Introduction
Hepatocellular carcinoma (HCC) is a leading cause of
cancer-associated mortality worldwide. In 2012, there were ~782,500
new cases and ~745,500 incidences of mortality owing to liver
cancer, with China alone making up ~50% of this number (1). One issue in HCC management frequently
confronted by hepatologist is the accurate prediction of survival
outcome, which is necessary in order to provide optimal medical
care. A number of staging systems, including clinical
Tumor-Node-Metastasis (TNM) stage (2), Cancer of the Liver Italian Program
(CLIP) (3) and Barcelona Clinic Liver
Cancer (BCLC) (4), are used to
predict the prognosis of HCC and stratify patients for treatment.
However, patient outcome may be associated not only with disease
stage, but also with biological factors. With recent developments
in the fields of genomics and proteomics, more relevant prognostic
factors are yet to be identified to improve the prognostic strategy
of HCC.
In previous genome-wide microarray analysis, a
series of genes, including ATP-dependent DNA helicase Q4 (RECQL4),
disks large-associated protein 5 (5)
and family with sequence similarity 83 member D (6), were significantly upregulated in HCC
tissues. RECQL4, as one of the human DNA helicases, serves a
critical role in genomic instability and aging processes (7). Genome instability is deemed to have an
important part in the multistep development of human cancer
(8). Furthermore, interaction has
been observed between RECQL4 and proteins involved in genome
surveillance (9). Previous studies
have demonstrated that mutations in RECQL4 cause three autosomal
recessive diseases, Rothmund-Thomson, Rapadilino and Baller-Gerold
syndromes (10–12). The potential for unlimited replication
is a hallmark of cancer cells (8).
RECQL4 serves an essential role in the initiation of DNA
replication (13–15) and is directly or indirectly involved
in multiple DNA repair pathways, through interactions with diverse
repair proteins (16–18). Several studies have revealed that
increased RECQL4 expression is observed in sporadic osteosarcoma,
prostate carcinogenesis and breast tumorigenesis (19–21).
Therefore, the role of RECQL4 in human cancer, including HCC,
necessitates further investigation.
The aims of the present study were to detect RECQL4
expression in HCC tissue, evaluate the association between RECQL4
expression and patient clinicopathological features and the
prognostic significance of RECQL4 expression in HCC.
Materials and methods
Specimens
A total of 205 pairs of fresh HCC tissues and
corresponding adjacent normal liver tissues (ANLT) were obtained
from HCC patients who underwent radical curative surgery at the
Affiliated Hospital of Guilin Medical University (Guilin, China)
between March 2001 and September 2007. The mean age of the patients
was 50.22 years (range, 21–74 years). The diagnosis of HCC was
based on the results of clinical symptoms, serological,
ultrasonography (US), computed tomography, magnetic resonance
imaging, pathological examination, according to the primary liver
cancer clinical diagnosis and staging criteria. The baseline
information, shown in Table I,
includes age, gender, family history, hepatitis B surface antigen
(HBsAg), a-fetoprotein (AFP), cirrhosis, tumor size and number,
BCLC disease stage, metastasis and recurrence. All samples were
snap-frozen in liquid nitrogen and stored at −80°C immediately
following surgical resection. The inclusion criteria of the present
study were as follows: i) Samples were confirmed to be HCC by
pathological examination, and the patients underwent radical
resection; ii) all patients enrolled have complete background
information and follow-up records, including periodic review of
liver function, AFP value, imaging information, recurrence time and
treatment regimen. Patients diagnosed with cholangiocarcinoma or
those that suffered perioperative mortality or with incomplete
clinical data were excluded. Additionally, patients who suffered
from infectious diseases, autoimmune disease, hematologic disease
or used drugs that affect the hematopoietic system within 1 month
prior to starting treatment, HIV-positive patients and those who
lost contact in the follow-up period were excluded.
 | Table I.Association between
clinicopathological characteristics and RECQL4 mRNA expression in
HCC. |
Table I.
Association between
clinicopathological characteristics and RECQL4 mRNA expression in
HCC.
|
|
| RECQL4
expression |
|
|
|---|
|
|
|
|
|
|
|---|
| Variable | Patients, n | Low, n (%) | High, n (%) | χ2 | P-value |
|---|
| Age, years |
|
|
| 0.448 | 0.503 |
| ≤55 | 138 | 41 (29.7) | 97
(70.3) |
|
|
|
>55 | 67 | 23 (34.3) | 44
(65.7) |
|
|
| Sex |
|
|
| 0.892 | 0.345 |
| Male | 172 | 56 (32.6) | 116 (67.4) |
|
|
|
Female | 33 | 8
(24.2) | 25
(75.8) |
|
|
| Family history |
|
|
| 0.082 | 0.775 |
| No | 172 | 53 (30.8) | 119 (69.2) |
|
|
|
Yes | 33 | 11 (33.3) | 22
(66.7) |
|
|
| Alcohol
consumption |
|
|
| 0.554 | 0.457 |
| No | 101 | 34 (33.7) | 67
(66.3) |
|
|
|
Yes | 104 | 30 (28.8) | 74
(71.2) |
|
|
| HBsAg |
|
|
| 1.454 | 0.228 |
|
Negative | 41 | 16 (39.0) | 25
(61.0) |
|
|
|
Positive | 164 | 48 (29.3) | 116 (70.7) |
|
|
| AFP, ng/ml |
|
|
| 4.246 | 0.039 |
|
≤100 | 75 | 30 (40.0) | 45
(60.0) |
|
|
|
>100 | 130 | 34 (26.2) | 96
(73.8) |
|
|
| Cirrhosis |
|
|
| 2.715 | 0.099 |
| No | 20 | 3
(15.0) | 17
(85.0) |
|
|
|
Yes | 185 | 61 (33.0) | 124 (67.0) |
|
|
| Tumor size, cm |
|
|
| 7.852 | 0.005 |
| ≤6 | 89 | 37 (41.6) | 52
(58.4) |
|
|
|
>6 | 116 | 27 (23.3) | 89
(76.7) |
|
|
| Tumor number |
|
|
| 0.509 | 0.475 |
|
Single | 137 | 45 (32.8) | 92
(67.2) |
|
|
|
Multiple | 68 | 19 (27.9) | 49
(72.1) |
|
|
| BCLC stage |
|
|
| 6.293 | 0.012 |
|
0-A | 92 | 37 (40.2) | 55
(59.8) |
|
|
|
B-C | 113 | 27 (23.9) | 86
(76.1) |
|
|
| Metastasis |
|
|
| 0.789 | 0.374 |
| No | 176 | 57 (32.4) | 119 (67.6) |
|
|
|
Yes | 29 | 7
(24.1) | 22
(75.9) |
|
|
| Recurrence |
|
|
| 1.737 | 0.188 |
| No | 135 | 38 (28.1) | 97
(71.9) |
|
|
|
Yes | 70 | 26 (37.1) | 44
(62.9) |
|
|
The present study was approved by the Ethics
Committee of The Affiliated Hospital of Guilin Medical University
(Guilin, China) and complies with the Ethical Guidelines of the
Declaration of Helsinki. All patients provided written informed
consent prior to investigation.
Following surgical resection, the patients with HCC
received long-term follow-up via monitoring of serum AFP levels and
US examination every 2 months, a chest radiograph every 6 months
during the first 2 postoperative years and at 3–6-month intervals
thereafter. Computerized tomography or magnetic resonance imaging
would be performed if the result of AFP test or US examination were
abnormal. Disease-free survival (DFS) time was measured from the
date of surgery to the date of recurrence, metastasis, mortality or
the last follow-up. Overall survival (OS) time was measured from
the date of surgery to the date of death or last follow-up.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA was extracted from HCC frozen tissue
samples using TRIzol (Invitrogen; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA) reagent, and cDNA was synthesized by using
PrimeScript RT reagent kit (Takara Bio, Inc., Otsu, Japan)
according to the manufacturer's instructions. The temperature
protocol of reverse transcription was as follows: 42°C for 2 min in
order to remove the contamination of genomic DNA, then reverse
transcription at 37°C for 15 min and 85°C for 5 sec. qPCR analysis
was performed using SYBR Premix Ex Taq (Takara Bio, Inc., Otsu,
Japan), according to the manufacturer's instructions. Each well was
mixed with 15 µl Master Mix (SYBR® Green PCR Master Mix;
Applied Biosystems; Thermo Fisher Scientific, Inc.). The protocol
was performed with an initial denaturation step at 95°C for 10 min,
followed by 40 cycles of denaturation at 95°C for 2 sec, annealing
at 55°C for 5 sec and extension at 72°C for 15 sec. The sequences
of the primers used were: RECQL4 (158 bp) forward,
5′-TCAACATGAAGCAGAAACACTAC-3′ and reverse,
5′-CTGCTCGTTCAGGAAACAAGACT-3′; and β-actin (142 bp) forward,
5′-GACAGGATGCAGAAGGAGATTACT-3′ and reverse,
5′-TGATCCACATCTGCTGGAAGGT-3′. The levels of RECQL4 were normalized
to the levels of β-actin expression using the 2−ΔΔCq
methodas reported by Livak and Schmittgen (22).
Statistical analysis
All quantitative data are expressed as the mean ±
standard deviation and were analyzed using an independent t-test.
Categorical variables were compared using χ2 test. The
DFS and OS rates were calculated using the Kaplan-Meier method, and
comparisons of survival curves between groups were assessed with
log-rank test. Multivariate analysis was performed using the Cox
proportional hazards model, and only variables that were
statistically significant in univariate analysis were included in
this model. All statistical analyses were performed using SPSS13.0
statistical software (SPSS, Inc., Chicago, IL, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
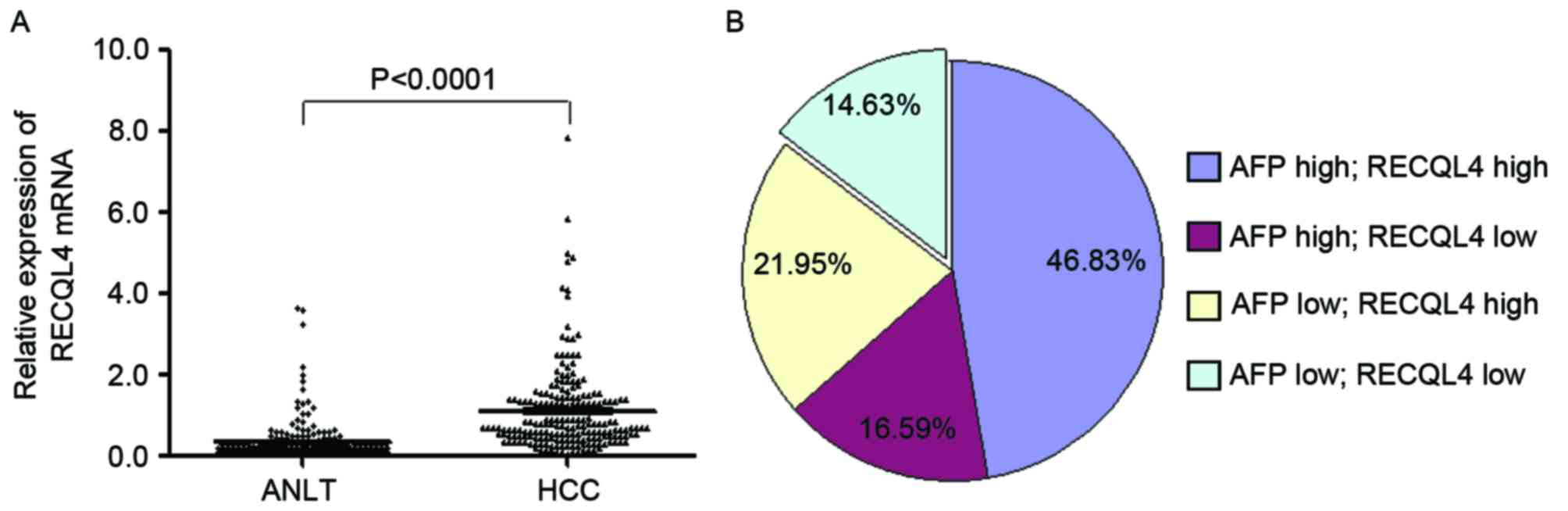
Expression of RECQL4 mRNA is
upregulated in human HCC tissues
RECQL4 mRNA expression was examined in 205 samples
of fresh HCC tissues and their corresponding ANLT by RT-qPCR. As
shown in Fig. 1A, the relative
expression of RECQL4 mRNA in HCC cancer tissues (1.10±0.07) was
significantly higher compared with ANLT (0.33±0.04) when normalized
to β-actin (P<0.001). The RECQL4 mRNA levels were increased in
141 cases (68.8%), but decreased in 64 cases (31.2%). Notably, the
upregulation of RECQL4 mRNA expression and the increase of serum
AFP levels did not completely overlap. High RECQL4 expression along
with high serum AFP level was detected in 96 cases (46.83%), high
serum AFP level alone was detected in 34 cases (16.59%), and
upregulation of RECQL4 but not AFP was detected in 45cases (21.95%;
Fig. 1B). These results indicated
that RECQL4 might be a novel histological biomarker for HCC. When
these two markers were combined, the HCC diagnosis rate was
increased to 85.37%.
Association between RECQL4 mRNA and
clinical pathological characteristics of HCC
To further investigate the association between
RECQL4 mRNA expression and clinicopathological parameters of HCC,
the characteristics of the 205 HCC patients were analyzed. As shown
in Table I, the level of RECQL4 mRNA
expression was positively associated with AFP level (>100 ng/ml)
(χ2=4.246, P=0.039), tumor size (>6 cm)
(χ2=7.852, P=0.005), and BCLC stage
(χ2=6.293, P=0.012), but was not associated with age
(>55 years), gender, family history, alcohol consumption, HBsAg
expression, liver cirrhosis, tumor number, metastasis or
postoperative recurrence (all P>0.05).
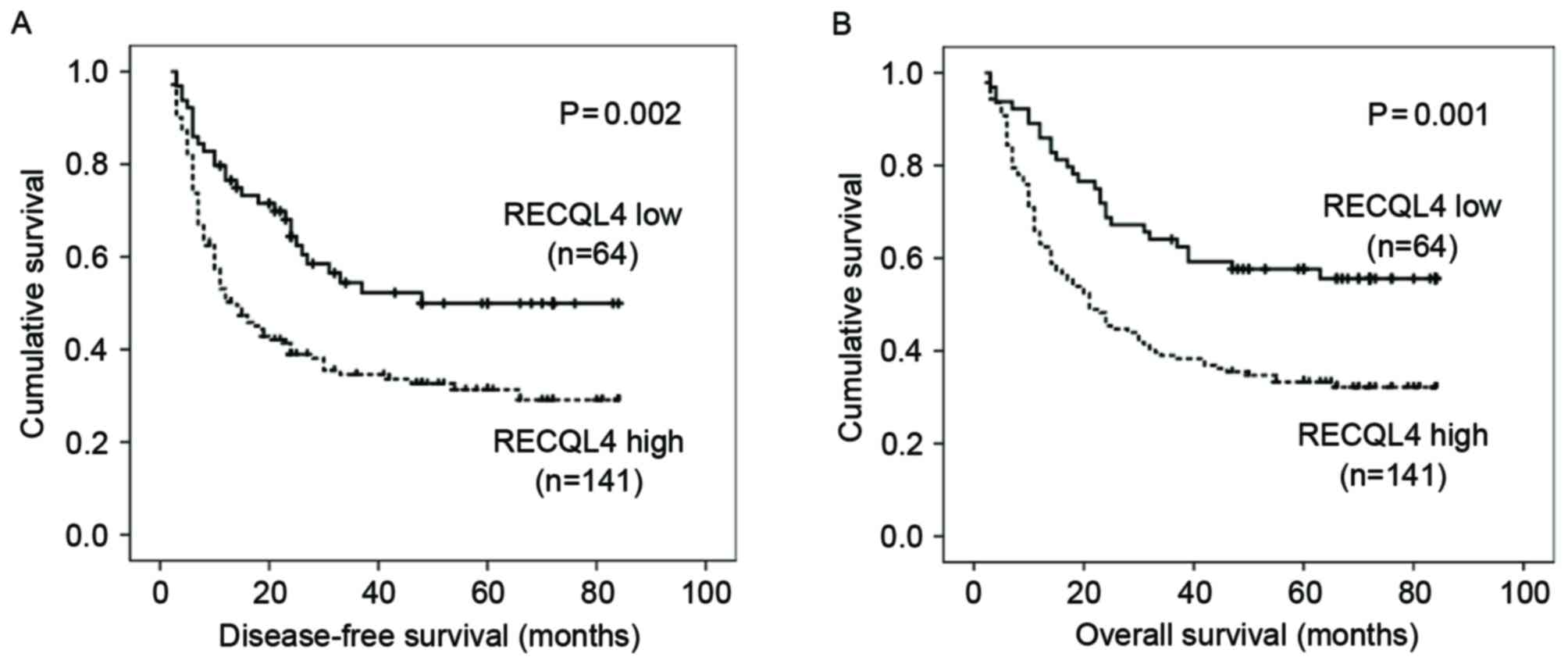
Univariate analysis of prognostic
factors of DFS and OS
Kaplan-Meier survival analysis revealed that
patients expressing high levels of RECQL4 mRNA had significantly
shorter DFS and OS times compared with those with low RECQL4 mRNA
expression (log-rank test: P=0.002, and P=0.001, respectively;
Fig. 2). Mean DFS and OS in the
high-RECQL4 mRNA expression group was 34.23 months [95% confidence
interval (CI), 28.42–40.03] and 38.37 months (95% CI, 32.84–43.90)
respectively, compared with 50.73 months (95% CI, 41.88–59.58) and
56.31 months (95% CI, 48.33–64.30) in the low-RECQL4 mRNA
expression group (P=0.002 and P=0.001, respectively; Table II). Apart from high RECQL4 mRNA
expression, other factors, including size of tumor (>6 cm),
multiple tumor number, stage B-C (according to BCLC staging) and
metastasis, were also strongly associated with a shorter DFS and
OS, and recurrence was associated with a shorter OS (Table II).
| Table II.Association between RECQL4 mRNA
expression, clinical parameters and disease-free/overall
survival. |
Table II.
Association between RECQL4 mRNA
expression, clinical parameters and disease-free/overall
survival.
|
|
| Disease-free
survival | Overall
survival |
|---|
|
|
|
|
|
|---|
| Clinical
characteristics | Patients, n | Mean, months | 95% CI | P-value | Mean, months | 95% CI | P-value |
|---|
| RECQL4 mRNA |
|
|
| 0.002 |
|
| 0.001 |
|
Low | 64 | 50.73 | 41.88–59.58 |
| 56.31 | 48.33–64.30 |
|
|
High | 141 | 34.23 | 28.42–40.03 |
| 38.37 | 32.84–43.90 |
|
| Age, years |
|
|
| 0.646 |
|
| 0.634 |
|
≤55 | 138 | 38.09 | 32.06–44.11 |
| 43.70 | 37.84–49.57 |
|
|
>55 | 67 | 40.68 | 32.17–49.19 |
| 45.85 | 37.62–54.08 |
|
| Sex |
|
|
| 0.299 |
|
| 0.141 |
|
Female | 33 | 45.30 | 31.98–58.63 |
| 53.41 | 41.20–65.62 |
|
|
Male | 172 | 37.82 | 32.53–43.10 |
| 42.81 | 37.63–47.50 |
|
| Family history |
|
|
| 0.155 |
|
| 0.115 |
| No | 172 | 37.20 | 31.90–42.50 |
| 42.85 | 37.65–48.06 |
|
|
Yes | 33 | 48.00 | 35.61–60.39 |
| 53.12 | 41.56–64.68 |
|
| Alcohol
consumption |
|
|
| 0.139 |
|
| 0.081 |
| No | 101 | 43.60 | 36.17–51.04 |
| 48.07 | 41.02–55.13 |
|
|
Yes | 104 | 34.88 | 28.50–41.26 |
| 40.51 | 34.20–46.81 |
|
| HBsAg |
|
|
| 0.652 |
|
| 0.616 |
|
Negative | 41 | 35.44 | 25.01–45.87 |
| 41.84 | 31.60–52.09 |
|
|
Positive | 164 | 39.74 | 34.18–45.30 |
| 44.61 | 39.30–49.93 |
|
| AFP, ng/ml |
|
|
| 0.200 |
|
| 0.209 |
|
≤100 | 75 | 42.88 | 35.17–50.58 |
| 48.09 | 40.94–55.24 |
|
|
>100 | 130 | 37.19 | 30.73–43.65 |
| 41.20 | 35.06–47.34 |
|
| Cirrhosis |
|
|
| 0.694 |
|
| 0.824 |
| No | 20 | 35.40 | 19.79–51.01 |
| 41.85 | 27.14–56.56 |
|
|
Yes | 185 | 39.23 | 34.05–44.14 |
| 44.24 | 39.27–49.21 |
|
| Tumor size, cm |
|
|
| <0.001 |
|
| <0.001 |
| ≤6 | 89 | 57.76 | 50.66–64.85 |
| 62.66 | 56.55–68.77 |
|
|
>6 | 116 | 25.25 | 19.59–30.91 |
| 29.59 | 24.04–35.14 |
|
| Tumor number |
|
|
| <0.001 |
|
| <0.001 |
|
Single | 137 | 44.85 | 38.77–50.92 |
| 50.84 | 45.03–56.65 |
|
|
Multiple | 68 | 26.57 | 19.03–34.11 |
| 31.75 | 24.25–39.25 |
|
| BCLC stage |
|
|
| <0.001 |
|
| <0.001 |
|
0-A | 92 | 54.29 | 47.04–61.54 |
| 60.09 | 53.47–66.72 |
|
|
B-C | 113 | 26.41 | 20.70–32.12 |
| 31.76 | 25.94–37.58 |
|
| Metastasis |
|
|
| 0.023 |
|
| 0.048 |
| No | 176 | 41.15 | 35.76–46.53 |
| 45.63 | 40.51–50.75 |
|
|
Yes | 29 | 23.56 | 14.71–32.42 |
| 34.12 | 22.84–45.39 |
|
| Recurrence |
|
|
|
|
|
| <0.001 |
| No | 135 |
|
|
| 34.55 | 28.81–40.28 |
|
|
Yes | 70 |
|
|
| 63.22 | 56.70–69.75 |
|
Multivariate analysis of independent
predictors on DFS and OS
To evaluate the predictive roles of these factors in
HCC prognosis further (other than recurrence factor, which was
measured only for OS), high RECQL4 mRNA expression and other
clinical pathological parameters [size of tumor (>6 cm),
multiple tumor number, BCLC stage B-C and metastasis] that were
identified to be statistically significant by univariate analysis
were analyzed using the multivariate Cox proportional hazards model
for DFS and OS. Cox multivariate analysis revealed that high RECQL4
mRNA expression (HR, 1.635; 95% CI, 1.062–2.515; P=0.025), as well
as size of tumor (>6 cm) (HR, 2.670; 95% CI, 1.704–4.183;
P<0.001), BCLC stage B-C (HR, 1.835; 95% CI, 1.116–3.018;
P=0.017) were independent predictors for DFS (Table III). High RECQL4 mRNA expression
(HR, 1.618; 95% CI, 1.050–2.493; P=0.029), size of tumor (>6 cm)
(HR, 2.536; 95% CI, 1.621–3.967; P<0.001), BCLC stage B-C
(HR,1.679; 95% CI, 1.128–2.760; P=0.041) and disease recurrence
(HR, 2.832; 95% CI, 1.827–4.391; P<0.001) were independent
predictors for OS (Table III).
| Table III.Cox multivariate proportional hazards
model of independent predictors on disease-free and overall
survival. |
Table III.
Cox multivariate proportional hazards
model of independent predictors on disease-free and overall
survival.
| A, Disease-free
survival |
|---|
|
|---|
| Parameter | HR (95% CI) | P-value |
|---|
| Tumor size, cm (≤6
vs. >6 cm) | 2.670
(1.704–4.183) | <0.001 |
| Tumor number
(single vs. multiple) | 1.092
(0.692–1.723) | 0.707 |
| Metastasis (no vs.
yes) | 1.116
(0.685–1.816) | 0.660 |
| BCLC stage (0-A vs.
B-C) | 1.835
(1.116–3.018) | 0.017 |
| RECQL4 mRNA (low
vs. high) | 1.635
(1.062–2.515) | 0.025 |
|
| B, Overall
survival |
|
|
Parameter | HR (95%
CI) | P-value |
|
| Tumor size, cm (≤6
vs. >6 cm) | 2.536
(1.621–3.967) | <0.001 |
| Tumor number
(single vs. multiple) | 1.033
(0.652–1.637) | 0.890 |
| Metastasis (no vs.
yes) | 1.212
(0.742–1.981) | 0.443 |
| BCLC stage (0-A vs.
B-C) | 1.679
(1.021–2.760) | 0.041 |
| Recurrence (no vs.
yes) | 2.832
(1.827–4.391) | <0.001 |
| RECQL4 mRNA (low
vs. high) | 1.618
(1.050–2.493) | 0.029 |
Discussion
RECQL4 expression is associated with cancer-prone
syndromes and premature aging. RECQL4 shares homology in its
N-terminal domain with the yeast replication initiation protein
Sld2, which participates in DNA replication initiation (13–15,23,24).
Unlimited replicative potential is a hallmark of HCC cells. In the
present study, the expression of RECQL4 mRNA was investigated in
HCC tissues, and RECQL4 mRNA was found to be highly expressed in
liver cancer tissues compared with ANLT. Similar to other
oncogenes, overexpression of RECQL4 may confer an unlimited
proliferative potential to hepatoma cells and promote
hepatocellular tumorigenesis (20,21).
The upregulation of RECQL4 mRNA expression in HCC
tissues was positively associated with serum AFP levels (>100
ng/ml). Despite being a recommended tumor marker for HCC screening,
detecting AFP alone is not optimal for the surveillance or
diagnosis of HCC, owing to its deficiencies in the sensitivity and
specificity of testing (25).
Therefore, the identification of novel molecular markers with
superior sensitivity and specificity is urgently required. The
present study indicated that RECQL4 maybe a potential novel
biomarker for HCC diagnosis, and the positive rate of HCC diagnosis
may be improved to 85.37% by detecting a combination of AFP and
RECQL4. In addition, the increase in the level of RECQL4 mRNA
expression was also positively associated with large tumor size
(>6 cm) and stage B-C disease. Therefore, the authors
hypothesize that RECQL4 contributes to malignant progression of
HCC.
Under univariate analysis, high RECQL4 expression,
tumor size >6 cm, multiple tumor nodules, metastasis and stage
B-C disease were identified to associate with poor DFS and OS times
of HCC patients. Large tumors (>5 cm) and multiple tumors are
more closely associated with bilobar tumor involvement, tumor
invasion of adjacent organs, microvascular invasion and
histologically positive margins (26). In addition, tumor size (>5 cm) and
multinodular disease were reported to significantly increase the
risk of postoperative recurrence (26–28). The
data from the present study demonstrated that intermediate and
advanced BCLC stage is predictive of a poorer prognosis for HCC
patients following surgical resection. For HCC patients who
received no anticancer treatment, the severity of the BCLC stage is
strongly consistent with a poorer median survival as well (29). Notably, high RECQL4 mRNA expression in
HCC patients was also predictive of a significantly shorter
survival compared with patients with low RECQL4 expression. These
clinical data suggest that RECQL4 maybe a useful prognostic marker
for HCC.
In the present study, notable predictive factors of
survival for HCC were identified. High RECQL4 expression, size of
tumor >6 cm, and stage B-C disease were shown to be independent
predictors of DFS and OS for HCC patients. Large tumor size (>5
cm) has been consistently shown to be an independent prognostic
marker in HCC patients (30,31). Generally, HCC patients with larger
tumors (>6 cm) have a poorer prognosis. Since an inaccurate
prediction can bring about severe harm to patients, as independent
predictors for the outcomes of HCC, the expression of RECQL4, tumor
size and BCLC stage can aid hepatologists in providing more
accurate prognosis predictions, improved risk assessment assessing
and in planning therapeutic trials.
In conclusion, the results of the current study
found that the expression of RECQL4 mRNA was significantly higher
in HCC tissue compared with adjacent normal liver tissues. Whether
the upregulation of RECQL4 expression contributes to
hepatocarcinogenesis will be a key research question to be
investigated in future experiments. It may be possible to use
RECQL4 as a novel biomarker for HCC diagnosis. This retrospective
study also provides evidence that RECQL4 may serve as an
independent predictor of prognosis for HCC patients. Furthermore,
targeting RECQL4 may provide a promising strategy for the treatment
of HCC patients with high RECQL4 expression. However, further
research is required to elucidate the underlying molecular
mechanism of HCC.
Acknowledgements
The present study was supported in part by grants
from the National Natural Science Foundation of China (grant no.
81773148), and the Innovation and Entrepreneurship Project of
University Students in Guangxi (grant nos. 201610598047 and
201610601006).
Glossary
Abbreviations
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
HR
|
hazard ratios
|
|
CI
|
confidence intervals
|
|
DFS
|
disease-free survival
|
|
OS
|
overall survival
|
|
TNM
|
tumor-node-metastasis
|
|
BCLC
|
Barcelona Clinic Liver Cancer
|
|
AFP
|
α-fetoprotein
|
|
HBsAg
|
hepatitis B surface antigen
|
|
ANLT
|
adjacent noncancerous liver
tissues
|
|
RT-qPCR
|
reverse transcription-quantitative
polymerase chain reaction
|
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Greene FL, Page DL, Fleming ID, Fritz AG,
Balch CM, Haller DG and Morrow M: AJCC Cancer Staging Manual. 6th.
Springer; Chicago, IL: 2002, View Article : Google Scholar
|
|
3
|
A new prognostic system for hepatocellular
carcinoma: A retrospective study of 435 patients: The Cancer of the
Liver Italian Program (CLIP) investigators. Hepatology. 28:751–755.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Llovet JM, Brú C and Bruix J: Prognosis of
hepatocellular carcinoma: The BCLC staging classification. Semin
Liver Dis. 19:329–338. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liao W, Liu W, Yuan Q, Liu X, Ou Y, He S,
Yuan S, Qin L, Chen Q, Nong K, et al: Silencing of DLGAP5 by siRNA
significantly inhibits the proliferation and invasion of
hepatocellular carcinoma cells. PLoS One. 8:e807892013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liao W, Liu W, Liu X, Yuan Q, Ou Y, Qi Y,
Huang W, Wang Y and Huang J: Upregulation of FAM83D affects the
proliferation and invasion of hepatocellular carcinoma. Oncotarget.
6:24132–24147. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Croteau DL, Singh DK, Hoh Ferrarelli L, Lu
H and Bohr VA: RECQL4 in genomic instability and aging. Trends
Genet. 28:624–631. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Petkovic M, Dietschy T, Freire R, Jiao R
and Stagljar I: The human Rothmund-Thomson syndrome gene product,
RECQL4, localizes to distinct nuclear foci that coincide with
proteins involved in the maintenance of genome stability. J Cell
Sci. 118:4261–4269. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kitao S, Shimamoto A, Goto M, Miller RW,
Smithson WA, Lindor NM and Furuichi Y: Mutations in RECQL4 cause a
subset of cases of Rothmund-Thomson syndrome. Nat Genet. 22:82–84.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Siitonen HA, Kopra O, Kääriäinen H,
Haravuori H, Winter RM, Säämänen AM, Peltonen L and Kestilä M:
Molecular defect of RAPADILINO syndrome expands the phenotype
spectrum of RECQL diseases. Hum Mol Genet. 12:2837–2844. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Van Maldergem L, Siitonen HA, Jalkh N,
Chouery E, De Roy M, Delague V, Muenke M, Jabs EW, Cai J, Wang LL,
et al: Revisiting sis-radial ray hypoplasia association:
Baller-Gerold syndrome caused by mutations in the RECQL4 gene. J
Med Genet. 43:148–152. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sangrithi MN, Bernal JA, Madine M,
Philpott A, Lee J, Dunphy WG and Venkitaraman AR: Initiation of DNA
replication requires the RECQL4 protein mutated in Rothmund-Thomson
syndrome. Cell. 121:887–898. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xu X and Liu Y: Dual DNA unwinding
activities of the Rothmund-Thomson syndrome protein, RECQ4. EMBO J.
28:568–577. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Collart C, Allen GE, Bradshaw CR, Smith JC
and Zegerman P: Titration of four replication factors is essential
for the Xenopus laevis midblastula transition. Science.
341:893–896. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fan W and Luo J: RecQ4 facilitates UV
light-induced DNA damage repair through interaction with nucleotide
excision repair factor xeroderma pigmentosum group A (XPA). J Biol
Chem. 283:29037–29044. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Schurman SH, Hedayati M, Wang Z, Singh DK,
Speina E, Zhang Y, Becker K, Macris M, Sung P, Wilson DM III, et
al: Direct and indirect roles of RECQL4 in modulating base excision
repair capacity. Hum Mol Genet. 18:3470–3483. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Singh DK, Karmakar P, Aamann M, Schurman
SH, May A, Croteau DL, Burks L, Plon SE and Bohr VA: The
involvement of human RECQL4 in DNA double-strand break repair.
Aging Cell. 9:358–371. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Maire G, Yoshimoto M, Chilton-MacNeill S,
Thorner PS, Zielenska M and Squire JA: Recurrent RECQL4 imbalance
and increased gene expression levels are associated with structural
chromosomal instability in sporadic osteosarcoma. Neoplasia.
11:260–268. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Su Y, Meador JA, Calaf GM, Proietti
De-Santis L, Zhao Y, Bohr VA and Balajee AS: Human RecQL4 helicase
plays critical roles in prostate carcinogenesis. Cancer Res.
70:9207–9217. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fang H, Nie L, Chi Z, Liu J, Guo D, Lu X,
Hei TK, Balajee AS and Zhao Y: RecQL4 helicase amplification is
involved in human breast tumorigenesis. PLoS One. 8:e696002013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zegerman P and Diffley JF: Phosphorylation
of Sld2 and Sld3 by cyclin-dependent kinases promotes DNA
replication in budding yeast. Nature. 445:281–285. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xu X, Rochette PJ, Feyissa EA, Su TV and
Liu Y: MCM10 mediates RECQ4 association with MCM2-7 helicase
complex during DNA replication. EMBO J. 28:3005–3014. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bruix J and Sherman M; American
Association for the Study of Liver Diseases, : Management of
hepatocellular carcinoma: An update. Hepatology. 53:1020–1022.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ng KK, Vauthey JN, Pawlik TM, Lauwers GY,
Regimbeau JM, Belghiti J, Ikai I, Yamaoka Y, Curley SA, Nagorney
DM, et al: Is hepatic resection for large or multinodular
hepatocellular carcinoma justified? Results from a
multi-institutional database. Ann Surg Oncol. 12:364–373. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kow AW, Kwon CH, Song S, Shin M, Kim JM
and Joh JW: Risk factors of peritoneal recurrence and outcome of
resected peritoneal recurrence after liver resection in
hepatocellular carcinoma: Review of 1222 cases of hepatectomy in a
tertiary institution. Ann Surg Oncol. 19:2246–2255. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ishizawa T, Hasegawa K, Aoki T, Takahashi
M, Inoue Y, Sano K, Imamura H, Sugawara Y, Kokudo N and Makuuchi M:
Neither multiple tumors nor portal hypertension are surgical
contraindications for hepatocellular carcinoma. Gastroenterology.
134:1908–1916. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Giannini EG, Farinati F, Ciccarese F,
Pecorelli A, Rapaccini GL, Di Marco M, Benvegnù L, Caturelli E,
Zoli M, Borzio F, et al: Prognosis of untreated hepatocellular
carcinoma. Hepatology. 61:184–190. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Liu PH, Hsu CY, Hsia CY, Lee YH, Su CW,
Huang YH, Lee FY, Lin HC and Huo TI: Prognosis of hepatocellular
carcinoma: Assessment of eleven staging systems. J Hepatol.
64:601–608. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gomaa AI, Hashim MS and Waked I: Comparing
staging systems for predicting prognosis and survival in patients
with hepatocellular carcinoma in Egypt. PLoS One. 9:e909292014.
View Article : Google Scholar : PubMed/NCBI
|