Introduction
Acute myocardial infarction (AMI) is a leading cause
for mortality worldwide, and coronary heart disease incidence,
which may lead to AMI, continues to trend upwards (1). The treatment guidelines for AMI include
percutaneous coronary intervention or thrombolytic treatment, which
contribute to the early reperfusion of the ischemic region;
although these treatments may prevent a certain extent of
myocardial damage, an ischemia/reperfusion (IR) injury may occur,
resulting in the loss of cardiac function and cardiomyocyte death
(2,3).
Reducing the extent of IR injury will aid in the improvement of the
therapy for AMI.
Visnagin,
4-methoxy-7-methyl-5H-furo[3,2-g][1]benzopyran-5-one, is extracted
from the fruit of Ammi visnaga. Visnagin and related
compounds, including khellin and visnadin, are used to treat angina
pectoris as they exhibit peripheral and coronary vasodilatation
activity (4). Visnagin also can
inhibit blood vessel contraction and decrease blood pressure
through inhibiting Ca2+ channels to prevent calcium
influx into the cell (5). It was
previously reported that visnagin could prevent oxalate-induced
cell death in renal epithelial cells; it also exerted an
anti-inflammatory effect on lipopolysaccharide (LPS)-stimulated
cells and a neuroprotective effect against kainic acid (KA)-induced
neuronal death (6). However, the
cardioprotective effect of visnagin for cardiomyocytes in IR injury
has not been demonstrated.
In recent years, nanotechnology has been developed
and applied in the treatment of various diseases.
Nanoparticle-based therapeutic systems, particularly drug delivery
systems, have become a popular research field due to their
targeting of functional zones to effectively deliver therapies
(7). Hydrogels are a drug delivery
system based on polymer-controlled release; temperature-sensitive
hydrogels are the most commonly researched for drug delivery.
N-isopropylacrylamide (NIPAAm) is a temperature-sensitive hydrogel,
its lower critical solution temperature (LCST) is 32°C; when the
temperature is below the LCST, it is in a liquid phase, and above
the LCST it is in a gel phase (8). To
improve the application of hydrogel, co-monomers, including
methacrylic acid (MAA), may be used so that hydrogels, including
NIPAAm-MAA, also exhibit a pH-responsive characteristic, which is a
pH value of ≥6.7 capable of triggering the pH-response (9). The continuous aggregation of NIPAAm-MAA
nanoparticles (NP) in the intercellular space of the IR region
contributes to the gel formation due to the temperature being
higher than that of the LCST, which ensures that the NP can
continuously aggregate in the IR region (10). Furthermore, the pH-responsive
characteristic of NP guarantees the NP can be solely decomposed in
the IR region, due to the pH value of IR region being >6.7, this
ensures the NP-encapsulated drugs can be released in the IR region
(11,12). Consequently NP may be an optimal drug
delivery system for the treatment of IR injury.
Autophagy is a cell-protective process in response
to stress. During the process of autophagy, bilayers on the area of
the rough endoplasmic reticulum without ribosomes surround
dysfunctional proteins and organelles to form the autophagosome,
then fuses with lysosomes to induce the release of lysosomal
enzymes, which degrade the contents of the autophagosome,
ultimately releasing metabolites for use by the cell (13,14).
In the present study, NIPAAm-MAA nanoparticles (NP)
loaded with visnagin were synthesized. Following IR injury, NP were
specifically transported to MI, where visnagin was released. The
heart function was improved and the infarct size was decreased.
Furthermore, light chain (LC) 3II expression and the number of
autophagosomes were increased, and apoptosis was inhibited.
Therefore, we hypothesize that NP may be the ideal drug delivery
system for targeted IR injury treatment, and visnagin may be a
novel drug for IR injury treatment.
Materials and methods
Synthesis of NIPAAm-MAA NP
NIPAAm-MAA NP were synthesized in 1,4-dioxane
solution through the free radical polymerization of monomers in an
N2 atmosphere. The ratio of NIPAAm to MAA was 8:0.5;
they were conjugated with 2-(dimethylamino) ethyl methacrylate
(DMAEMA). Benzoyl peroxide (BPO; 0.2 g) was added into the solution
to block the reaction; the nanoparticles were obtained at 70°C for
24 h in an N2 atmosphere and precipitated.
Scanning electron microscopy
(SEM)
The size, aggregation and shape of the NP were
observed with SEM. SEM was conducted with a high-resolution INSPECT
F50 (FEI; Thermo Fisher Scientific, Inc., Waltham, MA, USA). The NP
samples were dissolved in water (0.5 mg/ml), heated to 100°C, then
cooled to room temperature. Images of the NP were obtained through
SEM.
Drug-loaded NP
The nanoprecipitation method was used to prepare
visnagin-loaded NP (NP-visnagin) and fluorescein isothiocyanate
(FITC)-loaded NP (NP-FITC). Briefly, 100 mg lyophilized NP was
dissolved in 10 ml water and stirred. Visnagin (20 mg) was added
into the solution to be directly loaded into the NP. For the FITC
loading, 100 mg lyophilized NP were dissolved in 10 ml water and
stirred, FITC (10 mg) was then added into this solution. The
resultant solution was emulsified in polyvinyl alcohol (0.5 wt%)
and chitosan (2 wt%) solution and stirred at 20 × g using a
propeller-type agitator with four blades. Following solution
agitation for ~1 h, the entire suspension was centrifuged (4,000 ×
g for 20 min). The supernatant was removed and purified water (5
ml) was added to the sediment. This mixture was centrifuged again
to remove the excess polyvinyl alcohol and the unencapsulated
reagent. This process was then repeated and the resulting
NP-visnagin or NP-FITC was freeze-dried for 24 h and stored at
−20°C until subsequent use.
Drug release assay
The release conditions for NIPAAm-MAA NP were 37°C
and pH 5. NP-visnagin (8.5 mg) was dissolved in 30 ml
NaH2PO4-Na2HPO4
solution at 37°C. The release of visnagin over time was analyzed
through an ultraviolet-visible spectrometer.
Animal model of IR
All animal studies were approved by the ethical
committee of Chongqing Three Gorges Medical College (Chongqing,
China). A total of 125 male Sprague-Dawley rats (weight 200 g) were
purchased from the Experimental Animal Center of Chongqing Three
Gorges Medical College (Chongqing, China), and were divided into 8
groups (the sham group comprised of 10 rats; A total of 15 rats
were used to perform the optical bioluminescence imaging assay with
3 groups, each group containing 5 rats, and 100 rats were used to
perform the agent treatment assays with 4 groups, each group
containing 25 rats.). All the rats were fed in a pathogen-free
environment, at a temperature between 24–28°C, ventilated between
10–20 times per hour, with a relative humidity of 50–60%. The
light/dark cycle was (natural) circadian light, the food was
sterilized by irradiation, and the water contained bacitracin (4
g/l) and neomycin (4 g/l), the food and water were provided
adequately. In the experiment process, all the rats were
anesthetized with 4% pentobarbital sodium (0.4 ml/100 g) and placed
on a 37°C pad. Rats were ventilated during the procedure with a
MiniVent ventilator (Hugo Sachs Elektronik GmbH, March-Hugstetten,
Germany). A left thoracotomy was performed to expose the heart, and
the left anterior descending coronary artery (LAD) was occluded
with a 6-0 prolene suture. The regional ischemia was confirmed
through visual inspection. After 45 min ischemia, the ligation was
released. Ischemia injury in the tissue was confirmed subsequent to
re-perfusion. A sham group of rats underwent the same surgical
procedure, without ligation, the results of sham group were used to
confirm the successful establishment of IR model (data not shown).
All animals were sacrificed under anesthesia at the end of the
experiments.
Cardiac function analyses
A total of 30 min after the establishment of the IR
model, the rats received PBS (3 ml/kg), NP (5 mg/kg) in saline,
visnagin (2 mg/kg) in saline or NP-visnagin (1 mg/kg) in saline,
through a caudal vein injection in saline intravenously.
Hemodynamic measurements and echocardiography were used to analyze
cardiac function in rats. Two weeks after injection, the rats were
anesthetized prior to transthoracic M-mode echocardiography using a
Vevo770 system (VisualSonics Inc., Toronto, ON, Canada) with a
30-MHz probe (RMV 707B). A total of two weeks following the
injection of the reagents, the micromanometer catheter (Millar
1.4F, SPR 835; Millar, Inc., Houston, TX, USA) was used to detect
blood pressure by insertion into the right common carotid artery;
the Power Laboratory system (ADInstruments, Dunedin, New Zealand)
was used to record and analyze blood pressure.
Terminal deoxynucleotidyl transferase
dUTP nick end labeling (TUNEL) staining and caspase activity
Apoptosis was detected through TUNEL staining with
an In Situ Cell Death Detection kit (Roche Diagnostics,
Basel, Switzerland) according to the manufacturer's protocol. Total
cardiomyocytes were labeled by DAPI, whereas apoptotic
cardiomyocytes were labeled with green fluorescein staining. The
caspase-3 and caspase-9 activity was detected through a Caspase-3
colorimetric assay kit and a Caspase-9 colorimetric assay kit
(BioVision, Inc., Milpitas, CA, USA) according to the
manufacturer's protocol, and the caspase activity was detected by a
microplate reader at 405 nm.
Infarct size
At 24 h after reperfusion, the LAD was re-occluded
and 1% Evans blue dye (Sigma Aldrich; Merck KGaA, Darmstadt,
Germany) was injected into the inferior vena cava to identify the
area at risk (AAR); the heart was cut into 1 mm-thick cross
sections for incubation with 1% 2,3,5-triphenyltetrazolium chloride
(TTC, Sigma-Aldrich; Merck KGaA). At 7 days, the left ventricles of
the rat hearts were obtained for Masson staining to analyze the
infarct site. Photographs were captured with a digital camera
(Pentax K-X, Pentax, Inc., Japan). The infarct size was detected
with computer-assisted planimetry software (QW in version 3; Leica
Microsystems GmbH, Wetzlar, Germany).
Immunofluorescence
LC3 dots and NP-fluorescein isothiocyanate (FITC)
were detected with immunofluorescence staining. NP-FITC (2 mg/kg)
was injected into the inferior vena cava and hearts were harvested
from the mice. All the hearts were immersed in 4% paraformaldehyde
for 24 h and then dehydrated in 30% sucrose solutions for 2 h, then
dehydrated in ascending ethylic alcohols (50, 70, 80, 90 and 100%)
for 15 min at each concentration, cleared with 100% xylene and
embedded in 100% paraffin, and following by cutting into 5-µm thick
sections. The sections were deparaffinized and hydrated in a graded
alcohol series to distilled water, and then were permeabilized with
0.1% triton X-100 for 15 min and washed 3 times with 1% PBS. The
sections were incubated with antibodies (Anti-FITC; diltion, 1:500;
catalog no. #ab19224; Abcam, Cambridge, UK; LC3, dilution, 1:1,000,
CST Biological Reagents Co., Ltd.; catalog no. #3868; and Troponin
I; dilution, 1:500; catalog no. #ab10231; Abcam) at 4°C for
overnight. The sections were washed 3 times with 1% PBS, then
incubated with the Alexa Fluor® 647-conjucated secondary
antibodies [F(ab')2-Goat anti-Mouse IgG (H+L), dilution, 1:500;
catalog no. #A-21425 and Donkey anti-Rabbit IgG (H+L), dilution,
1:500; catalog no. #A10043 all Invitrogen; Thermo Fisher
Scientific, Inc.] at 37°C for 2 h. The sections were washed 3 times
with 1% PBS and observed through laser scanning confocal microscope
at ×400 magnification (TCS-SP5; Leica Microsystems GmbH).
Optical bioluminescence imaging (BLI)
in vivo
BLI, a reliable noninvasive imaging tool, was used
to evaluate the distribution of NP-FITC to the heart. Following the
injection of NP-FITC (2 mg/kg) and FITC (1 mg/kg), at 0.5, 1, 6 and
24 h, rats were anesthetized with 4% pentobarbital sodium, placed
on the 37°C pad and imaged with BLI using a Xenogen in vivo
imaging system (Caliper Life Sciences; PerkinElmer, Inc., Waltham,
MA, USA) to detect the fluorescence intensity.
Western blotting
LC3 expression was evaluated by western blot
analysis. All the tissue protein was extracted by a
Radioimmunoprecipitation assay (Beyotime Institute of
Biotechnology, Shanghai, China), and the protein concentration was
determined by an Enhanced BCA Protein assay kit (Beyotime Institute
of Biotechnology) according to the manufacturer's protocol. A total
of 50 µg protein was added per lane and separated by a 12% SDS-PAGE
gel, and blotted onto polyvinylidene fluoride (PVDF) membranes. The
membranes were blocked in a solution of 5% non-fat dried milk in
PBST (0.05% Tween-20 in PBS) for 1 h at room temperature, and
incubated with primary antibodies (LC3; dilution, 1:1,000; catalog
no. #3868; and GAPDH; dilute on, 1:1,000; catalog no. #5174 both
from CST Biological Reagents Co., Ltd., Shanghai, China) overnight
at 4°C. The membranes were washed three times for 10 min in PBST,
and incubated with secondary antibody (rabbit IgG, dilution, 1:500;
catalog no. #sc-2794; Santa Cruz Biotechnology, Inc., Dallas, TX,
USA) at 37°C for 1 h, and the membranes were washed three times for
10 min in PBST. The immunoreactive signal was detected through the
BeyoECL Plus kit (Beyotime Institute of Biotechnology), and the
ChemiDocXRS+ (Bio-Rad Laboratories, Inc., Hercules, CA, USA) was
used to obtain the images. Image J 3.0 (National Institutes of
Health, Bethesda, MD, USA) was used to quantify the band intensity
relative to GAPDH.
Transmission electron microscopy
(TEM)
TEM was used to detect autophagosomes. Following the
injection of visnagin-loaded NP, the hearts underwent retrograde
perfusion by PBS, and the left ventricle was harvested and fixed
with 4% glutaraldehyde for 24 h at room temperature, following
post-fixation with 2% osmium tetroxide for 2 h and 1% aqueous
uranyl acetate for 1 h at room temperature. The tissue was washed
in an ascending series of ethanol (50, 60, 70, 80, 90, 95 and
100%), and transferred to a mixture (10 ml) of propylene oxide and
EMbed 812 (Electron Microscopy Sciences, Hatfield, PA, USA; ratio
1:1), the tissue was incubated for 1 h at room temperature, then
place in a 60°C oven to polymerize for 48 h. Sections (80-nm thick)
were cut using a Leica ultramicrotome (Leica Microsystems GmbH) and
a Diatome diamond knife (Diatome Ltd., Nidau, Switzerland), and
were collected on 200-mesh copper grids and stained in 5% uranyl
acetate in ethanol for 15 min at room temperature and 5% Reynold's
lead citrate for 10 min at room temperature. The slices were then
observed with transmission electron microscopy at 40–120 kV (CM10;
Philips Medical Systems B.V., Eindhoven, The Netherlands).
Statistical analysis
All the data were expressed as the means ± standard
deviation and analyzed by SPSS 17.0 (SPSS, Inc., Chicago, IL, USA).
Intergroup comparisons were performed through a t test or analysis
of variance followed by Bonferroni post-hoc testing. P<0.05 was
considered to indicate a statistically significant difference.
Results
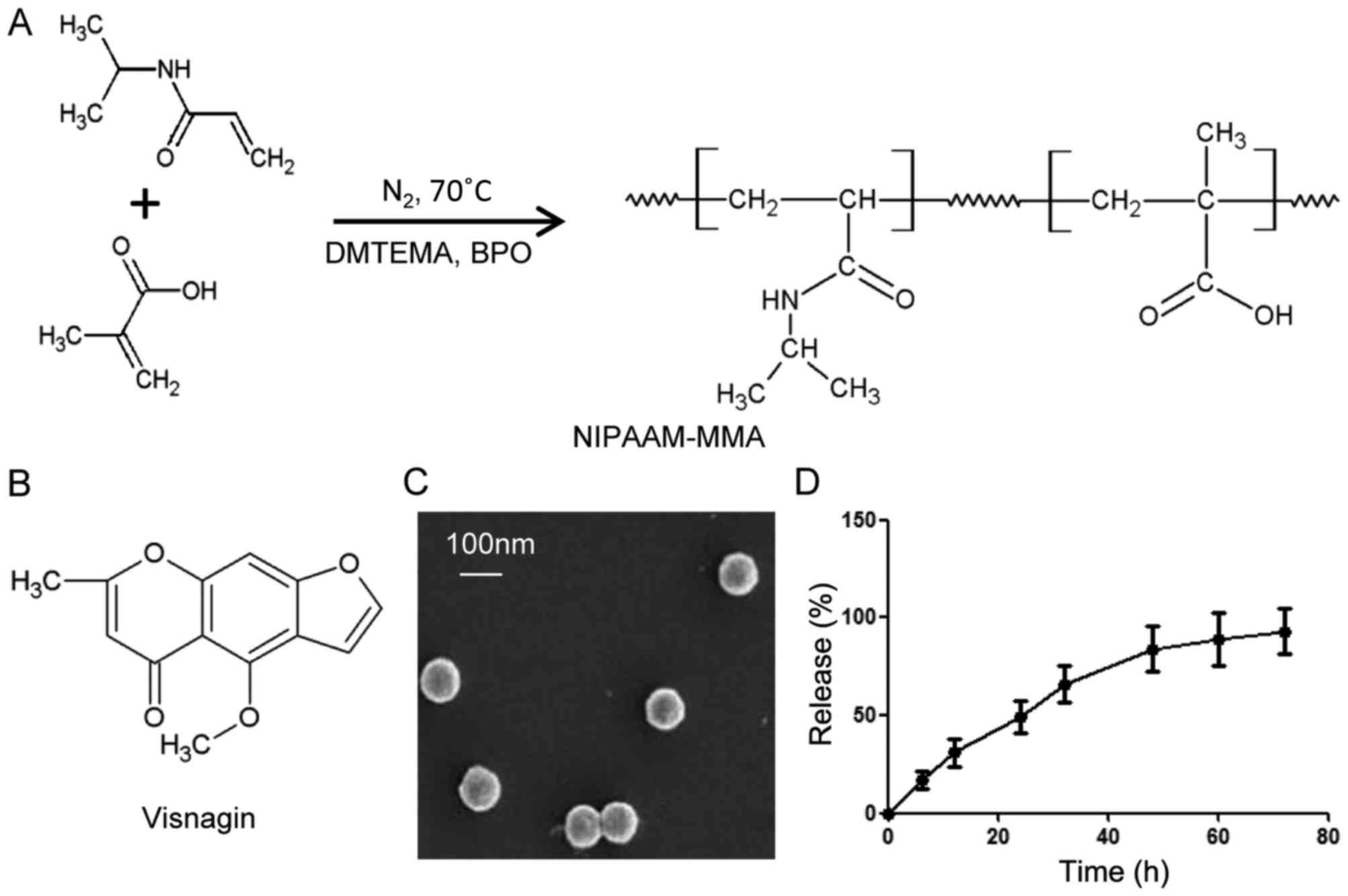
Visnagin-loaded NP synthesis
In order to obtain the perfect drug delivery
material, NIPAAm and MAA were selected for the synthesis of NP,
catalyzed by DMAEMA, BPO and N2 (Fig. 1A). With the aim of drug delivery,
visnagin was loaded into the NP (Fig.
1B); the loading rate was 100% (data not shown). The size and
shape of the NP were observed with SEM (Fig. 1C); the size of the NP was approaching
100 nm, and they were microspherical in shape. To determine the
release rate for NP-visnagin, a drug release assay was conducted;
initially, the release rate linearly increased, indicating that the
amount of released visnagin increased over time, whereas the
release ratio was decreased from 50 h, and trended towards a halt
(Fig. 1D). These results demonstrated
that NP synthesized with NIPAAm-MAA were an excellent
visnagin-loading material, and that the characteristics of NP were
suitable for visnagin release.
NP-visnagin targeted to the ischemic
region to induce cardiomyocyte protection subsequent to IR
To detect the targeting ability of NP, NP-FITC was
synthesized for a BLI in vivo assay. In the rats with IR
injury, at 0.5 h after NP-FITC injection, NP-FITC was concentrated
in the heart; the concentration of NP-FITC in the heart increased
over time, as demonstrated by the increase in fluorescence
(Fig. 2A and B). The PBS-injected
group exhibited no fluorescence intensity increase in the heart,
and in the group injected with FITC alone, the fluorescence
intensity increased to a visibly lesser extent (Fig. 2A and B). Through an immunofluorescence
assay, it was indicated that NP-FITC had predominantly localized to
the infarcted area after NP-FITC injection (Fig. 2C and D). In addition, treatment with
either intravenous NP-visnagin or visnagin alone reduced IR injury
at the onset of reperfusion (Fig. 2E and
F); based on TTC staining, intravenous NP-visnagin treatment
significantly reduced the MI size compared with visnagin alone, and
was >2-fold more effective (Fig. 2E
and F). Additionally, the percentage AAR in the left ventricle
was not significantly different between groups (Fig. 2G). These results demonstrate that
NP-visnagin targeted the ischemic region and conferred superior
cardioprotection against myocardial IR injury compared with
visnagin alone.
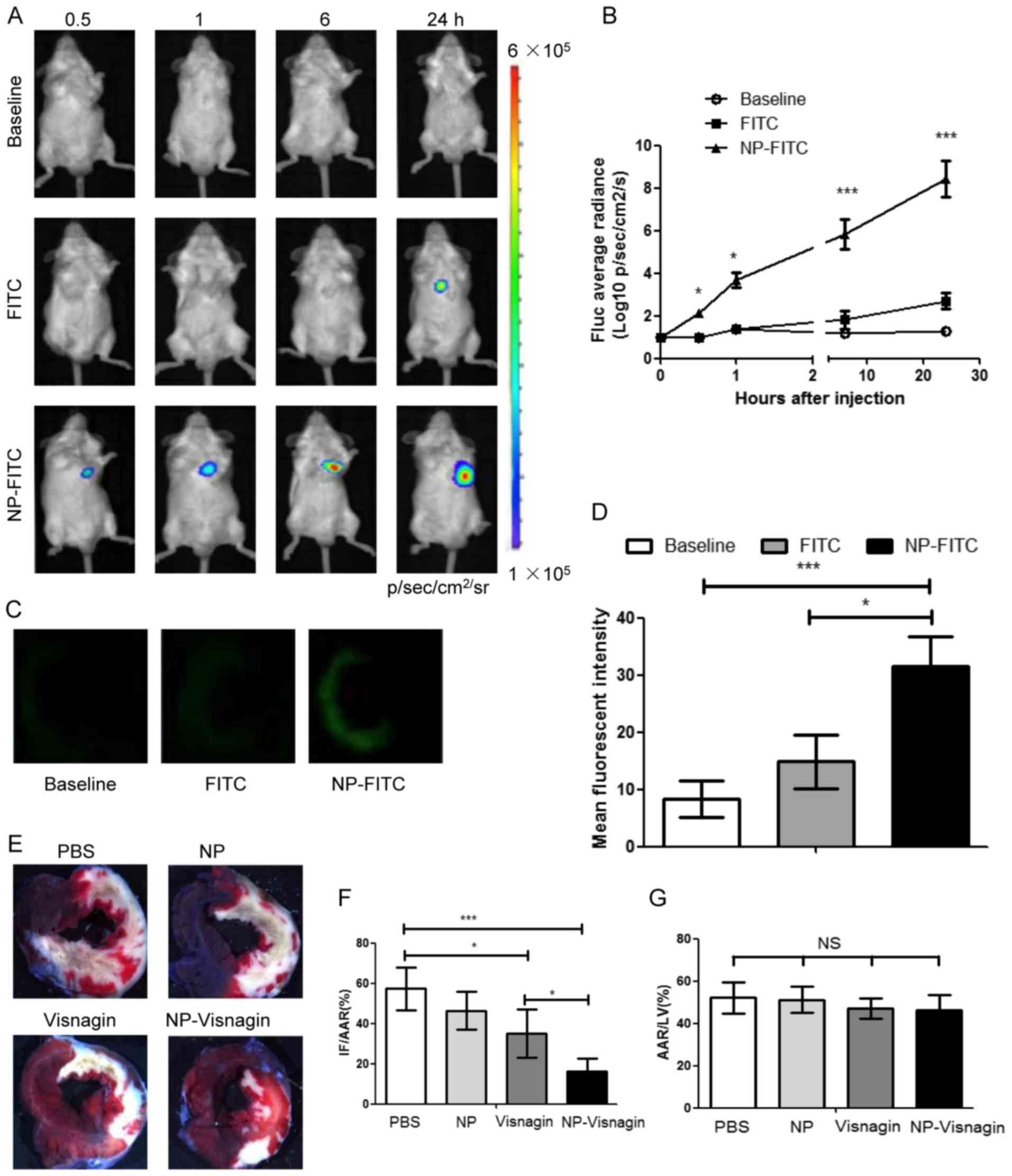 | Figure 2.NP-visnagin targeted to the reperfused
myocardium and exerted cardioprotective effects. (A) Following the
intravenous injection of PBS (baseline), FITC or NP-FITC, in
vivo BLI was performed at each time point. (B) Quantitative
analysis of BLI data for NP-FITC compared with FITC alone. (C)
Fluorescence images of heart cross-sections at 12 h after the
intravenous injection of PBS, FITC or NP-FITC. (D) Quantification
of the fluorescence intensity of the non-ischemic myocardium and
AAR. (E) Representative stereomicrographs of heart sections double
stained with TTC and Evans blue at 72 h after intravenous
injection. (F) Quantitative analysis of IF/AAR. (G) Quantitative
analysis of AAR/LV. *P<0.05; ***P<0.005. NP, nanoparticles;
FITC, fluorescein isothiocyanate; BLI, bioluminescence imaging;
TTC, 2,3,5-triphenyltetrazolium chloride; IF, infarct area; AAR,
area at risk; LV, left ventricle; NS, not significant. |
NP-visnagin ameliorated cardiac
dysfunction at 4 weeks subsequent to IR
Echocardiography results demonstrated that
NP-visnagin or visnagin alone significantly ameliorated cardiac
dysfunction, although the effect of NP-visnagin was greater
(Fig. 3A-C). NP-visnagin
significantly decreased the left ventricular end-diastolic
dimension and end-systolic dimensions, and increased the left
ventricular ejection fraction and fractional shortening (Fig. 3B). Furthermore, NP-visnagin increased
the left ventricular systolic pressure and rate of rise of left
ventricular pressure (dP/dt), and decreased the left ventricular
end-diastolic pressure (Fig. 3C).
Thus, NP-visnagin ameliorated cardiac dysfunction through improving
the systolic and diastolic function and pressure. Additionally,
Masson staining indicated that NP-visnagin significantly inhibited
fibrosis (Fig. 3D and E). These
results indicated that NP-visnagin or visnagin alone ameliorated
cardiac dysfunction and blocked fibrosis, whereas the effect of
NP-visnagin was greater.
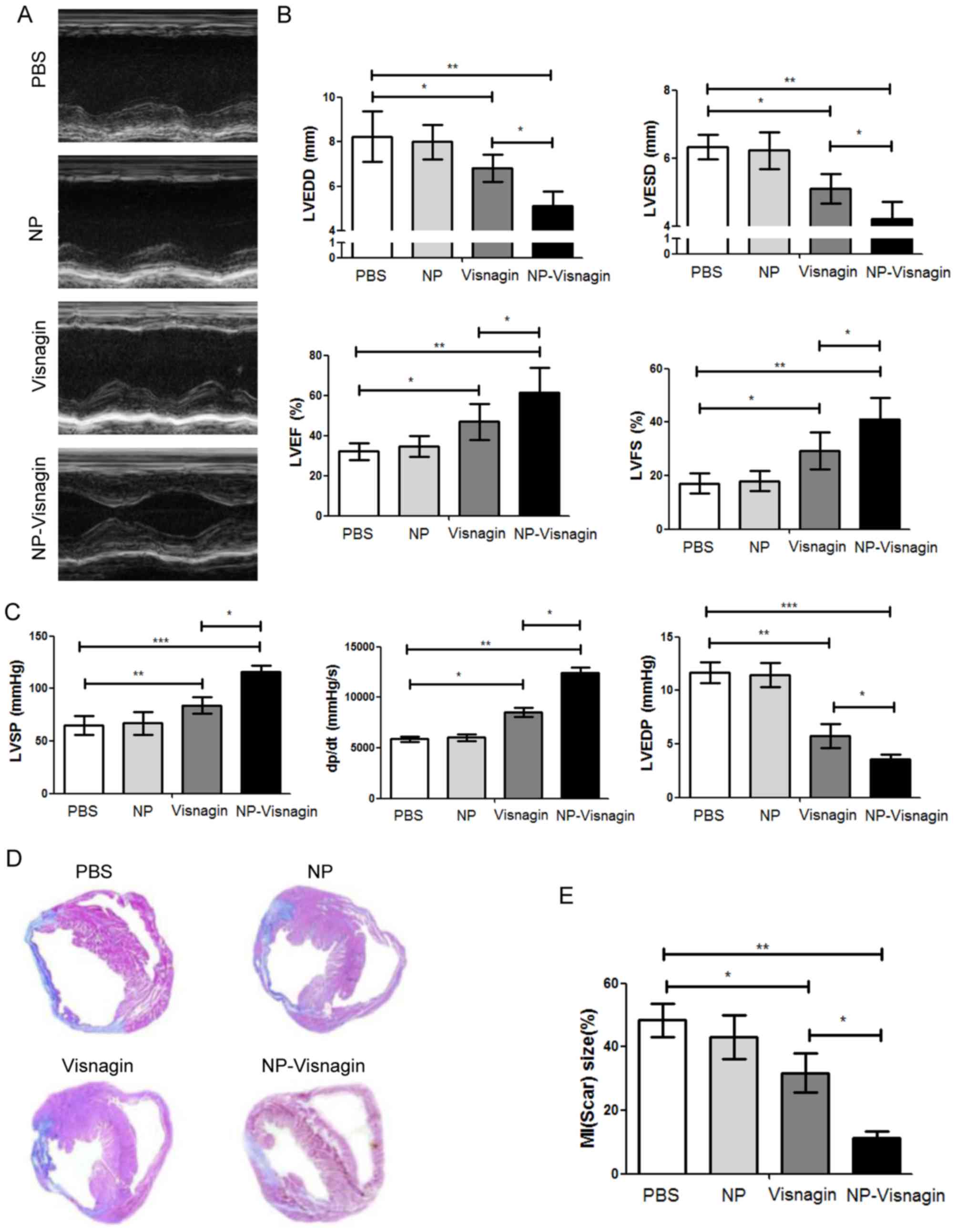 | Figure 3.NP-visnagin ameliorated cardiac
dysfunction 4 weeks after ischemia/reperfusion. (A) M-mode
echocardiography was performed for rats at 4 weeks after
intravenous injection with NP-visnagin and other treatments. (B)
Effect of NP-visnagin on LVEDD, LVESD, LVEF and LVFS. (C) Systolic
blood pressure was detected through the micromanometer catheter
method, and the LVSP, the rate of rise of left ventricular pressure
(dP/dt) and LVEDP were calculated. (D) Based on Masson staining,
the effects of NP-visnagin and the other treatments on fibrosis at
4 weeks after intravenous injection were detected; representative
images are shown. (E) Quantification of fibrosis. *P<0.05;
**P<0.01; ***P<0.005. NP, nanoparticles; LVEDD, left
ventricular end-diastolic dimension; LVESD, left ventricular
end-systolic dimension; LVEF, left ventricular ejection fraction;
LVFS, left ventricular fractional shortening; LVSP, left
ventricular systolic pressure; LVEDP, left ventricular
end-diastolic pressure; MI, myocardial infarction. |
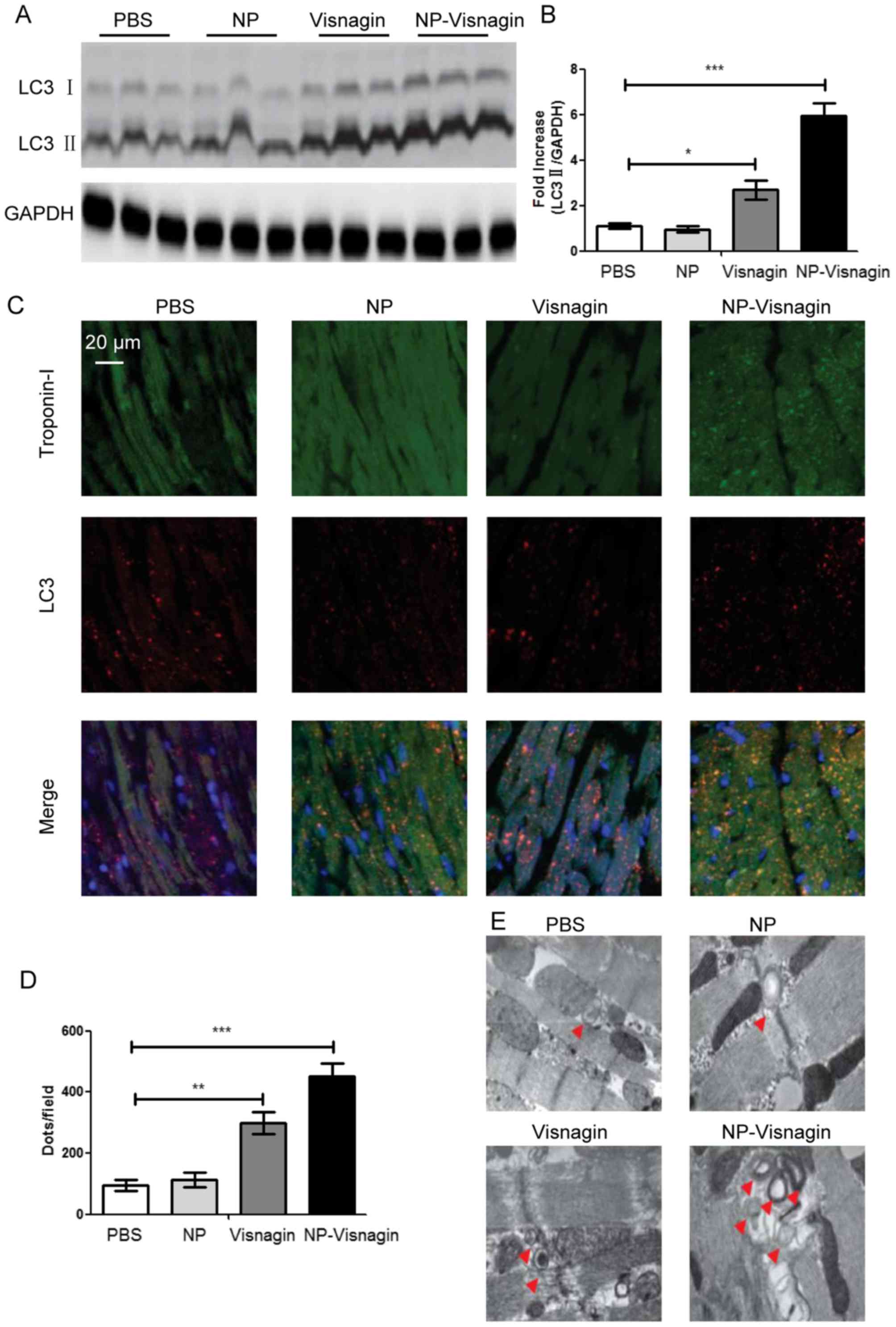
NP-visnagin enhanced autophagy in the
ischemic region after IR
As it had been identified that NP-visnagin protected
cardiomyocytes after IR, further study was conducted to reveal the
mechanism for the NP-visnagin protection of cardiomyocytes. As
autophagy is an established protective mechanism for cells under
stress, and LC3 is a marker of autophagic flux, proteins from the
AAR were analyzed with a western blot assay. The results
demonstrated that NP-visnagin significantly increased the level of
LC3II; although visnagin alone also improved the expression of
LC3II, the effect of NP-visnagin was greater (Fig. 4A and B). To further confirm
NP-visnagin-induced autophagy, immunofluorescence studies were
conducted. The results of immunofluorescence were consistent with
western blot assay, as both NP-visnagin and visnagin alone could
enhance the autophagic flux, and the effect of NP-visnagin was
greater (Fig. 4C and D). TEM is
considered the gold standard for autophagic flux detection;
following the NP-visnagin and visnagin treatment of IR injury, the
ischemia region was analyzed by TEM. The number of visible bilayer
structure bodies was significantly improved following visnagin
treatment, with the highest number observed in the NP-visnagin
group (Fig. 4E). Collectively, the
data demonstrated that NP-visnagin protected cardiomyocytes against
IR injury through the induction of autophagy.
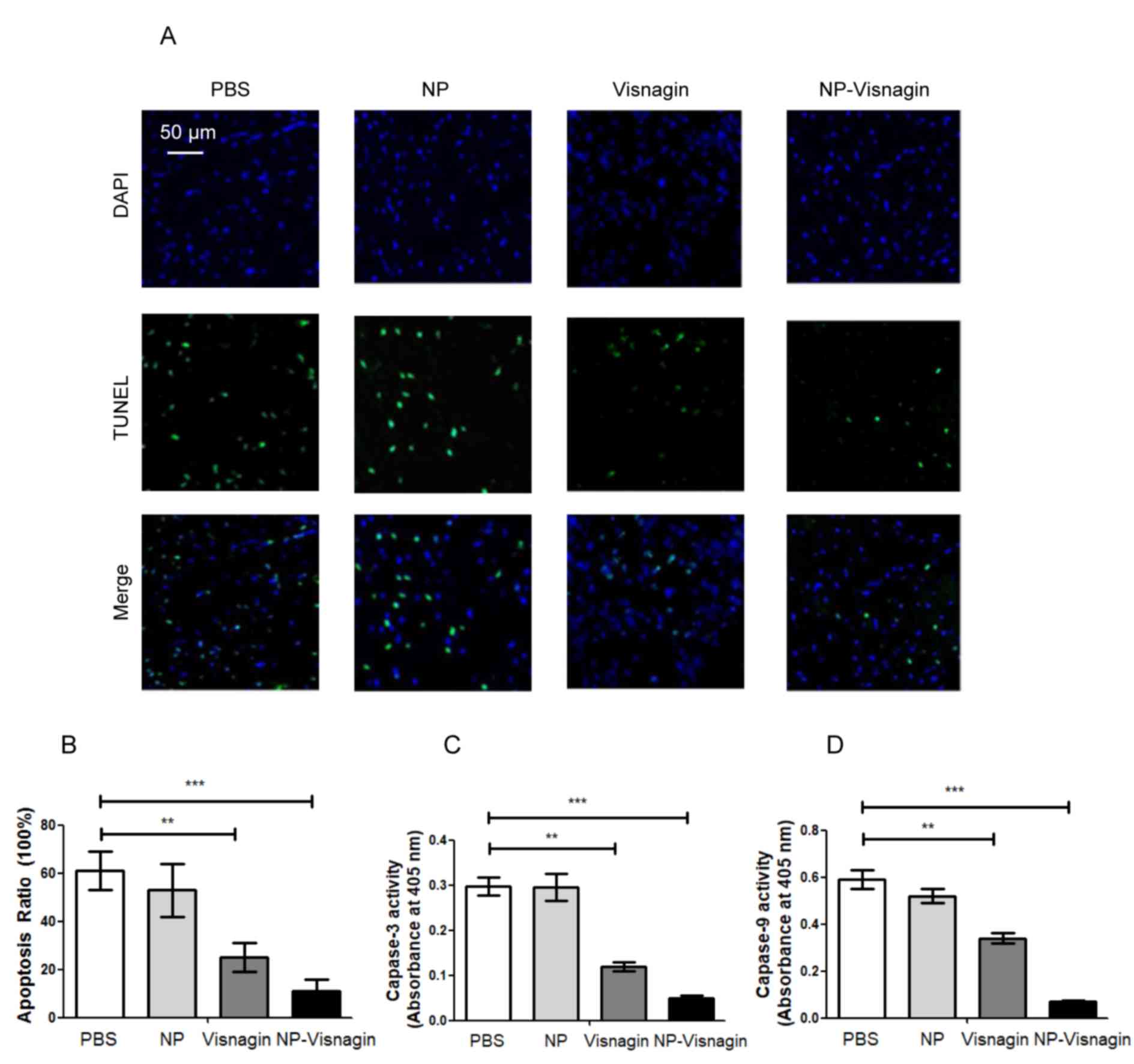
NP-visnagin inhibited apoptosis in the
ischemic region after IR
In IR injury, apoptosis is the most predominant
mechanism for cell death. In order to detect apoptosis, TUNEL and
caspase activity assays were used. As demonstrated in Fig. 5A and B, subsequent to IR injury,
following treatment PBS or NP treatment, the apoptotic index was
significantly increased compared with the effect of visnagin or
NP-visnagin treatment, and the effect of NP-visnagin was the most
pronounced. Additionally, in the visnagin and NP-visnagin treatment
groups, caspase-3 and −9 activity were significantly decreased
compared with the PBS and NP groups, and the effect of NP-visnagin
was greater (Fig. 5C and D). These
results indicated that NP-visnagin inhibited apoptosis in IR injury
to protect the damaged cells.
Discussion
In the present study, it was identified that the
intravenous injection of NIPAAm-MAA NP specifically targeted the IR
myocardium after reperfusion; NP-visnagin protected the myocardium
against IR injury, reduced the MI region and ameliorated cardiac
dysfunction; furthermore, the mechanism for the protective effects
of NP-visnagin on the myocardium against IR injury may have
included the induction of autophagy and the inhibition of
apoptosis.
A previous study demonstrated that patients at a
high risk of MI who receive pretreatment with statins prior to
ischemia present with a reduced region of MI, whereas treatment
with statins had no effect on the MI region when administered at
the time of reperfusion (15). In the
present study, it was observed that the intravenous injection of
NP-visnagin at the time of reperfusion could significantly reduce
the MI region at 24 h after reperfusion, as well as ameliorating
cardiac dysfunction, and inhibiting fibrosis and hypertrophy at 4
weeks after IR. Although visnagin alone reduced the MI region and
ameliorated cardiac dysfunction, the effect was less than
NP-visnagin. These results indicated that visnagin was a potential
therapeutic agent for IR injury, and NP could be an ideal delivery
material for visnagin. Optical BLI and fluorescence imaging
indicated that intravenously injected NP-FITC was selectively
transported into the reperfusion myocardium. Takahama et al
(16) reported that polyethylene
glycol conjugated with liposomes was selectively delivered into the
reperfusion myocardium infarct and border region in a rat model,
but the precise mechanism by which the liposomes were delivered to
the reperfusion myocardium in IR injury was not clarified. The
present study identified that NP-FITC was delivered not only to the
heart, but also specifically to the infarct site, indicating that
NIPAAm-MAA may markedly enhance the drug delivery into the
myocardium by improving the vascular permeability. A previous study
reported that the reoxygenation of the anoxic cardiac myocardium
after IR could induce the uptake of nanoparticles through
endocytosis (17).
Visnagin is a natural compound extracted from the
fruit of Ammi visnaga; it was previously reported that
visnagin may exhibit cell protective effects (18). It was demonstrated that visnagin
protected kidney epithelial cells against oxalate injury, and
neurons against KA-induced apoptosis (19,20).
Furthermore, there were reports that visnagin could inhibit
LPS-induced inflammation in microglial cells, and that it was a
potent cardioprotective compound against doxorubicin-induced
cardiomyopathy; a potential mechanism was the binding of
mitochondrial malate dehydrogenase by visnagin to trigger the
tricarboxylic acid cycle and promote the metabolism of the
myocardium (5,21). Additionally, in the field of
anti-cancer research, visnagin was also demonstrated to promote
aryl hydrocarbon receptor (AHR) signaling, inducing the inhibition
of cell growth, differentiation and migration in human
hepatocellular carcinoma (22).
Autophagy is a self-protective cell process in
response to stress stimulation. It has been reported that autophagy
may alleviate metabolic crisis through ATP generation in myocardial
IR injury; a low ATP level is an inducer of cardiomyocyte autophagy
by the activation of the AMP-activated protein kinase/mammalian
target of rapamycin complex 1-Unc-51-like autophagy-activating
kinase 1 (ULK1) pathway (23).
Cardiac autophagy enables the recovery of energy, and is essential
for cardiomyocyte survival. Additionally, autophagy promotes
proteostasis in IR injury (13). Once
autophagy is activated in IR injury, it can remove cytotoxic
ubiquitinated proteins and attenuate protein aggregation. The
increase in autophagic activity can compensate for the damage to
the ubiquitin proteasome system, and promote the stability of
proteolysis. Furthermore, in conditions of reactive oxygen species
over-production and inflammatory response in IR injury, the
induction of autophagy may remove dysfunctional mitochondria and
recycle waste to maintain the energy balance, preventing damaged
mitochondrial from releasing cytotoxic substances, and promoting
cardiomyocyte survival (14,24).
In contrast with autophagy, it has been demonstrated
that apoptosis may be associated with the pathogenesis of the
myocardium in IR injury and contribute to cardiomyocyte death
(25). Apoptotic morphological
phenotype alterations are observed in IR injury, suggesting that
cardiomyocyte apoptosis is stimulated (26). Oxygen free radicals, mitochondrial
damage and calcium accumulation are potential inducers of
cardiomyocyte apoptosis in IR injury. Oxygen free radicals are
generated and accumulated, and ultimately activate a chain reaction
leading to the destruction of nucleic acids (27). Mitochondrial damage can contribute to
the release of apoptosis-inducing factors from the mitochondria,
including apoptotic peptidase-activating factor 1, which can
promotes cysteinyl aspartate-specific proteases (i.e. caspases) to
induce apoptosis. The accumulation of Ca2+ in the
mitochondria may activate mitochondrial membrane permeability
transition pores and contribute to the release of cytochrome c into
the cytoplasm, which activates caspases to induce apoptosis
(28).
Previous studies have demonstrated that AHR
signaling participates in the modulation of autophagy and
apoptosis. AHR is upstream of the Beclin1/Bcl2 complex; it can
inhibit the interaction between Beclin1 and Bcl2 to contribute to
the release of Beclin1. However, AHR may also promote the
development of the autophagy-related 14 (Atg14)-Vps34 complex into
the Atg14-Vps34-ULK1 complex, which acts as an activator of
autophagy (29–31). AHR is also the activator of
anti-apoptotic proteins, including Bcl2, Bcl-XL and survivin, and
the inhibitor of pro-apoptotic proteins, including Bcl2-associated
X, Bcl2-interacting protein and P53 (32,33).
Visnagin has been reported as an inducer of AHR (20,22); it
was identified in the present study that NP-visnagin could
significantly promote autophagy and inhibit apoptosis in the
ischemia region. This indicated that the protective mechanism of
NP-visnagin may be through the induction of autophagy and the
inhibition of apoptosis.
In summary, it was demonstrated that NIPAAm-MAA NP
loaded with visnagin targeted the IR myocardium with
cardioprotective effects, reducing the MI size and ameliorating
cardiac dysfunction through the induction of autophagy and the
inhibition of apoptosis. NIPAAm-MAA NP-based technology may be
useful as a novel drug delivery system for IR injury treatment.
Additionally, the identification of the cardioprotective effects of
visnagin suggests that visnagin may be a novel potential drug for
IR injury treatment, although its cardioprotective mechanism
requires further clarification.
Acknowledgements
The present study was supported by Chongqing
Municipal Education Commission Science and Technology Research
Projects (grant no. KJ1502605).
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Capodanno D: Long-term EXAMINATION of
drug-eluting stents in acute myocardial infarction. Lancet.
387:316–318. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Doll JA and Roe MT: Time to treatment as a
quality metric for acute STEMI care. Lancet. 385:1056–1057. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Inoue T: Ischemia-reperfusion injury is
still a big hurdle to overcome for treatment of acute myocardial
infarction. J Cardiol. 67:305–306. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kaul B and Staba EJ: Visnagin:
Biosynthesis and isolation from ammi visnagi suspension cultures.
Science. 150:1731–1732. 1995. View Article : Google Scholar
|
|
5
|
Liu Y, Asnani A, Zou L, Bentley VL, Yu M,
Wang Y, Dellaire G, Sarkar KS, Dai M, Chen HH, et al: Visnagin
protects against doxorubicin-induced cardiomyopathy through
modulation of mitochondrial malate dehydrogenase. Sci Transl Med.
6:266ra1702014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Abu-Hashem AA and El-Shazly M: Synthesis,
reactions and biological activities of furochromones: A review. Eur
J Med Chem. 90:633–665. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hu CM, Fang RH, Luk BT and Zhang L:
Nanoparticle-detained toxins for safe and effective vaccination.
Nat Nanotechnol. 8:933–938. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bearat HH, Lee BH and Vernon BL:
Comparison of properties between NIPAAm-based simultaneously
physically and chemically gelling polymer systems for use in vivo.
Acta Biomater. 8:3629–3642. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chao TI, Xiang S, Lipstate JF, Wang C and
Lu J: Poly(methacrylic acid)-grafted carbon nanotube scaffolds
enhance differentiation of hESCs into neuronal cells. Adv Mater.
22:3542–3547. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zeighamian V, Darabi M, Akbarzadeh A,
Rahmati-Yamchi M, Zarghami N, Badrzadeh F, Salehi R, Mirakabad FS
and Taheri-Anganeh M: PNIPAAm-MAA nanoparticles as delivery
vehicles for curcumin against MCF-7 breast cancer cells. Artif
Cells Nanomed Biotechnol. 44:735–742. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim SW, Oh KT, Youn YS and Lee ES:
Hyaluronated nanoparticles with pH- and enzyme-responsive drug
release properties. Colloids Surf B Biointerfaces. 116:359–64.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Boateng S and Sanborn T: Acute myocardial
infarction. Dis Mon. 59:83–96. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sala-Mercado JA, Wider J, Undyala VV,
Jahania S, Yoo W, Mentzer RM Jr, Gottlieb RA and Przyklenk K:
Profound cardioprotection with chloramphenicol succinate in the
swine model of myocardial ischemia-reperfusion injury. Circulation.
122:S179–S184. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Przyklenk K, Undyala VV, Wider J,
Sala-Mercado JA, Gottlieb RA and Mentzer RM Jr: Acute induction of
autophagy as a novel strategy for cardioprotection: Getting to the
heart of the matter. Autophagy. 7:432–433. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hirsch A, Windhausen F, Tijssen JG,
Verheugt FW, Cornel JH and de Winter RJ: Long-term outcome after an
early invasive versus selective invasive treatment strategy in
patients with non-ST-elevation acute coronary syndrome and elevated
cardiac troponin T (the ICTUS trial): A follow-up study. Lancet.
369:827–835. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Takahama H, Minamino T, Asanuma H, Fujita
M, Asai T, Wakeno M, Sasaki H, Kikuchi H, Hashimoto K, Oku N, et
al: Prolonged targeting of ischemic/reperfused myocardium by
liposomal adenosine augments cardioprotection in rats. J Am Coll
Cardiol. 53:709–717. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cabigas EB, Ding G, Chen T, Saafir TB,
Pendergrass KD, Wagner MB and Davis ME: Age- and chamber-specific
differences in oxidative stress after ischemic injury. Pediatr
Cardiol. 33:322–331. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ragab FA, Hassan GS, Yossef HA and Hashem
HA: Synthesis of 6- and 9-alkylaminomethyl furoflavones as
gastroprotective agents. Eur J Med Chem. 42:1117–1127. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Badr JM, Hadad GM, Nahriry K and Hassanean
HA: Validated HPLC method for simultaneous estimation of khellol
glucoside, khellin and visnagin in Ammi visnaga L. fruits and
pharmaceutical preparations. Nat Prod Res. 29:593–601. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kwon MS, Lee JK, Park SH, Sim YB, Jung JS,
Won MH, Kim SM and Suh HW: Neuroprotective Effect of Visnagin on
Kainic Acid-induced Neuronal Cell Death in the Mice Hippocampus.
Korean J Physiol Pharmacol. 14:257–263. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee JK, Jung JS, Park SH, Park SH, Sim YB,
Kim SM, Ha TS and Suh HW: Anti-inflammatory effect of visnagin in
lipopolysaccharide-stimulated BV-2 microglial cells. Arch Pharm
Res. 33:1843–1850. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vrzal R, Frauenstein K, Proksch P, Abel J,
Dvorak Z and Haarmann-Stemmann T: Khellin and visnagin
differentially modulate AHR signaling and downstream CYP1A activity
in human liver cells. PLoS One. 8:e749172013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gatica D, Chiong M, Lavandero S and
Klionsky DJ: Molecular mechanisms of autophagy in the
cardiovascular system. Circ Res. 116:456–467. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dutta D, Calvani R, Bernabei R,
Leeuwenburgh C and Marzetti E: Contribution of impaired
mitochondrial autophagy to cardiac aging: Mechanisms and
therapeutic opportunities. Circ Res. 110:1125–1138. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kolwicz SC Jr, Purohit S and Tian R:
Cardiac metabolism and its interactions with contraction, growth,
and survival of cardiomyocytes. Circ Res. 113:603–616. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nishida K, Yamaguchi O and Otsu K:
Crosstalk between autophagy and apoptosis in heart disease. Circ
Res. 103:343–351. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kolwicz SC Jr, Purohit S and Tian R:
Cardiac metabolism and its interactions with contraction, growth,
and survival of cardiomyocytes. Circ Res. 113:603–616. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Viola HM, Arthur PG and Hool LC: Transient
exposure to hydrogen peroxide causes an increase in
mitochondria-derived superoxide as a result of sustained alteration
in L-type Ca2+ channel function in the absence of apoptosis in
ventricular myocytes. Circ Res. 100:1036–1044. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhang Y, Dong S, Wang H, Tao S and Kiyama
R: Biological impact of environmental polycyclic aromatic
hydrocarbons (ePAHs) as endocrine disruptors. Environ Pollut.
213:809–824. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ni HM, Bhakta A, Wang S, Li Z, Manley S,
Huang H, Copple B and Ding WX: Role of hypoxia inducing factor-1β
in alcohol-induced autophagy, steatosis and liver injury in mice.
PLoS One. 9:e1158492014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Farrall AL and Whitelaw ML: The
HIF1alpha-inducible pro-cell death gene BNIP3 is a novel target of
SIM2s repression through cross-talk on the hypoxia response
element. Oncogene. 28:3671–3680. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Vilahur G, Cubedo J, Casani L, Padro T,
Sabate-Tenas M, Badimon JJ and Badimon L: Reperfusion-triggered
stress protein response in the myocardium is blocked by
post-conditioning. Systems biology pathway analysis highlights the
key role of the canonical aryl-hydrocarbon receptor pathway. Eur
Heart J. 34:2082–2093. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Qi Y, Tian X, Liu J, Han Y, Graham AM,
Simon MC, Penninger JM, Carmeliet P and Li S: Bnip3 and AIF
cooperate to induce apoptosis and cavitation during epithelial
morphogenesis. J Cell Biol. 198:103–114. 2012. View Article : Google Scholar : PubMed/NCBI
|