Introduction
Breast cancer is the most prevalent and lethal
malignancy among females worldwide (1). In 2018, 1,735,350 incident breast cancer
cases are estimated to be diagnosed in the United States of America
and 609,640 associated mortalities are anticipated (2). Breast cancer is highly heterogeneous in
biological and clinical features, and multimodality measures,
including surgery, endocrinotherapy, chemotherapy and radiotherapy
have been developed for treatment, in the past few decades.
Precision medicine arising in recent years has been significant in
prolonging the survival of patients with specific genetic
backgrounds and improving their quality of life (3).
Molecular diagnosis allows the stratification of
breast cancer into four major subtypes based on the expression of
estrogen receptor (ER), progesterone receptor (PR) and human
epidermal growth factor receptor 2 (HER2) (4). Targeted therapies blocking the functions
of ER or HER2 have exhibited prominent clinical benefits in
patients with tumors positive for the ER, or HER2 receptors
(5,6).
However, the clinical outcome of a large number of patients remains
poor due to 30–40% of breast cancer cases being ER-negative and
70–80% being HER2-negative. Furthermore, 15–20% of patients with
triple negative breast cancer (TNBC) are negative for ER, PR and
HER2 (7). TNBC is a distinct subtype
of breast cancer that is characterized by frequent recurrence and
metastasis (8), and chemotherapy is
currently the only available systemic treatment approach.
Chemotherapy has been effective; however, it results in strong side
effects and high costs (9). In
general, patients who achieve pathological complete responses (pCR)
following neoadjuvant chemotherapy (NAC) typically have a favorable
prognosis (10). However, at present,
it is unclear what clinicopathological and molecular features may
be used to identify this subpopulation of patients.
Androgen receptor (AR) is a nuclear receptor, which,
upon the binding of androgen, forms a hormone-receptor complex that
acts on the androgen response elements of target genes to mediate
gene transcription (11). AR is
widely expressed in human tissues, including testis, ovary and
breast (12). Deletion of the
AR-encoding gene in mice leads to abnormal mammary gland
development and growth retardation (13). AR has drawn increasing attention in
the management of breast cancer in recent years, as AR is expressed
in ~80% of primary breast cancers and often at a higher level in
comparison with ER (14,15). This AR alteration explains the
clinical benefit rate of 20–25% in patients with breast cancer
treated by testosterone, as demonstrated in the 1970s (16). Testosterone was later replaced with
tamoxifen and aromatase inhibitors, due to its masculinizing
effects (17). These ER-modulating
drugs have been widely used; however, their efficacy can be limited
by patient intolerance (18,19). The observation that aromatase
inhibitors elevate androgen levels highlights the potential
significance of AR-modulating agents (20).
AR is upregulated in up to 53% of TNBC tumors
(14,21,22). There
are six subcategories of TNBC classified by gene expression
profiles: Basal-like 1, basal-like 2, immunomodulatory,
mesenchymal, mesenchymal stem-like and luminal androgen receptor
(LAR) (23). The LAR-type tumors are
usually abundant with AR upregulation (7). Unsurprisingly, a preclinical study
demonstrated that LAR-type breast cancer cell lines are sensitive
to AR antagonists (24). These
findings suggest AR may be a valuable prognostic marker in
TNBC.
In order to explore the clinical significance of AR
in TNBC, the expression of AR in 188 TNBC patients was examined and
its association with the outcome of 102 patients who were treated
with NAC was assessed. Using a cohort of 49 patients with tissue
samples collected prior to and following NAC, the effect of NAC on
AR expression in TNBC was also studied, and the prognosis function
of AR in correlation with survival rates was evaluated.
Materials and methods
Ethical approval
The present study was approved by the Research
Ethics Committee of Xiangya Hospital Central South University
(Changsha, China; approval no. 201303083). Written informed consent
was obtained from all patients to include their data in this
retrospective study.
Patient selection
A total of 188 patients, aged 49.42±9.73 years old
(mean ± standard deviation) with primary TNBC who underwent
treatment at Xiangya Hospital, Central South University, between
July 2011 and July 2014 were included. The patients were chosen
based on the pathological features, therapeutic approaches,
metastatic status, and availability of a complete medical record,
which included age, menstrual status, body mass index (BMI),
relevant family history, tumor grade and size, lymph node
involvement, clinical stage, Ki-67 expression, and clinical
follow-up information. All patients were diagnosed to have invasive
ductal carcinoma with no systemic metastases. Expression of HER2
was re-evaluated due to the positive threshold of the HER-2 testing
was 10%, reduced from 30% in 2009, and in fluorescent in
situ hybridization for positivity, the HER2/CEP17 ratio is ≥2,
or HER2 copy number is >6 signals per cell (25). HER2-positive patients were excluded
from the present study. Of the total 188 patients, 102 were treated
with NAC, which included 3–4 cycles (3 weeks/cycle) of docetaxel
(75 mg/m2), pirarubicine (50 mg/m2), or
cyclophosphamide (500 mg/m2). Matched pre- and
post-chemotherapy tissues were available for 49 patients. The pre-
and post-chemotherapy tissues were collected by needle core biopsy
and surgical excision, respectively.
Immunohistochemistry
Immunohistochemical analysis was performed following
a commonly used protocol outlined by the study of Shi et al
(26) with minor modifications.
Briefly, tissues were fixed, paraffin-embedded, and dissected into
4-µm thick sections. Serial sections were dewaxed in xylene,
rehydrated by a series of decreasing percentages of ethanol in
water, and rinsed with PBS. Antigen retrieval was performed by
heating the sections in a 95°C water bath in the presence of EDTA
in a microwave for 20 min. The slides were additionally treated
with 3% hydrogen peroxide (reagent 1; catalog no. PV-9000;
ZSGB-BIO; OriGene Technologies, Beijing, China) and blocked with
normal goat serum (ZSGB-BIO; OriGene Technologies) for 40 min in
room temperature. The tissue sections were then incubated overnight
at 4°C with a monoclonal mouse anti-AR (dilution 1:50; catalog no.
ab9474; Abcam, Cambridge, UK). The next day, the slides were
incubated with an undiluted polymer helper (reagent 2; catalog no.
PV-9000; ZSGB-BIO; OriGene Technologies) for 20 min at 37°C,
followed by staining with appropriate undiluted secondary
antibodies (reagent 3-mouse, catalog no. PV-9000, ZSGB-BIO; OriGene
Technologies) conjugated with poly-peroxidase for 20 min at 37°C.
Color was developed using diaminobenzidine as a chromogen. All
slides were assessed and scored by pathologists (light microscope;
Leica Microsystems GmbH, Wetzlar, Germany; magnifications, ×100 and
×400). By using the double-blind reading, pathologists selected 10
high magnification fields of view (×400) randomly, and counted
>100 cells in each field. Staining of AR was considered positive
when ≥1% of the tumor cell nuclei were stained.
Prognostic analysis
When accessible, patients were followed up monthly
until mortality or July 2016, the cutoff date for data collection.
Complete follow-up information was obtained for 188 patients by
outpatient review and phone communication. The patient data,
including dates of treatment and first recurrence, metastatic
status, and the TNBC-associated mortality were used to assess the
overall (OS) and disease-free survivals (DFS). OS was defined as
the period of time from the date of surgery to the date of
mortality associated with breast cancer or the last follow-up time.
DFS was defined as the period of time from the date of surgery to
the date of first recurrence, metastasis, or mortality associated
with breast cancer.
Statistical analysis
The data were analyzed by Statistical Package for
Social Sciences software version 22.0 (IBM Corp., Armonk, NY, USA).
Associations between AR expression, and clinicopathological
features and the outcome of NAC were assessed using χ2
or Fisher's exact tests. A Kaplan-Meier estimator and log-rank test
were used to assess the patient survival rate. A multivariate
analysis using the Cox proportional hazard regression model was
performed to assess prognosis. P<0.05 was considered to indicate
a statistically significant difference.
Results
AR is expressed in TNBC
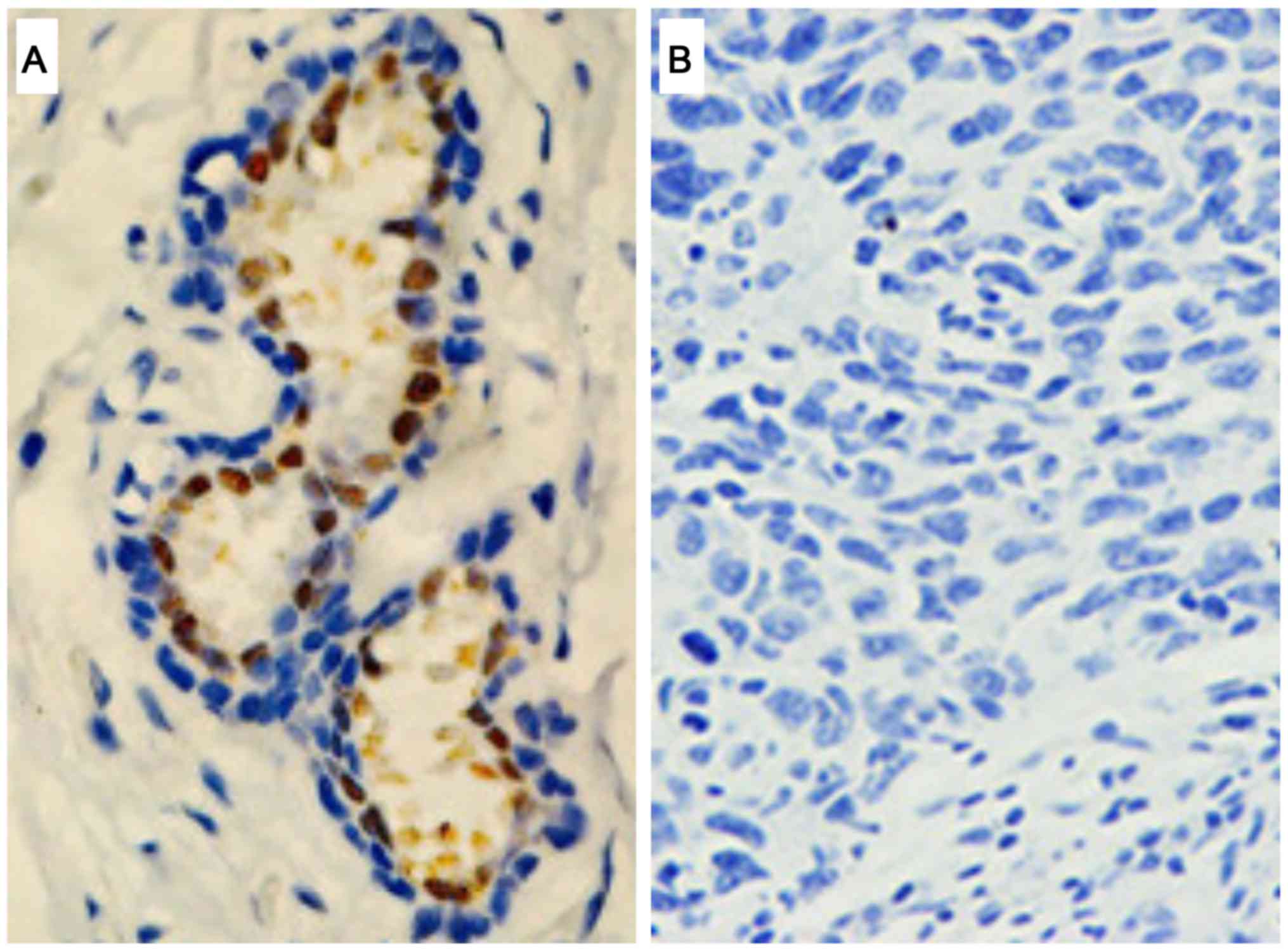
AR expression in TNBC was assessed by
immunohistochemistry (Table I). Among
the 188 patients diagnosed with TNBC, tumor sections from 41
patients (21.8%) stained positively for AR (AR+;
Fig. 1A), while others exhibited no
evident AR expression (AR–; Fig. 1B). Statistical analysis indicated a
significant association between AR expression and smaller tumors
(P=0.042; Table I), suggesting AR was
likely expressed during the early stage of cancer progression.
Consistently, the AR protein expression was significantly
associated with the localization of the tumors; TNBC with no lymph
node metastases more likely expressed AR (P=0.032, Table I). No significant association between
AR expression with age, menstrual status, BMI, family history,
tumor grade, clinical stage or Ki-67 expression was identified
(Table I).
 | Table I.Association between AR expression and
clinicopathological characteristics in 188 patients with TNBC. |
Table I.
Association between AR expression and
clinicopathological characteristics in 188 patients with TNBC.
|
| AR |
|
|
|---|
|
|
|
|
|
|---|
|
Characteristics | Positive (%) | Negative (%) | χ2 | P-value |
|---|
| Age (years) |
|
≤50 | 24 (21.6) | 87 (78.4) | 0.006 | 0.941 |
|
>50 | 17 (22.1) | 60 (77.9) |
|
|
| Menstrual
status |
|
Pre-menopause | 27 (21.8) | 97 (78.2) | <0.001 | 0.987 |
|
Post-menopause | 14 (21.9) | 50 (78.1) |
|
|
| BMI |
|
<24 | 28 (23.5) | 91 (76.5) | 0.563 | 0.453 |
|
≥24 | 13 (18.8) | 56 (81.2) |
|
|
| Family history |
| No | 36 (23.4) | 118 (76.6) | 1.228 | 0.268 |
|
Yes | 5 (14.7) | 29 (85.3) |
|
|
| Tumor grade |
|
I–II | 29 (21.5) | 106 (78.5) | 0.030 | 0.862 |
|
III | 12 (22.6) | 41 (77.4) |
|
|
| Tumor size
(cm) |
| ≤5 | 37 (25) | 111 (75) | 4.155 | 0.042 |
|
>5 | 4 (10) | 36 (90) |
|
|
| Lymph node
metastasis |
| No | 27 (28.1) | 69 (71.9) | 4.590 | 0.032 |
|
Yes | 14 (15.2) | 78 (84.8) |
|
|
| Clinical stage |
|
I–II | 31 (24.4) | 96 (75.6) | 1.553 | 0.213 |
|
III | 10 (16.4) | 51 (83.6) |
|
|
| Ki-67 |
|
<14 | 10 (23.3) | 33 (76.7) | 0.068 | 0.794 |
|
≥14 | 31 (21.4) | 114 (78.6) |
|
|
AR expression has no significant
effect on the outcome of chemotherapy
Of the 188 patients, 102 were treated with NAC
(Table II). Their responses were
assessed according to the guideline of the response evaluation
criteria in solid tumors (27) and
are summarized in Table II, together
with the clinicopathological features of the patients, in order to
identify the factors that affect response to NAC. The results
indicated that a higher BMI was the only parameter predicting pCR.
Among 102 patients treated by NAC, 20 (19.6%) were positive for AR
prior to treatment whereas the other 82 were negative (Table II). Following chemotherapy, 5/20
AR-positive patients (25%) exhibited pCR, while 12/82 AR-negative
patients (14.6%) exhibited pCR. However, no statistically
differences were identified between the two cohorts (P=0.316).
| Table II.Association between chemotherapeutic
effect and clinicopathologic characteristics in 102 patients with
TNBC. |
Table II.
Association between chemotherapeutic
effect and clinicopathologic characteristics in 102 patients with
TNBC.
|
| Chemotherapeutic
effect |
|
|
|---|
|
|
|
|
|
|---|
|
Characteristics | pCR (%) | Non-pCR (%) | χ2 | P-value |
|---|
| Age (years) |
|
|
|
|
|
≤50 | 11 (18.3) | 49 (81.7) | 0.291 | 0.589 |
|
>50 | 6 (14.3) | 36 (85.7) |
|
|
| Menstrual
status |
|
|
|
|
|
Pre-menopause | 13 (18.6) | 57 (81.4) | 0.583 | 0.445 |
|
Post-menopause | 4 (12.5) | 28 (87.5) |
|
|
| BMI |
|
|
|
|
|
<24 | 5 (7.8) | 59 (92.2) | 9.697 | 0.002 |
|
≥24 | 12 (31.6) | 26 (68.4) |
|
|
| Family history |
|
|
|
|
| No | 15 (17.9) | 69 (82.1) | 0.486 | 0.730 |
|
Yes | 2 (11.1) | 16 (88.9) |
|
|
| Tumor grade |
|
|
|
|
|
I–II | 15 (19.7) | 61 (80.3) | 2.023 | 0.226 |
|
III | 2 (7.7) | 24 (92.3) |
|
|
| Tumor size
(cm) |
|
|
|
|
| ≤5 | 10 (14.5) | 59 (85.5) | 0.726 | 0.394 |
|
>5 | 7 (21.2) | 26 (78.8) |
|
|
| Lymph node
metastasis |
|
|
|
|
| No | 6 (16.2) | 31 (83.8) | 0.008 | 0.927 |
|
Yes | 11 (16.9) | 54 (83.1) |
|
|
| Clinical stage |
|
|
|
|
|
I–II | 10 (18.9) | 43 (81.1) | 0.385 | 0.535 |
|
III | 7 (14.3) | 42 (85.7) |
|
|
| AR |
|
|
|
|
|
Negative | 12 (14.6) | 70 (85.4) | 1.244 | 0.316 |
|
Positive | 5 (25.0) | 15 (75.0) |
|
|
| Ki-67 |
|
|
|
|
|
<14 | 3 (13.0) | 20 (87.0) | 0.281 | 0.756 |
|
≥14 | 14 (17.7) | 65 (82.3) |
|
|
A total of 49/102 patients underwent
post-chemotherapy surgery to remove residual tumors, which were
sampled ex vivo for immunohistochemistry analysis. The
results indicated that tumors from 21/49 patients (42.9%) expressed
AR (Table III). Which was
significantly higher than the pre-chemotherapy data (19.6%)
(Table III), suggesting an
enrichment of AR-expressing tumors following chemotherapy
(P=0.008). As shown in Table III,
12 patients with AR-negative tumors were identified to have
AR-positive nodules following chemotherapy.
| Table III.Association between AR status and NAC
in 49 patients with TNBC. |
Table III.
Association between AR status and NAC
in 49 patients with TNBC.
|
| AR status prior to
NAC |
|
|
|---|
| AR status following
NAC | Positive (%) | Negative (%) | χ2 | P-value |
|---|
| Positive | 6 (28.6) | 15 (71.4) | 6.772 | 0.008 |
| Negative | 3 (10.7) | 25 (89.3) |
|
|
AR expression predicts a poor
prognosis for stage III TNBC
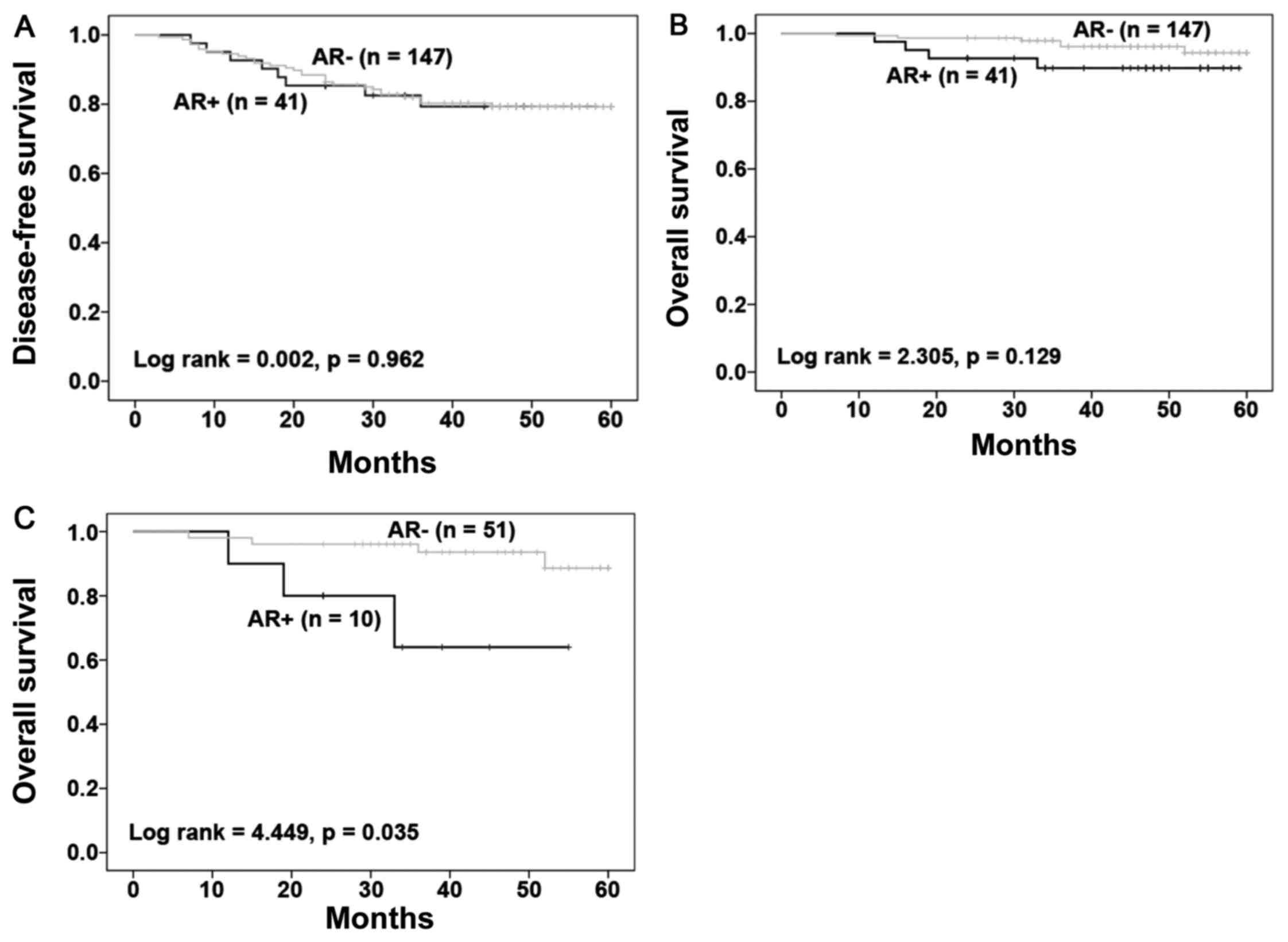
Whether AR expression was associated with patient
prognosis was then investigated. A total of 188 patients were
followed-up for up to 60 months, with 37 developing recurrent
diseases and 10 succumbing to breast cancer-associated mortality.
Kaplan-Meier survival analysis with a log-rank test was performed
to assess the association between AR expression and patient
survival. In AR-positive patients, the recurrence rate was 19.5%
(8/41), which was similar to 19.7% (29/147) in AR-negative
patients. During this period, the mortality in AR+ TNBC
was 9.76% (4/41) and the mortality in AR−TNBC was 4.08%
(6/147). The results indicated no significant correlation of AR
expression with the disease-free and overall survivals of patients
(Fig. 2A and B). However, AR
expression in stage III tumors (10/61 stage III cases) predicted a
poor survival of the patients (Fig.
2C; P=0.035) compared with those with no AR positivity (51
patients). In stage III tumors, the mortality in AR+
TNBC was 30% (3/10) and the mortality in AR-TNBC was 7.8% (4/51).
Among 127 stage I–II patients AR expression was not associated with
the survival of patients with early stage of cancer (data not
shown).
DFS is associated with age of patients
and clinical stage of disease
Univariate and multivariate analyses were performed
using 188 patients to identify crucial factors for DFS. Age >50
and clinical stage III were identified to be major risk factors for
reduced DFS compared with a younger age and early stages,
respectively, by univariate and multivariate analyses (Table IV). Lymph node metastasis was also a
risk factor for shorter DFS based on univariate analysis (Table IV). Advanced clinical stage was also
significantly associated with reduced OS based on univariate and
multivariate analyses.
| Table IV.Univariate and multivariate analysis
of disease-free survival in 188 patients with TNBC. |
Table IV.
Univariate and multivariate analysis
of disease-free survival in 188 patients with TNBC.
|
| Univariate | Multivariate |
|
|
|---|
|
|
|
|
|
|
|---|
| Parameters | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age (>50 years
vs. ≤50 years) | 2.007 | 1.041–3.870 | 0.038 | 2.003 | 1.030–3.896 | 0.041 |
| Tumor grade (III
vs. I–II) | 1.490 | 0.759–2.926 | 0.247 | 1.538 | 0.781–3.029 | 0.213 |
| Tumor size (>5
cm vs. ≤5 cm) | 1.258 | 0.594–2.666 | 0.549 | 0.700 | 0.291–1.687 | 0.427 |
| Lymph node
metastasis (Yes vs. no) | 2.350 | 1.181–4.678 | 0.015 | 1.783 | 0.808–3.935 | 0.152 |
| Clinical stage (III
vs. I–II) | 2.502 | 1.312–4.770 | 0.005 | 2.378 | 1.029–5.497 | 0.043 |
| AR (Positive vs.
negative) | 1.019 | 0.466–2.229 | 0.962 | 1.272 | 0.572–2.828 | 0.555 |
| Ki-67 (≥14 vs.
<14) | 1.677 | 0.699–4.023 | 0.247 | 1.488 | 0.614–3.603 | 0.379 |
Discussion
Androgen receptor mediates key processes in mammary
gland development, including ductal branching, formation of the
milk-producing alveoli and lobuloalveolar development (13). Accumulating evidence highlights its
crucial functions in cancer progression (7,28–30). In the present study, the expression of
AR in 188 patients with TNBC was determined using
immunohistochemistry and its potential value in predicting the
prognosis of patients with TNBC treated with NAC was assessed. The
results of the present study demonstrated that AR expression was
induced by NAC treatment and that AR expression in advanced-stage
tumors predicts a poor prognosis in patients with TNBC.
The immunohistochemistry data indicated that 21.8%
of the 188 TNBC cases are positive for AR. This is consistent with
previous findings that 10–53% TNBC tumors express AR (21,31–34). The
significant variations between different studies are attributable
to a lack of commonly accepted standards and analytical protocols
to determine the expression of AR by immunohistochemistry. Since AR
is not recognized as a prognostic molecule marker in breast cancer,
ER is usually assessed instead (35).
Furthermore, the thresholds for ER and HER2 expressions in the
American Society of Clinical Oncology/College of American
Pathologists guideline have been changed (25,35), which
resulted in significant decreases in the number of TNBC diagnoses.
In the present study, all TNBC cases were diagnosed following the
most recent guideline recommendations for the evaluation of ER, PR,
AR and HER-2 (25,35). Furthermore, patients with TNBC of
various ethnic backgrounds may express AR at different levels, with
previous meta-analysis demonstrating that AR expression was
slightly increased in Asians when compared with Caucasians
(36).
The results of the present study suggested that AR
is detected more often in smaller tumors or in cases with no lymph
node metastases. This is consistent with previous findings that
AR+ carcinomas were highly differentiated and had a low
Ki-67 labeling index (33,34,37,38). In
preclinical experiments, AR had an anti-proliferative effect
through stimulating the expression of ERβ, which inhibited cell
growth (39), and AR has been
demonstrated to mediate signaling pathways, including Janus
kinase/signal transducer and activator of transcription 3,
microtubule affinity regulating kinase, NOTCH and
phosphatidylinositol 3-kinase (PI3K)/mechanistic target of
rapamycin kinase (mTOR)/AKT serine/threonine kinase (40). The multifaceted roles of AR in TNBC
implicate that it may be a useful clinical marker.
No significant association was identified between AR
expression and the response to NAC in the present study although a
lower pCR rate has previously been demonstrated in AR+
compared with AR– patients (41). This may be due to the limited number
of AR+ cases treated with NAC in the present study.
Also, NAC induced AR expression in certain patients with TNBC,
which is likely due to a lower susceptibility of AR+
cells to NAC when compared with AR− cells in the present
study. A hypothesis is that chemotherapy drugs kill more
AR− cells than AR+ cells, resulting in the
upregulation of AR gene expression and AR+ cells
exhibiting chemotherapeutics resistance (42), thus hormone receptor negative breast
cancer are more likely to benefit from chemotherapy. Chemotherapy
insensitive or resistant triple-negative breast cancer may have
high levels of AR expression; therefore, AR-directed therapy may be
used in AR+ TNBC, which poorly responds to
chemotherapy.
No consistent findings have been reported regarding
the association between AR expression and patient survival. While
AR expression predicts better OS and DFS in general breast cancer
or patients with TNBC (41,43–45), there
are also reports that AR positivity is associated with poor
prognosis (34,46–48) or is
irrelevant to patient survival (37).
The results of the present study demonstrated no significant
association between AR expression with the survival of 188 patients
with TNBC without stratification. The contradictory conclusions
warrant future multi-institutional studies, in which universal
standards should be used in the examination of AR expression and
the definition of TNBC. However, AR+ status was
significantly associated with poor overall survival of stage III
patients, suggesting the prognostic value of AR for patients with
advanced stage TNBC. This result is consistent with previous
findings that AR+ TNBC cells are chemoresistant
(42). In ER-negative TNBC, AR
stimulates tumor growth by activating the ER signaling pathway
(49). As with the molecular apocrine
profile (ER−, AR+), it exhibits a high
invasive ability and poor prognosis (50). A total of 90% of patients with TNBC
have gene mutations, deletions or amplifications (23), consequently the mechanism of AR in
TNBC is not clearly understood.
Prostate cancer is the second most prevalent cancer
among males worldwide and it is also a hormone dependent cancer
(2). Androgens stimulate the
occurrence and development of TNBC molecular by binding AR, and the
modulation of androgen levels can be effective in the treatment of
prostate cancer (51). Therefore,
AR-directed therapy may be effective in a specific group of
patients, those with AR+ TNBC, which may increase
survival rates. As bicalutamide treatment gains great success in
prostate cancer (52), numerous
preclinical or clinical studies are committed to the application of
AR antagonists in TNBC (53–57). LAR breast cancer cell lines are
sensitive to AR antagonists. Furthermore, the study of Cuenca-Lopez
et al (53) reported that
AR+ TNBC cell line, which did not belong to the LAR
subtype, also had a sensitivity to AR inhibition. In early clinical
trials, patients with advanced AR+ TNBC were treated
with bicalutamide with a clinical benefit rate of 20% (54). In a phase II clinical trial of
enzalutamide, which has a six-fold higher affinity to AR than
previous bicalutamide, 42% patients with advanced AR+
TNBC attained a clinical benefit time of 16 weeks in preliminary
data (55). Subsequently, cytochrome
P450 enzyme inhibitors, including abiraterone acetate, act on
microsomal enzyme to suppress androgen production (56). The study of O'Shaughnessy et al
(57), identified that in
post-menopausal women with letrozole-pretreated metastatic
ER+ breast cancer, combining abiraterone acetate with
exemestane did not improve progression free survival compared with
treatment with single exemestane.
Selective androgen receptor modulators (SARMs) are
novel AR-directed therapies, which have high specificity for AR
without masculinizing side effects. Additionally, SARMs improve the
side effects of advanced breast cancer by increasing muscle mass
and restoring bone mineral density (58). GTx-024 is the one of the precedent
SARMs (59). At present, there are a
number of drugs about TNBC currently undergoing clinical trials.
Nevertheless, an absence of adequate evidence has resulted in these
drugs requiring approval. The combination therapy of TNBC may be
considered due to the involvement of AR-mediation in numerous
signaling pathways. The study of Lehmann et al (24), discovered that in AR+ TNBC
cells, PI3K/mTOR inhibitors in combination with an AR antagonist
had an additive growth inhibitory effect. The present study merely
discussed AR expression and its relation to survival time in TNBC.
Whether AR will function as a therapeutic target is subject to the
outcome of clinical trials.
In the 188 patients with TNBC evaluated in this
study, AR was expressed in ~21% of them, most often in small
nodules or tumors with no lymph node metastases. AR expression does
not determine the outcome of NAC; however, NAP may be enriched
during chemotherapeutic treatment. The results of the present study
suggest that AR expression has potential prognostic value in the
prognosis of TNBC, but is limited to patients in the advanced stage
of disease.
Acknowledgements
The authors would like to thank the members of
Breast Cancer Prevention and Clinical Research Center (Changsha,
China) for data collection.
Funding
The present study was funded by the National Natural
Science Foundation of China for Young Scholar (grant no. 81302289)
and Breast Cancer Clinical Medical Technology Research Center in
Hunan Province (grant no. 2010TP4053).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Author contributions
LT and KZ conceived and designed the experiments. YL
performed the experiments and analyzed data. LT, KZ and YL provided
final approval of the manuscript.
Ethical approval and consent to
participate
All procedures performed in studies involving human
participants were in accordance with the ethical standards of the
institutional and/or national research committee and with the 1964
Helsinki declaration and its later amendments or comparable ethical
standards. Informed consent was obtained from all individual
participants included in the study.
Consent for publication
Written informed consent was obtained from all
patients to publish their data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Arnedos M, Vicier C, Loi S, Lefebvre C,
Michiels S, Bonnefoi H and Andre F: Precision medicine for
metastatic breast cancer-limitations and solutions. Nat Rev Clin
Oncol. 12:693–704. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cancer Genome Atlas Network: Comprehensive
molecular portraits of human breast tumours. Nature. 490:61–70.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lumachi F, Santeufemia DA and Basso SM:
Current medical treatment of estrogen receptor-positive breast
cancer. World J Biol Chem. 6:231–239. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ross JS, Slodkowska EA, Symmans WF,
Pusztai L, Ravdin PM and Hortobagyi GN: The HER-2 receptor and
breast cancer: Ten years of targeted anti-HER-2 therapy and
personalized medicine. Oncologist. 14:320–368. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lehmann BD, Bauer JA, Chen X, Sanders ME,
Chakravarthy AB, Shyr Y and Pietenpol JA: Identification of human
triple-negative breast cancer subtypes and preclinical models for
selection of targeted therapies. J Clin Invest. 121:2750–2767.
2011. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Steward L, Conant L, Gao F and
Margenthaler J: Predictive factors and patterns of recurrence in
patients with triple negative breast cancer. Ann Surg Oncol.
21:2165–2171. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hassett MJ, O'Malley AJ, Pakes JR,
Newhouse JP and Earle CC: Frequency and cost of
chemotherapy-related serious adverse effects in a population sample
of women with breast cancer. J Natl Cancer Inst. 98:1108–1117.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liedtke C, Mazouni C, Hess KR, André F,
Tordai A, Mejia JA, Symmans WF, Gonzalez-Angulo AM, Hennessy B,
Green M, et al: Response to neoadjuvant therapy and long-term
survival in patients with triple-negative breast cancer. J Clin
Oncol. 26:1275–1281. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shang Y, Myers M and Brown M: Formation of
the androgen receptor transcription complex. Mol Cell. 9:601–610.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
McNamara KM, Moore NL, Hickey TE, Sasano H
and Tilley WD: Complexities of androgen receptor signalling in
breast cancer. Endocr Relat Cancer. 21:T161–T181. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yeh S, Hu Y, Wang P, Xie C, Xu Q, Tsai M,
Dong Z, Wang R, Lee T and Chang C: Abnormal mammary gland
development and growth retardation in female mice and MCF7 breast
cancer cells lacking androgen receptor. J Exp Med. 198:1899–1908.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Niemeier LA, Dabbs DJ, Beriwal S, Striebel
JM and Bhargava R: Androgen receptor in breast cancer: Expression
in estrogen receptor-positive tumors and in estrogen
receptor-negative tumors with apocrine differentiation. Mod Pathol.
23:205–212. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Park S, Koo JS, Kim MS, Park HS, Lee JS,
Lee JS, Kim SI, Park BW and Lee KS: Androgen receptor expression is
significantly associated with better outcomes in estrogen
receptor-positive breast cancers. Ann Oncol. 22:1755–1762. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Goldenberg IS: Testosterone propionate
therapy in breast cancer. JAMA. 188:1069–1072. 1964. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Garay JP and Park BH: Androgen receptor as
a targeted therapy for breast cancer. Am J Cancer Res. 2:434–445.
2012.PubMed/NCBI
|
|
18
|
Chia K, O'Brien M, Brown M and Lim E:
Targeting the androgen receptor in breast cancer. Curr Oncol Rep.
17:42015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fujii R, Hanamura T, Suzuki T, Gohno T,
Shibahara Y, Niwa T, Yamaguchi Y, Ohnuki K, Kakugawa Y, Hirakawa H,
et al: Increased androgen receptor activity and cell proliferation
in aromatase inhibitor-resistant breast carcinoma. J Steroid
Biochem Mol Biol. 144:513–522. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Maugeri-Saccà M, Barba M, Vici P, Pizzuti
L, Sergi D, De Maria R and Di Lauro L: Aromatase inhibitors for
metastatic male breast cancer: Molecular, endocrine, and clinical
considerations. Breast Cancer Res Treat. 147:227–235. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Qi JP, Yang YL, Zhu H, Wang J, Jia Y, Liu
N, Song YJ, Zan LK, Zhang X, Zhou M, et al: Expression of the
androgen receptor and its correlation with molecular subtypes in
980 chinese breast cancer patients. Breast Cancer (Auckl). 6:1–8.
2012.PubMed/NCBI
|
|
22
|
McNamara KM, Yoda T, Takagi K, Miki Y,
Suzuki T and Sasano H: Androgen receptor in triple negative breast
cancer. J Steroid Biochem Mol Biol. 133:66–76. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Xu H, Eirew P, Mullaly SC and Aparicio S:
The omics of triple-negative breast cancers. Clin Chem. 60:122–133.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lehmann BD, Bauer JA, Schafer JM,
Pendleton CS, Tang L, Johnson KC, Chen X, Balko JM, Gómez H,
Arteaga CL, et al: PIK3CA mutations in androgen receptor-positive
triple negative breast cancer confer sensitivity to the combination
of PI3K and androgen receptor inhibitors. Breast Cancer Res.
16:4062014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wolff AC, Hammond ME, Hicks DG, Dowsett M,
McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M,
Fitzgibbons P, et al: Recommendations for human epidermal growth
factor receptor 2 testing in breast cancer: American Society of
Clinical Oncology/College of American Pathologists clinical
practice guideline update. Arch Pathol Lab Med. 138:241–256. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Shi SR, Guo J, Cote RJ, Young L, Hawes D,
Shi Y, Thu S and Taylor CR: Sensitivity and detection efficiency of
a novel two-step detection system (PowerVision) for
immunohistochemistry. Appl Immunohistochem. 7:201–208. 1999.
View Article : Google Scholar
|
|
27
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chia KM, Liu J, Francis GD and Naderi A: A
feedback loop between androgen receptor and ERK signaling in
estrogen receptor-negative breast cancer. Neoplasia. 13:154–166.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Micello D, Marando A, Sahnane N, Riva C,
Capella C and Sessa F: Androgen receptor is frequently expressed in
HER2-positive, ER/PR-negative breast cancers. Virchows Arch.
457:467–476. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Robinson JL, Macarthur S, Ross-Innes CS,
Tilley WD, Neal DE, Mills IG and Carroll JS: Androgen receptor
driven transcription in molecular apocrine breast cancer is
mediated by FoxA1. EMBO J. 30:3019–3027. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Rakha EA, El-Sayed ME, Green AR, Lee AH,
Robertson JF and Ellis IO: Prognostic markers in triple-negative
breast cancer. Cancer. 109:25–32. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
McNamara KM, Yoda T, Miki Y, Chanplakorn
N, Wongwaisayawan S, Incharoen P, Kongdan Y, Wang L, Takagi K, Mayu
T, et al: Androgenic pathway in triple negative invasive ductal
tumors: Its correlation with tumor cell proliferation. Cancer Sci.
104:639–646. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Thike AA, Chong Yong-Zheng L, Cheok PY, Li
HH, Yip Wai-Cheong G, Bay Huat B, Tse GM, Iqbal J and Tan PH: Loss
of androgen receptor expression predicts early recurrence in
triple-negative and basal-like breast cancer. Mod Pathol.
27:352–360. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Choi JE, Kang SH, Lee SJ and Bae YK:
Androgen receptor expression predicts decreased survival in early
stage triple-negative breast cancer. Ann Surg Oncol. 22:82–89.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hammond ME, Hayes DF, Dowsett M, Allred
DC, Hagerty KL, Badve S, Fitzgibbons PL, Francis G, Goldstein NS,
Hayes M, et al: American Society of Clinical Oncology/College of
American Pathologists guideline recommendations for
immunohistochemical testing of estrogen and progesterone receptors
in breast cancer (unabridged version). Arch Pathol Lab Med.
134:e48–e72. 2010.PubMed/NCBI
|
|
36
|
Zhang L, Fang C, Xu X, Li A, Cai Q and
Long X: Androgen receptor, EGFR, and BRCA1 as biomarkers in
triple-negative breast cancer: A meta-analysis. Biomed Res Int.
2015:3574852015.PubMed/NCBI
|
|
37
|
Mrklić I, Pogorelić Z, Ćapkun V and Tomić
S: Expression of androgen receptors in triple negative breast
carcinomas. Acta Histochem. 115:344–348. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ricciardi GR, Adamo B, Ieni A, Licata L,
Cardia R, Ferraro G, Franchina T, Tuccari G and Adamo V: Androgen
receptor (AR), E-Cadherin, and Ki-67 as emerging targets and novel
prognostic markers in triple-negative breast cancer (TNBC)
patients. PloS One. 10:e01283682015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Honma N, Horii R, Iwase T, Saji S, Saji S,
Younes M, Takubo K, Matsuura M, Ito Y, Akiyama F and Sakamoto G:
Clinical importance of estrogen receptor-beta evaluation in breast
cancer patients treated with adjuvant tamoxifen therapy. J Clin
Oncol. 26:3727–3734. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Anestis A, Karamouzis MV, Dalagiorgou G
and Papavassiliou AG: Is androgen receptor targeting an emerging
treatment strategy for triple negative breast cancer? Cancer Treat
Rev. 41:547–553. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Loibl S, Müller BM, von Minckwitz G,
Schwabe M, Roller M, Darb-Esfahani S, Ataseven B, du Bois A,
Fissler-Eckhoff A, Gerber B, et al: Androgen receptor expression in
primary breast cancer and its predictive and prognostic value in
patients treated with neoadjuvant chemotherapy. Breast Cancer Res
Treat. 130:477–487. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lehmann BD and Pietenpol JA:
Identification and use of biomarkers in treatment strategies for
triple-negative breast cancer subtypes. J Pathol. 232:142–150.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Luo X, Shi YX, Li ZM and Jiang WQ:
Expression and clinical significance of androgen receptor in triple
negative breast cancer. Chin J Cancer. 29:585–590. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Gasparini P, Fassan M, Cascione L, Guler
G, Balci S, Irkkan C, Paisie C, Lovat F, Morrison C, Zhang J, et
al: Androgen receptor status is a prognostic marker in non-basal
triple negative breast cancers and determines novel therapeutic
options. PLoS One. 9:e885252014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Vera-Badillo FE, Templeton AJ, de Gouveia
P, Diaz-Padilla I, Bedard PL, Al-Mubarak M, Seruga B, Tannock IF,
Ocana A and Amir E: Androgen receptor expression and outcomes in
early breast cancer: A systematic review and meta-analysis. J Natl
Cancer Inst. 106:djt3192014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Hu R, Dawood S, Holmes MD, Collins LC,
Schnitt SJ, Cole K, Marotti JD, Hankinson SE, Colditz GA and Tamimi
RM: Androgen receptor expression and breast cancer survival in
postmenopausal women. Clin Cancer Res. 17:1867–1874. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Sutton LM, Cao D, Sarode V, Molberg KH,
Torgbe K, Haley B and Peng Y: Decreased androgen receptor
expression is associated with distant metastases in patients with
androgen receptor-expressing triple-negative breast carcinoma. Am J
Clin Pathol. 138:511–516. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
McGhan LJ, McCullough AE, Protheroe CA,
Dueck AC, Lee JJ, Nunez-Nateras R, Castle EP, Gray RJ, Wasif N,
Goetz MP, et al: Androgen receptor-positive triple negative breast
cancer: A unique breast cancer subtype. Ann Surg Oncol. 21:361–367.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Doane AS, Danso M, Lal P, Donaton M, Zhang
L, Hudis C and Gerald WL: An estrogen receptor-negative breast
cancer subset characterized by a hormonally regulated
transcriptional program and response to androgen. Oncogene.
25:3994–4008. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Tsutsumi Y: Apocrine carcinoma as
triple-negative breast cancer: Novel definition of apocrine-type
carcinoma as estrogen/progesterone receptor-negative and androgen
receptor-positive invasive ductal carcinoma. Jpn J Clin Oncol.
42:375–386. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Komura K, Sweeney CJ, Inamoto T, Ibuki N,
Azuma H and Kantoff PW: Current treatment strategies for advanced
prostate cancer. Int J Urol. 2017.
|
|
52
|
Loblaw DA, Virgo KS, Nam R, Somerfield MR,
Ben-Josef E, Mendelson DS, Middleton R, Sharp SA, Smith TJ, Talcott
J, et al: Initial hormonal management of androgen-sensitive
metastatic, recurrent, or progressive prostate cancer: 2006 update
of an American Society of Clinical Oncology practice guideline. J
Clin Oncol. 25:1596–1605. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Cuenca-López MD, Montero JC, Morales JC,
Prat A, Pandiella A and Ocana A: Phospho-kinase profile of triple
negative breast cancer and androgen receptor signaling. BMC Cancer.
14:3022014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Gucalp A, Tolaney S, Isakoff SJ, Ingle JN,
Liu MC, Carey LA, Blackwell K, Rugo H, Nabell L, Forero A, et al:
Phase II Trial of bicalutamide in patients with androgen
receptor-positive, estrogen receptor-negative metastatic breast
cancer. Clin Cancer Res. 19:5505–5512. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Traina TA, Miller K, Yardley DA, Eakle J,
Schwartzberg LS, O'Shaughnessy J, Gradishar W, Schmid P, Winer E,
Kelly C, et al: Enzalutamide for the treatment of androgen
receptor-expressing triple-negative breast cancer. J Clin Oncol.
JCO20167134952018.
|
|
56
|
Attard G, Reid AH, A'Hern R, Parker C,
Oommen NB, Folkerd E, Messiou C, Molife LR, Maier G, Thompson E, et
al: Selective inhibition of CYP17 with abiraterone acetate is
highly active in the treatment of castration-resistant prostate
cancer. J Clin Oncol. 27:3742–3748. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
O'Shaughnessy J, Campone M, Brain E, Neven
P, Hayes D, Bondarenko I, Griffin TW, Martin J, De Porre P, Kheoh
T, et al: Abiraterone acetate, exemestane or the combination in
postmenopausal patients with estrogen receptor-positive metastatic
breast cancer. Ann Oncol. 27:106–113. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Narayanan R, Coss CC and Dalton JT:
Development of selective androgen receptor modulators (SARMs). Mol
Cell Endocrinol: pii. S0303-7207(17)30340-4. 2017.
|
|
59
|
Narayanan R, Ahn S, Cheney MD, Yepuru M,
Miller DD, Steiner MS and Dalton JT: Selective Androgen receptor
modulators (SARMs) negatively regulate triple-negative breast
cancer growth and epithelial: Mesenchymal stem cell signaling. PLoS
One. 9:e1032022014. View Article : Google Scholar : PubMed/NCBI
|