Introduction
Worldwide, gastric cancer (GC) remains a leading
cause of cancer death, second only to lung cancer (1). Recurrence of GC often appears in the
form of peritoneal dissemination, liver, lymph nodes and bone
recurrence metastases are often seen (1). Central nervous system (CNS) metastasis
from advanced gastric or gastro-esophageal (GE) junction cancer is
extremely rare, occurring in 0.16–0.69% of patients (2–5). CNS
metastasis is often multiple and associated with metastasis to
other organs and a resection is uncommon. Response to treatment is
poor: the prognosis is often dismal, as the median survival time
ranges from 1.3 to 2.4 months (2–6). Among
patients with gastric or GE junction cancer and brain metastasis,
the mean interval from gastrectomy to the occurrence of brain
metastasis is reported to be 9 months (range 1–23 months) in the
United States study (3), and 9.6
months (range 0.1–43.7 months) in the Japanese study (2). Several reports (2–4) and two
reviews (5,6) have described CNS metastases from GC;
however, in these studies, the correlation between human epidermal
growth factor 2 (HER-2 status) and CNS metastases is lacking; and
reports on CNS involvement from HER-2 positive GC are fragmentary
and very poor (7).
Overexpression/amplification of HER-2 in breast
cancer, resulting in HER-2-positive subtypes, is associated with
more aggressive behaviour when compared with HER-2-negative breast
cancer and is also associated with increased risk of local growth
and distant metastasis; furthermore, HER-2-positive breast cancer
also appears to be associated with an increased risk of developing
CNS metastases (8–12). The higher incidence of CNS metastasis
from HER-2 positive breast cancer was also reported to be
associated with Trastuzumab-based therapy (13). The humanized anti-HER-2 monoclonal
antibody Trastuzumab is an effective treatment for patients with
HER-2 positive breast cancer (14,15) and
more recently, Trastuzumab in combination with chemotherapy
improved progression-free survival and overall survival (OS) in
patients with HER-2 positive advanced gastric or GE junction cancer
(16).
To our knowledge to date, there are no studies that
evaluate the correlation between HER-2 expression in gastric and GE
junction cancer with CNS metastases. The purposes of this
retrospective study are to assess the incidence of CNS metastases
in a series of consecutive patients with gastric or GE junction
cancer and to correlate the CNS involvement with HER-2 status.
Materials and methods
Study design
The objectives of this retrospective study are to
evaluate the incidence of CNS metastases in a series of patients
with gastric or GE junction cancer and to evaluate the relationship
between HER-2 status with this incidence.
After obtaining internal ethical committee approval
for the study, the records of 300 consecutive patients with gastric
or GE junction cancer diagnosed between January 1, 2007 and
December 31, 2013 admitted to the Piacenza General Hospital, Italy,
were reviewed. Date of gastroscopy, histologic diagnosis, stage at
diagnosis, treatment of primary and metastatic cancer and follow-up
were collected in an electronic data base. The site of metastasis
was categorized as loco-regional/lymph nodes or distant, visceral
and CNS. Diagnosis of CNS recurrence was based on either computed
tomography and/or magnetic resonance imaging scans of the brain.
CNS imaging studies were performed in patients who developed
neurological signs showing clinical suspicion of CNS recurrence,
such as headache, gait disturbance, hemiparesis, aphasia, visual
troubles and/or muscular weakness. Histological samples of gastric
or GE junction tumours in patients with CNS metastases were
reviewed and tested for HER-2. HER-2 positive disease was defined
according to the ToGA trial criteria (16).
The clinical course, treatment, and OS of patients
with gastric or GE junction cancer and CNS metastases were also
analyzed and reported.
Statistical analysis
The clinical course of patients with CNS metastases
was calculated from the initial diagnostic gastroscopy that
confirmed the cancer. OS of these patients was calculated from the
date of diagnosis of GC and death. To evaluate the prognosis of CNS
involvement, survival was furthermore calculated from date of the
diagnosis of CNS metastases by imaging studies to date of death.
The median OS was calculated by the Kaplan-Meier method using STATA
Release 11 software.
Results
Between 2007 and 2013, 300 patients were diagnosed
with gastric or GE junction cancer at the Piacenza General
Hospital. Diagnosis was done by esophagogastroduodenoscopy (EGDS)
and biopsies. Seven out of 300 patients (2.33%) were found to have
CNS metastases on imaging studies performed in symptomatic
patients. The characteristics of the subjects are shown in Table I.
 | Table I.Characteristics of patients with
gastric or gastro-esophageal junction cancer and CNS
metastases. |
Table I.
Characteristics of patients with
gastric or gastro-esophageal junction cancer and CNS
metastases.
| Characteristic | Number of patients
(n=7) |
|---|
| Sex |
|
|
Female | 4 |
| Male | 3 |
| Median age, years
(range) | 55 (46–77) |
| Site of primary
gastric cancer |
|
|
Cardia | 5 |
|
Corpus | 1 |
|
Antrum | 1 |
| Histological
type |
|
|
Intestinal | 4 |
|
Diffuse | 3 |
| Stage at
diagnosis |
|
| I | 0 |
| II | 0 |
| III | 0 |
| IV | 7 |
| Metastasis sites
prior to CNS |
|
|
Liver | 4 |
|
Peritoneum | 4 |
|
Lymphonodes | 4 |
| Lung | 3 |
| Bone | 1 |
| Prior to
chemotherapy | 4 |
| Prior to chemotherapy
and | 2 |
| Trastuzumab |
|
| Neurological symptoms
of CNS involvement |
|
| Headache,
muscular weakness, gait disturbance | 4 |
|
Hemiparesis, aphasia | 2 |
| Visual
troubles | 1 |
There were four women and three men, the median age
was 55 years (range 46–77 years).
Primary sites of gastric tumour were cardia (5
patients), corpus (1 patient) and antrum (1 patient); histological
types were intestinal in 4 and diffuse in 3 cases.
All seven patients with CNS involvement had advanced
disease at diagnosis, with metastases in other organs: liver,
peritoneum and lymphonodes (4 patients), lung (3 patients),
lymphonodes and bone (1 case). Four patients received chemotherapy
and two chemotherapy plus Trastuzumab before CNS involvement.
All patients had neurological symptoms of CNS
involvement: headache, gait disturbance and muscular weakness were
the initial manifestations in four patients, hemiparesis and
aphasia in two cases and visual troubles in the remaining patient.
Six patients showed multiple intracranial lesions and one had
leptomeningeal carcinomatosis. Six out of seven patients with CNS
metastases (85.71%) showed HER-2 positivity on immunohistochemistry
(Table II). Treatment of CNS
metastases was based on whole-brain radiation therapy (WBRT) in six
cases: four patients received systemic chemotherapy; two patients
received Trastuzumab plus chemotherapy, and one of those cases also
intratecal chemotherapy plus Trastuzumab, (patients with
leptomeningeal carcinomatosis); one patient was treated with best
palliative care.
| Table II.HER-2 status, management and survival
of 7 patients with gastric or gastro-esophageal junction cancer and
CNS metastasis. |
Table II.
HER-2 status, management and survival
of 7 patients with gastric or gastro-esophageal junction cancer and
CNS metastasis.
| Case no. | Sex | HER-2 status of
gastro-esophageal cancer | Time from diagnosis
of gastro-esophageal cancer to CNS metastasis (months) | Treatment | Time from diagnosis
of gastro-esophageal cancer to mortality (months) | Time from diagnosis
of CNS metastasis to mortality (months) |
|---|
| 1 | F | POS | 7.2 | CT+WBRT | 10.3 | 3.1 |
| 2 | F | POS | 3.2 | CT+WBRT+TRA | 7.7 | 4.5 |
| 3 | F | POS | 0.5 | CT+WBRT | 4.6 | 4.1 |
| 4 | F | POS | 10.3 | CT+WBRT+TRA | 16.8 | 6.5 |
| 5a | M | POS | 6.2 | CT+WBRT+IT-TRA | 9.4 | 3.2 |
| 6 | M | POS |
4.3 | Supportive
care |
6.4 | 2.1 |
| 7 | M | NEG | 12.6 | CT+WBRT | 19.2 | 6.6 |
| Median (range) |
| – | 6.2 (0.5–12.6) | – | 9.4 (4.6–19.2) | 4.1 (2.1–6.6) |
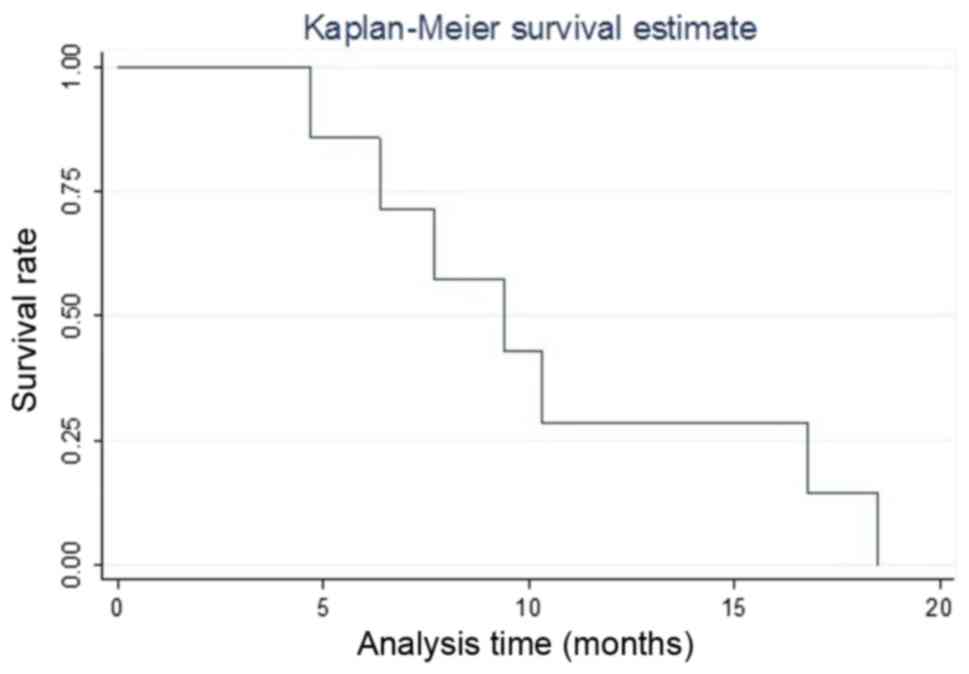
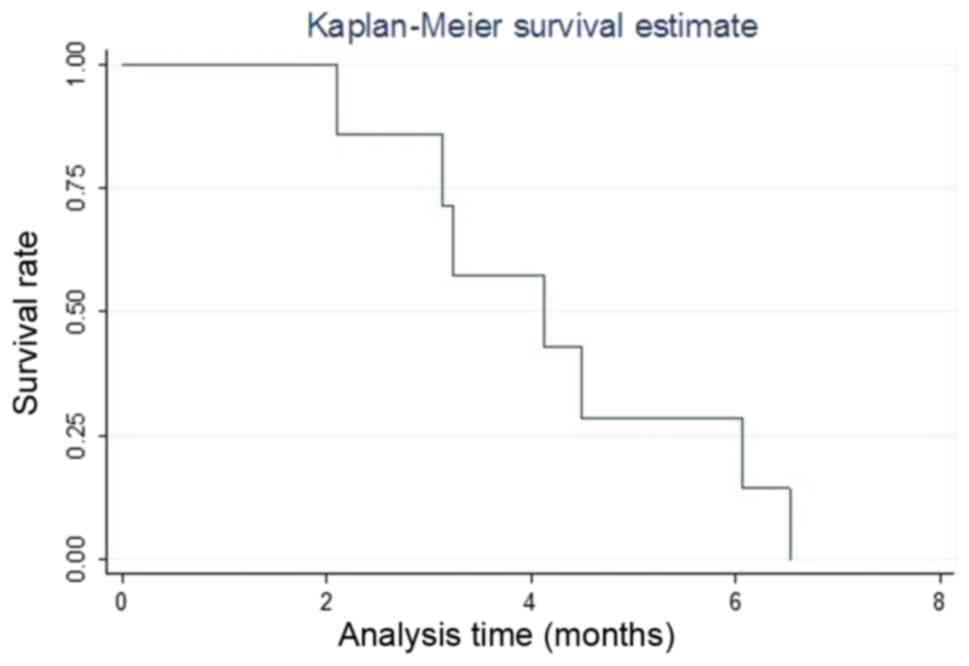
The median time from the diagnosis of gastric or GE
junction cancer to the diagnosis of CNS metastases in the seven
patients was 6.2 months (range 0.5–12.6 months), median OS time
from the diagnosis of GC in the 7 patients was 9.4 months (range:
4.6–19.2 months) (Fig. 1), while the
median OS time from the diagnosis of CNS metastases was 4.1 months
(range 2.1–6.6 months) (Fig. 2).
Discussion
HER-2 has increasingly become an important biomarker
of gastric and GE junction cancers. Current estimations suggest
approximately 16% of gastric and GE junction tumours over-express
HER-2, although the precise figure remains uncertain with reported
frequencies of HER-2-positive GC ranging from 6.0 to 30.0%. A
meta-analysis showed that HER-2 overexpression was associated with
poor prognosis in GC patients. HER-2 positive rates may be
associated with sex, tumor site, TNM staging system, distant
metastasis, lymph node metastasis, Lauren's classification, and
differentiation grade in GC patients. The HER-2 expression rate in
Asians may be higher than that in Europeans (17,18).
CNS metastases are manifestations of
advanced/systemic cancer. Lung cancer, melanoma, kidney cancer and
breast cancer (especially HER-2 positive and triple negative) show
the highest incidence of brain metastases (8,9,13). Other primary neoplasms such as
prostate and gastrointestinal cancer rarely metastatize to the CNS
(13). The increased incidence of
brain metastases in HER-2 amplified breast cancer has been reported
to be multifactorial: direct biological effect, poor CSF
penetration of Trastuzumab, to render the brain a ‘sanctuary site’
for HER-2 neoplastic metastatic cells (13). However it must be emphasized that a
retrospective analysis of 9,524 women with early breast cancer
enrolled in 10 adjuvant trials, identified HER-2 as a risk factor
for the development of CNS metastases independently of Trastuzumab
exposure (19). These data argue for
a biological predisposition to metastatize to the brain of HER-2
positive breast cancer cells. The clinical predilection of HER-2
cancer cells to colonize the brain probably relies on paracrine
mechanism and recently it was suggested that heterodimerization of
HER-2 and tropomyosin-related kinase B (TrkB) receptors gives HER-2
cancer cells a survival advantage in the brain (20). Brain metastases from gastric or GE
junction cancer are very rare; <1% as reported in previous
retrospective studies. York et al (3) reported that only 24 out of 3,320 (0.7%)
GC patients were identified with brain metastasis over a 40-year
period (1957–1997) at the MD Anderson Cancer Center. Likewise,
Kasakura et al (2) identified
brain metastasis in only 11 out of 2,322 (0.47%) patients between
1980 and 1998. It must be emphasized that in these previous
reports, HER-2 status of patients with gastric or GE junction
cancer and brain metastasis was unknown. Our group firstly reported
a case of a patient with HER-2-over-expressing GC who developed
leptomeningeal carcinomatosis (LC) and in this case we demonstrated
the HER-2 positive status of malignant cells in the cerebrospinal
fluid by fluorescence in situ hybridization (21). This patient was treated with
intratecal Trastuzumab plus Methotrexate, dexamethasone and
radiotherapy; however she died 3 months after the diagnosis of LC.
(This patient was not included in the present study). In a recent
systematic review of 2,538 patients with brain metastases from the
gastrointestinal tract, 148 patients (5.83%) had gastric or GE
junction cancer (6); the HER-2 status
of these patients was not reported. In the present study, we report
that in a series of 300 patients with gastric or GE junction
cancer, 7 cases developed brain metastases (2.33%), of which 6
cases had multiple brain solid lesions and one had leptomeningeal
carcinomatosis. We are aware that our series is a small sample; in
fact, only seven cases were included. However, it must be
emphasized that brain metastases from gastric or gastric-esophageal
cancer are very rare. In line with research reported in previous
reviews (5,6) the majority of our patients, 5 of 7
patients (71%) who developed CNS metastases had primary tumours in
the gastric cardia and concurrent systemic metastases were present
in all 7 patients, and most commonly involved the liver,
peritoneum, lymphonodes (56.8%), lung (42.6%) and bone (14.2%). It
must be emphasized that in our series HER-2 status of GC and CNS
metastases is known: 6 of 7 patients (85.71%) showed
HER-2-over-expression of the primary GC.
The first four cases of HER-2-positive GC were
diagnosed and treated prior to the availability of Trastuzumab in
HER-2-positive GC, so these data can argue for a biological
predisposition of HER-2 GC cells, to metastatize to the brain
independently of Trastuzumab therapy such as HER-2-positive breast
cancer cells. The median duration from the diagnosis of GC to the
diagnosis of CNS metastases in our patients was 6.2 months (range:
0.5–12.4 months), which is lower as regards to the reported data
(2,3).
In fact, among GC patients with brain metastasis, the mean interval
from gastrectomy to the occurrence of brain metastasis is reported
to be 9 months (range 1–23 months) in the United States study
(3), and 9.6 months (range 0.1–43.7
months) in the Japanese study (2).
Response to treatment is poor: The prognosis is often dismal, as
the median survival time ranged from 1.3–2.4 months (5,6) and
treatment is palliative. According to these data, the median OS
time from the diagnosis of CNS metastases in the 7 patients was 4.1
months (range 2.1–6.5 months).
Cinar et al (7)
reported 3 patients with HER-2-positive GE junction cancer
presenting with widespread metastatic disease prior to development
of symptoms from the primary tumours; 2 of these 3 patients
presented with brain metastases. These two patients died
approximately 10 and 24 months after diagnosis, a very long time
when compared with our patients. Kim et al (22) reported a case with internal auditory
canal metastasis due to leptomeningeal carcinomatosis from HER-2
positive GC. The interval from the date of diagnosis of GC and
leptomeningeal carcinomatosis was seven months, and the patient
survival time following the CNS involvement was only two months.
Yang et al (23) described a
case of a HER-2-positive GC patient who 8 months after surgery for
the primary tumour developed a solitary brain metastasis treated
with stereotactic radiotherapy. This patient is alive and healthy 8
months after radiotherapy. These Authors (7,22,23) raise the hypothesis that
HER-2-positivity may be associated with a possible propensity for
CNS metastases. In conclusion, we have reviewed retrospectively the
records of 300 patients with gastric or GE junction cancer. Seven
of these patients showed CNS metastases (2.33%) and six of the
seven patients with CNS metastases showed HER-2-over-expression of
their cancer. While acknowledging the limitations of a
retrospective study, our 6 cases, as with the five patients
previously described (7,21–23), raise
the hypothesis that HER-2-over-expressed GC may have similar
behaviour of HER-2-positive breast cancer showing a predilection
for brain metastases, which are rare in GE junction cancer.
While accepting the limitations of the small number
of patients with brain metastasis from gastric and GE junction
cancer analyzed in this report, our data suggest the possibility of
a CNS recurrence susceptibility in patients with HER-2-positive GC.
To the best of our knowledge, this is the first report that
correlates CNS metastases and HER-2 status in gastric or GE
junction cancer.
Acknowledgements
A part of this study was presented at the American
Society of Clinical Oncology Annual Meeting 2015 (Chicago, IL,
USA).
References
|
1
|
Townsend CM Jr, Beauchamp DR and Evers MB:
Sabiston textbook of surgery. 18th. Saunders/Elsevier;
Philadelphia, PA: 2007
|
|
2
|
Kasakura Y, Fujii M, Mochizuki F, Suzuki T
and Takahashi T: Clinicopathological study of brain metastasis in
gastric cancer patients. Surg Today. 30:485–490. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
York JE, Stringer J, Ajani JA, Wildrick DM
and Gokaslan ZL: Gastric cancer and metastasis to the brain. Ann
Surg Oncol. 6:771–776. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lee JL, Kang YK, Kim TW, Chang HM, Lee GW,
Ryu MH, Kim E, Oh SJ, Lee JH, Kim SB, et al: Leptomeningeal
carcinomatosis in gastric cancer. J Neurooncol. 66:167–174. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Go PH, Klaassen Z, Meadows MC and
Chamberlain RS: Gastrointestinal cancer and brain metastasis. A
rare and ominous sign. Cancer. 117:3630–3640. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Esmaeilzadeh M, Majlesara A, Faridar A,
Hafezi M, Hing B, Esmaeilnia-Shirvani H, Nayazi B, Mehrabi A and
Makamura M: Brain metastasis from gastrointestinal cancers: A
systematic review. Int J Clin Pract. 68:890–899. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cinar P, Calkins SM, Venook AP and Kelley
RK: Case series of patients with HER-2-overexpressed primary
metastatic gastro-esophageal adenocarcinoma. Anticancer Res.
34:7357–7360. 2014.PubMed/NCBI
|
|
8
|
Heitz F, Harter P, Lueck HJ,
Fissler-Eckhoff A, Lorenz-Salehi F, Scheil-Bertram S, Traut A and
du Bois A: Triple negative and HER-2-overexpressing breasts cancers
exhibit an elevated risk and an earlier occurrence of cerebral
metastases. Eur J Cancer. 45:2792–2798. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lin NU, Bellon JR and Winer EP: CNS
metastases in breast cancer. J Clin Oncol. 22:3608–3617. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lin NU, Carey LA, Liu MC, Younger J, Come
SE, Ewend M, Harris GJ, Bullitt E, Van den Abbeele AD, Henson JW,
et al: Phase II trial of lapatinib for brain metastases in patients
with human epidermal growth factor receptor 2-positive breast
cancer. J Clin Oncol. 26:1993–1999. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lin NU, Diéras V, Paul D, Lossignol D,
Christodoulou C, Stemmler HJ, Roché H, Liu MC, Greil R, Ciruelos E,
et al: Multicenter phase II study of lapatinib in patients with
brain metastases from HER-2-positive breast cancer. Clin Cancer
Res. 15:1452–1459. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lin NU and Winer EP: Brain metastases: The
HER-2 paradigm. Clin Cancer Res. 13:1648–1655. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Preusser M, Capper D, Mutlu IA, Berghoff
AS, Birner P, Bartsch R, Marosi C, Zielinski C, Mehta MP, Winkler
F, et al: Brain metastases: Pathobiology and emerging targeted
therapies. Acta Neuropathol. 123:205–222. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Musolino A, Ciccolallo L, Panebianco M,
Fontana E, Zanoni D, Bozzetti C, Michiara M, Silini EM and
Ardizzoni A: Multifactorial central nervous system recurrence
susceptibility in patients with HER-2-positive breast cancer.
Cancer May. 1:1837–1846. 2011. View Article : Google Scholar
|
|
15
|
Ross JS, Slodkowska EA, Symmans WF,
Pusztai L, Ravdin PM and Hortobagyi GN: The HER-2 receptor and
breast cancer: Ten years of targeted anti-HER-2 therapy and
personalized medicine. Oncologist. 14:320–368. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bang YJ, Van Cutsem E, Feyereislova A,
Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T,
et al: Trastuzumab in combination with chemotherapy versus
chemotherapy alone for treatment of HER-2-positive advanced gastric
or gastro-oesophageal junction cancer (ToGA): A phase 3,
open-label, randomised controlled trial. Lancet. 376:687–697. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lei YY, Huang JY, Zhao QR, Jiang N, Xu HM,
Wang ZN, Li HQ, Zhang SB and Sun Z: The clinicopathological
parameters and prognostic significance of HER2 expression in
gastric cancer patients: A meta-analysis of literature. World J
Surg Oncol. 15:682017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kyung WS, Jeon T, Kim S, Kim SS, Kim K,
Suh BJ, Hwang S, Choi S, Ryu S, Min JS, et al: Epidemiologic study
of human epidermal growth factor receptor 2 expression in
advanced/metastatic gastric cancer: An assessment of human
epidermal growth factor receptor 2 status in tumor tissue samples
of gastric and gastro-esophageal junction cancer. J Gastric Cancer.
17:52–62. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pestalozzi BC, Zahrieh D, Price KN,
Holmberg SB, Lindtner J, Collins J, Crivellari D, Fey MF, Murray E,
Pagani O, et al: Identifying breast cancer patients at risk for
central nervous system (CNS) metastases in trials of the
international breast cancer study group (IBCSG). Ann Oncol.
17:935–944. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Choy C, Ansari KI, Neman J, Hsu S, Duenas
MJ, Li H, Vaidehi N and Jandial R: Cooperation of neurotrophin
receptor TrkB and HER-2 in breast cancer cells facilitates brain
metastases. Breast Cancer Res. 19:512017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cavanna L, Rocchi A, Gorgni S, Ambroggi M,
Foroni RP, Ubiali A and Civardi G: Cerebrospinal fluid cytology
diagnosis of HER-2-positive leptomeningeal carcinomatosis from
HER-2-positive metastatic gastric cancer: Case report. J Clin
Oncol. 29:e367–e368. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim CH, Shin JE, Roh HG, Lee JS and Yoon
SY: Sudden hearing loss due to internal auditory canal metastasis
of HER-2-positive gastric cancer: A case report. Oncol Lett.
8:394–396. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yang GL, Luo TH, Zhang HQ, Ling CQ and LI
B: A case report of gastric cancer with brain metastasis: Rare
peripheral nervous system symptoms. Oncol Lett. 11:2893–2895. 2016.
View Article : Google Scholar : PubMed/NCBI
|