associations between mortalin and Bcl-2 or Bax in patients with ICC
would be beneficial to improve therapeutic strategy and to identify
prognostic markers. Importantly, ICC patients expressing a low
level of Bax or a high level of Bcl-2 were associated with a
relatively poor prognosis.
Cox regression analysis indicated that Bcl-2 was an
independent predictor of ICC prognosis, while Bax was not suitable
as a predictor. Evaluation of the combinatorial effects of the 3
markers revealed that the subgroup presenting with high mortalin
and Bcl-2 expression and low Bax expression had the worst prognosis
of all ICC patients examined. However, the present study was
limited by only investigating ICC tissues from patients who were
diagnosed and treated at a single hospital.
In conclusion, mortalin and Bcl-2 overexpression
and/or the low expression of Bax are implicated in the
anti-apoptotic effect and tumor progression of ICC. Mortalin or
Bcl-2 expression, or a combination of mortalin, Bcl-2 and Bax
expression may be used to predict the prognosis of ICC, as well as
being potential therapeutic targets.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (grant nos. 81260084 and 81472840), the
Scientific Research Foundation of the Education Department of
Yunnan Province (grant no. 2017YJS079) and the Alliance Special
Foundation of Kunming Medical University (grant no. 2015FB056).
Glossary
Abbreviations
Abbreviations:
|
ICC
|
intrahepatic cholangiocarcinoma
|
|
Bcl-2
|
B-cell lymphoma 2
|
|
Bax
|
Bcl-2-like protein 4
|
|
IHC
|
immunohistochemistry
|
|
OS
|
overall survival
|
|
HCC
|
hepatocellular carcinoma
|
|
TNM
|
tumor-node-metastasis
|
|
GGT
|
γ-glutamyl transpeptidase
|
|
CEA
|
carcinoembryonic antigen
|
|
CA19-9
|
carbohydrate antigen 19-9
|
References
|
1
|
Rahnemai-Azar AA, Weisbrod AB, Dillhoff M,
Schmidt C and Pawlik TM: Intrahepatic cholangiocarcinoma: Current
management and emerging therapies. Expert Rev Gastroenterol
Hepatol. 11:439–449. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lubezky N, Facciuto M, Harimoto N,
Schwartz ME and Florman SS: Surgical treatment of intrahepatic
cholangiocarcinoma in the USA. J Hepatobiliary Pancreat Sci.
22:124–130. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yamashita S, Koay EJ, Passot G, Shroff R,
Raghav KP, Conrad C, Chun YS, Aloia TA, Tao R, Kaseb A, et al:
Local therapy reduces the risk of liver failure and improves
survival in patients with intrahepatic cholangiocarcinoma: A
comprehensive analysis of 362 consecutive patients. Cancer.
123:1354–1362. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Buettner S, van Vugt JL, IJzermans JN and
Koerkamp B Groot: Intrahepatic cholangiocarcinoma: Current
perspectives. Onco Targets Ther. 10:1131–1142. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang H, Yang T, Wu M and Shen F:
Intrahepatic cholangiocarcinoma: Epidemiology, risk factors,
diagnosis and surgical management. Cancer Lett. 379:198–205. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Oliveira DV, Zhang S, Chen X, Calvisi DF
and Andersen JB: Molecular profiling of intrahepatic
cholangiocarcinoma: The search for new therapeutic targets. Expert
Rev Gastroenterol Hepatol. 11:349–356. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Si A, Li J, Xing X, Lei Z, Xia Y, Yan Z,
Wang K, Shi L and Shen F: Effectiveness of repeat hepatic resection
for patients with recurrent intrahepatic cholangiocarcinoma:
Factors associated with long-term outcomes. Surgery. 161:897–908.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Reed JC: Bcl-2 and the regulation of
programmed cell death. J Cell Biol. 124:1–6. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hatok J and Racay P: Bcl-2 family
proteins: Master regulators of cell survival. Biomol Concepts.
7:259–270. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Thomas S, Quinn BA, Das SK, Dash R, Emdad
L, Dasgupta S, Wang XY, Dent P, Reed JC, Pellecchia M, et al:
Targeting the Bcl-2 family for cancer therapy. Expert Opin Ther
Targets. 17:61–75. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kelly PN and Strasser A: The role of Bcl-2
and its pro-survival relatives in tumourigenesis and cancer
therapy. Cell Death Differ. 18:1414–1424. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ermiah E, Buhmeida A, Khaled BR, Abdalla
F, Salem N, Pyrhönen S and Collan Y: Prognostic value of bcl-2
expression among women with breast cancer in Libya. Tumour Biol.
34:1569–1578. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Casneuf VF, Fonteyne P, Van Damme N,
Demetter P, Pauwels P, de Hemptinne B, De Vos M, Van de Wiele C and
Peeters M: Expression of SGLT1, Bcl-2 and p53 in primary pancreatic
cancer related to survival. Cancer Invest. 26:852–859. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Brady HJ and Gil-Gόmez G: Bax. The
pro-apoptotic Bcl-2 family member, Bax. Int J Biochem Cell Biol.
30:647–650. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu Z, Ding Y, Ye N, Wild C, Chen H and
Zhou J: Direct activation of bax protein for cancer therapy. Med
Res Rev. 36:313–341. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gross A, Jockel J, Wei MC and Korsmeyer
SJ: Enforced dimerization of BAX results in its translocation,
mitochondrial dysfunction and apoptosis. EMBO J. 17:3878–3885.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wadhwa R, Kaul SC, Ikawa Y and Sugimoto Y:
Identification of a novel member of mouse hsp70 family. Its
association with cellular mortal phenotype. J Biol Chem.
268:6615–6621. 1993.PubMed/NCBI
|
|
18
|
Kaul SC, Deocaris CC and Wadhwa R: Three
faces of mortalin: A housekeeper, guardian and killer. Exp
Gerontol. 42:263–274. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wadhwa R, Yaguchi T, Hasan MK, Mitsui Y,
Reddel RR and Kaul SC: Hsp70 family member, mot-2/mthsp70/GRP75,
binds to the cytoplasmic sequestration domain of the p53 protein.
Exp Cell Res. 274:246–253. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Londono C, Osorio C, Gama V and Alzate O:
Mortalin, apoptosis, and neurodegeneration. Biomolecules.
2:143–164. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Saxena N, Katiyar SP, Liu Y, Grover A, Gao
R, Sundar D, Kaul SC and Wadhwa R: Molecular interactions of Bcl-2
and Bcl-xL with mortalin: Identification and functional
characterization. Biosci Rep. 33:e000732013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Na Y, Kaul SC, Ryu J, Lee JS, Ahn HM, Kaul
Z, Kalra RS, Li L, Widodo N, Yun CO and Wadhwa R: Stress chaperone
mortalin contributes to epithelial-mesenchymal transition and
cancer metastasis. Cancer Res. Mar 9–2016.(Epub ahead of print).
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cui X, Li Z, Piao J, Li J, Li L, Jin A and
Lin Z: Mortalin expression in pancreatic cancer and its clinical
and prognostic significance. Hum Pathol. 64:171–178. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sun J, Che SL, Piao JJ, Xu M, Chen LY and
Lin ZH: Mortalin overexpression predicts poor prognosis in early
stage of non-small cell lung cancer. Tumour Biol.
39:10104283176959182017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Huang XY, Zhang C, Cai JB, Shi GM, Ke AW,
Dong ZR, Zhang PF, Fan J, Peng BG and Zhou J: Comprehensive
multiple molecular profile of epithelial mesenchymal transition in
intrahepatic cholangiocarcinoma patients. PLoS One. 9:e968602014.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Talwalkar JA, Seaberg E, Kim WR and
Wiesner RH: Predicting clinical and economic outcomes after liver
transplantation using the Mayo primary sclerosing cholangitis model
and Child-Pugh score. National institutes of diabetes and digestive
and kidney diseases liver transplantation database group. Liver
Transpl. 6:753–758. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wittekind C: Pitfalls in the
classification of liver tumors. Pathologe. 27:289–293. 2006.(In
German). View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kang Q, Cai JB, Dong RZ, Liu LX, Zhang C,
Zhang PF, Zou H, Xie N, Zhang L, Zhang XY, et al: Mortalin promotes
cell proliferation and epithelial mesenchymal transition of
intrahepatic cholangiocarcinoma cells in vitro. J Clin Pathol.
70:677–683. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen J, Liu WB, Jia WD, Xu GL, Ma JL,
Huang M, Deng YR and Li JS: Overexpression of Mortalin in
hepatocellular carcinoma and its relationship with angiogenesis and
epithelial to mesenchymal transition. Int J Oncol. 44:247–255.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ando K, Oki E, Zhao Y, Ikawa-Yoshida A,
Kitao H, Saeki H, Kimura Y, Ida S, Morita M, Kusumoto T and Maehara
Y: Mortalin is a prognostic factor of gastric cancer with normal
p53 function. Gastric Cancer. 17:255–262. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wadhwa R, Takano S, Robert M, Yoshida A,
Nomura H, Reddel RR, Mitsui Y and Kaul SC: Inactivation of tumor
suppressor p53 by mot-2, a hsp70 family member. J Biol Chem.
273:29586–29591. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang J, Huang K, O'Neill KL, Pang X and
Luo X: Bax/Bak activation in the absence of Bid, Bim, Puma, and
p53. Cell Death Dis. 7:e22662016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Galluzzi L, Morselli E, Kepp O, Tajeddine
N and Kroemer G: Targeting p53 to mitochondria for cancer therapy.
Cell Cycle. 7:1949–1955. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Grover A, Priyandoko D, Gao R, Shandilya
A, Widodo N, Bisaria VS, Kaul SC, Wadhwa R and Sundar D: Withanone
binds to mortalin and abrogates mortalin-p53 complex: Computational
and experimental evidence. Int J Biochem Cell Biol. 44:496–504.
2012. View Article : Google Scholar : PubMed/NCBI
|