Introduction
Gastric cancer is one of most common carcinomas and
the second leading cause of cancer-associated mortality globally
(1). Furthermore, gastric cancer has
a poor prognosis and the five-year survival rate is <20%
(2). The annual incidence of gastric
cancer in China accounts for >40% of the incidence worldwide
(3). As the majority of patients are
diagnosed at an advanced stage, numerous patients lose the
opportunity for surgery. Previously, the majority of patients
received systemic chemotherapy, which was characterized by a low
concentration of the drug in the local lesion, little benefit, and
numerous side effects. With the development of interventional
technology, multiple national and international researchers
(4–6)
have demonstrated that intra-arterial chemoembolization through the
tumor feeding arteries increases the drug concentration, improves
the curative effect and reduces the number of adverse reactions.
However, intra-arterial chemotherapy has little effect against
circulating tumor cells, which are distributed throughout the
body.
In order to solve the problems above, the present
study investigated a novel therapeutic concept: A combination of
intra-arterial and intravenous chemotherapy for unresectable,
advanced gastric cancer, which considers local and systemic aspects
to achieve a complementary effect. In the present study, our group
retrospectively analyzed the clinical data of 128 patients with
unresectable, advanced gastric cancer, in order to compare the
short-term effects, long-term effects and adverse reactions in
patients who received regional intra-arterial chemoembolization
plus systemic chemotherapy (combination group) with those who
received systemic chemotherapy only (venous group), and assessed
which patients were suitable for combined treatment.
Patients and methods
Patients
A total of 128 patients who were diagnosed with
unresectable, advanced gastric cancer at The Fourth Hospital of
Hebei Medical University (Shijiazhuang, China) between January 2009
and September 2012 were enrolled in the present study. The present
study was reviewed and approved by the Institutional Review Board
of The Fourth Hospital of Hebei Medical University, and written
informed consent was obtained from patients prior to treatment. The
patients were divided into two groups: Those who received regional
intra-arterial chemoembolization plus systemic chemotherapy
(combined group; n=62) and those who received systemic chemotherapy
only (venous group; n=66). There were 50 males and 12 females in
the combined group and the average age was 63.0±11.2 years (range,
30–88 years). There were 44 cases of cardiac cancer, 9 cases of
gastric fundus carcinoma and 9 cases of gastric antrum carcinoma in
the combined group. Twenty-two patients had poorly differentiated
carcinoma and 40 patients had moderately well-differentiated
carcinoma. The tumor-node-metastasis (TNM) stage distribution
(7) was as follows: 26 IIIC-stage
cases and 36 IV-stage cases. There were 7 patients without lymph
node metastasis, 32 patients with local lymph node metastasis and
23 patients with distant lymph node metastasis. A total of 19
patients had hepatic metastasis and 21 patients had organ
metastases. There were 49 males and 17 females in the venous group
and the average age was 60.4±12.5 years (range, 31–90 years). There
were 38 cases of cardiac cancer, 14 cases of gastric fundus
carcinoma and 14 cases of gastric antrum carcinoma. A total of 20
patients had poorly differentiated carcinoma, and 46 patients had
moderately well-differentiated carcinoma. The TNM stage
distribution was as follows: 20 IIIC-stage cases and 46 IV-stage
cases. There were 4 patients without lymph node metastasis, 41
patients with local lymph node metastasis and 21 patients with
distant lymph node metastasis. A total of 21 patients had hepatic
metastasis and 31 patients had organ metastases.
Equipment and materials
Digital subtraction angiography was performed with a
GE4100 Innova machine (GE Healthcare, Chicago, IL, USA). RH,
5F-Yashiro and Corba catheters, Progreat and Stride microcatheters,
and the micro godet system were from Terumo Corporation (Tokyo,
Japan). Gelatin sponge particles (150–350, 560–710 and 710–1,000
µm) were from Hangzhou Alicon Pharm Sci & Tec Co., Ltd.
(Hangzhou, China).
Inclusion criteria
All the patients in the present study had a
histologically confirmed gastric carcinoma. Surgery is the first
choice of treatment for patients with operable gastric cancer, and
it has a substantial influence on prognosis. Considering this,
operable patients with II–IIIB stage tumors and the patients who
underwent surgical treatment were removed from the research, and
the included patients had unresectable, IIIC-IV advanced stage
gastric cancer. Patients diagnosed with unresectable, advanced
gastric cancer should meet the following criteria: i) Diagnosis of
stage IIIC or IV metastasis of lymph nodes by enhanced computed
tomography (CT) or magnetic resonance imaging (MRI); ii) tumor
infiltration and encompassment of major blood vessels, including
the hepatic artery, celiac artery and portal vein; iii) distant
metastasis (for example, liver metastasis). To be included,
patients needed an Eastern Cooperative Oncology Group performance
status (8) of ≤2. The patients also
needed to have adequate bone marrow function (neutrophilic
granulocyte count ≥1.5×109/l and platelet count
≥100×109/l), and adequate blood coagulation, renal and
hepatic function to be included.
Exclusion criteria
Patients who had completed previous anti-cancer
therapies prior to inclusion, including adjuvant chemotherapy,
radiation therapy, surgery or biotherapy were excluded, as were
patients with resectable II–IIIB TNM stage gastric cancer. Other
exclusion criteria were as follows: Being pregnant or currently
breast-feeding, the presence of other malignant tumors, massive
ascites, poor blood coagulation, or the disease that may interfere
with chemotherapy evaluation.
Chemotherapy regimens
The combined group and venous group were given
paclitaxel, cisplatin and 5-fluorouracil (TCF), modified TCF
(paclitaxel, oxaliplatin and 5-fluorouracil/tegafur), folinic acid,
5-fluorouracil and oxaliplatin (FOLFOX) or modified FOLFOX (folinic
acid, tegafur and oxaliplatin). A total of 30 patients in the
combined group received TCF or modified TCF regimens, and 32
patients received FOLFOX or modified FOLFOX regimens. In total, 32
and 34 patients, respectively, received these treatments in the
venous group. Drug dosages were increased or decreased
appropriately according to age, physical status and side effects.
Chemotherapy was given every 28 days, and all patients received at
least 2–3 cycles of chemotherapy.
Interventional approaches
The 5F-Yashiro vascular sheath was inserted
following percutaneous femoral artery puncture using the Seldinger
technique (9), then hooked onto the
celiac axis and linked to an external high-pressure injector to
perform high-pressure angiography. If the target vessel diameter
was smaller than the 5F-Yashiro catheter or was too difficult to
super-select for the 5F-Yashiro catheter, a micro godet was used to
achieve intubation. The catheter was inserted into the left gastric
artery, left under the phrenic artery and splenic artery for cancer
of the cardiac and fundus, and through the left and right gastric
artery for cancer of the gastric fundus and lesser curvature. For
tumors located in the greater curvature, angiography of the
gastroduodenal artery, right gastroepiploic artery and splenic
artery was performed. Angiography of the gastroduodenal artery and
right gastric artery was performed for gastric antrum cancer.
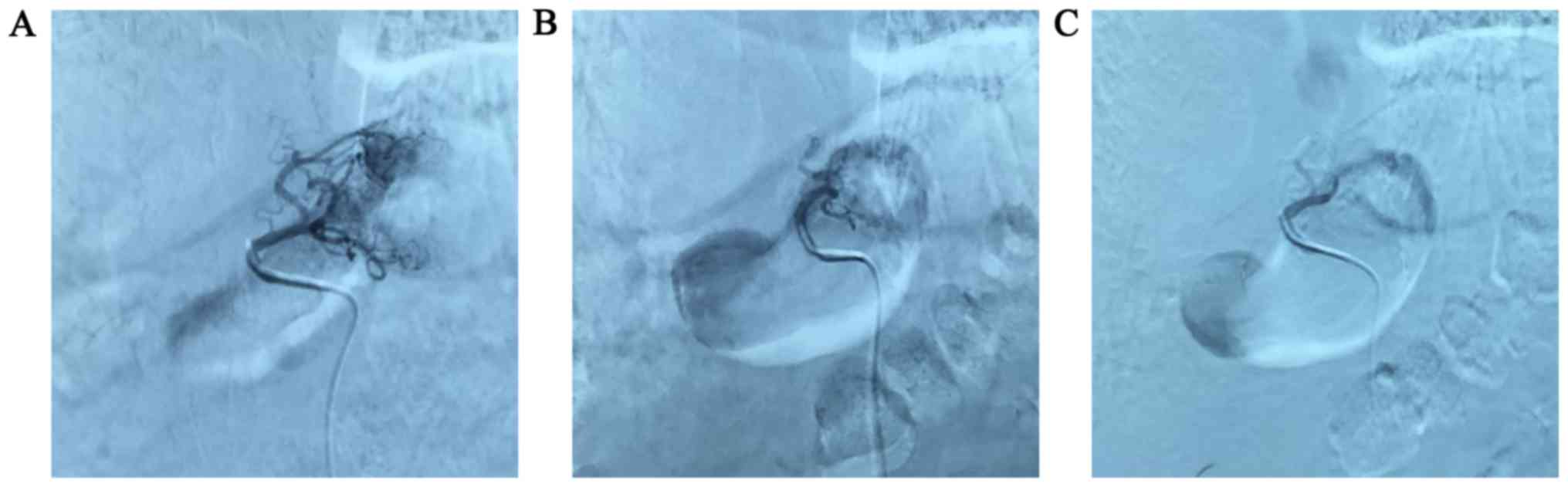
Arteries which supplied blood to the tumor were selected, and the
target artery was identified for chemotherapy and embolism
according to the results of angiography. When liver metastases were
present, chemoembolization of the hepatic arteries was performed.
Following embolization, angiography was performed to ensure there
were no feeding arteries (Fig. 1). In
the present study, each patient underwent at least 1 interventional
treatment and the average number of treatments was 2.7. The
short-term effects of chemotherapy were evaluated in all
patients.
Prognostic indicator
Objective response rate (ORR), overall survival (OS)
and time to symptomatic progression (TTP) were used as prognostic
indicators.
Imaging indicators
Examination consisted of chest and abdominal
enhanced CT or enhanced MRI and, if necessary, positron emission
tomography (PET)-CT or emission (E)CT were performed. Prior to
treatment, tumor size, tumor number and maximum tumor diameter were
recorded. Patients underwent these examinations every 2–3 cycles of
chemotherapy until either mortality or termination of the present
study (December 10th, 2015).
Laboratory indicators
Multiple laboratory indices were analyzed in the
patient groups, including routine blood samples, liver and kidney
function, serum creatinine, blood urea nitrogen, and expression of
carcino-embryonic antigen and carbohydrate antigen 19-9 (CA19-9).
The neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte
ratio (PLR), changes in the NLR following 1 cycle of chemotherapy
(cNLR) and changes in the PLR following 1 cycle of chemotherapy
(cPLR) were also calculated.
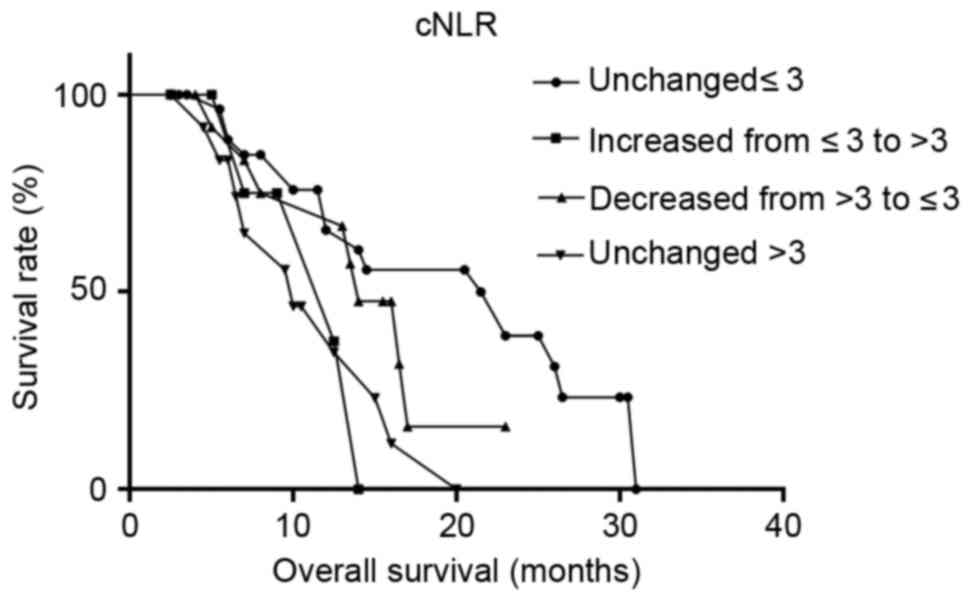
The median NLR was 3.43 and the median PLR was
158.53 in the present study. The NLR and PLR were then divided into
two groups, and the cNLR and cPLR into four groups, to investigate
any influences on the OS of patients in the combined group. NLR was
divided using a cutoff value of 3 into two groups (>3 and ≤3),
and the PLR was divided using a cutoff value of 160 into two groups
(>160 and ≤160). The change in the cNLR was divided into four
groups: Unchanged ≤3; increased from ≤3 to >3, decreased from
>3 to ≤3; and unchanged >3. Similarly, the change in the cPLR
was divided into four groups: Unchanged ≤160, increased from ≤160
to >160, decreased from >160 to ≤160, and unchanged
>160.
Adverse reactions
According to the World Health Organization standard
for side effects of a couplet anti-tumor treatment (10), the adverse side effects experienced by
patients in the combined and venous groups were recorded and
evaluated.
Treatment efficacy
In the present study, the curative effect was judged
by the New Response Evaluation Criteria In Solid Tumors criteria
(11), and consisted of a complete
response (CR), partial remission (PR), stable disease (SD) and
progressive disease (PD). Objective response rate (ORR) was
calculated as: (CR+PR)/measurable number of cases) ×100%.
Statistical analysis
Data were analyzed using SPSS version 21.0 (IBM
Corp., Armonk, NY, USA). χ2 and Fisher's exact tests
were used to assess qualitative data, and the unpaired Student's
t-test was used to assess normally distributed quantitative data.
The Kaplan-Meier method was used to calculate the survival time and
the log-rank test was used to compare the different groups. The
Kaplan-Meier method was also used for univariate analysis, and Cox
regression analysis was employed for multivariate analysis.
GraphPad Prism version 7 (GraphPad Software, Inc., La Jolla, CA,
USA) was used to plot the survival curves. P<0.05 was considered
to indicate a statistically significant difference.
Results
Comparison of general clinical
data
Age, sex, tumor site, pathological type, TNM stage,
lymph node metastasis and organ metastasis status were not
significantly different between patients in the two groups
(P>0.05; Table I).
 | Table I.Clinicopathological characteristics of
the two groups. |
Table I.
Clinicopathological characteristics of
the two groups.
| Variable | Combined group
(n=62) | Venous group
(n=66) | P-value |
|---|
| Age, years | 63.0±11.2 | 60.4±12.5 | 0.220a |
| Sex, n (%) |
|
| 0.387b |
| Male | 50 (80.6) | 49 (74.2) |
|
|
Female | 12 (19.4) | 17 (25.8) |
|
| Site of lesion, n
(%) |
|
| 0.288b |
|
Cardia | 44 (71.0) | 38 (57.6) |
|
| Gastric
fundus | 9 (14.5) | 14 (21.2) |
|
| Gastric
antrum | 9 (14.5) | 14 (21.2) |
|
| Degree of
differentiation, n (%) |
|
| 0.533b |
| Poor | 22 (35.5) | 20 (30.3) |
|
|
Moderate-well | 40 (64.5) | 46 (69.7) |
|
| Stage, n (%) |
|
| 0.170b |
|
IIIC-stage | 26 (41.9) | 20 (30.3) |
|
|
IV-stage | 36 (58.1) | 46 (69.7) |
|
| Lymph node
metastasis, n (%) |
|
| 0.388b |
|
None | 7 (11.3) | 4 (6.1) |
|
| Local
lymph node metastasis | 32 (51.6) | 41 (62.1) |
|
| Distant
lymph node metastasis | 23 (37.1) | 21 (31.8) |
|
| Organ metastasis, n
(%) |
|
| 0.132b |
|
None | 41 (66.1) | 35 (53.0) |
|
|
Yes | 21 (33.9) | 31 (47.0) |
|
| Chemotherapy
regimen |
|
| 0.991b |
|
TCFc | 30 (48.4) | 32 (48.5) |
|
|
FOLFOXd | 32 (51.6) | 34 (51.5) |
|
Comparison of short-term curative
effects
Of the 62 patients in the combined group, no
patients were rated as having a CR, 22 as having a PR, 30 as SD and
10 as PD. The ORR was 35.5% (22/62). For the 66 patients in the
venous group, these figures were 0, 13, 35 and 18, respectively.
The ORR was 19.7% (13/66), which was significantly different
compared with the combined group (P=0.045; Table II).
| Table II.Short-term curative effect of the two
groups. |
Table II.
Short-term curative effect of the two
groups.
| Response rate
(%) | Combined group
(n=62) | Venous group
(n=66) | χ2 | P-value |
|---|
| CR, n | 0 (0) | 0 (0) |
|
|
| PR, n | 22 (35.5) | 13 (19.7) |
|
|
| SD, n | 30 (48.4) | 35 (53.0) |
|
|
| PD, n | 10 (16.1) | 18 (27.3) |
|
|
| ORR, n | 22 (35.5) | 13 (19.7) | 4.010 | 0.045 |
Comparison of long-term curative
effects
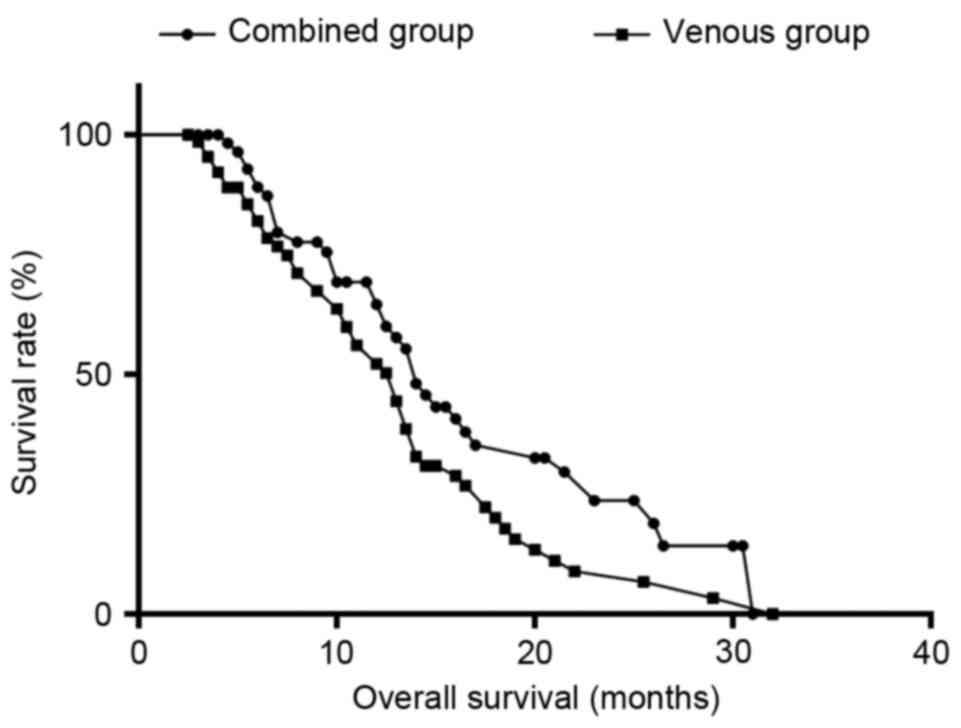
The survival time of the 128 patients was calculated
and the total median (m)OS was 13.5 months [95% confidence
intervals (CI)=12.42–14.58]. The mOS was 14 (95% CI=12.19–15.81)
and 13 months (95% CI=10.71–15.29) in the combined group and the
venous group, and the 1-year and 2-year survival rates in the two
groups were 45.2 and 9.7%, and 40.9 and 6.1%, respectively. There
were significant differences between the survival curves of the
combined group and the venous group (P=0.044; Fig. 2).
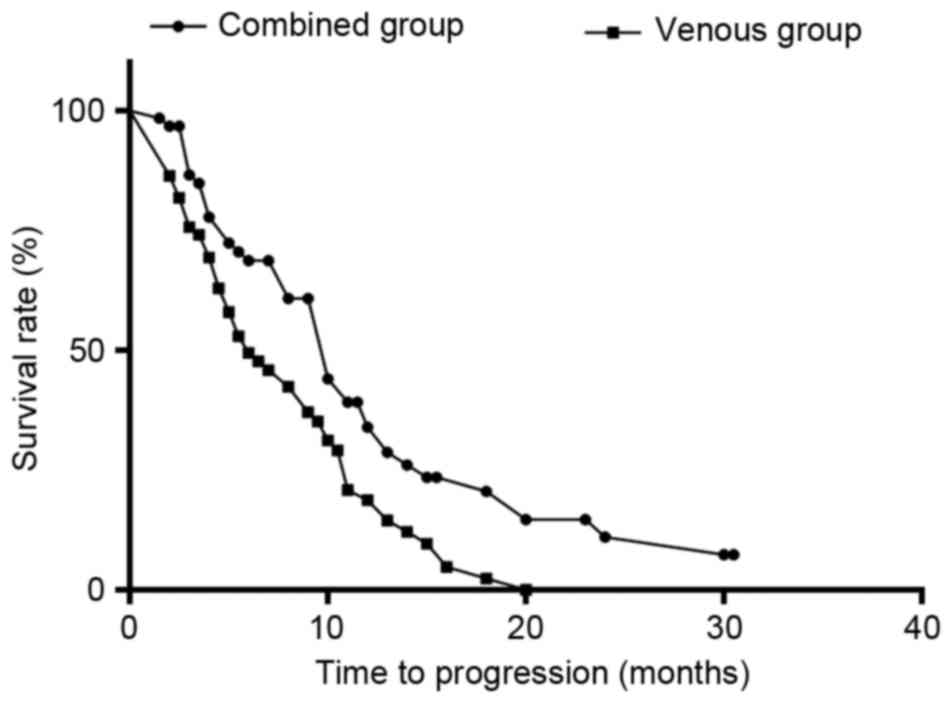
The total median (m)TTP was 9 months (95%
CI=7.60–10.40), and the mTTP was 10 months (95% CI=8.38–11.62) and
6 months (95% CI=3.60–8.40) in the combined group and venous group,
respectively. TTP was significantly different between the two
groups (P=0.003; Fig. 3).
Univariate analysis of OS in the
combined group
The purpose of the present study was to evaluate the
efficacy and safety of combined intra-arterial and intravenous
chemotherapy in the treatment of unresectable, advanced gastric
cancer, and assess which patients are suitable for the combined
treatment. Therefore, univariate analysis and multivariate analysis
were conducted only for the combined group and only patients from
the combined group were represented in the figures.
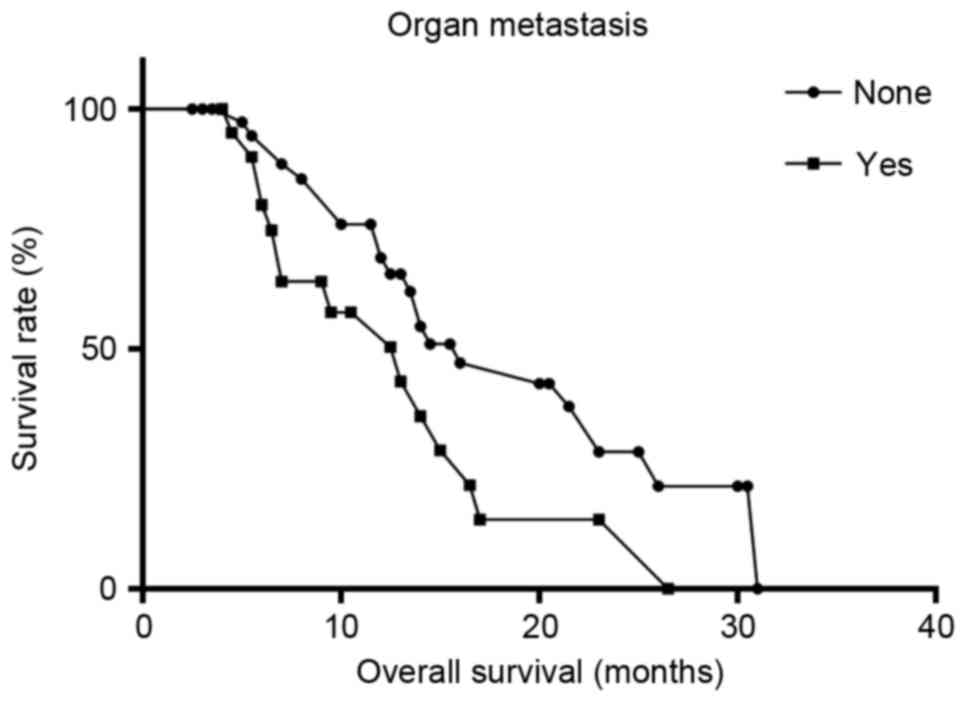
Univariate analysis revealed that organ metastasis
(P=0.046), TNM stage (P=0.017), CA19-9 levels (P=0.036), NLR
(P=0.048), cNLR (P=0.021) and degree of tumor staining (P=0.010)
were associated with patient OS in the combined group (Table III). In patients without organ
metastasis, CA19-9 ≤37 U/ml, TNM-IIIC stage, NLR ≤3, cNLR unchanged
≤3 and distinct tumor staining, mOS was significantly increased
(Figs. 4–9).
| Table III.Univariate analysis of prognostic
factors in the combined group. |
Table III.
Univariate analysis of prognostic
factors in the combined group.
| Variable | mOS (months) | P-value |
|---|
| Sex |
| 0.794 |
|
Male | 14.5 |
|
|
Female | 13.0 |
|
| Age, years |
| 0.840 |
|
>60 | 14.0 |
|
|
≤60 | 13.5 |
|
| Organ
metastasis |
| 0.046 |
|
Yes | 13.0 |
|
| No | 16.0 |
|
| Lymph node
metastasis |
| 0.651 |
|
None | 16.5 |
|
| Local
lymph node metastasis | 13.5 |
|
| Distant
lymph node metastasis | 14.0 |
|
| TNM stage |
| 0.017 |
|
IIIC | 21.5 |
|
| IV | 13.0 |
|
|
Differentiation |
| 0.981 |
|
Poor | 14.5 |
|
|
Moderate-well | 14.0 |
|
| Interventions |
| 0.186 |
|
1–2 | 12.0 |
|
| ≥3 | 15.0 |
|
| Chemotherapy
regimen |
| 0.221 |
|
TCF | 23.0 |
|
|
FOLFOX | 14.0 |
|
| Site of lesion |
| 0.614 |
|
Cardia | 14.0 |
|
| Gastric
fundus | 21.5 |
|
| Gastric
antrum | 15.0 |
|
| Tumor staining |
| 0.010 |
|
Distinct | 21.5 |
|
| Not
distinct | 12.0 |
|
| CEA, ng/ml |
| 0.706 |
|
>5 | 13.5 |
|
| ≤5 | 16.0 |
|
| CA19-9, U/ml |
| 0.036 |
|
>37 | 12.5 |
|
|
≤37 | 15.0 |
|
| NLR |
| 0.048 |
|
>3 | 13.5 |
|
| ≤3 | 14.5 |
|
| cNLR |
| 0.021 |
|
Unchanged >3 | 10.0 |
|
|
Decreased from >3 to
≤3 | 14.0 |
|
|
Unchanged ≤3 | 23.0 |
|
|
Increased from ≤3 to
>3 | 12.5 |
|
| PLR |
| 0.428 |
|
>160 | 13.0 |
|
|
≤160 | 14.5 |
|
| cPLR |
| 0.092 |
|
Unchanged >160 | 12.5 |
|
|
Decreased from >160 to
≤160 | 26.0 |
|
|
Unchanged ≤160 | 14.5 |
|
|
Increased from ≤160 to
>160 | 14.0 |
|
Multivariate analysis of OS in the
combined group
Multivariate analysis revealed that TNM-stage
(P=0.025) and the degree of tumor staining (P=0.015) were
independent factors affecting patient OS in the combined group
(Table IV).
| Table IV.Multivariate analysis of prognostic
factors in the combined group. |
Table IV.
Multivariate analysis of prognostic
factors in the combined group.
|
|
|
|
|
| 95% CI for
Exp(β) |
|---|
|
|
|
|
|
|
|
|---|
| Variables | β | df |
P-valuea | Exp(β) | Lower | Upper |
|---|
| TNM stage | −0.882 | 1 | 0.025 | 0.414 | 0.191 | 0.896 |
| Tumor staining | 0.869 | 1 | 0.015 | 2.383 | 1.184 | 4.798 |
Comparison of adverse reactions
A statistical analysis of adverse reactions
including myelosuppression, liver dysfunction, gastrointestinal
reactions and neurotoxicity was performed. Of these, bone-marrow
suppression and digestive-tract reactions were the most frequent
toxic reactions. No treatment termination or mortality occurred as
a result of toxic reactions in either group. There was no
significant difference in the number of toxic reactions between the
two groups (P>0.05; Table V).
| Table V.Toxicity assessment for the two
groups. |
Table V.
Toxicity assessment for the two
groups.
|
| Combined group
(n=62) | Venous group
(n=66) |
|
|---|
|
|
|
|
|
|---|
| Adverse side
effect | 0 | I | II | III | IV | 0 | I | II | III | IV | P-value |
|---|
| Leukopenia | 50 | 7 | 2 | 2 | 1 | 51 | 9 | 3 | 0 | 3 | 0.602 |
|
Thrombocytopenia | 58 | 2 | 2 | 0 | 0 | 64 | 0 | 1 | 0 | 1 | 0.372 |
| Anemia | 55 | 2 | 5 | 0 | 0 | 55 | 6 | 4 | 1 | 0 | 0.424 |
| Nausea and
vomiting | 5 | 45 | 10 | 2 | 0 | 3 | 46 | 15 | 1 | 1 | 0.647 |
| Hepatic
inadequacy | 59 | 2 | 1 | 0 | 0 | 63 | 1 | 2 | 0 | 0 | 0.849 |
| Neurological
toxicity | 61 | 1 | 0 | 0 | 0 | 63 | 3 | 0 | 0 | 0 | 0.620 |
Discussion
The concept of interventional treatment for gastric
cancer was introduced in the 1980s, and has achieved a positive
clinical effect. Interventional methods have developed from single
perfusion chemotherapy to chemoembolization, and in order to
further improve the curative effect, researchers have attempted to
combine intravenous and intra-arterial administration. Zhang et
al (12) used an arteriovenous
combination of 5-fluorouracil, leucovorin, etoposide, oxaliplatin
and epirubicin in patients with unresectable advanced gastric
cancer, and Nakajima et al (13) used neo-adjuvant chemotherapy for
inoperable gastric cancer via local and general delivery routes.
These studies demonstrated that combined treatment significantly
improves the local and systemic effects of treatment in patients
with advanced gastric cancer.
In the present study, the mOS in the combined group
was 14 months, and the 1-year and 2-year survival rates were 45.2
and 9.7%, respectively; shorter than those reported by Shi et
al (14), where the median
survival time was 18 months and the 1-year and 2-year survival
rates were 76.5 and 33.1%, respectively. Potential reasons for this
are as follows: i) The present study is retrospective and the
overall response rates were obtained from medical histories, thus,
there may have been individual subjectivity and diversity; ii) Of
the 62 patients with advanced gastric cancer who underwent regional
arterial infusion chemotherapy combined with intravenous
chemotherapy, ~58.1% of patients were TNM-IV stage, and 33.9% of
patients had organ metastases, thus the overall effect was limited;
iii) Patients in the combined group had an average of 2.7
interventional treatments, which was fewer than that in previous
studies, including the study by Shi et al (14), where the patients underwent 7 cycles
of interventional treatment on average.
In the present study, the combined group had an
advantage in terms of the short-term and long-term effects of
treatment compared with the venous group. The main reasons are as
follows: i) Regional arterial infusion chemotherapy in the combined
group boosted the drug concentration and maximized the effect of
chemotherapy. In a study by Zhu and Pu (15), the concentration of 5-fluorouracil in
portal venous blood following intra-arterial administration was
4–40-fold higher than that following venous administration, and
high concentrations of 5-fluorouracil were maintained for a
significantly longer time period. Therefore, compared with systemic
chemotherapy only, combined venous and arterial chemotherapy
concentrates the drug in question and prolongs the duration of its
effect on tumor cells, resulting in an improved anti-cancer effect.
ii) Embolization therapy in the combined group removed the source
of the blood supply to the tumor, and resulted in tumor cell
ischemia and necrosis. iii) Intra-arterial chemotherapy induces
tumor cell apoptosis; for example, Tao and Zou (16) demonstrated that preoperative regional
artery chemotherapy in patients with gastric cancer results in an
improved curative effect, due to the inhibition of cell
proliferation and induction of apoptosis. iv) For patients with
distant metastases, in particular patients with hepatic metastases,
chemoembolization effectively controls the disease. v) For patients
with gastrointestinal bleeding, embolization effectively controls
and prevents further hemorrhage, and improves quality of life and
survival time.
Multivariate analysis revealed that distinct tumor
staining was an independent factor affecting patient OS in the
combined group, which is in line with the results of Zou and Tao
(17), who revealed that distinct
tumor staining and tumor blood supply consistency were associated
with the effect of interventional treatment.
Cancer-associated inflammatory reactions have gained
increased attention, and NLR and PLR are important in the prognosis
of advanced gastric cancer (18–20). The
present study emphasized the predictive effect of NLR, PLR, cNLR
and cPLR in patients with advanced gastric cancer who received
combined intra-arterial and intravenous chemotherapy; and
univariate analysis revealed that patients with NLR ≤3 and cNLR
unchanged ≤3 had an increased survival time.
NLR comprehensively reflects inflammation and immune
status in patients with cancer, and increased NLR induces the
inflammatory reaction and reduces anti-cancer activity. This
results in the promotion of tumor growth, leading to a poor
prognosis (21). Previous studies
have reported that gastric cancer patients, with an elevated NLR
have a poor prognosis (21,22), which is in accordance with the results
of the present study. The mechanisms underlying the predictive
function of NLR in the prognosis of patients with gastric cancer is
unclear, but may involve the following: i) Increased neutrophil
number and function; with evidence suggesting that neutrophils
contain and secrete cytokines and enzymes which may stimulate
angiogenesis, increase tumor adhesion, inhibit apoptosis and
facilitate distant metastasis (23,24).
Therefore, an elevated neutrophil count may stimulate tumor growth
and progression (25). ii) Decreased
lymphocyte count and function: Lymphocytes serve a crucial function
in the process of cellular adaptive immunity, which plays an
essential role in immunosurveillance, recognition and destruction
of cancer cells (26,27). Lymphopenia may reduce the anticancer
function and lead to a worse outcome for cancer patients (28). Morris et al (29) have reported that a high number of
tumor-infiltrating lymphocytes was strongly associated with
favorable outcomes in patients with colon cancer, effectively
confirming the aforementioned point.
In conclusion, regional intra-arterial
chemoembolization combined with systemic chemotherapy in patients
with unresectable, advanced gastric cancer is safe and effective,
and patients with an earlier TNM stage and distinct tumor staining
may achieve an improved clinical benefit. Compared with intravenous
chemotherapy, combined chemotherapy in patients with unresectable,
advanced gastric cancer has a positive curative effect in the long-
and short-term. NLR and cNLR have a predictive effect on prognosis
and the curative effect of chemotherapy in patients with advanced
gastric cancer, and this inexpensive and convenient means of
forecasting should be confirmed by further research and widespread
use in the clinic.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81072966/H2902).
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hamilton JP and Meltzer SJ: A Review of
the Genomics of Gastric Cancer. Clin Gastroenterol Hepatol.
4:416–425. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Crew KD and Neugut AI: Epidemiology of
gastric cancer. World J Gastroenterol. 12:354–362. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zhu XD and Li J: Gastric carcinoma in
China: Current status and future perspectives (Review). Oncol Lett.
1:407–412. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang CW, Zou SC, Shi D and Zhao DJ:
Clinical significance of preoperative regional intra-arterial
infusion chemotherapy for advanced gastric cancer. World J
Gastroenterol. 10:3070–3072. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li M, Zhang J, Wang D, Zhong B, Tucker S,
Lu S, Cheng J, Cao C, Xu J and Pan H: A phase II study of
intra-arterial chemotherapy of 5-fluorouracil, cisplatin, and
mitomycin C for advanced nonresectable gastric cancer. Anticancer
Drugs. 20:941–945. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shchepotin IB, Cborny V, Hanfelt J and
Evans SR: Palliative superselective intra-arterial chemotherapy for
advanced nonresectable gastric cancer. J Gastrointest Surg.
3:426–431. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: the 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 6:1471–4. 2010.
View Article : Google Scholar
|
|
8
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Seldinger SI: Catheter replacement of the
needle in percutaneous arteriography; a new technique. Acta Radiol.
39:368–376. 1953. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Miller AB, Hoogstraten B, Staguet M and
Winkler A: Reporting results of cancer treatment. Cancer.
47:207–214. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Cancer. 45:228–247.
2009.
|
|
12
|
Zhang C, Li G, Fan C, Xu J, Cao J, Liu S
and Li N: Comparison of efficacy of different route of
administration of chemotherapy on unresectable, advanced gastric
cancer. World J Surg Oncol. 10:1622012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nakajima T, Ishihara S, Motohashi H,
Kitamura Y, Nakajima Y, Fujii M, Tokunaga A, Matai K, Anzai H and
Nishi M: Neo-Adjuvant chemotherapy for inoperable gastric cancer
via local and general delivery routes (FLEP Therapy)Cancer
Treatment An Update. Springer; Paris Germany: pp. 411–413. 1994,
View Article : Google Scholar
|
|
14
|
Shi DH, Cao JM, Gao DZ, Xu J, Kong WD, Li
CL and Wang ZQ: Modified FOLFOX regimen combined with
interventional therapy for the treatment of advanced gastric
cancer: A clinical study. Intervent Radiol. 18:759–762. 2009.
|
|
15
|
Zhu ZD and Pu YD: The study of
pharmacokinetics of 5-Fu after left gastric artery intra-arterial
infusion in treatment of gastric carcinoma. Chin J Bases Clin
General Surg. 8:26–28. 2001.
|
|
16
|
Tao HQ and Zou SC: Effect of preoperative
regional artery chemotherapy on proliferation and apoptosis of
gastric carcinoma cells. World J Gastroenterol. 8:451–454. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zou SC and Tao HQ: Several questions
related on preoperative regional arterial chemotherapy for gastric
and colorectal cancer. World Chin J Digest. 15:477–481. 2007.
|
|
18
|
Gu X, Gao XS, Cui M, Xie M, Peng C, Bai Y,
Guo W, Han L, Gu X and Xiong W: Clinicopathological and prognostic
significance of platelet to lymphocyte ratio in patients with
gastric cancer. Oncotarget. 7:49878–49887. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cho IR, Park JC, Park CH, Jo JH, Lee HJ,
Kim S, Shim CN, Lee H, Shin SK, Lee SK and Lee YC: Pre-treatment
neutrophil to lymphocyte ratio as a prognostic marker to predict
chemotherapeutic response and survival outcomes in metastatic
advanced gastric cancer. Gastric Cancer. 17:703–710. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yamanaka T, Matsumoto S, Teramukai S,
Ishiwata R, Nagai Y and Fukushima M: The baseline ratio of
neutrophils to lymphocytes is associated with patient prognosis in
advanced gastric cancer. Oncology. 73:215–220. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee S, Oh SY, Kim SH, Lee JH, Kim MC, Kim
KH and Kim HJ: Prognostic significance of neutmphil lymphocyte
ratio and platelet lymphocyte ratio in advanced gastric cancer
patients treated with FOLFOX chemotherapy. BMC Cancer. 13:3502013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang SC, Chou JF, Strong VE, Brennan MF,
Capanu M and Coit DG: Pre-treatment neutrophil to lymphocyte ratio
independently predicts disease specific survival in resectable GE
junction and gastric adenocarcinoma. Ann Surg. 263:292–297. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bald T, Quast T, Landsberg J, Rogava M,
Glodde N, Lopez-Ramos D, Kohlmeyer J, Riesenberg S, van den
Boorn-Konijnenberg D, Hömig-Hölzel C, et al:
Ultraviolet-radiation-induced inflammation promotes angiotropism
and metastasis in melanoma. Nature. 507:109–113. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wada Y, Yoshida K, Tsutani Y, Shigematsu
H, Oeda M, Sanada Y, Suzuki T, Mizuiri H, Hamai Y, Tanabe K, et al:
Neutrophil elastase induces cell proliferation and migration by the
release of TGF-α, PDGF and VEGF in esophageal cell lines. Oncol
Rep. 17:161–167. 2007.PubMed/NCBI
|
|
25
|
Tian N and Zhang PT: Relationship between
neutrophilia and cancer progress or metastasis. Chin Canc.
19:470–476. 2010.
|
|
26
|
Schreiber RD, Old LJ and Smyth MJ: Cancer
immunoediting: integrating immunity's roles in cancer suppression
and promotion. Science. 331:1565–1570. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Smyth MJ, Dunn GP and Schreiber RD: Cancer
immunosurveillance and immunoediting: The roles of immunity in
suppressing tumor development and shaping tumor immunogenicity. Adv
Immunol. 90:1–50. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ray-Coquard I, Cropet C, Van Glabbeke M,
Sebban C, Le Cesne A, Judson I, Tredan O, Verweij J, Biron P,
Labidi I, et al: Lymphopenia as a Prognostic Factor for Overall
Survival in Advanced Carcinomas, Sarcomas, and Lymphomas. Cancer
Res. 69:5383–5391. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Morris M, Platell C and Iacopetta B:
Tumor-infiltrating lymphocytes and perforation in colon cancer
predict positive response to 5-fluorouracil chemotherapy. Clin
Cancer Res. 14:1413–1417. 2008. View Article : Google Scholar : PubMed/NCBI
|