Introduction
Hepatocellular carcinoma (HCC) is one of the most
common malignancies leading to death worldwide (1). Although the diagnosis and treatment of
HCC have been improved, prognosis is poor (2). The death rate of patients with HCC was
nearly constant from 2000 to 2011 (3). Moreover, HCC was estimated to represent
the third-leading cause in China of malignancy-related death
subsequent to 2011 (3). Poor
prognosis is partly related to the initial diagnosis of HCC when
the tumor stage is advanced, indicating the likelihood that
curative resection is not possible (4–7). Further,
the high incidence of metastasis and recurrence after curative
resection significantly impairs the efficacy of treatment (8–10).
Therefore, there is an urgent need to develop an accurate tool to
aid early diagnosis as well as to predict prognosis to improve the
outcomes of patients with HCC.
Serum proteins are considered to the most clinically
applicable markers for routine analyses, because they offer the
advantages of noninvasiveness, cost-effectiveness, and high
reproducibility (11). Currently,
α-fetoprotein (AFP) is the most frequently used biomarker for HCC
surveillance (4,5). However, because of its unsatisfactory
performance, even using the optimal cutoff value (10–20 ng/ml)
(12), AFP is not recommended as an
adjunct to abdominal ultrasound (4,13).
Prothrombin induced by vitamin K absence-II (PIVKA-II), also known
as des-γ-carboxy prothrombin, is a useful marker for diagnosing
HCC, and elevated levels of PIVKA-II are associated with poor
prognosis of patients undergoing different treatments (14–18).
Moreover, PIVKA-II performs better compared with AFP for the
diagnosis and prognosis of HCC (18,19) and
therefore is considered a promising biomarker for managing HCC.
However, the clinical significance of PIVKA-II was mainly assessed
by studies of Japanese patients with HCC (20–22), and
the use of PIVKA-II levels to assess Chinese patients is limited.
Moreover, most Chinese HCC patients are infected with hepatitis B
virus (HBV). In contrast, the majority of patients in Japan are
infected with hepatitis C virus (HCV), which may bias the
interpretation of PIVKA-II data acquired by studies of a Japanese
cohort (23). Therefore, it is
essential to conduct a study mainly focusing on Chinese patients
with HBV-related HCC to evaluate the clinical significance of
PIVKA-II levels.
Pathological parameters such as differentiation,
microvascular invasion (MVI), and Ki67 expression level are major
risk factors for tumor recurrence and mortality of patients with
HCC (24–26). However, these parameters are
detectable only through microscopic examination of surgical
specimens, and correct interpretation of the findings requires
experienced pathologists. Moreover, predicting such parameters is a
major issue in assessing the prognosis of patients with HCC.
Therefore, the discovery of a serum biomarker for predicting
prognosis-related pathological parameters will likely enhance
management of HCC. Unfortunately, we are unaware of any relevant
published data for Chinese patients with HBV-associated HCC.
Therefore, to develop an appropriate management
strategy, we conducted a retrospective study of 117 Chinese
patients with HBV-associated HCC to determine the distribution of
serum PIVKA-II concentrations according to Barcelona Clinic Liver
Cancer (BCLC) stages (4),
particularly stage 0-A (defined as early HCC), and assessed the
ability of PIVKA-II levels to predict prognosis-related
pathological parameters.
Patients and methods
Patients
The present retrospective study included 117
patients with HBV-associated HCC who underwent curative resection
at Zhongshan Hospital (Fudan University, Shanghai, China). HCC was
defined according to the results of imaging studies and biochemical
assays, and diagnosis was confirmed using histopathology according
to the criteria of the guidelines of the American Association for
the Study of Liver Diseases (4).
Staging was determined according to the BCLC system (27), and tumor differentiation was
determined using the Edmondson grading system (23). Patients undergoing vitamin K or
warfarin treatment were excluded (19). The Research Ethics Committee of
Zhongshan Hospital granted approval for the use of human subjects,
and informed consent was obtained from each patient.
Sample collection, storage, and
measurements
Peripheral blood samples were collected 3 days
before curative resection. Blood samples were centrifuged
immediately after collection to separate serum, and approximately 3
ml of serum was collected from each patient. After separation,
serum samples were stored at −80°C. PIVKA-II concentrations were
measured using a Lumipulse G1200 automated immunoassay instrument
(Fujirebio, Inc., Tokyo, Japan), and AFP concentrations were
determined using a Cobas e 601 module (Roche Diagnostics, GmbH,
Mannheim, Germany).
Pathological parameters
We collected data for the pathological parameters
MVI (28), Ki67 (29), glypican 3 (GPC3) (30), heat shock protein 70 (HSP70) (31,32), and
cytokeratin 19 (CK19) (10,33,34). MVI
was defined as the presence of a tumor thrombus in a vascular space
lined by endothelial cells in the tumor parenchyma or stroma
(19). Immunohistochemistry was used
to analyze the expression of Ki67, GPC3, HSP70, and CK19, and two
independent pathologists assessed expression levels. KI67
expression was determined according to the median percentage of
positive tumor cells within the stroma, and the cutoff value in the
present study was defined as 20.00%.
Statistical analysis
Statistical analysis was performed using SPSS 20.0
software (IBM Corp., Armonk, NY, USA). Values of continuous
variables are expressed as the mean ± standard error of the mean.
The chi-squared test, Fisher's exact probability tests, and
Student's t-test were used, as appropriate, to evaluate the
significance of differences in data between groups. If the
differences within groups were not normally distributed, the
nonparametric Mann-Whitney test or the Wilcoxon signed-rank test
was used. A receiver operating characteristic (ROC) curve and area
under curve (AUC) were used to evaluate the predictive value of
clinical variables, including PIVKA-II levels. To identify
independent predictors for MVI and high Ki67 expression, variables
with P<0.05 (chi-squared test) were included in the logistic
regression model, using a stepwise selection procedure (19), and P<0.05 was considered
significant.
Results
Patient characteristics
The clinical characteristics of the 117 patients are
summarized in Table I. According to
the BCLC staging system, 83 patients were classified as early-stage
HCC (stage 0, n=17; stage A, n=66), and the other 34 patients were
classified as intermediate-stage HCC (stage B, n=24) or advanced
HCC (stage C, n=10).
 | Table I.Correlation between preoperative
serum PIVKA and clinicopathological characteristics. |
Table I.
Correlation between preoperative
serum PIVKA and clinicopathological characteristics.
| Clinical
characteristics | No. of patients
(n=117) | PIVKA-II≤40
(mAU/ml) | PIVKA-II>40
(mAU/ml) | P-value |
|---|
| Age, years |
|
|
|
|
|
≤50 | 31 | 6 | 25 | 0.350 |
|
>50 | 86 | 24 | 62 |
|
| Sex |
|
|
|
|
|
Female | 14 | 7 | 7 | 0.026 |
|
Male | 103 | 23 | 80 |
|
| ALT, U/l |
|
|
|
|
|
≤40 | 87 | 24 | 63 | 0.412 |
|
>40 | 30 | 6 | 24 |
|
| AST, U/l |
|
|
|
|
|
≤40 | 89 | 25 | 64 | 0.279 |
|
>40 | 28 | 5 | 23 |
|
| AFP, ng/ml |
|
|
|
|
|
≤20 | 48 | 14 | 34 | 0.466 |
|
>20 | 69 | 16 | 53 |
|
| No. of tumors |
|
|
|
|
|
Single | 82 | 22 | 60 | 0.652 |
|
Multiple | 35 | 8 | 27 |
|
| Tumor size, cm |
|
|
|
|
| ≤5 | 70 | 25 | 45 | 0.002 |
|
>5 | 47 | 5 | 42 |
|
| Tumor border |
|
|
|
|
|
Clear | 109 | 29 | 80 | 0.371 |
|
Unclear | 8 | 1 | 7 |
|
| Satellite
lesion |
|
|
|
|
| No | 95 | 27 | 68 | 0.152 |
|
Yes | 22 | 3 | 19 |
|
| Macrovascular
invasion |
|
|
|
|
| No | 107 | 30 | 77 | 0.052 |
| Yes | 10 | 0 | 10 |
|
| Microvascular
invasion |
|
|
|
|
| No | 64 | 24 | 40 | 0.001 |
|
Yes | 53 | 6 | 47 |
|
| Edmondson
stage |
|
|
|
|
|
I–II | 47 | 14 | 33 | 0.400 |
|
III–IV | 70 | 16 | 54 |
|
| BCLC stage |
|
|
|
|
|
0+A | 83 | 26 | 57 | 0.028 |
|
B+C | 34 | 4 | 30 |
|
| CK19 |
|
|
|
|
|
Negative | 72 | 18 | 54 | 0.841 |
|
Positive | 45 | 12 | 33 |
|
| GPC3 |
|
|
|
|
|
Negative | 36 | 11 | 25 | 0.470 |
|
Positive | 81 | 19 | 62 |
|
| HSP70 |
|
|
|
|
|
Negative | 27 | 6 | 21 | 0.643 |
|
Positive | 90 | 24 | 66 |
|
| Ki67 |
|
|
|
|
|
Low | 62 | 21 | 41 | 0.030 |
|
High | 55 | 9 | 46 |
|
Analysis of PIVKA-II and AFP
levels
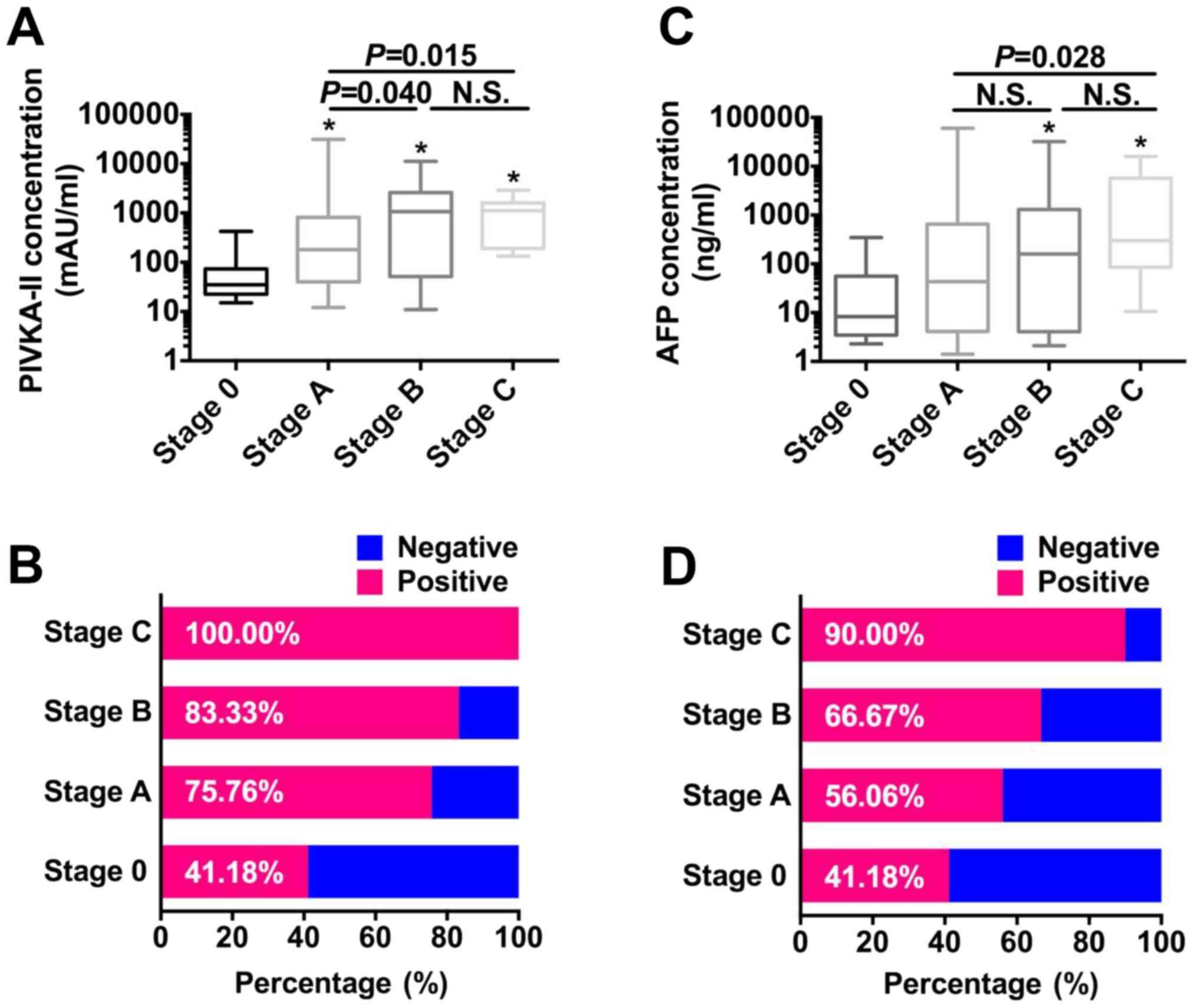
The median PIVKA-II levels increased from very early
(stage 0) to advanced (stage C) (Fig.
1A). PIVKA-II levels of patients with stage 0 were
significantly lower compared with those of patients with stage A,
B, or C HCC (all P<0.050). PIVKA-II levels increased
significantly from BCLC stages A to B (P=0.040). Similar results
were obtained when the levels of PIVKA-II of patients with stage A
HCC were compared with those of patients with stage C HCC (P=0.015)
(Fig. 1A). However, there was no
significant difference between PIVKA-II levels of patients with
stages B or C HCC (P=0.923). When the cutoff was defined as 40
mAU/ml, the optimal value for HCC diagnosis of Chinese patients
(16), the positive rate of detection
of PIVKA-II increased from very-early to advanced HCC
(41.18–100.00%) (Fig. 1B), and all
patients with stage C HCC were positive for PIVKA-II. In contrast,
the median AFP level did not increase, and there were significant
differences only between stages 0 and B or C (both P<0.050) and
between stages A and C (P=0.028) (Fig.
1C). However, similar to the PIVKA-II data, the rates of
AFP-positive samples increased with tumor progression
(41.18–90.00%) when cutoff value for AFP was defined as 20 ng/ml
(23) (Fig.
1D).
Evaluating the potential significance
of combining PIVKA-II with AFP values for patients with early-stage
HCC
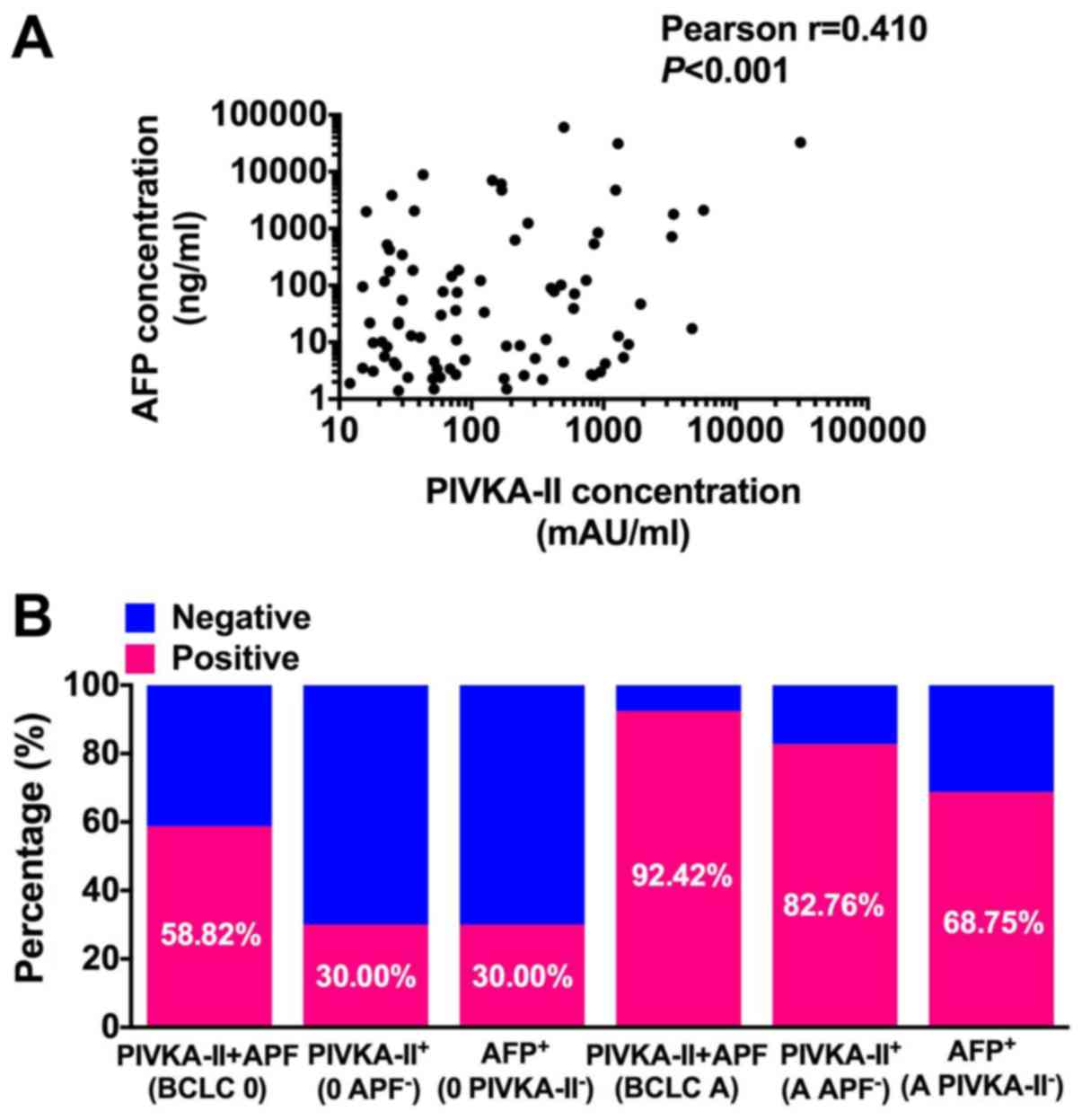
The rate of samples positive for PIVKA-II or AFP was
relatively low, particularly for BCLC stage 0 (<50.00% each)
(Fig. 1B and D). Therefore, we
investigated the potential value of combining the PIVKA-II and AFP
data for patients with early-stage HCC. This analysis revealed a
significant correlation between their levels, although the
Pearson's r value was 0.41 (Fig. 2A),
indicating a weak correlation between these two biomarkers and the
potential value of combining AFP and PIVKA-II values. Therefore, we
further analyzed the significance of combining PIVKA-II and AFP
rates for patients with BCLC stages 0 and A.
The rates of positive detection using the
combination of PIVKA-II and AFP levels were 58.82 and 92.42% for
stages 0 and A, respectively (Fig.
2B). In the stage 0 group, the PIVKA-II-positive rate of
AFP-negative patients was 30.00%, the AFP-positive rate of
PIVKA-II-negative patients was 30.00% (Fig. 2B). For the stage A group, the
PIVKA-II-positive rate of AFP-negative patients was 82.76%, the
AFP-positive rate of PIVKA-II-negative patients was 68.75%.
Together, these results reveal low overlap between PIVKA-II and AFP
levels in patients with early HCC and indicate the promise of
combining PIVKA-II and AFP levels for managing these patients.
Correlation between serum PIVKA-II
levels and patients' clinicopathological characteristics
The correlations between the PIVKA-II serum levels
and patients' clinical characteristics are shown in Table I. Patients with high serum PIVKA-II
levels were more likely to have a larger tumor (>5 cm, P=0.002)
and an advanced tumor stage (P=0.028). Further, we found that male
patients were more likely to have higher serum PIVKA-II levels
(P=0.026), suggesting that sex ratio bias should be considered when
using PIVKA-II as a biomarker for HCC. When we evaluated the
correlation between PIVKA-II levels and pathological parameters
MVI, CK19, GPC3, HSP70, and Ki67, we found that the PIVKA-II level
correlated significantly with MVI (P=0.001) and high Ki67
expression (P=0.030), indicating that patients with high serum
PIVKA-II levels likely have a more aggressive tumor phenotype.
Serum PIVKA-II levels serve as an
independent predictor of MVI and tumor cell proliferation
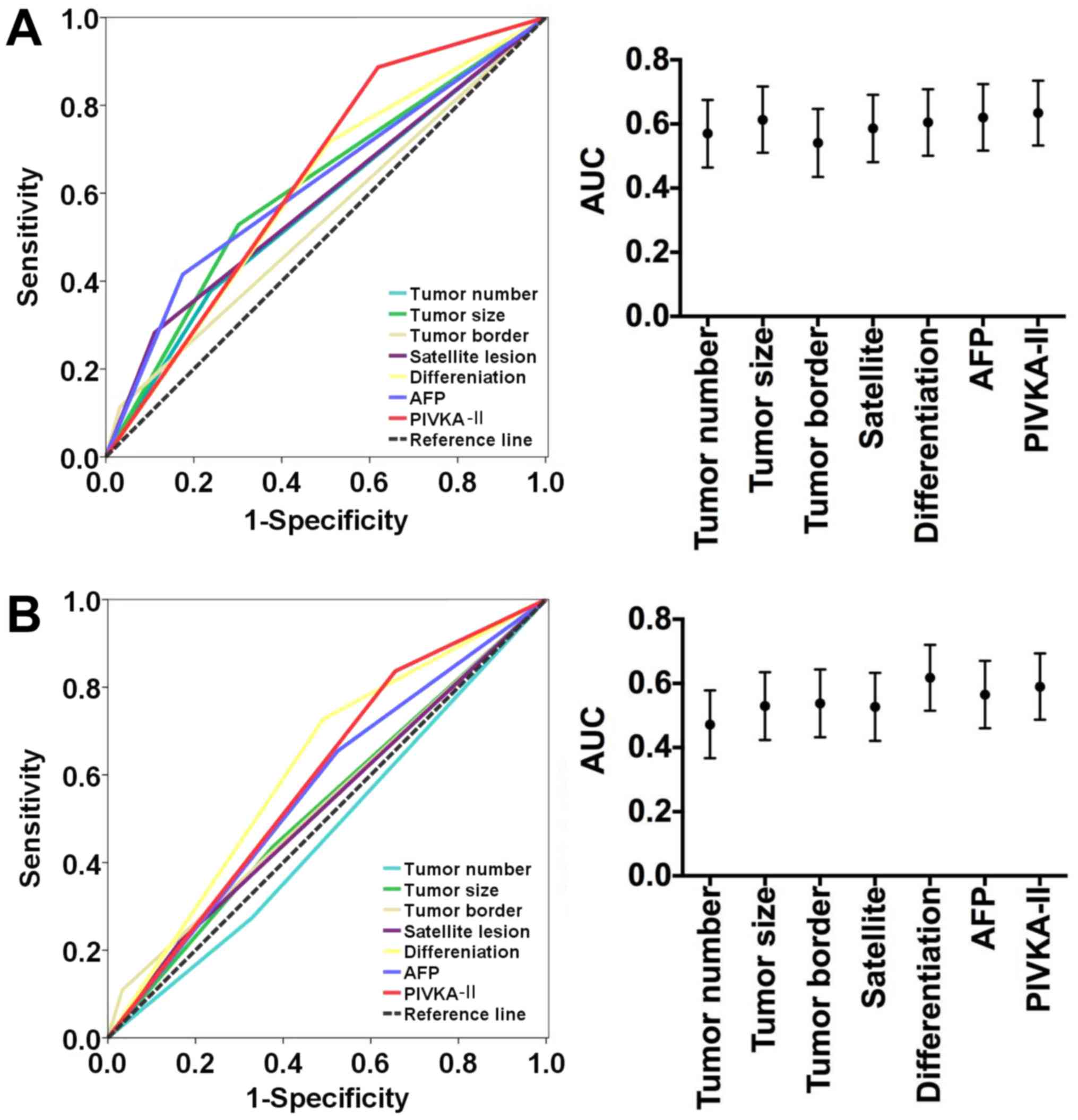
We next investigated whether PIVKA-II served as an
independent predictor for MVI and tumor cell proliferation, which
indicate the potential of HCC to progress. When we first assessed
the correlation between clinicopathological characteristics and
MVI, we found that age, AFP level, tumor size, satellite lesions,
macrovascular invasion, BCLC stage, and PIVKA-II level correlated
significantly with MVI (all P<0.050) (Table II). Multivariate analysis revealed
that PIVKA-II level [hazard ratio (HR), 3.77; 95% confidence
interval (CI), 1.31–10.88; P=0.014], age (HR, 0.36; 95% CI,
0.14–0.92; P=0.034), AFP level (HR, 2.88; 95% CI, 1.14–7.25;
P=0.025), and BCLC stage (HR, 2.91; 95% CI, 1.16–7.26; P=0.022)
were independent predictors for MVI (Table II). The AUC of the PIVKA-II level for
predicting MVI was 0.634 (95% CI, 0.533–0.735) with 88.70%
sensitivity and 38.10% specificity (Fig.
3A).
| Table II.Predictive factors of microvascular
invasion in hepatocellular carcinomas. |
Table II.
Predictive factors of microvascular
invasion in hepatocellular carcinomas.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Clinical
characteristics |
MVI− |
MVI+ | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
≤50 | 11 | 20 | 0.012 | 0.36 | 0.14–0.92 | 0.034 |
|
>50 | 53 | 33 |
|
|
|
|
| Sex |
|
|
|
|
|
|
|
Female | 7 | 7 | 0.706 |
| N.A. |
|
|
Male | 57 | 46 |
|
|
|
|
| ALT, U/l |
|
|
|
|
|
|
|
≤40 | 50 | 37 | 0.305 |
| N.A. |
|
|
>40 | 14 | 16 |
|
|
|
|
| AST, U/l |
|
|
|
|
|
|
|
≤40 | 52 | 37 | 0.149 |
| N.A. |
|
|
>40 | 14 | 16 |
|
|
|
|
| AFP, ng/ml |
|
|
|
|
|
|
|
≤20 | 36 | 12 | 0.001 | 2.88 | 1.14–7.25 | 0.025 |
|
>20 | 28 | 41 |
|
|
|
|
| No. of tumors |
|
|
|
|
|
|
|
Single | 49 | 33 | 0.093 |
| N.A. |
|
|
Multiple | 15 | 20 |
|
|
|
|
| Tumor size, cm |
|
|
|
|
|
|
| ≤5 | 45 | 25 | 0.011 |
| N.S. |
|
|
>5 | 19 | 28 |
|
|
|
|
| Tumor border |
|
|
|
|
|
|
|
Clear | 62 | 47 | 0.085 |
| N.A. |
|
|
Unclear | 2 | 6 |
|
|
|
|
| Satellite
lesion |
|
|
|
|
|
|
| No | 57 | 38 | 0.017 |
| N.S. |
|
|
Yes | 7 | 15 |
|
|
|
|
| Macrovascular
invasion |
|
|
|
|
|
|
| No | 63 | 44 | 0.003 |
| N.S. |
|
|
Yes | 1 | 9 |
|
|
|
|
| Edmondson
stage |
|
|
|
|
|
|
|
I–II | 32 | 15 | 0.017 |
| N.S. |
|
|
III–IV | 32 | 38 |
|
|
|
|
| BCLC stage |
|
|
|
|
|
|
|
0+A | 53 | 30 | 0.002 | 2.91 | 1.16–7.26 | 0.022 |
|
B+C | 11 | 23 |
|
|
|
|
| CK19 |
|
|
|
|
|
|
|
Negative | 42 | 30 | 0.318 |
| N.A. |
|
|
Positive | 22 | 23 |
|
|
|
|
| GPC3 |
|
|
|
|
|
|
|
Negative | 24 | 12 | 0.083 |
| N.A. |
|
|
Positive | 40 | 41 |
|
|
|
|
| HSP70 |
|
|
|
|
|
|
|
Negative | 12 | 15 | 0.222 |
| N.A. |
|
|
Positive | 52 | 38 |
|
|
|
|
| PIVKA-II |
|
|
|
|
|
|
|
≤40 | 24 | 6 | 0.001 | 3.77 | 1.31–10.88 | 0.014 |
|
>40 | 40 | 47 |
|
|
|
|
When we performed this two-step analysis, we found
that macrovascular invasion, Edmondson stage, CK19, GPC3, and
PIVKA-II levels correlated significantly with high Ki67 expression.
Further, multivariate analysis identified PIVKA-II level (HR, 2.99;
95% CI, 1.19–7.52; P=0.020), Edmondson stage (HR, 2.61; 95% CI,
1.16–5.88; P=0.020), and GPC3 (HR, 2.65; 95% CI, 1.10–6.36;
P=0.027) as independent predictors of high Ki67 expression, which
reflect the high proliferative potential of tumor cells (Table III). The AUC of the PIVKA-II level
used to predict Ki67 expression was 0.590 (95% CI, 0.487–0.694)
with 83.60% sensitivity and 34.40% specificity (Fig. 3B). Taken together, these results
showed PIVKA-II could serve as a promising indicator for predicting
progressive HCC.
| Table III.Predictive factors of Ki67 expression
in hepatocellular carcinomas. |
Table III.
Predictive factors of Ki67 expression
in hepatocellular carcinomas.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Clinical
characteristics |
Ki67low |
Ki67high | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
≤50 | 15 | 16 | 0.549 |
| N.A. |
|
|
>50 | 47 | 39 |
|
|
|
|
| Sex |
|
|
|
|
|
|
|
Female | 7 | 7 | 0.811 |
| N.A. |
|
|
Male | 55 | 48 |
|
|
|
|
| ALT, U/l |
|
|
|
|
|
|
|
≤40 | 48 | 39 | 0.421 |
| N.A. |
|
|
>40 | 14 | 16 |
|
|
|
|
| AST, Ul |
|
|
|
|
|
|
|
≤40 | 47 | 42 | 0.944 |
| N.A. |
|
|
>40 | 15 | 13 |
|
|
|
|
| AFP, ng/ml |
|
|
|
|
|
|
|
≤20 | 29 | 19 | 0.180 |
| N.A. |
|
|
>20 | 33 | 36 |
|
|
|
|
| No. of tumors |
|
|
|
|
|
|
|
Single | 42 | 40 | 0.557 |
| N.A. |
|
|
Multiple | 20 | 15 |
|
|
|
|
| Tumor size, cm |
|
|
|
|
|
|
| ≤5 | 39 | 31 | 0.471 |
| N.A. |
|
|
>5 | 23 | 24 |
|
|
|
|
| Tumor border |
|
|
|
|
|
|
|
Clear | 59 | 49 | 0.105 |
| N.A. |
|
|
Unclear | 2 | 6 |
|
|
|
|
| Satellite
lesion |
|
|
|
|
|
|
| No | 52 | 43 | 0.432 |
| N.A. |
|
|
Yes | 10 | 12 |
|
|
|
|
| Macrovascular
invasion |
|
|
|
|
|
|
| No | 60 | 47 | 0.029 |
| N.S. |
|
|
Yes | 2 | 8 |
|
|
|
|
| Microvascular
invasion |
|
|
|
|
|
|
| No | 41 | 23 | 0.008 |
| N.S. |
|
|
Yes | 21 | 32 |
|
|
|
|
| Edmondson
stage |
|
|
|
|
|
|
|
I–II | 32 | 15 | 0.007 | 2.61 | 1.16–5.88 | 0.020 |
|
III–IV | 30 | 40 |
|
|
|
|
| BCLC stage |
|
|
|
|
|
|
|
0+A | 45 | 38 | 0.678 |
| N.A. |
|
|
B+C | 17 | 17 |
|
|
|
|
| CK19 |
|
|
|
|
|
|
|
Negative | 44 | 28 | 0.026 |
| N.S. |
|
|
Positive | 18 | 27 |
|
|
|
|
| GPC3 |
|
|
|
|
|
|
|
Negative | 25 | 11 | 0.017 | 2.65 | 1.10–6.36 | 0.027 |
|
Positive | 37 | 44 |
|
|
|
|
| HSP70 |
|
|
|
|
|
|
|
Negative | 15 | 12 | 0.761 |
| N.A. |
|
|
Positive | 47 | 43 |
|
|
|
|
| PIVKA-II |
|
|
|
|
|
|
|
≤40 | 21 | 9 | 0.030 | 2.99 | 1.19–7.52 | 0.020 |
|
>40 | 41 | 46 |
|
|
|
|
Discussion
We conducted a retrospective study of Chinese
patients with HBV-associated HCC to assess the value of determining
PIVKA-II levels as a biomarker of HCC, in particular, for
early-stage disease. We found that the overlap between PIVKA-II and
AFP levels in patients with early HCC was low and that evaluating
their levels in combination may serve as an effective component of
strategies for the management of early-stage HCC. Further, we show
here that high PIVKA-II levels were significantly associated with
MVI and high Ki67 expression, indicating an increased probability
of tumors to progress. Together, our data strengthen the prognostic
value of PIVKA-II levels. Moreover, multivariate analysis revealed
that PIVKA-II levels were an independent predictor of MVI and high
Ki67 expression.
Although the impact of HBV infection is declining
because of the recent implementation of China's nationwide HBV
vaccination program, liver cirrhosis caused by chronic HBV
infection is the major cause of HCC (3), which differs from the causes of HCC in
Japanese, Europeans, or Americans (23). Hence, we investigated the clinical
significance of PIVKA-II on this cohort of patients. PIVKA-II is a
promising biomarker for the diagnosis and prognosis of HCC
(14–18). For example, our previous study
demonstrates that PIVKA-II is an independent indicator of early
recurrence in patients with early HCC (35). PIVKA-II exhibited greater diagnostic
performance compared with AFP because of its higher sensitivity and
specificity (18). Moreover, the
combination of PIVKA-II and AFP was not more advantageous compared
with PIVKA-II (16,18,19), and
this combination impaired the diagnostic efficiency of PIVKA-II in
some subgroups because of the poor performance of AFP. However, in
the present study, we observed low overlap between positive
PIVKA-II and AFP data for patients with early HCC, and combining
the data greatly increased the rates of positive detection of
patients with early HCC.
We speculated that this discordance is attributed to
factors such as patient selection and different staging systems. We
therefore strongly recommend using these two biomarkers together
for HCC screening, in particular, for more patients with
early-stage tumors. These patients should undergo high-resolution
imaging scans to establish a definite diagnosis. Such efforts will
likely increase the number of patients suitable for curative
resection to improve prognosis. Further, our results suggest
combining PIVKA-II and AFP levels when evaluating the response to
treatment of patients with early HCC to compensate for the
disadvantages of using a single marker and to provide comprehensive
information that will improve the accuracy of clinical
assessments.
Here we evaluated the correlation between PIVKA-II
with the pathological parameters tumor cell differentiation, MVI,
CK19, GPC3, and HSP70, because they are significantly associated
with the prognosis of HCC (5,29,31,34) and
are routinely determined by the Department of Pathology, Fudan
University. We found further that preoperative PIVKA-II was an
independent predictor for MVI (HR, 3.77; 95% CI, 1.31–10.88;
P=0.014), which is consistent with findings of studies of Japanese
(36) and Western European cohorts
(19). Together, these findings
strongly suggest an association between PIVKA-II expression and
tumor cell invasion. Moreover, for the first time to our knowledge,
we report that PIVKA-II levels served as an independent predictor
for high Ki67 expression (HR, 2.99; 95% CI, 1.19–7.52; P=0.020).
Previous studies established the correlation between the PIVKA-II
level and tumor size (19,36), and PIVKA-II maintains the growth of
HCC (37). The present study provides
direct clinical evidence of the correlation between PIVKA-II and
cell proliferation. Taken together, our findings indicate that high
PIVKA-II levels may reflect a more aggressive tumor phenotype and
will therefore significantly improve the evaluation of tumor
prognosis to facilitate the delivery of individualized treatment
strategies.
When we performed ROC analysis, we found that the
sensitivity and specificity of PIVKA-II for predicting MVI and high
Ki67 expression were approximately 90.00 and 30.00%, respectively.
These findings indicate that a high true-positive rate of PIVKA-II
may nevertheless serve as an effective screening tool, although the
true-negative rate was insufficient for this purpose. We suggest
that the reason for low specificity may be the cutoff value of 40
mAU/ml, which is considered optimal for diagnosing Chinese patients
with HCC (16). We did not use a
different another cutoff value because of the small number of
subjects (n=117) studied here. Nevertheless, the correlation
between PIVKA-II and pathogenesis was significant. Establishing a
panel containing all independent predictors might overcome this
limitation. In fact, based on present cohort of patients, we
established a model comprising AFP, BCLC stage, and PIVKA-II, which
showed an AUC of 0.755 with 71.80% sensitivity and 68.70%
specificity for predicting MVI (data not shown). Moreover, we are
conducting a large cohort, multicenter study to systematically
evaluate the predictive performance of PIVKA-II.
There are limitations to our study other than the
small number of subjects. First, our study was retrospective.
Second, we did not perform next-generation PIVKA-II detection,
because it is not routinely preformed in clinical laboratories
(38), and we will further
investigate its clinical significance in the near future. Third,
the mechanism of the regulation of PIVKA-II of tumor cell invasion
(e.g., via modulating the EMT) was not investigated in detail.
In conclusion, the present study shows low overlap
between PIVKA-II and AFP levels in Chinese patients with
HBV-associated early HCC, which required implementing a combination
strategy. Further, we found for the first time, that the PIVKA-II
level served as an independent predictor of MVI and high Ki67
expression, indicating the clinical significance of PIVKA-II levels
and their value for enhancing the management of patients with HCC.
Moreover, we contribute new insights into the mechanism of
metastasis of HCC cells that may facilitate future studies aimed to
develop more effective treatment strategies.
Acknowledgements
This study was supported by grants from the National
High Technology Research and Development Program (863 Program) of
China (2015AA020401), the State Key Program of National Natural
Science of China (81530077), the National Natural Science
Foundation of China (81472676, 81572823, 81372317 and 81572064),
the Projects from the Shanghai Science and Technology Commission
(13140901900, 134119a1201, 14DZ1940300, 14411970200 and
14140902301), the Strategic Priority Research Program of the
Chinese Academy of Sciences (XDA12010202), Specialized Research
Fund for the Doctoral Program of Higher Education and Research
Grants Council Earmarked Research Grants Joint Research Scheme
(20130071140008), Key Developing Disciplines of Shanghai Municipal
Commission of Health and Family Planning (2015ZB0201), Research
Project of Shanghai Municipal Commission of Health and Family
Planning (201540052), the Funding Plan for Outstanding Youth
Doctors Training of Shanghai (2016-01), the National Natural
Science Foundation of China (81572064), and the Research Funding of
Shanghai Municipal Commission of Health and Family Planning
(201440389).
Glossary
Abbreviations
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
AFP
|
α-fetoprotein
|
|
PIVKA-II
|
prothrombin induced by vitamin K
absence-II
|
|
HBV
|
hepatitis B virus
|
|
HCV
|
hepatitis C virus
|
|
MVI
|
microvascular invasion
|
|
BCLC
|
Barcelona clinic liver cancer
|
|
GPC3
|
glypican 3
|
|
HSP70
|
heat shock protein 70
|
|
CK19
|
cytokeratin 19
|
|
ROC
|
receiver operating characteristics
|
|
AUC
|
area under curve
|
|
HR
|
hazard ratio
|
|
CI
|
confidence interval
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Levrero M and Zucman-Rossi J: Mechanisms
of HBV-induced hepatocellular carcinoma. J Hepatol. 64 Suppl
1:S84–S101. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bruix J and Sherman M: American
Association for the Study of Liver Diseases: Management of
hepatocellular carcinoma: An update. Hepatology. 53:1020–1022.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bruix J, Reig M and Sherman M:
Evidence-based diagnosis, staging and treatment of patients with
hepatocellular carcinoma. Gastroenterology. 150:835–853. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dhanasekaran R, Venkatesh SK, Torbenson MS
and Roberts LR: Clinical implications of basic research in
hepatocellular carcinoma. J Hepatol. 64:736–745. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Prieto J, Melero I and Sangro B:
Immunological landscape and immunotherapy of hepatocellular
carcinoma. Nat Rev Gastroenterol Hepatol. 12:681–700. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhu GQ, Shi KQ, Yu HJ, He SY, Braddock M,
Zhou MT, Chen YP and Zheng MH: Optimal adjuvant therapy for
resected hepatocellular carcinoma: A systematic review with network
meta-analysis. Oncotarget. 6:18151–18161. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Guo W, Yang XR, Sun YF, Shen MN, Ma XL, Wu
J, Zhang CY, Zhou Y, Xu Y, Hu B, et al: Clinical significance of
EpCAM mRNA-positive circulating tumor cells in hepatocellular
carcinoma by an optimized negative enrichment and qRT-PCR-based
platform. Clin Cancer Res. 20:4794–4805. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yang XR, Xu Y, Shi GM, Fan J, Zhou J, Ji
Y, Sun HC, Qiu SJ, Yu B, Gao Q, et al: Cytokeratin 10 and
cytokeratin 19: Predictive markers for poor prognosis in
hepatocellular carcinoma patients after curative resection. Clin
Cancer Res. 14:3850–3859. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shen Q, Fan J, Yang XR, Tan Y, Zhao W, Xu
Y, Wang N, Niu Y, Wu Z, Zhou J, et al: Serum DKK1 as a protein
biomarker for the diagnosis of hepatocellular carcinoma: A
large-scale, multicentre study. Lancet Oncol. 13:817–826. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li C, Zhang Z, Zhang P and Liu J:
Diagnostic accuracy of des-gamma-carboxy prothrombin versus
α-fetoprotein for hepatocellular carcinoma: A systematic review.
Hepatol Res. 44:E11–E25. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Singal A, Volk ML, Waljee A, Salgia R,
Higgins P, Rogers MA and Marrero JA: Meta-analysis: Surveillance
with ultrasound for early-stage hepatocellular carcinoma in
patients with cirrhosis. Aliment Pharmacol Ther. 30:37–47. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Meguro M, Mizuguchi T, Nishidate T, Okita
K, Ishii M, Ota S, Ueki T, Akizuki E and Hirata K: Prognostic roles
of preoperative α-fetoprotein and des-γ-carboxy prothrombin in
hepatocellular carcinoma patients. World J Gastroenterol.
21:4933–4945. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim JM, Hyuck C, Kwon D, Joh JW, Lee JH,
Paik SW and Park CK: Protein induced by vitamin K antagonist-II
(PIVKA-II) is a reliable prognostic factor in small hepatocellular
carcinoma. World J Surg. 37:1371–1378. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ji J, Wang H, Li Y, Zheng L, Yin Y, Zou Z,
Zhou F, Zhou W, Shen F and Gao C: Diagnostic evaluation of
des-gamma-carboxy prothrombin versus α-fetoprotein for hepatitis B
virus-related hepatocellular carcinoma in China: A Large-Scale,
Multicentre study. PLoS One. 11:e01532272016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Weitz IC and Liebman HA: Des-gamma-carboxy
(abnormal) prothrombin and hepatocellular carcinoma: A critical
review. Hepatology. 18:990–997. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lok AS, Sterling RK, Everhart JE, Wright
EC, Hoefs JC, Di Biscegile AM, Morgan TR, Kim HY, Lee WM, Bonkovsky
HL, et al: Des-gamma-carboxy prothrombin and alpha-fetoprotein as
biomarkers for the early detection of hepatocellular carcinoma.
Gastroenterology. 138:493–502. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Poté N, Cauchy F, Albuquerque M, Voitot H,
Belghiti J, Castera L, Puy H, Bedossa P and Paradis V: Performance
of PIVKA-II for early hepatocellular carcinoma diagnosis and
prediction of microvascular invasion. J Hepatol. 62:848–854. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kamiyama T, Yokoo H, Kakisaka T, Orimo T,
Wakayama K, Kamachi H, Tsuruga Y, Yanmashita K, Shimamura T, Todo S
and Taketomi A: Multiplication of alpha-fetoprotein and protein
induced by vitamin K absence-II is a powerful predictor of
prognosis and recurrence in hepatocellular carcinoma patients after
a hepatectomy. Hepatol Res. 45:E21–E31. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Masuda T, Beppu T, Okabe H, Nitta H, Imai
K, Hayashi H, Chikamoto A, Yamamoto K, Ikeshima S, Kuramoto M, et
al: Predictive factors of pathological vascular invasion in
hepatocellular carcinoma within 3 cm and three nodules without
radiological vascular invasion. Hepatol Res. 46:985–991. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kondo Y, Kimura O and Shimosegawa T:
Significant biomarkers for the management of hepatocellular
carcinoma. Clin J Gastroenterol. 8:109–115. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hu B, Yang XR, Xu Y, Sun YF, Sun C, Guo W,
Zhang X, Wang WM, Qiu SJ, Zhou J and Fan J: Systemic
immune-inflammation index predicts prognosis of patients after
curative resection for hepatocellular carcinoma. Clin Cancer Res.
20:6212–6222. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cucchetti A, Piscaglia F, Grigioni AD,
Ravaioli M, Cescon M, Zanello M, Grazi GL, Golfieri R, Grigioni WF
and Pinna AD: Preoperative prediction of hepatocellular carcinoma
tumour grade and micro-vascular invasion by means of artificial
neural network: A pilot study. J Hepatol. 52:880–888. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rodriguez-Perálvarez M, Luong TV, Andreana
L, Meyer T, Dhillon AP and Burroughs AK: A systematic review of
microvascular invasion in hepatocellular carcinoma: Diagnostic and
prognostic variability. Ann Surg Oncol. 20:325–339. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhang HM, Li SP, Yu Y, Wang Z, He JD, Xu
YJ, Zhang RX, Zhang JJ, Zhu ZJ and Shen ZY: Bi-directional roles of
IRF-1 on autophagy diminish its prognostic value as compared with
Ki67 in liver transplantation for hepatocellular carcinoma.
Oncotarget. 7:37979–37992. 2016.PubMed/NCBI
|
|
27
|
Altekruse SF, McGlynn KA, Dickie LA and
Kleiner DE: Hepatocellular carcinoma confirmation, treatment, and
survival in surveillance, epidemiology, and end results registries,
1992–2008. Hepatology. 55:476–482. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yamashita Y, Tsuijita E, Takeishi K,
Fujiwara M, Kira S, Mori M, Aishima S, Taketomi A, Shirabe K,
Ishida T and Maehara Y: Predictors for microinvasion of small
hepatocellular carcinoma ≤2 cm. Ann Surg Oncol. 19:2027–2034. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Schmilovitz-Weiss H, Tobar A, Halpern M,
Levy I, Shabtai E and Ben-Ari Z: Tissue expression of squamous
cellular carcinoma antigen and Ki67 in hepatocellular
carcinoma-correlation with prognosis: A historical prospective
study. Diagn Pathol. 6:1212011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Haruyama Y, Yorita K, Yamaguchi T,
Kitajima S, Amano J, Ohtomo T, Ohno A, Kondo K and Kataoka T: High
preoperative levels of serum glypican-3 containing N-terminal
subunit are associated with poor prognosis in patients with
hepatocellular carcinoma after partial hepatectomy. Int J Cancer.
137:1643–1651. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang C, Zhang Y, Guo K, Wang N, Jin H, Liu
Y and Qin W: Heat shock proteins in hepatocellular carcinoma:
Molecular mechanism and therapeutic potential. Int J Cancer.
138:1824–1834. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kang GH, Lee BS, Lee ES, Kim SH, Lee HY
and Kang DY: Prognostic significance of p53, mTOR, c-Met, IGF-1R,
and HSP70 overexpression after the resection of hepatocellular
carcinoma. Gut Liver. 8:79–87. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sun DW, Zhang YY, Sun XD, Chen YG, Qiu W,
Ji M and Lv GY: Prognostic value of cytokeratin 19 in
hepatocellular carcinoma: A meta-analysis. Clin Chim Acta.
448:161–169. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Feng J, Zhu R, Chang C, Yu L, Cao F, Zhu
G, Chen F, Xia H, Lv F, Zhang S and Sun L: CK19 and Glypican 3
expression profiling in the prognostic indication for patients with
HCC after surgical resection. PLoS One. 11:e01515012016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wang BL, Tan QW, Gao XH, Wu J and Guo W:
Elevated PIVKA-II is associated with early recurrence and poor
prognosis in BCLC 0-A hepatocellular carcinomas. Asian Pac J Cancer
Prev. 15:6673–6678. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Shirabe K, Toshima T, Kimura K, Yamashita
Y, Ikeda T, Ikegami T, Yoshizumi T, Abe K, Aishima S and Maehara Y:
New scoring system for prediction of microvascular invasion in
patients with hepatocellular carcinoma. Liver Int. 34:937–941.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cui SX, Zhang YS, Chu JH, Song ZY and Qu
XJ: Des-gamma-carboxy prothrombin (DCP) antagonizes the effects of
gefitinib on human hepatocellular carcinoma cells. Cell Physiol
Biochem. 35:201–212. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kurokawa T, Yamazaki S, Mitsuka Y,
Moriguchi M, Sugitani M and Takayama T: Prediction of vascular
invasion in hepatocellular carcinoma by next-generation
des-r-carboxy prothrombin. Br J Cancer. 114:53–58. 2016. View Article : Google Scholar : PubMed/NCBI
|