Introduction
Epithelial ovarian cancer, accounting for >90% of
primary ovarian neoplasms, had four major histological subtypes:
Serous, endometrioid, mucinous and clear-cell subtypes (1). Several reports evaluating biological and
clinical behavior of ovarian cancers suggested that there have been
several classifications in addition to histological subtypes
(2–7).
The activation of JAK2/STAT3 pathway has been
reported to play critical roles in several oncogenic processes
including proliferation, survival, differentiation and angiogenesis
in several solid tumors (8,9). In ovarian cancers, some reports
suggested have reported that the activation of STAT3 was associated
with prognoses by univariate analysis (10,11). In
serous histological subtype, a report revealed that STAT3
polymorphisms were associated with unfavorable responses against
platinum-based chemotherapy (12). In
clear-cell subtype, it has been reported that IL-6R, an activator
of JAK2/STAT3 signaling, was correlated with unfavorable survival
by multivariate analysis, however, no relationship between
prognoses and activation of phosphorylated STAT3 (p-STAT3) was
observed (13).
Niclosamide (C13H8Cl2N2O4) is a small-molecule drug
of the teniacide anthelmintic family that is effective against
human tapeworms (14,15). This agent was previously reported to
have therapeutic activities in several cancers by inhibition of
STAT3 (14,16,17).
However, there have been no reports evaluating whether inhibiting
STAT3 signaling using this drug could modify the sensitivity to
platinums in ovarian cancers.
The present study was conducted to evaluate the
correlation between activation of JAK2/STAT3 pathway and
clinicopathological parameters in ovarian cancers. Additionally,
antitumor effect by inhibition of JAK2/STAT3 pathway was evaluated
in vitro evaluation.
Patients and methods
Patients and tissue microarray
Tissue blocks from a total of 341 patients with
epithelial ovarian carcinoma who received primal surgery at the
National Defense Medical College Hospital (Tokorozawa, Japan)
between 1984 and 2008 were used for the present study. A total of
341 patients who met the inclusion criteria were enrolled in this
investigation: i) patients who received no prior chemotherapy
before surgical therapy; ii) patients who were diagnosed to have
epithelial ovarian cancers by pathological evaluation; iii)
patients whose histological subtype was serous, endometrioid,
mucinous, and clear-cell type; iv) patients whose medical
information, and tissue blocks were available. The institutional
ethical review board of National Defense Medical College approved
the protocol of the present retrospective analyses. Comprehensive
informed consent using tumor samples had been obtained from each
patient at the time of primary treatment. After IRB approval, the
notice of the protocol including the use patients' samples were
open to the public, without any objection or rejection. So, all the
samples of the patients were used in the present study.
Two core specimens, 1.5 mm in diameter, for each
case were taken from cancer blocks and transferred to recipient
blocks using a Tissue Microarrayer (Beecher Instrument, Silver
Spring, MD, USA). All specimens were cut into 4-µm-thick slices to
make sections for immunohistochemical (IHC) staining. Satisfactory
IHC staining was obtained in all cases.
Characteristics of the patients were shown in
Table I. Median age of all patients
was 53 years (range, 16–82 years), and median follow-up duration
was 58 months (range, 1–257 months). The number of patients
according to the International Federation of Obstetrics and
Gynecology (FIGO) classification was as follows: 126 in stage I, 40
in stage II, 129 in stage III, and 46 in stage IV, respectively.
The subjects consisted of 197 patients with no residual tumors (RT)
after a primary cytoreductive surgery, 47 with optimal surgery, and
97 with suboptimal surgery. A total of 90 patients were treated
with taxanes and platinum chemotherapy: 78 cases with paclitaxel
and carboplatin (TC) and 12 cases with docetaxel and carboplatin
(DC) regimen. Platinum-based chemotherapy was used in 223 cases:
165 cases by combination with cyclophosphamide, adriamycin and
cisplatin (CAP), 31 cases by chemotherapy with irinotecan and
cisplatin (CPT-P), 15 cases by chemotherapy with etoposide and
cisplatin (EP), and 12 cases by the other regimens.
 | Table I.Characteristics of the patients. |
Table I.
Characteristics of the patients.
|
| Histology |
|
|---|
|
|
|
|
|---|
| Variables | Serous n=144 | Clear-cell n=85 | Endometrioid
n=52 | Mucinous n=60 | Total n=144 |
|---|
| Age (years) |
|
|
|
|
|
|
16–52 | 59 | 43 | 25 | 32 | 159 |
|
53–82 | 85 | 42 | 27 | 28 | 182 |
| FIGO stage |
|
|
|
|
|
| I | 17 | 44 | 24 | 41 | 126 |
| II | 12 | 8 | 15 | 5 | 40 |
| III | 79 | 29 | 10 | 11 | 129 |
| IV | 36 | 4 | 3 | 3 | 46 |
| Primary surgery |
|
|
|
|
|
|
Complete surgery (RT=0
cm) | 64 | 61 | 26 | 46 | 197 |
| Optimal
surgery (RT≤1 cm) | 21 | 10 | 12 | 4 | 47 |
|
Suboptimal surgery (RT>1
cm) | 59 | 14 | 14 | 10 | 97 |
| Primary
chemotherapy |
|
|
|
|
|
| Taxane
+ platinum | 64 | 11 | 12 | 3 | 90 |
|
Platinum-based therapy | 78 | 68 | 31 | 46 | 223 |
|
None | 2 | 6 | 9 | 11 | 28 |
Reagents/antibodies
Niclosamide was purchased from Selleck Chemicals
(Houston, TX, USA). The primary antibodies against p-STAT3, XIAP,
cleaved PARP, and β-actin and the secondary antibodies were
obtained from Cell Signaling Technology (Danvers, MA, USA). The
primary antibodies against STAT3 and p-JAK2 was obtained from Abcam
(Cambridge, MA, USA).
IHC staining
For IHC staining, antibodies used were phospho-JAK2
(Y1007 + Y1008; rabbit monoclonal, 1:100; Abcam) and phospho-STAT3
(Tyr705; rabbit monoclonal, 1:50; Cell Signaling Technology, Inc.).
Tissue microarray slides were deparaffinised in xylene and hydrated
with ethanol. The slides for p-JAK2 were boiled in an autoclave at
121°C for 15 min in citrate buffer (10 mM, pH 6.0), and then
allowed to cool at room temperature. The slides for p-STAT3 were
pretreated in an electric pot at 98°C for 40 min in EDTA buffer (1
mM, pH 8.0). Endogenous peroxidase activity was blocked by 0.3%
H2O2/methanol. The slides were incubated at
4°C overnight with primary antibodies and reacted with the DAKO
EnVision + system-horseradish peroxidase (HRP)-labelled polymer
(DAKO Denmark A/S, Glostrup, Denmark) as a secondary antibody for
30 min at room temperature. Specific antigen-antibody reactions
were visualized with 0.2% diaminobenzine tetrahydrochloride and
hydrogen peroxide, and counterstained with Mayer haematoxylin.
Positive staining was defined as the present of staining of >10%
of the nuclei.
Cell lines and culture conditions
Ovarian clear cell cancer cell line, KK, were used
(18). These cell lines were grown as
monolayer cultures in RPMI-1640 + Glutmax™-I (Invitrogen Japan KK,
Tokyo, Japan) medium supplemented with 10% fetal bovine serum
(Invitrogen Japan KK), 100 U penicillin per ml, and 100 mg
streptomycin per ml (Invitrogen Japan KK) in a humidified
atmosphere of 5% CO2 at 37°C, and routinely tested for
mycoplasma infection. Protein concentrations were determined by
Bradford assay (Bio-Rad Laboratories, Hercules, CA, USA). KK cells
were positive for expression of phospho-STAT3 in normal
condition.
Cell proliferation and cytotoxicity
assay
KK cells were seeded onto 96-well plates at
~1×104 or 4×104 cells cm−2 for
cytotoxicity assays. Cell viability was determined by MTT method
using Tetra Color ONE (Seikagaku Corporation, Tokyo, Japan)
according to the manufacturer's instructions. Cell cytotoxicity by
niclosamide was measured after 5 days from the treatment at
different concentration. For the evaluation of protein expression,
KK cells were harvested after 24 h from the treatment with
niclosamide. The experiments were repeated three times, and mean
values were used to construct the kinetic curves.
Preparation of cell lysate for western
blot analysis
Protein lysates were extracted in RIPA buffer
according to the manufacturer's instructions (Wako Pure Chemical
Industries, Ltd., Osaka, Japan). Ten µg cytosolic fractions were
and loaded onto Mini-PROTEIN TGXTM gel (Bio-Rad Laboratories).
After electrophoresis, proteins were transferred to PVDF membranes
using Trans-Blot® TurboTM Transfer System Transfer Pack
(Bio-Rad Laboratories). Subsequently, the membranes were blocked
for 1 h in 4% BSA in TBS with 0.5% Tween-20 (PBS-T) and incubated
overnight at 4°C in primary antibody in TBS-T with 4% BSA. The
following antibodies and concentrations were used: 1/2,500 rabbit
STAT3 (Abcam), 1/2,500 rabbit p-STAT3, 1/2,500 rabbit anti-XIAP,
1/2,500 rabbit cleaved PARP, and 1/5,000 rabbit β-actin (all Cell
Signaling Technology). After three washes with TBS-T, membranes
were incubated for 1 h at room temperature using HRP-conjugated
anti-rabbit secondary antibody as appropriate. After three washes
with TBS-T, they were visualized using the ECL detection system (GE
Healthcare UK Ltd., Chalfont, UK) by a LAS-3000 (Fujifilm, Tokyo,
Japan). Protein expression was determined densitometrically and
normalized against β-actin expression using Multi Gauge version 3.1
(Fujifilm).
Statistical analysis
Statistical analyses were performed using JMP Pro,
version 11 (SAS Institution Inc., Cary, NC, USA). Progression-free
survival (PFS) was defined as the interval between initial surgery
and the date of disease progression. Overall survival (OS) was
defined as the interval between initial surgery and death. The
serum tumor markers including CA125 were not used for the
definition of disease progression. Comparisons were evaluated with
the chi-square test or the Fisher's exact probability test when
appropriate. PFS and OS curves were generated using the method of
Kaplan-Meier. The comparison of the survival distributions was made
using a log-rank test. Cox's proportional hazards model was used
for univariate and multivariate analysis. P<0.05 was considered
to indicate a statistically significant difference.
Results
A total of 341 patients with epithelial ovarian
cancers were identified. Among them, positive nuclear p-STAT3
expression was observed in 95 cases (28%), positive nuclear p-JAK2
expression was in 284 (83%). Expression pattern of p-STAT3 and
p-JAK2 according to histological subtypes were shown in Table II. There was a significant
association of p-JAK2 expression and p-STAT3 in all samples
(P=0.034). Significant association of these protein expressions was
only observed in clear-cell histology (P=0.004). There were no
significant differences in age, FIGO stage, RT size at primary
surgery, histological subtype and primary chemotherapy according to
p-STAT3 expression (data not shown).
| Table II.Expressions of p-JAK2 and p-STAT3
according to histological subtypes. |
Table II.
Expressions of p-JAK2 and p-STAT3
according to histological subtypes.
|
| Histology |
|
|---|
|
|
|
|
|---|
| p-JAK2/p-STAT3 | Serous n=144 | Clear-cell
n=85 | Endometrioid
n=52 | Mucinous n=60 | Total n=144 |
|---|
|
Positive/positive | 34 | 27 | 16 | 9 | 86 |
|
Positive/negative | 93 | 36 | 26 | 43 | 198 |
|
Negative/positive | 3 | 2 | 1 | 3 | 9 |
|
Negative/negative | 14 | 20 | 9 | 5 | 48 |
|
P-valuea | 0.560 | 0.004 | 0.138 | 0.191 | 0.034 |
The patients with negative p-STAT3 had slightly
better PFS compared with the cases with positive p-STAT3, although
the difference was not statistically significant (P=0.055; hazard
ratio, 1.37; 95% confidence interval, 0.98–1.90; Fig. 1A). The patients with negative p-STAT3
had significantly improved OS compared with those with positive
p-STAT3 (P=0.002; hazard ratio, 1.75; 95% confidence interval,
1.22–2.48; Fig. 1B). In contrast,
positive p-JAK2 did not influence OS (P=0.142; hazard ratio, 1.47;
95% confidence interval, 0.90–2.59) and PFS (P=0.414, hazard ratio,
1.20; 95% confidence interval, 0.79–1.89; P=0.409) in the analyses
in all the patients. Multivariate analyses for OS revealed that
positive expression of p-STAT3 was identified as an independent
prognostic factor (hazard ratio, 1.48; 95% confidence interval,
1.02–2.11; P=0.039, Table III), in
addition to stage, histology, and RT diameter.
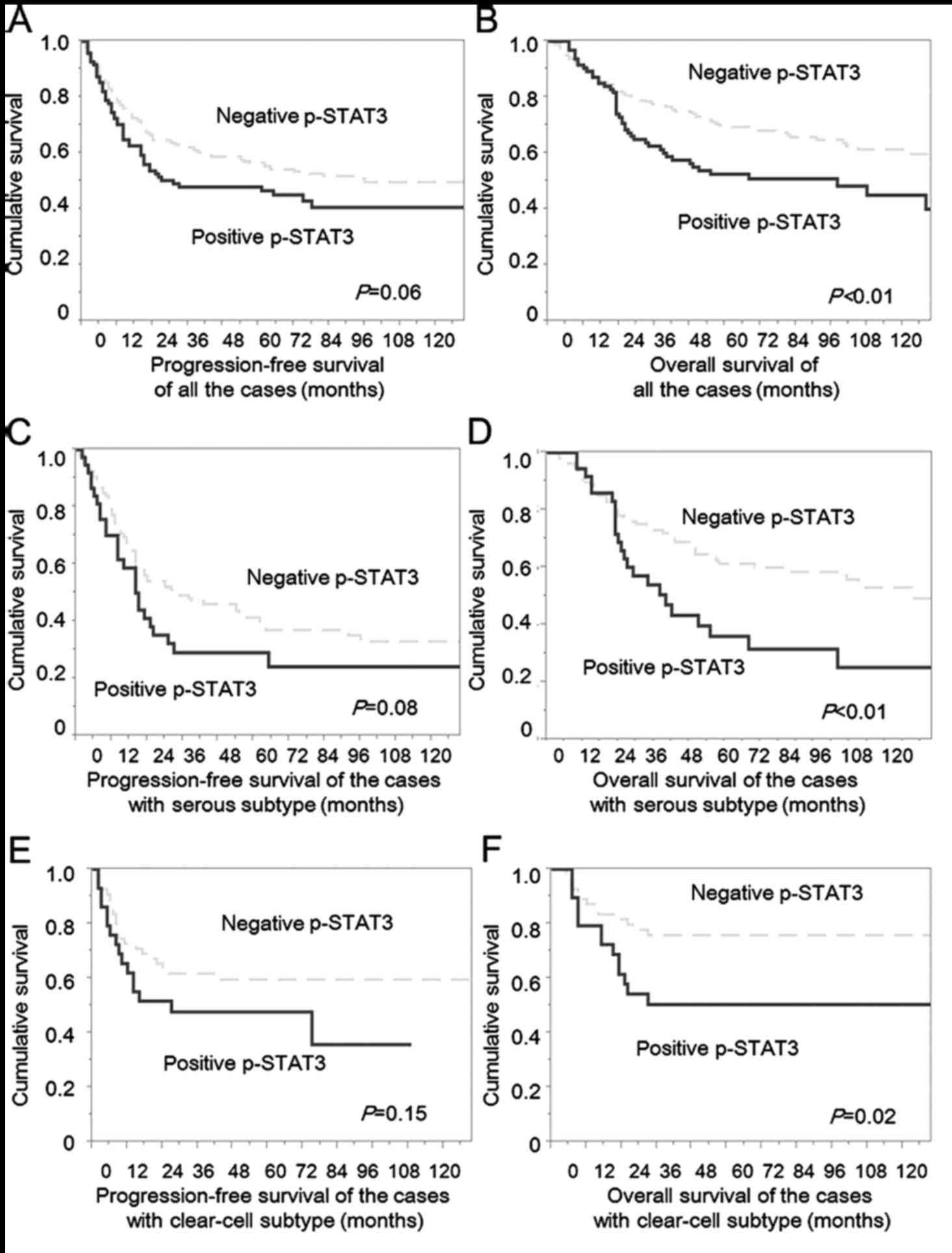 | Figure 1.PFS and OS curves of the cases with
ovarian cancers according to p-STAT3 expression. (A) PFS of all the
patients. The patients with negative p-STAT3 had a slightly better
progression-free survival compared with the cases with positive
p-STAT3, although the difference was not statistically significant
(P=0.055; hazard ratio, 1.37; 95% confidence interval, 0.98–1.90).
(B) OS of all the patients. The patients with negative p-STAT3 had
significantly better OS compared with the cases with positive
p-STAT3 (P=0.002; hazard ratio, 1.75; 95% confidence interval,
1.22–2.48). (C) PFS of the patient with serous subtype. The
patients with negative p-STAT3 had slightly better progression-free
survival compared with the cases with positive p-STAT3, although
the difference was not statistically significant (P=0.077; hazard
ratio, 1.49; 95% confidence interval, 0.93–2.31). (D) OS of the
patient with serous subtype. The patients with negative p-STAT3 had
significantly better OS compared with the cases with positive
p-STAT3 (P=0.002; hazard ratio, 2.10; 95% confidence interval,
1.27–3.42). (E) PFS of the patient with clear-cell subtype. The
patients with negative p-STAT3 had slightly better progression-free
survival compared with the cases with positive p-STAT3, although
the difference was not statistically significant (P=0.147; hazard
ratio, 1.59; 95% confidence interval, 0.83–3.03). (F) OS of the
patient with clear-cell subtype. The patients with negative p-STAT3
had significantly better OS compared with the cases with positive
p-STAT3, although the difference was not statistically significant
(P=0.019; hazard ratio, 2.32; 95% confidence interval, 1.11–4.89).
Dotted line, cases with negative p-STAT3; solid line, cases with
positive p-STAT3. PFS, progression-free survival; OS, overall
survival; p-STAT3, phosphorylated STAT3. |
| Table III.Univariate and Multivariate analyses
for overall survival according to histological subtypes. |
Table III.
Univariate and Multivariate analyses
for overall survival according to histological subtypes.
|
| All subtypes | Serous subtype | Clear-cell
subtype |
|---|
|
|
|
|
|
|---|
|
| Univariate
analysis | Multivariate
analysis | Univariate
analysis | Multivariate
analysis | Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (years) |
|
|
|
|
|
|
|
|
|
|
|
|
| ≥53 vs.
<53 | 1.44 | 0.040 | 1.29 | 0.155 | 1.33 | 0.26 | 1.30 | 0.30 | 0.75 | 0.45 | 0.72 | 0.40 |
|
| (1.02–2.06) |
| (0.91–1.55) |
| (0.82–2.21) |
| (0.79–2.19) |
| (0.36–1.56) |
| (0.32–1.55) |
|
| FIGO stage |
|
|
|
|
|
|
|
|
|
|
|
|
| II–IV
vs. I | 5.30 | <0.001 | 3.63 | <0.001 | 5.52 | 0.002 | 3.31 | 0.057 | 6.88 | <0.001 | 5.33 | 0.001 |
|
| (3.23–9.30) |
| (2.07–6.69) |
| (1.73–33.6) |
| (0.97–20.70) |
| (2.81–20.7) |
| (1.94–17.13) |
|
| Histological
subtype |
|
|
|
|
|
|
|
|
|
|
|
|
|
Clear-cell vs. others | 0.95 | 0.828 | 1.59 | 0.045 | NA |
| NA |
| NA |
| NA |
|
|
| (0.62–1.42) |
| (1.01–2.50) |
|
|
|
|
|
|
|
|
|
| RT (cm) |
|
|
|
|
|
|
|
|
|
|
|
|
| ≥1 vs.
<1 | 5.12 | <0.001 | 3.25 | <0.001 | 4.57 | <0.001 | 3.73 | <0.001 | 6.75 | <0.001 | 3.00 | 0.014 |
|
| (3.61–7.30) |
| (2.02–4.84) |
| (2.80–7.54) |
| (2.22–6.35) |
| (2.99–14.7) |
| (1.26–7.09) |
|
| Primary
chemotherapy |
|
|
|
|
|
|
|
|
|
|
|
|
| Others
vs. taxane + platinum | 1.10 | 0.628 | 1.34 | 0.151 | 1.46 | 0.12 | 1.59 | 0.063 | 0.91 | 0.86 | 0.86 | 0.80 |
|
| (0.75–1.67) |
| (0.89–2.06) |
| (0.90–2.40) |
| (0.98–2.62) |
| (0.35–3.09) |
| (0.29–3.13) |
|
| p-STAT3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Positive vs. negative | 1.75 | 0.003 | 1.48 | 0.039 | 2.12 | 0.005 | 1.42 | 0.20 | 2.32 | 0.026 | 2.31 | 0.039 |
|
| (1.22–2.48) |
| (1.02–2.11) |
| (1.27–3.42) |
| (0.83–2.36) |
| (1.11–4.89) |
| (1.05–5.09) |
|
In the analyses of serous type, positive p-STAT3 was
observed in 37 cases (26%), and positive nuclear p-JAK2 expression
was detected in 127 cases (88%). Primary surgery was suboptimal in
21 (57%) of 37 positive p-STAT3 and in 38 (36%) of 107 negative
p-STAT3. Positive expression of p-STAT3 was significantly
associated with larger RT size (P=0.024, complete+optimal vs.
suboptimal). There were no significant differences in age, FIGO
stage, chemotherapy and positive p-JAK2 according to positive
p-STAT3. The patients with negative p-STAT3 had slightly better PFS
compared with the cases with positive p-STAT3, although the
difference was not statistically significant (P=0.077; hazard
ratio, 1.49; 95% confidence interval, 0.93–2.31; Fig. 1C). Additionally, the patients with
negative p-STAT3 had significantly better OS compared with the
cases with positive p-STAT3 (P=0.002; hazard ratio, 2.10; 95%
confidence interval, 1.27–3.42 Fig.
1D). In multivariate analyses, positive p-STAT3 was not
selected as an independent prognostic factor for both OS and PFS in
the analyses of the patients with serous histology (Tables III and IV).
| Table IV.Univariate and multivariate analyses
for progression-free survival according to histological
subtypes. |
Table IV.
Univariate and multivariate analyses
for progression-free survival according to histological
subtypes.
|
| All subtypes | Serous subtype | Clear-cell
subtype |
|---|
|
|
|
|
|
|---|
|
| Univariate
analysis | Multivariate
analysis | Univariate
analysis | Multivariate
analysis | Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (years) |
|
|
|
|
|
|
|
|
|
|
|
|
| ≥53 vs.
<53 | 1.44 | 0.021 | 1.26 | 0.15 | 1.44 | 0.092 | 1.46 | 0.085 | 0.79 | 0.46 | 0.66 | 0.23 |
|
| (1.05–1.98) |
| (0.92–1.74) |
| (0.94–2.23) |
| (0.95–2.29) |
| (0.41–1.48) |
| (0.34–1.29) |
|
| FIGO stage |
|
|
|
|
|
|
|
|
|
|
|
|
| II–IV
vs. I | 5.14 | <0.001 | 3.87 | <0.001 | 4.07 | <0.001 | 2.61 | 0.041 | 4.99 | <0.001 | 4.60 | <0.001 |
|
| (3.37–8.19) |
| (2.42–6.40) |
| (1.70–13.3) |
| (1.04–8.78) |
| (2.50–10.8) |
| (2.12–10.58) |
|
| Histological
subtype |
|
|
|
|
|
|
|
|
|
|
|
|
|
Clear-cell vs. others | 1.00 | 0.995 | 1.65 | 0.014 | NA |
| NA |
| NA |
| NA |
|
|
| (0.71–1.45) |
| (1.11–2.40) |
|
|
|
|
|
|
|
|
|
| RT (cm) |
|
|
|
|
|
|
|
|
|
|
|
|
| ≥1 vs.
<1 | 3.80 | <0.001 | 2.44 | <0.001 | 2.87 | <0.001 | 2.56 | <0.001 | 4.65 | <0.001 | 2.10 | 0.073 |
|
| (2.77–5.20) |
| (1.73–3.45) |
| (1.88–4.36) |
| (1.63–4.04) |
| (2.17–9.31) |
| (0.93–4.56) |
|
| Primary
chemotherapy |
|
|
|
|
|
|
|
|
|
|
|
|
| Others
vs. taxane + platinum | 0.73 | 0.076 | 0.89 | 0.54 | 1.10 | 0.076 | 0.94 | 0.79 | 1.03 | 0.96 | 0.77 | 0.63 |
|
| (0.97–1.87) |
| (0.64–1.28) |
| (0.73–1.67) |
| (0.62–1.44) |
| (0.44–3.00) |
| (0.30–2.41) |
|
| p-STAT3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Positive vs. negative | 1.37 | 0.063 | 1.22 | 0.24 | 1.49 | 0.092 | 1.07 | 0.77 | 1.60 | 0.16 | 1.62 | 0.18 |
|
| (0.98–1.90) |
| (0.87–1.70) |
| (0.93–2.31) |
| (0.65–1.70) |
| (0.82–3.03) |
| (0.80–3.20) |
|
In the analyses of a total of 85 patients with
clear-cell histology, positive nuclear p-STAT3 was observed in 29
cases (34%), and positive nuclear p-JAK2 expression was in observed
in 63 cases (74%). Positivity of p-STAT3 was significantly related
with positivity of p-JAK2 (P=0.004) (Table II). There were no significant
differences in age, FIGO stage and RT size according to p-STAT3
expression. The patients with negative p-STAT3 had slightly better
PFS compared with the cases with positive p-STAT3, although the
difference was not statistically significant (P=0.147; hazard
ratio, 1.59; 95% confidence interval, 0.83–3.03) (Fig. 1E). Further, the patients with negative
p-STAT3 had significantly better OS compared with the cases with
positive p-STAT3 (P=0.019; hazard ratio, 2.32; 95% confidence
interval, 1.11–4.89; Fig. 1F).
Multivariate analyses for OS revealed that positive expression of
p-STAT3 was identified as an independent prognostic factor (hazard
ratio, 2.31; 95% confidence interval, 1.05–5.09; P=0.039), in
addition to stage, histology (Table
III).
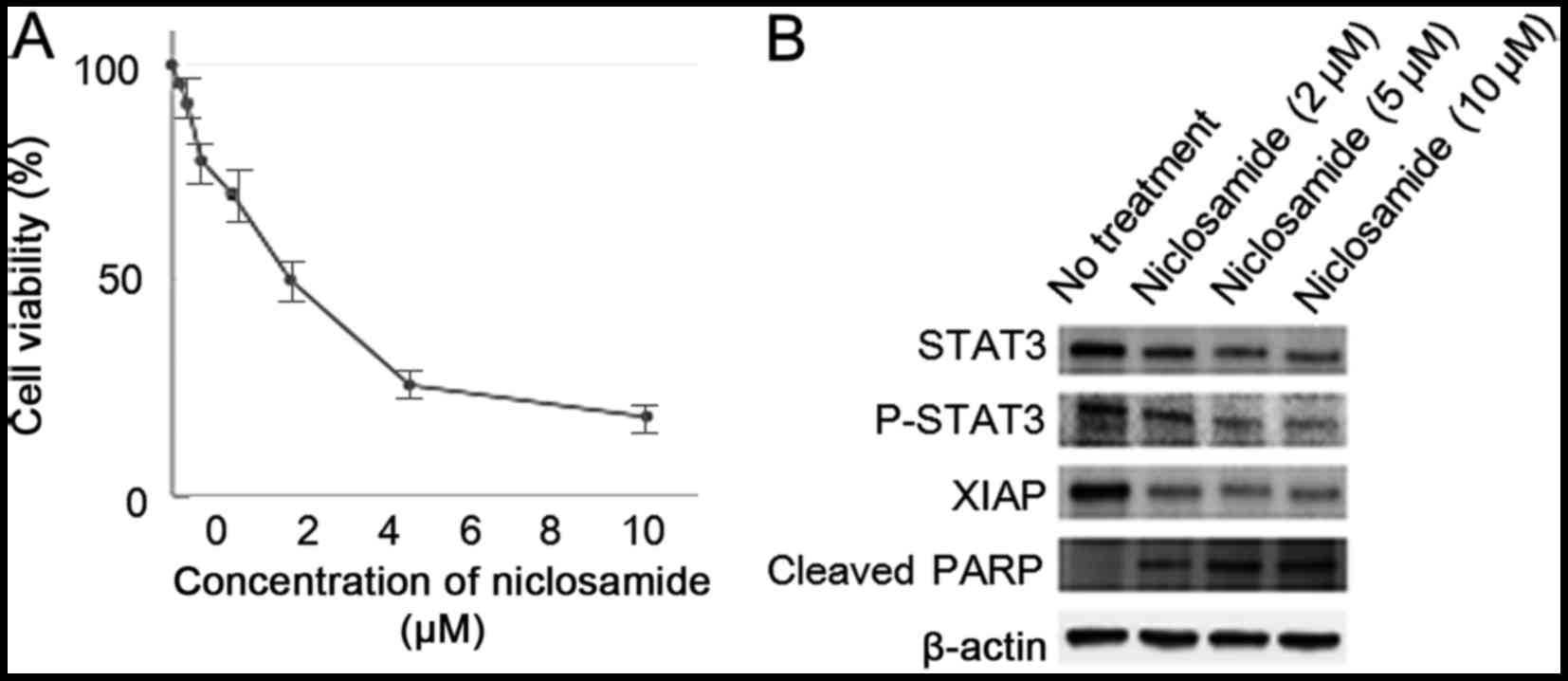
Cell viability of KK cells decreased by the
treatment with niclosamide in a dose-dependent manner. Experiments
were repeated three times with similar results. Additionally,
niclosamide treatment decreased expression of p-STAT3, and
inhibitor of apoptosis protein XIAP, and increased apoptosis
related protein cleaved PARP in a dose-dependent manner in KK cells
(Fig. 2).
Discussion
In the present study, activation of STAT3 was
identified as an independent prognostic factor for ovarian cancers,
especially in the patients with clear cell histology. To our
knowledge, it is the first report to demonstrate the correlation
between the activation of STAT3 and unfavorable survival for OS by
multivariate analysis in ovarian cancers including four major
histological subtypes. Hazard ratio by p-STAT3 status for OS in
multivariate analyses in all cases, clear-cell type and serous type
was 1.48, 2.31 and 1.42. These results lead us to conclude that the
activation of STAT3 plays critical roles in survival in ovarian
cancers with clear-cell type in particular. Positive rate of
p-STAT3 in all cases, clear-cell subtype, and serous type was 28,
34 and 26% in the present study. Previous reports documented that
positive rate of p-STAT3 expression ranged from 29 to 58% of all
histological subtypes, and from 39 to 90% in clear-cell subtype
(10,11,13,19).
Although the frequency of positive p-STAT3 in the present study was
a slightly lower than those of the published findings, the criteria
of the present study clearly enabled us to distinguish the patients
with worse OS from all ovarian cancer patients, and especially from
the patients with clear cell histology.
Previous reports demonstrated that positive nuclear
p-STAT3 expression was associated with histological grade, lymph
node metastasis, clear-cell type, serous type and stage (10,11). In
the present study, positive p-STAT3 was associated with RT size
after primary surgery in serous type. To the best of our knowledge,
it is the first report to demonstrate the association between the
activation of STAT3 and RT status after primary surgery in ovarian
cancers. In the present study, the low affinity between positive
p-STAT3 and poor outcome in serous type by multivariate analysis is
probably attributable to the relevance that depends strongly on RT
size.
It was demonstrated that niclosamide had therapeutic
activities via apoptosis in cancer cell line established from
ascites of a patient with ovarian clear cell carcinoma showing less
sensitivity to cisplatin (18).
Additionally, oral niclosamide inhibited tumor growth and
progression in an intraperitoneal xenograft mouse model
representative of human ovarian cancer without significant side
effects (20). Recently, niclosamide
has been shown to inhibit several pathways including NF-κB, Notch,
ROS, mTORC1, and Wnt/β-catenin pathway (16,21–25). So
there might be several mechanisms of anti-neoplastic activity in
niclosamide other than inhibition of JAK2/STAT3 pathway.
Several studies evaluated inhibition of JAK2/STAT3
pathway in ovarian cancers, and it is suggested that activation of
STAT3 was associated with proliferation, chemo-resistance, and
cancer stem-cell phenotype (26–30). So,
it was speculated that worse PFS in the patients with positive
p-STAT3 tumors was contributed by a high abundance of the patients
that showed chemo-resistance of primary tumors, although
significance was not obtained (P=0.055). Additionally,
significantly worse OS in the patients with positive p-STAT3 tumors
might be attributed by acquired chemo-resistance caused by
stem-cell phenotype in recurrent tumors. Also, a study demonstrated
that inhibition of STAT3 activation by JAK2-specific inhibitor
AG490 blocked STAT3 phosphorylation, cell motility, and induction
IL-6 production (31). So, IL-6
pathway might have contributed to worse prognoses of clear-cell
ovarian cancers. Finally, a kinase inhibitor of JAK1 and JAK2,
Ruxolitinib Phosphate, is now evaluated in phase 1/2 study for
Mullerian cancers in combination with paclitaxel and carboplatin
(32). Nevertheless, it is speculated
that niclosamide would show activity against ovarian cancer
patients whose tumors had JAK2/STAT3 activation.
The activation of JAK2/STAT3 pathway had significant
impact on survival of ovarian cancers, especially for the cases
with clear-cell histology. Although further analyses are needed,
suppression of this pathway could be a candidate for the treatment
of ovarian cancers, especially chemotherapy-resistant clear cell
type.
Acknowledgements
The authors would like to thank Ms. Hiromi Kubota
for their contribution to this study.
References
|
1
|
Jelovac D and Armstrong DK: Recent
progress in the diagnosis and treatment of ovarian cancer. CA
Cancer J Clin. 61:183–203. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pignata S, Cannella L, Leopardo D, Pisano
C, Bruni GS and Facchini G: Chemotherapy in epithelial ovarian
cancer. Cancer Lett. 303:73–83. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tothill RW, Tinker AV, George J, Brown R,
Fox SB, Lade S, Johnson DS, Trivett MK, Etemadmoghadam D, Locandro
B, et al: Novel molecular subtypes of serous and endometrioid
ovarian cancer linked to clinical outcome. Clin Cancer Res.
14:5198–5208. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bast RC Jr, Hennessy B and Mills GB: The
biology of ovarian cancer: New opportunities for translation. Nat
Rev Cancer. 9:415–428. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Takano M, Kikuchi Y, Yaegashi N, Kuzuya K,
Ueki M, Tsuda H, Suzuki M, Kigawa J, Takeuchi S, Tsuda H, et al:
Clear cell carcinoma of the ovary: A retrospective multicentre
experience of 254 patients with complete surgical staging. Br J
Cancer. 94:1369–1374. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Takano M, Sugiyama T, Yaegashi N, Suzuki
M, Tsuda H, Sagae S, Udagawa Y, Kuzuya K, Kigawa J, Takeuchi S, et
al: The impact of complete surgical staging upon survival in
early-stage ovarian clear cell carcinoma: A multi-institutional
retrospective study. Int J Gynecol Cancer. 19:1353–1357. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Takano M, Tsuda H and Sugiyama T: Clear
cell carcinoma of the ovary: Is there a role of histology-specific
treatment? J Exp Clin Cancer Res. 31:532012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yu H and Jove R: The STATs of cancer-new
molecular targets come of age. Nat Rev Cancer. 4:97–105. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kong H, Zhang Q, Zeng Y, Wang H, Wu M,
Zheng T, Zeng Y and Shi H: Prognostic significance of
STAT3/phosphorylated-STAT3 in tumor: A meta-analysis of
literatures. Int J Clin Exp Med. 8:8525–8539. 2015.PubMed/NCBI
|
|
10
|
Rosen DG, Mercado-Uribe I, Yang G, Bast RC
Jr, Amin HM, Lai R and Liu J: The role of constitutively active
signal transducer and activator of transcription 3 in ovarian
tumorigenesis and prognosis. Cancer. 107:2730–2740. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Min H and Wei-hong Z: Constitutive
activation of signal transducer and activator of transcription 3 in
epithelial ovarian carcinoma. J Obstet Gynaecol Res. 35:918–925.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Permuth-Wey J, Fulp WJ, Reid BM, Chen Z,
Georgeades C, Cheng JQ, Magliocco A, Chen DT and Lancaster JM:
STAT3 polymorphisms may predict an unfavorable response to
first-line platinum-based therapy for women with advanced serous
epithelial ovarian cancer. Int J Cancer. 138:612–619. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yanaihara N, Hirata Y, Yamaguchi N,
Noguchi Y, Saito M, Nagata C, Takakura S, Yamada K and Okamoto A:
Antitumor effects of interleukin-6 (IL-6)/interleukin-6 receptor
(IL-6R) signaling pathway inhibition in clear cell carcinoma of the
ovary. Mol Carcinog. 55:832–841. 2016. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
You S, Li R, Park D, Xie M, Sica GL, Cao
Y, Xiao ZQ and Deng X: Disruption of STAT3 by niclosamide reverses
radioresistance of human lung cancer. Mol Cancer Ther. 13:606–616.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lateef M, Zargar SA, Khan AR, Nazir M and
Shoukat A: Successful treatment of niclosamide- and
praziquantel-resistant beef tapeworm infection with nitazoxanide.
Int J Infect Dis. 12:80–82. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ren X, Duan L, He Q, Zhang Z, Zhou Y, Wu
D, Pan J, Pei D and Ding K: Identification of niclosamide as a new
small-molecule inhibitor of the STAT3 signaling pathway. ACS Med
Chem Lett. 1:454–459. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xiang D, Yuan Y, Chen L, Liu X, Belani C
and Cheng H: Niclosamide, an anti-helminthic molecule,
downregulates the retroviral oncoprotein Tax and pro-survival Bcl-2
proteins in HTLV-1-transformed T lymphocytes. Biochem Biophys Res
Commun. 464:221–228. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sasa H, Ishii K, Hirata J, Kikuchi Y,
Nagata I, Kawai T, Senoo A, Sugita M, Sugishita T and Tenjin Y:
Establishment and characterization of a CA-125-producing human
ovarian clear cell carcinoma cell line. Hum Cell. 6:279–286.
1993.(In Japanese). PubMed/NCBI
|
|
19
|
Anglesio MS, George J, Kulbe H,
Friedlander M, Rischin D, Lemech C, Power J, Coward J, Cowin PA,
House CM, et al: IL6-STAT3-HIF signaling and therapeutic response
to the angiogenesis inhibitor sunitinib in ovarian clear cell
cancer. Clin Cancer Res. 17:2538–2548. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Arend RC, Londoño-Joshi AI, Samant RS, Li
Y, Conner M, Hidalgo B, Alvarez RD, Landen CN, Straughn JM and
Buchsbaum DJ: Inhibition of Wnt/β-catenin pathway by niclosamide: A
therapeutic target for ovarian cancer. Gynecol Oncol. 134:112–120.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
King ML, Lindberg ME, Stodden GR, Okuda H,
Ebers SD, Johnson A, Montag A, Lengyel E, MacLean Ii JA and Hayashi
K: WNT7A/β-catenin signaling induces FGF1 and influences
sensitivity to niclosamide in ovarian cancer. Oncogene.
34:3452–3462. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jin Y, Lu Z, Ding K, Li J, Du X, Chen C,
Sun X, Wu Y, Zhou J and Pan J: Antineoplastic mechanisms of
niclosamide in acute myelogenous leukemia stem cells: Inactivation
of the NF-kappaB pathway and generation of reactive oxygen species.
Cancer Res. 70:2516–2527. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen M, Wang J, Lu J, Bond MC, Ren XR,
Lyerly HK, Barak LS and Chen W: The anti-helminthic niclosamide
inhibits Wnt/Frizzled1 signaling. Biochemistry. 48:10267–10274.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sack U, Walther W, Scudiero D, Selby M,
Kobelt D, Lemm M, Fichtner I, Schlag PM, Shoemaker RH and Stein U:
Novel effect of antihelminthic Niclosamide on S100A4-mediated
metastatic progression in colon cancer. J Natl Cancer Inst.
103:1018–1036. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pan JX, Ding K and Wang CY: Niclosamide,
an old antihelminthic agent, demonstrates antitumor activity by
blocking multiple signaling pathways of cancer stem cells. Chin J
Cancer. 31:178–184. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fujiwara Y, Takaishi K, Nakao J, Ikeda T,
Katabuchi H, Takeya M and Komohara Y: Corosolic acid enhances the
antitumor effects of chemotherapy on epithelial ovarian cancer by
inhibiting signal transducer and activator of transcription 3
signaling. Oncol Lett. 6:1619–1623. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Abubaker K, Luwor RB, Escalona R, McNally
O, Quinn MA, Thompson EW, Findlay JK and Ahmed N: Targeted
disruption of the JAK2/STAT3 pathway in combination with systemic
administration of paclitaxel inhibits the priming of ovarian cancer
stem cells leading to a reduced tumor burden. Front Oncol.
4:752014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Abubaker K, Luwor RB, Zhu H, McNally O,
Quinn MA, Burns CJ, Thompson EW, Findlay JK and Ahmed N: Inhibition
of the JAK2/STAT3 pathway in ovarian cancer results in the loss of
cancer stem cell-like characteristics and a reduced tumor burden.
BMC Cancer. 14:3172014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gritsina G, Xiao F, O'Brien SW, Gabbasov
R, Maglaty MA, Xu RH, Thapa RJ, Zhou Y, Nicolas E, Litwin S, et al:
Targeted blockade of JAK/STAT3 signaling inhibits ovarian carcinoma
growth. Mol Cancer Ther. 14:1035–1047. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhong LX, Li H, Wu ML, Liu XY, Zhong MJ,
Chen XY, Liu J and Zhang Y: Inhibition of STAT3 signaling as
critical molecular event in resveratrol-suppressed ovarian cancer
cells. J Ovarian Res. 8:252015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Colomiere M, Ward AC, Riley C, Trenerry
MK, Cameron-Smith D, Findlay J, Ackland L and Ahmed N: Cross talk
of signals between EGFR and IL-6R through JAK2/STAT3 mediate
epithelial-mesenchymal transition in ovarian carcinomas. Br J
Cancer. 100:134–144. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
U.S. National Library of Medicine,
National Cancer Institute (NCI), . Ruxolitinib phosphate,
paclitaxel, and carboplatin in treating patients with stage III–IV
epithelial ovarian, fallopian tube, or primary peritoneal cancer.
https://clinicaltrials.gov/ct2/show/NCT02713386March
18–2016
|