Introduction
Hassall's corpuscles (HCs) are characteristic
structures of the normal thymus and are commonly used as diagnostic
features for identifying the human thymus (1). The majority of studies consider that
they are derived from epithelial cells of the thymic medulla
(2–4).
Typical HCs are occasionally identified in areas with medullary
differentiation of World Health Organization (WHO) type B1-3
thymoma; however, they are not identified in type A and AB thymoma
(5–11). Thymoma with an abundance of HCs is
rare, with only five cases having been reported in the literature
(12), to the best of our knowledge.
The present case report concerns a type B2 thymoma with an
abundance of HCs in a 58-year-old Chinese woman and considers its
clinicopathological characteristics, immunological phenotype and
biological behavior. The aim of describing this rare type of
thymoma is so that it can be recognized and classified by
pathologists. In addition, it is advised that clinical doctors
should follow-up these patients due to its undefined biological
behavior.
Case report
A 58-year-old Chinese woman was admitted to the
Hainan Branch of General Hospital of the Chinese People's
Liberation Army (Hainan, China) on 19 April 2015 due to a repeated
pain in the right anterior chest for 6 months. The pain was often
exacerbated when the body posture was changed and was accompanied
simultaneously by malaise, without eyelid ptosis, cough, headache,
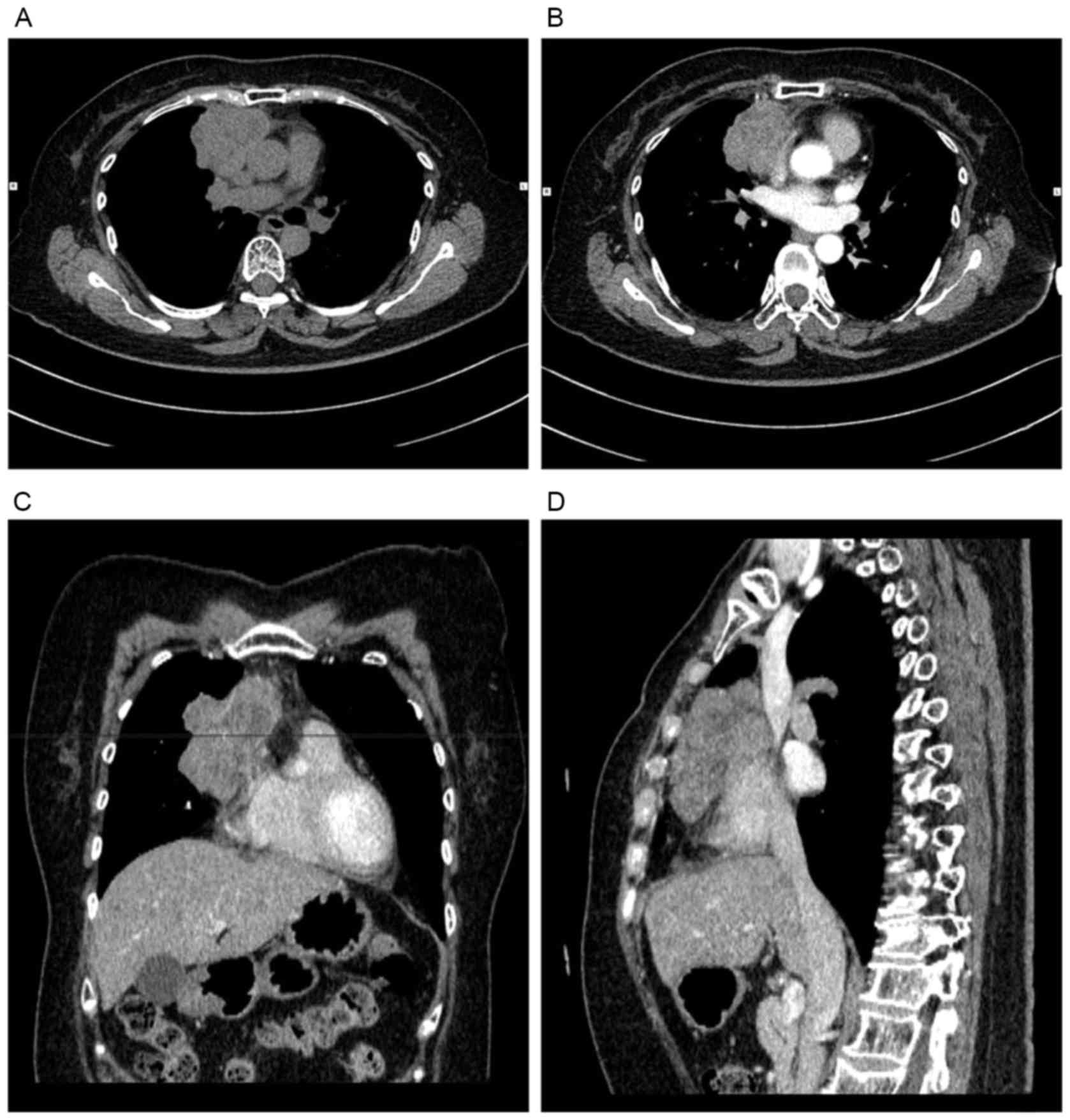
shortness of breath or dizziness. A computed tomography (CT) scan
of the chest revealed a heterogeneous mass, with a size of
8.2×6.2×4.6 cm in the right anterior superior mediastinum,
involving the right pericardium and wrapping around the superior
and inferior vena cava (Fig. 1).
Thus, an exploratory thoracotomy was performed. However, it was not
possible to resect the tumor completely as it was difficult to
separate it from the superior and inferior vena cava. Grossly, the
tumor adhered to the down lobe of the right lung, the size was
7.5×7.5×5 cm, the encapsulation was not intact, the cut surface was
yellow-grey and the texture was of a medium hardness. The resected
samples were fixed in 10% neutral formalin solution, and embedded
in paraffin. Serial sections were stained with hematoxylin and
eosin (H&E). Microscopically, a large quantity of HCs with
various morphologies, including solid, cystic, round and irregular,
were initially identified to be diffusely distributed. The size of
the HCs varied from extremely small to large. Large and polygonal
neoplastic epithelial cells were scattered individually or in small
clusters among immature lymphocytes, and formed a delicate loose
network. Their nucleoli were prominent. Only a limited number of
the tumor cells were arranged in the small papillary or nested
histoarchitecture in the focal area. Certain tumor cells were
involved in the lung tissues and adipose tissue out of the pleura.
Furthermore, the HCs in the tumor involved in the lung tissues
appeared to be small, and there were no cystic structures. Cystic
spaces filled with fibrin, blood or HCs, cholesterol crystal,
scarring, necrosis and calcium deposits were identified (Fig. 2). Immunohistochemically, Sections
(4-µm thick) from a representative block were deparaffinized in 99%
xylene for 15 min at room temperature, rehydrated in graded alcohol
(ethanol) with 100, 95, 80 and 75% in turn, incubated with 3%
H2O2 to block the activity of endogenous
peroxidases for 10 min at room temperature. The sections were then
subjected to heat-induced antigen retrieval in 0.1 mol/l citrate
buffer at pH 6.0 for 3 min following treatment with EDTA buffer at
pH 9.0 in a microwave for 15 min. The slides were then incubated
with ready-to-use mouse anti-human primary monoclonal antibody
against pan-cytokeratin (CK; MAB-0671), CK19 (kit-0020), cluster of
differentiation (CD)99 (MAB-0059), CD20 (MAB-0669), and CD1a
(MAB-0336), rabbit anti-human monoclonal antibodies against
epithelial membrane antigen (EMA) (kit-0011), CD5 (MAB-0252), and
CD117 (MAB-0590) for 1 h at 37°C. After excess primary antibody was
removed with PBS buffer solution, the ready-to-use goat
anti-mouse/rabbit IgG polymer conjugated with horseradish
peroxidase (kit-0016) were applied and incubated for 20 min at room
temperature. Then, a subsequent reaction was performed and
visualized using 40 µl 3.3′-diaminobenzidine (DAB) buffer with
fresh configuration (concentration, 0.2 g/20 ml PBS) for 5–8 min at
room temperature. Finally, the slides were incubated with
hematoxylin staining solution for 20 sec, and washed using water.
All of these reagents were provided by Maxim Biotech, Develop Co.
(Fuzhou, Fujian, China). After mounting, the slides were observed
by a light microscope (DM2500, Leica Microsystems Wetzlar GmbH).
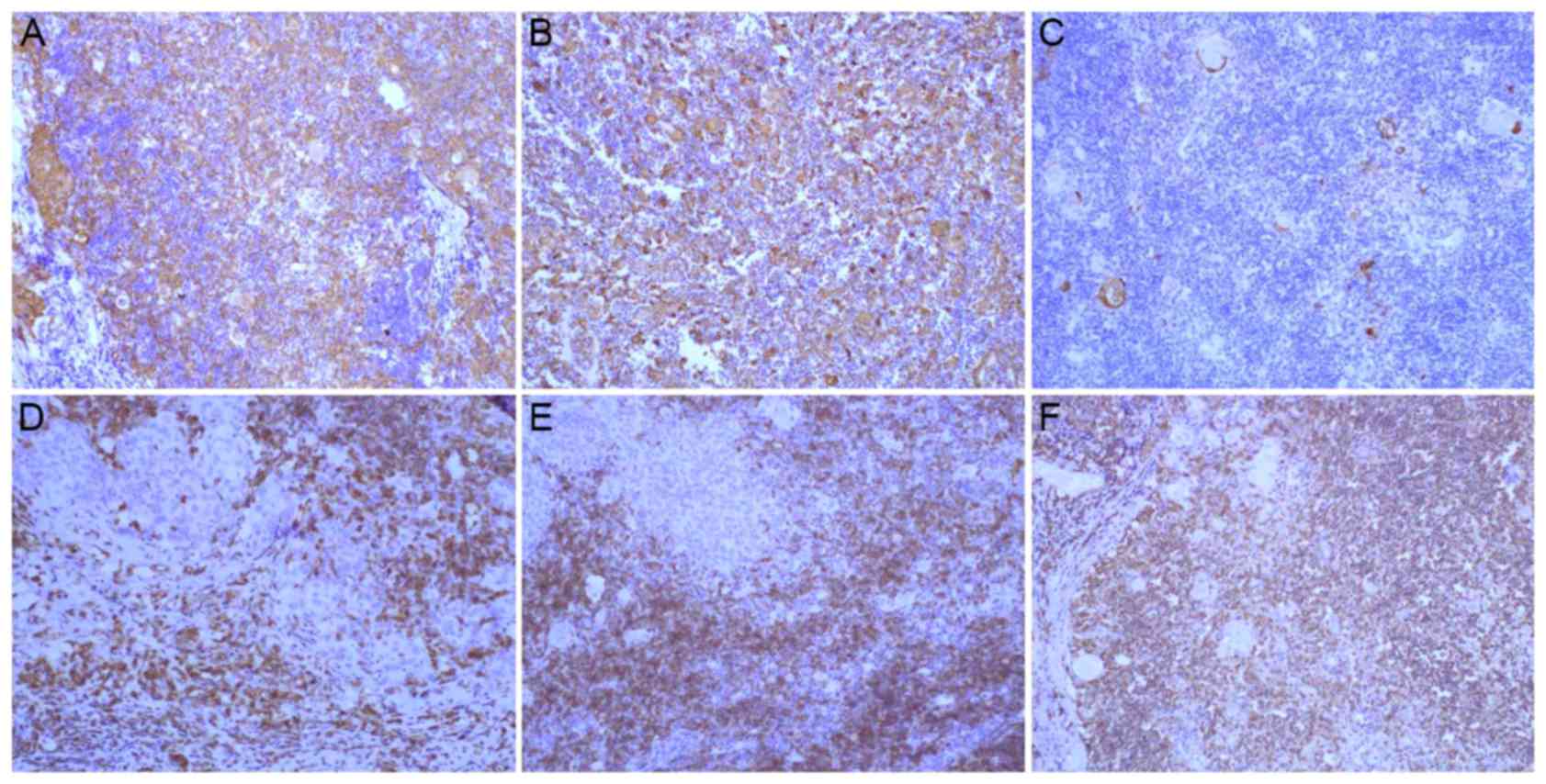
The results demonstrated that the tumor cells were positive for
pan-CK and CK19, and negative for EMA and CD5, CD117 and CD20
(Fig. 3). Intraepithelial lymphocytes
were positive for CD1a, CD5 and CD99. The index of Ki-67 was high
(~80%). Therefore, type B2 thymoma with an abundance of HCs was
eventually diagnosed. However, she did not undergo further therapy
and was discharged from the hospital for financial reasons.
Therefore, the patient was not followed-up until she revisited due
to pain in the right anterior chest 9 months after surgery.
Unfortunately, the patient was unwilling to undergo an imaging
examination again.
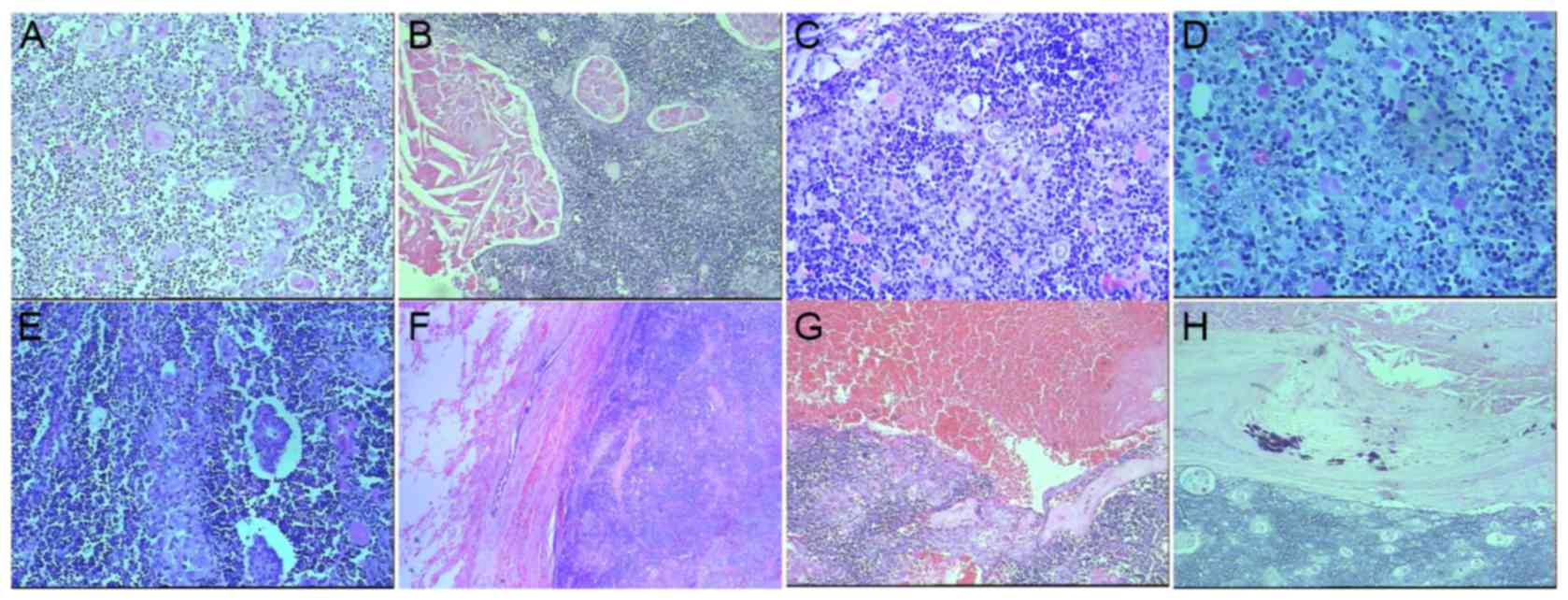 | Figure 2.Microscopically, large HCs with
various shapes, including solid, cystic, round and irregular HCs,
were found to diffusely distribute. The size of HCs varied from (A)
very small (magnification, ×200) to (B) very large (magnification,
×100). (C, magnification, ×400) Large and polygonal neoplastic
epithelial cells scattered individually or in small clusters among
immature lymphocytes, and (D, magnification, ×400) formed a
delicate loose network with prominent nucleoli. (E) Only a limited
number of tumor cells were arranged in small papillary or nested
histoarchitecture in focal area (magnification, ×200). (F) Certain
tumor cells were involved in the lung tissues (magnification,
×100). Cystic spaces filled with (G) fibrin, blood or HCs
(magnification, ×100). (H) Cholesterol crystal, scarring, necrosis
and calcium deposits were identified (magnification, ×100). |
Discussion
HCs, which are characteristic structures of the
human thymus, are derived from epithelial cells of the thymic
medulla (2–4). The physical nature of these structures
differs between mammalian species, for example, they are abundant
in the human thymus, but relatively rare in the mouse thymus
(13). It has been suggested
previously that HCs serve a function in the removal of apoptotic
thymocytes and the maturation of developing thymocytes within the
thymus (14). However, the function
remains to be elucidated. Typical HCs are occasionally identified
in areas with medullary differentiation of WHO type B1-3 thymoma;
however, they have not been identified in type A and AB thymoma
(5–11). Thymoma with an abundance of HCs is
rare, and has been termed ‘corpuscular thymoma’ by Laeng et
al (12). To the best of our
knowledge, only five cases have been reported previously (12). Clinically, the occurrence of the
majority of thymoma are latent and not easily observed. Only one
case demonstrated the symptom of eyelid ptosis. The other four
cases were asymptomatic and were incidentally identified.
Simultaneously, no association with myasthenia gravis or other
autoimmune diseases was observed. The patient in the present study
exhibited none of the aforementioned symptoms or diseases, with the
exception of a repeated pain in the right anterior chest. The age
range of the known cases was between 41 and 86 years, including the
present case, and the average age was 64 years when the diagnosis
was performed. The cases reported were of three men and three
women, suggesting that sex is not a factor.
Histopathologically, the morphology varied, although
they resembled type B2 or B3 thymoma (12). In the present case, the majority of
the epithelial cells formed a loose network and only a limited
number of tumor cells were arranged in a small papillary or nested
histoarchitecture in the focal area. The HCs were polymorphic,
including solid, cystic, round, and irregular shapes. The size of
HCs varied from extremely small to large. Cystic spaces, which were
filled with fibrin, blood or HCs, were also observed.
Immunohistochemically, the tumor cells were positive for CK19 and
pan-CK with reticular formation, and negative for EMA, CD5, CD117
and CD20. These characteristics differed from those of type B3
thymoma or squamous cell carcinoma. In addition, intraepithelial
lymphocytes were positive for CD1a, CD5 and CD99, and immature T
cells were identified. The above histopathological characteristics
and immunohistochemical features supported the diagnosis of type B2
thymoma. However, of note are the numerous HCs with polymorphism
and different sizes in thymoma, which instigated the observation of
various HCs. Only five cases, including three of type B2 and two of
type B3, have been described in the literature (12), to the best of our knowledge.
Furthermore, these previous studies had the same aim as that of the
present case report, and investigated whether this rare observation
maybe a distinct entity or variant of organotypical thymoma WHO
B2/B3, and also investigated the missing association between
thymoma with an abundance of HCs and thymic carcinoma. However, the
results demonstrated that the prevalence of HCs did not herald the
association between type B2/B3 thymoma and thymic carcinoma.
Finally, the previous studies considered that the corpuscular
differentiation was an option for neoplastic cells in organotypical
thymoma and may give rise to the predominant histoarchitectural
pattern, resulting in a rare distinct variant (12). This was also concluded in the present
case. In addition, a previous study demonstrated numerous and large
HCs, with highly polymorphic shapes, were identified in human
fetuses, and these increased rapidly in number and size at ~28
weeks of gestation, prior to subsequently increasing at a decreased
rate (1). It was speculated that
these HCs changes were also associated with the negative selection
process of thymocytes (1). It remains
to be elucidated whether a large quantity of HCs in the thymoma may
assist with removing apoptotic self-reacting thymocytes. However,
the study by Laeng et al (12)
detected the apoptotic cells in five cases of thymoma and the
results demonstrated that apoptotic cells were prominent in areas
of regressive change in all cases. Additionally, the labeling
indices of apoptotic cells outnumbered those for proliferating
neoplastic cells (12). However,
further studies are required to elucidate this molecular
mechanism.
Regarding biological behavior, the five cases
reported in the literature appeared indolent. By contrast, the
tumor in the present study was involved in the lung tissues and
right pericardium, although a number of distinctions, including
cholesterol crystal, scarring, necrosis and calcium deposits,
suggested that it was a long-standing lesion. Furthermore, the
tumor wrapped around the superior and inferior vena cava. Thus, the
biological behavior of the type of thymoma remains undefined.
Patients such as these should be followed-up
regularly. The patient in the present case report began having a
severe pain in the right anterior chest 9 months after surgery. It
was predicted that the tumor may recur for two reasons. One was
that the tumor was invasive, and the other was that the tumor
tissue adhering to the pericardium was not resected completely.
However, recurrence could not be confirmed as the individual did
not agree to undergo an imaging examination.
In conclusion, the type B2 or B3 thymoma abundance
of HCs is rare. Further elucidation is required as to whether it
represents a variant of WHO type B2 or B3 thymoma or whether it
qualifies as a distinct entity. In addition, it should be
differentiated from thymic hyperplasia.
Glossary
Abbreviations
Abbreviations:
|
CK
|
cytokeratin
|
|
CT
|
computed tomography
|
|
EMA
|
epithelial membrane antigen
|
|
HCs
|
Hassall's corpuscles
|
References
|
1
|
Asghar A, Syed YM and Nafis FA:
Polymorphism of Hassall's corpuscles in thymus of human fetuses.
Int J Appl Basic Med Res. 2:7–10. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Laster AJ, Itoh T, Palker TJ and Haynes
BF: The human thymic microenvironment: Thymic epithelium contains
specific keratins associated with early and late stages of
epidermal keratinocyte maturation. Differentiation. 31:67–77. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nicolas JF, Reano A, Kaiserlian D and
Thivolet J: Epithelial cell heterogeneity in mammalian thymus:
Monoclonal antibody to high molecular weight keratins exclusively
binds to Hassall's corpuscles. Histochem J. 21:357–364. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Boyd RL, Tucek CL, Godfrey DI, Izon DJ,
Wilson TJ, Davidson NJ, Bean AG, Ladyman HM, Ritter MA and Hugo P:
The thymic microenvironment. Immunol Today. 14:445–459. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kuo TT, Mukai K, Eimoto T, Laeng RH, Henry
K and Chan JKC: Type A thymomaTravis WD, Brambilla E,
Müller-Hermelink HK and Harris CC: Tumours of the Lungs, Pleura and
Mediastinum. World Health Organisation Classification of Tumours,
IARC Press; Lyon, France: pp. 154–158. 2004
|
|
6
|
Marino M and Müller-Hermelink HK: Thymoma
and thymic carcinoma. Relation of thymoma epithelial cells to the
cortical and medullary differentiation of thymus. Virchows Arch.
407:119–149. 1985. View Article : Google Scholar
|
|
7
|
Marx A and Müller-Hermelink HK: From basic
immunobiology to the upcoming WHO-classification of tumors of the
thymus. Pathol Res Pract. 195:515–533. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Müller-Hermelink HK, Marx A and Kirchner
T: Advances in the diagnosis and classification of thymic
epithelial tumoursAnthony PP and MacSween RNM: Recent Advances in
Histopathology. Churchill Livingstone, Edinburgh: pp. 49–72.
1994
|
|
9
|
Pan CC, Chen WY and Chiang H: Spindle cell
and mixed spindle/lymphocytic thymomas. An integrated
clinicopathologic and immunohistochemical study of 81 cases. Am J
Surg Path. 25:111–120. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Quintanilla-Martinez L, Wilkins EW Jr,
Choi N, Efird J, Hug E and Harris NL: Thymoma: Histologic
subclassification is an independent prognostic factor. Cancer.
74:606–617. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shimosato Y and Mukai K: Tumors of the
mediastinumRosai J and Sobin LH: Atlas of Tumor Pathology, Armed
Forces Institute of Pathology. Washington DC: pp. 93–101. 1997
|
|
12
|
Laeng RH, Eimoto T, Kuo TT, Zettl A, Marx
A, Moschopulos M, Tateyama H and Shimokawa K: Corpuscularthymoma:
Entity or variant of organotypicalthymomas WHO B2/B3? Pathol Res
Pract. 202:697–704. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Farr AG, Dooley JL and Erickson M:
Organization of thymic medullary epithelial heterogeneity:
Implications for mechanisms of epithelial differentiation. Immunol
Rev. 189:20–27. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Watanabe N, Wang YH, Lee HK, Ito T, Wang
YH, Cao W and Liu YJ: Hassall's corpuscles instruct dendritic cells
to induce CD4+CD25+ regulatory T cells in human thymus. Nature.
436:1181–1185. 2005. View Article : Google Scholar : PubMed/NCBI
|