Introduction
As the most common non-Hodgkin lymphoma, diffuse
large B cell lymphoma (DLBCL) contributes to the high mortality
rate of lymphoma with its aggressive features, and incidences have
increased over the past decades (1).
Due to the clinical application of Rituximab, the survival rate of
DLBCL patients has improved (2,3).
Prognostic factors such as age, clinical symptoms and serum
products, once used for predicting the survival of patients, no
longer give such a clear indication of survival rate. The
efficiency of International Prognostic Index (IPI) may be enhanced
by the inclusion of additional prognostic biomarkers during
diagnosis (4). Furthermore,
chemotherapy treatment is followed by a high incidence of
recurrence, which is unable to be prevented by the initial
therapeutic strategy, making the predictions more complicated
(5). Therefore, prognostic predictors
in lymphoma patients may be of considerable value in guiding
treatment, or may act as novel therapeutic targets.
MicroRNA-155 (miR-155) has been well established as
a hematopoietic oncogene, and is overexpressed in aggressive
lympho-proliferative disorders such as DLBCL, Hodgkin lymphoma,
Burkitt lymphoma and various types of T cell lymphomas (6–9). Although
the pathological signaling pathway of miR-155 remains to be
elucidated, it is a useful biomarker in diagnosis, aiding with
therapeutic decisions and prediction outcomes. Various studies have
suggested miR-155 has the potential to be a therapeutic target in
the treatment of lymphoma (10–12);
however, little is known about its specific effect on DLBCL
prognosis.
The association between Epstein-Barr virus (EBV)
infection and lymphoma has been confirmed by a number of studies
(13–15). EBV is present in two forms, similar to
other human herpes viruses: latency and lytic replication. The main
EBV latent products include EBV nuclear antigens, latent membrane
proteins (LMPs), EBV-encoded small RNAs and miRs (16). It is well demonstrated that viral
latent products contribute to oncologic induction. It has been
demonstrated that EBV infection is limited to latent phase genes,
of which LMP1 is significantly linked to the development of
lymphoma as an oncogenic protein (17).
To the best of the authors' knowledge, neither
miR-155 or LMP1 has been studied as a survival predictor for any
tumor. The two have differing expression levels in DLBCL, and are
associated with its development. Therefore, the present study aimed
to investigate whether the two molecules have an effect on patient
outcomes. Formalin-fixed and paraffin-embedded (FFPE) DLBCL samples
were collected at our center from May 2010 to April 2015, and the
levels of LMP1 and miR-155 were analyzed. The present study aimed
to evaluate the association between the data collected patients'
outcomes by univariate analysis and multivariate analysis. The
results showed that LMP1 and miR-155 had a significantly effect on
progression-free survival (PFS) and patient outcomes, and
highlighted two reliable biomarkers for the survival prediction of
DLBCL.
Materials and methods
Patients and tissue samples
The study population consisted of a retrospective
series of 197 de novo cases of DLBCL obtained from the
Affiliated Zhongda Hospital, Southeast University (Nanjing, China),
from May 2010 to December 2011. Patients were further selected
according to the following eligibility criteria: Diagnosis of
pathologically confirmed DLBCL; and treated with CHOP
(cyclophosphamide, vincristine, doxorubicin and prednisone) or a
CHOP-based regimen. FFPE tumor tissue biopsies were obtained prior
to treatment. Acquisition of the patient data was followed-up by
the Affiliated Zhongda Hospital, Southeast University, and the
samples underwent total RNA of total RNA extraction from FFPE.
Overall, 82 patients were analyzed in the current study, and data
regarding their clinical features and survival time were collected.
Survival time was calculated from the date of diagnosis to the date
of event. The date of event was defined as date of death in case of
OS, date of progression in case of PFS and right censoring (date of
last follow-up without the event). In all cases, the collection of
tissues and clinical data of patients was approved by the
Affiliated Zhongda Hospital, Southeast University institutional
review board. The experiment was undertaken with written informed
consent from each patient, and the study conformed with The Code of
Ethics of the World Medical Association (Declaration of Helsinki),
printed in the British Medical Journal (18 July 1964).
Total RNA extraction from FFPE
tissue
The FFPE tissue cores were used for total RNA
extraction using an RNAprep Pure FFPE kit (DP439; Tiangen Biotech,
Beijing, China) according to the manufacturer's protocol. Xylenes
(CAS: 1330-20-7; Macklin Co., Shanghai, China) and absolute ethyl
alcohol (CAS: 64-17-5; Macklin Co., Shanghai, China) were used to
dissolve the paraffin around the samples.
Microarray analysis
Sample preparation and microarray hybridization were
performed by Shanghai Biotechnology Corporation in China (for
details, please see 86-021-51320288, project no. BH150192). A total
of seven samples, including two of lymphadenitis, two of T cell
lymphoma, one of Hodgkin lymphoma and two of DLBCL, were selected
randomly for microarray analysis. The differential expression of
miRNAs was identified via fold-change filtering (fold-change ≥3.0
or ≤0.5) and standard Student's t-test (P<0.05). The microarray
data was calculated using Rstudio (3.3.2 for Windows).
Immunohistochemical (IHC)
analysis
An UltraSensitive S-P IHC kit (Maixin, Fuzhou,
China) was used for IHC staining, according to the manufacturer's
protocol. Sections (4 µm) were deparaffinized in a xylene bath for
5 min at room temperature twice, then subsequently incubated for 5
min in absolute, 95%, 85 and 70% ethyl alcohol, then washed with
PBS three times for 3 min. The antigen retrieval was performed by
incubating the sections in a 0.01 M citrate buffer (pH 6.0) for 20
min at 98°C and the sections were washed with PBS three times after
cooling down. Each section was then incubated with 50 µl
3,3′-diaminobenzidine working solution for 10 min at room
temperature, to develop peroxidase activity. A total of 50 µl
normal non-immune serum was used to block the nonspecific reaction
for each section. Following that, the sections were incubated with
primary antibody anti-LMP1 (1:100; Santa Cruz Biotechnology, Inc.,
Dallas, TX, USA) at 4°C overnight and washed with PBS three times,
prior to incubation with a secondary antibody for 30 min. The
sections were then incubated with streptavidin peroxidase solution
for 10 min for coloration, counterstained with hematoxylin and
mounted. Then, they were stained using a streptavidin peroxidase
system and the signal was visualized using diaminobenzidine
substrate.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR) for LMP1 and miR-155
quantification
For each tissue sample, 300 ng total RNA was
reverse-transcribed. HiScript II Q RT SuperMix for qPCR (+gDNA
wiper) (R223; Vazyme Biotech Co., Ltd., Nanjing, China) was used
for LMP1 reverse transcription, and HiScript Q Select RT SuperMix
for qPCR (+gDNA wiper) (R133; Vazyme Biotech Co., Ltd.) was used
for miR-155 reverse transcription, according to each manufacturer's
protocol. ChamQ SYBR qPCR Master Mix (Q311, Vazyme Biotech Co.,
Ldt.) was used to profile the expression of LMP1 and miR-155 in
lymphoid samples. The relative expression levels of mRNAs were
normalized to that of the internal control GAPDH for LMP1 and U6
for miR-155. The total RNA from a lymphadenitis tissue sample was
used as a control. The primers used were as follows: LMP1 forward,
5′-TGAGCAGGAGGGTGATCATC-3′ and reverse, 5′-CTATTCCTTTGCTCTCATGC-3′;
hsa-mir155-5p forward, 5′-TTAATGCTAATCGTGATAG-3′ and reverse,
5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACACCCCTA-3′; GAPDH
forward, 5′-CCATCACCATCTTCCAGGAG-3′ and reverse,
5′-ACAGTCTTCTGGGTGGCAGT-3′; U6 forward, 5′-CTCGCTTCGGCAGCACA-3′ and
reverse, 5′-AACGCTTCACGAATTTGCG-3′. The cycling conditions were
95°C for 30 sec, followed by 40 cycles of 95°C for 5 sec and 60°C
for 10 sec. The Cq value was obtained using ABI StepOne Software
(Life Technologies, Foster City, CA, USA). Relative mRNA levels
were calculated using Cq values, and corrected for GAPDH and U6
expression according to the equation 2−ΔΔCq (18).
Statistical analysis
Univariate survival analysis was performed using a
log-rank statistical test, while multivariate survival analysis was
performed using a Cox proportional hazard model, to estimate the
hazard ratio (HR) for the variables of interest and the 95%
confidence interval (CI) using SPSS software, version 19.0 (IBM,
Inc., Armonk, NY, USA). The Kaplan-Meier method was fitted for the
two groups with different biomarkers and the significance for
survival difference was assessed by log-rank test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Expression of LMP1 and miR-155 in
lymph node tissues
Data obtained from pathological tissues from 82
patients were available for the present study. Of these, two DLBCL
tissues were selected randomly for microarray analysis, while two
lymphadenitis tissues, two T cell lymphoma tissues and one Hodgkin
lymphoma tissue were used as controls and for contrast. A total of
2,550 miRNAs were tested at the initial time and 70 of them were
selected for further study according to their fold-change filtering
(fold-change ≥3.0 or ≤0.5) and the results of the standard
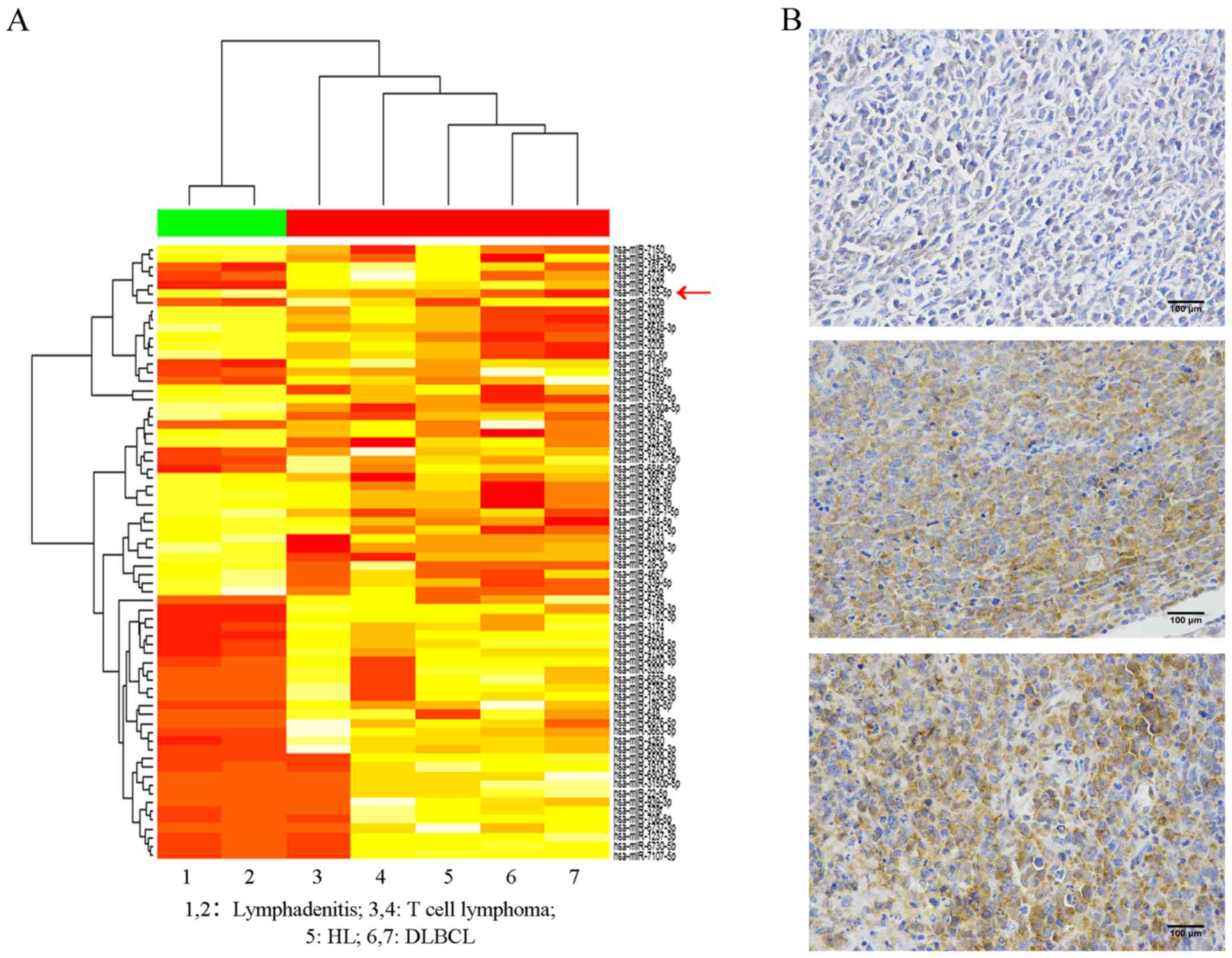
Student's t-test (P<0.05). As presented in Fig. 1A, following clustering analysis, a
marked difference was observed between lymphadenitis and lymphoma.
Various miRNAs had opposite expression trends in the five lymphoma
tissues, compared with the two lymphadenitis tissues, including
miR-155, which is labelled with a red arrow. The results revealed
that lymphadenitis tissues lacked expression of miR-155, whereas
high expression of miR-155 was observed in the samples of lymphoma,
and it was particularly high in DLBCL. Therefore, it may be
concluded that the increased expression of miR-155 distinguished
DLBCL from lymphadenitis and other types of lymphoma.
To assess the expression of LMP1, IHC analysis was
conducted for all samples. The results indicated that LMP1
exhibited various expression levels in the different samples
(Fig. 1B). Patient 1 was a male
patient who was 67 years old. He did not suffer from fever,
drenching sweats or weight loss at all. Lactic acid dehydrogenase
(LDL) levels in his serum remained normal. However, the lymphoma
cells invaded the colon. His Ann Arbor Stage was IV and IPI score
was 3. Therefore, he was willing to receive five rounds of
Rituximab-CHOP (RCHOP) chemotherapy and planned for auto-HSCT in
addition. Patient 2 was a 46 year-old male patient. He had B
symptoms of fever with a temperature >38°C and high LDH levels
in serum. In addition to this, the lymphoma cells invaded his liver
and spleen. His Ann Arbor Stage was IV and IPI score was 2.
Unfortunately, the patient did not receive therapy and died two
months later. Finally, Patient 3 was a 76 year-old female with EBV
(+). She had B symptoms of drenching sweats in addition to fever,
but a normal serum LDH level. However, she had extensive extranodal
problems in the stomach and pleura. Her Ann Arbor Stage was IV and
IPI score was 3. Although this patient was in a poorer condition
compared with patients 1 and 2, she exhibited a partial response
after five rounds of RCHOP chemotherapy. The IHC features of these
samples demonstrated that the patients who expressed LMP1 accounted
for 50% (41/82) of the total patients.
Clinical features of patients
The clinical characteristics according to the
expression of each biomarker are presented in Table I. Patients were categorized into
LMP1-positive and LMP1-negative expression groups (n=41 in each
group). However, miR-155 was highly expressed in all patients in
the present study. Considering that the variables did not follow a
normal distribution in this analysis, in order to evaluate the role
of high-expression miR-155 in DLBCL, the present study rearranged
the order of the patients according to the expression of miR-155;
the median of the patients was revealed (12-fold) and used to
divide them into two groups: the high group, which had an
expression of miR-155 12-fold lower or equal (n=42); and the
very-high group, which had an expression of miR-155 12-fold higher
(n=40). From these groups, we concluded that patients >60 years
of age accounted for 2/3 of this population, in addition to those
with serum LDH levels under or equal to the normal level. In
addition, >50% of the patients were at Stage III to IV or IPI
0-2, and most of them had extranodal extension including the
spleen, liver, bone marrow and other organs (Fig. 2).
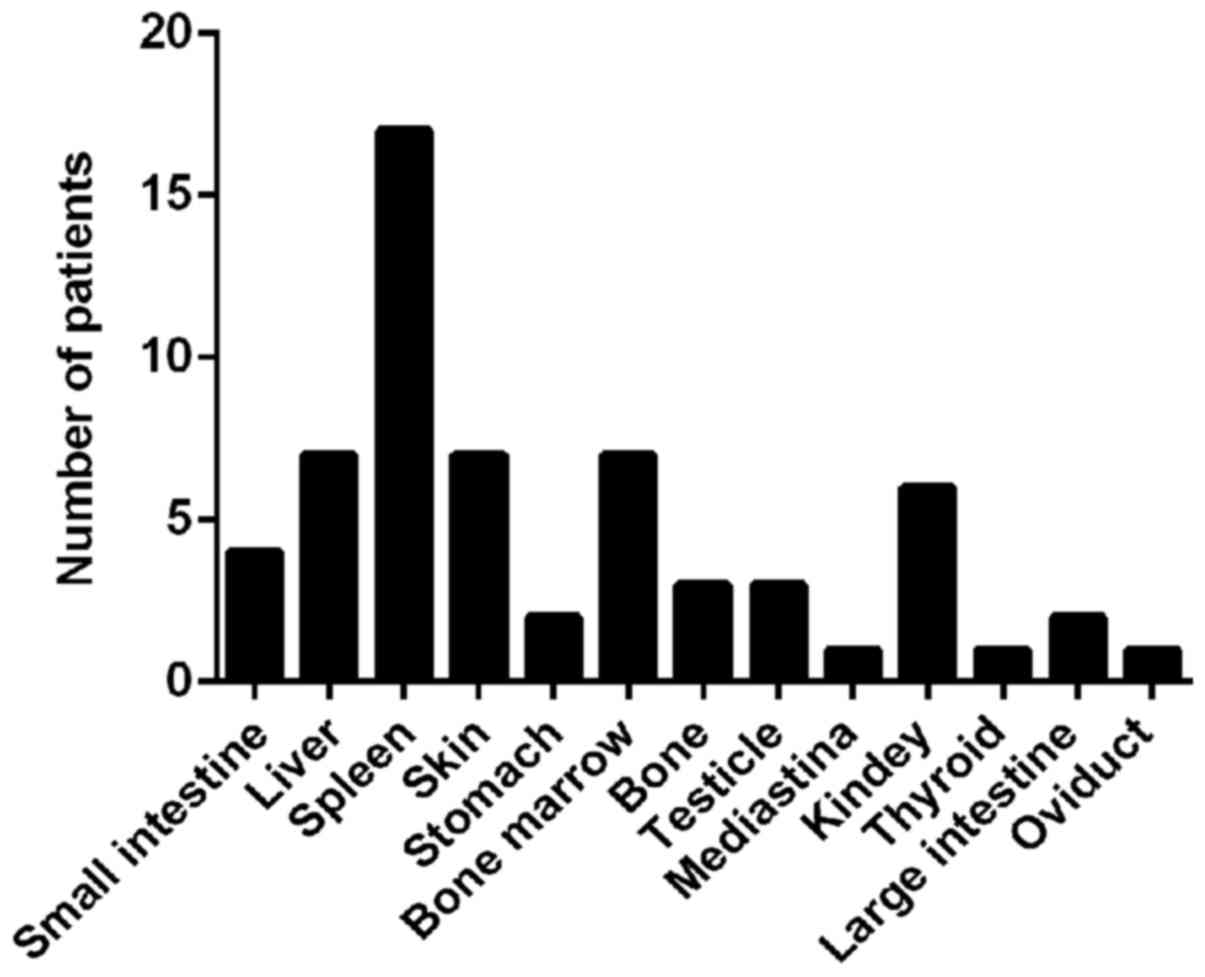 | Figure 2.Patients with extranodal extension of
organs. Small intestine, n=4; liver, n=7; spleen, n=17; skin, n=7;
stomach, n=2; bone marrow, n=7; bone, n=3; testicle, n=3;
mediastina, n=1; kidney, n=6; thyroid, n=1; large intestine, n=2;
oviduct, n=1. |
 | Table I.Clinical feature according to the
biomarkers. |
Table I.
Clinical feature according to the
biomarkers.
|
|
| LMP1 | miR-155∆ |
|---|
|
|
|
|
|
|---|
| Clinical feature | All patients n=82
(%) | Positive
(n=41) | Negative
(n=41) | High (n=42) | Very-high
(n=40) |
|---|
| Age at diagnosis, n
(%) |
|
|
|
|
|
|
≤60 | 27 (33) | 12 (29) | 15 (37) | 17 (40) | 10 (25) |
|
>60 | 55 (67) | 29 (71) | 26 (63) | 25 (60) | 30 (75) |
| Sex, n (%) |
|
|
|
|
|
|
Male | 48 (58) | 24 (59) | 24 (59) | 26 (62) | 22 (55) |
|
Female | 34 (42) | 17 (41) | 17 (41) | 16 (38) | 18 (45) |
| Serum LDH level, n
(%) |
|
|
|
|
|
| ≤200
U/l | 52 (63) | 27 (65) | 25 (61) | 26 (62) | 26 (65) |
| >200
U/l | 30 (37) | 14 (35) | 16 (39) | 16 (38) | 14 (35) |
| B symptoms, n
(%) |
|
|
|
|
|
|
Absent | 49 (59) | 24 (59) | 25 (61) | 24 (57) | 25 (63) |
|
Present | 33 (41) | 17 (41) | 16 (39) | 18 (43) | 15 (37) |
| Stage, n (%) |
|
|
|
|
|
| I | 17 (21) | 6 (15) | 11 (27) | 9 (21) | 8 (20) |
| II | 14 (17) | 7 (17) | 7 (17) | 7 (17) | 7 (17) |
|
III | 19 (23) | 11 (27) | 8 (19) | 16 (38) | 3 (8) |
| IV | 32 (39) | 17 (41) | 15 (37) | 10 (24) | 22 (55) |
| IPI, n (%) |
|
|
|
|
|
| 0 | 5 (6) | 0 (0) | 5 (12) | 3 (7) | 2 (5) |
| 1 | 18 (22) | 10 (24) | 8 (19) | 11 (26) | 7 (17) |
| 2 | 35 (43) | 21 (51) | 14 (35) | 18 (43) | 17 (43) |
| 3 | 14 (17) | 6 (15) | 8 (19) | 6 (14) | 8 (20) |
| 4 | 10 (12) | 4 (10) | 6 (15) | 4 (10) | 6 (15) |
| ENE, n (%) |
|
|
|
|
|
|
Yes | 45 (55) | 23 (56) | 22 (54) | 18 (43) | 27 (68) |
| No | 37 (45) | 18 (44) | 19 (46) | 24 (57) | 13 (32) |
| Rituximab, n
(%) |
|
|
|
|
|
|
Yes | 23 (28) | 8 (19) | 15 (37) | 17 (40) | 6 (15) |
| No | 59 (72) | 33 (81) | 26 (63) | 25 (60) | 34 (85) |
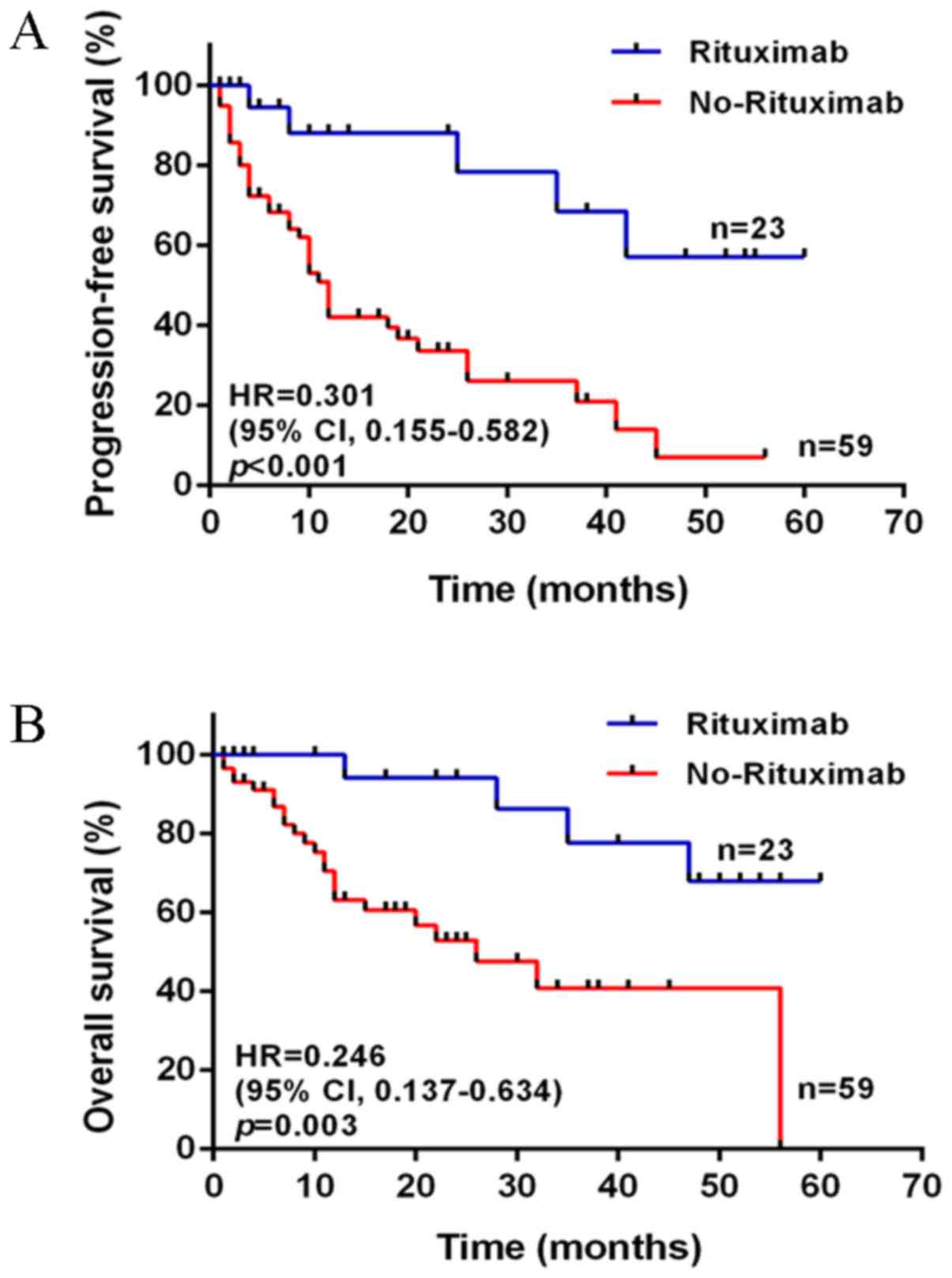
Furthermore, from Table
I, it was also observed that a number of patients involved in
the present study were treated with Rituximab, accounting for
nearly 30%; the others did not receive Rituximab treatment due to a
lack of financial support or other non-medical reasons. The
patients were separated into two groups: Rituximab (n=23) and
non-Rituximab (n=59). Following comparison of their PFS and overall
survival (OS), it was concluded that Rituximab markedly improved
the outcomes of patients, leading to a longer duration of
progression (Fig. 3).
Survival analysis according to
expression levels of LMP1 and miR-155
For the patients who were treated with the RCHOP
regimen, univariate log-rank analysis identified the significant
variables according to the following factors (all of the
P<0.05): IPI, LMP1 and miR-155 in PFS; LMP1 in OS (Table II). The median follow-up duration was
12 months (range, 1–60). The PFS was better in the IPI 0–2 group
compared with the IPI 3–4 group (HR, 0.200; 95% CI, 0.024–0.822;
P=0.034) in accordance with previous studies. Furthermore, PFS was
additionally influenced by the expression of LMP1 and miR-155. The
patients without LMP1 expression usually had a longer PFS and OS
duration compared with those who expressed LMP1 (PFS: HR, 0.110;
95% CI, 0.021–0.593; P=0.012; OS: HR, 0.144; 95% CI, 0.022–0.844;
P=0.037; Fig. 4A and B). However, the
results demonstrated that increased expression of miR-155 only had
an adverse effect on PFS (HR, 0.183; 95% CI, 0.021–0.770; P=0.026;
Fig. 4C), and was not a predictor of
OS (Fig. 4D).
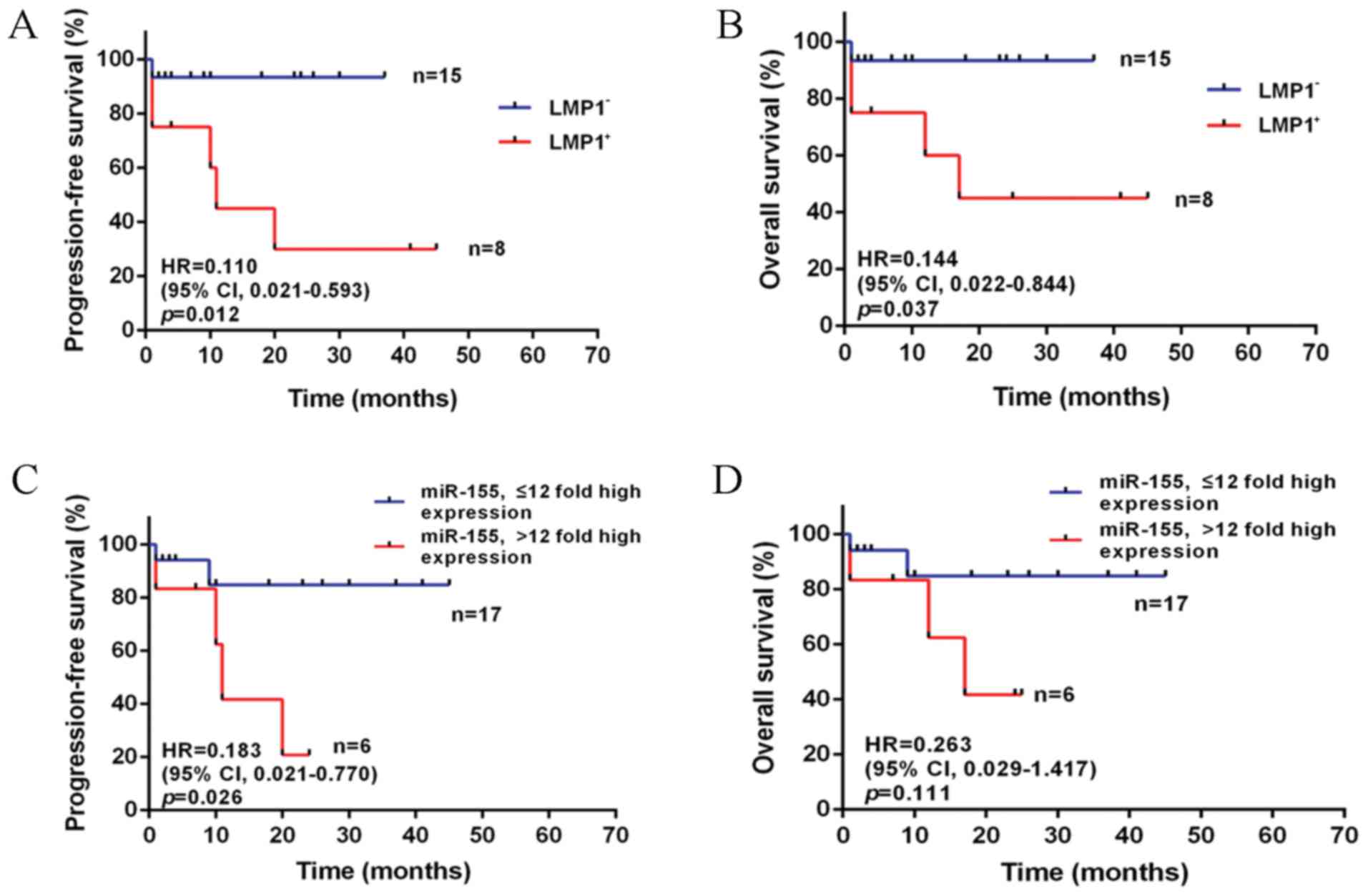 | Figure 4.PFS and OS of patients with lymphoma
treated with RCHOP according to the expression of LMP1 and miR-155.
(A) PFS and (B) OS by LMP1. The difference between patients with
LMP1+ (n=8) and LMP1- (n=15) was statistically significant in PFS
(P=0.012) and OS (P=0.037). (C) PFS and (D) OS by miR-155. The
difference between the group of high expression of miR-155 (≤12
fold, n=17) and the group of very high expression of miR-155
(>12 fold, n=6) was statistically significant in PFS (P=0.026);
however, not in OS (P=0.111). PFS, progression free survival; OS,
overall survival; HR, hazard ratio; CI, confidence interval; CHOP,
cyclophosphamide, vincristine, doxorubicin and prednisone; R,
Rituximab; miRNA/miR, microRNA; LMP-1, latent membrane protein
1. |
| Table II.Univariate analysis for PFS and OS in
diffuse large B cell lymphoma patients treated with RCHOP. |
Table II.
Univariate analysis for PFS and OS in
diffuse large B cell lymphoma patients treated with RCHOP.
|
| PFS | OS |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, ≤60/>60
years | 0.671 | 0.103–4.615 | 0.707 | 0.814 | 0.103–6.434 | 0.850 |
| Sex,
Male/Female | 0.759 | 0.148–3.750 | 0.728 | 1.155 | 0.199–6.816 | 0.871 |
| LDH, ≤200/>200
U/l | 0.449 | 0.043–2.713 | 0.326 | 1.001 | 0.112–8.950 | 0.999 |
| B symptom,
yes/no | 0.870 | 0.173–4.270 | 0.858 | 1.001 | 0.167–5.991 | 0.999 |
| Stage,
I–II/III–IV | 0.915 | 0.183–4.517 | 0.911 | 1.330 | 0.233–7.812 | 0.746 |
| IPI, 0–2/3-4 | 0.200 | 0.024–0.822 | 0.034a | 0.291 | 0.034–1.525 | 0.138 |
| ENE, yes/no | 1.403 | 0.284–7.289 | 0.669 | 2.098 | 0.376–13.16 | 0.392 |
| LMP1,
positive/negative | 0.110 | 0.021–0.593 | 0.012a | 0.144 | 0.022–0.844 | 0.037a |
| miR-155, ≤12/>12
fold high expression | 0.183 | 0.021–0.770 | 0.026a | 0.263 | 0.029–1.417 | 0.111 |
As presented in Table
III, for the patients who were treated with a CHOP regimen
lacking Rituximab, IPI was identified as a predictive factor only
for OS (HR, 0.211; 95% CI, 0.085–0.461; P<0.001), but not PFS,
by univariate log-rank analysis. The effect of LMP1 and miR-155 on
PFS and OS remained the same as that of Rituximab treatment (PFS,
LMP1: HR, 0.341; 95% CI, 0.175–0.634; P=0.001; OS, LMP1: HR, 0.317;
95% CI, 0.156–0.803; P=0.015; PFS, miR-155: HR, 0.503; 95% CI,
0.261–0.951; P=0.043; OS, miR-155: HR, 0.409; 95% CI, 0.190–0.977;
P=0.048; Fig. 5). The median
follow-up duration was 13 months (range, 1–60).
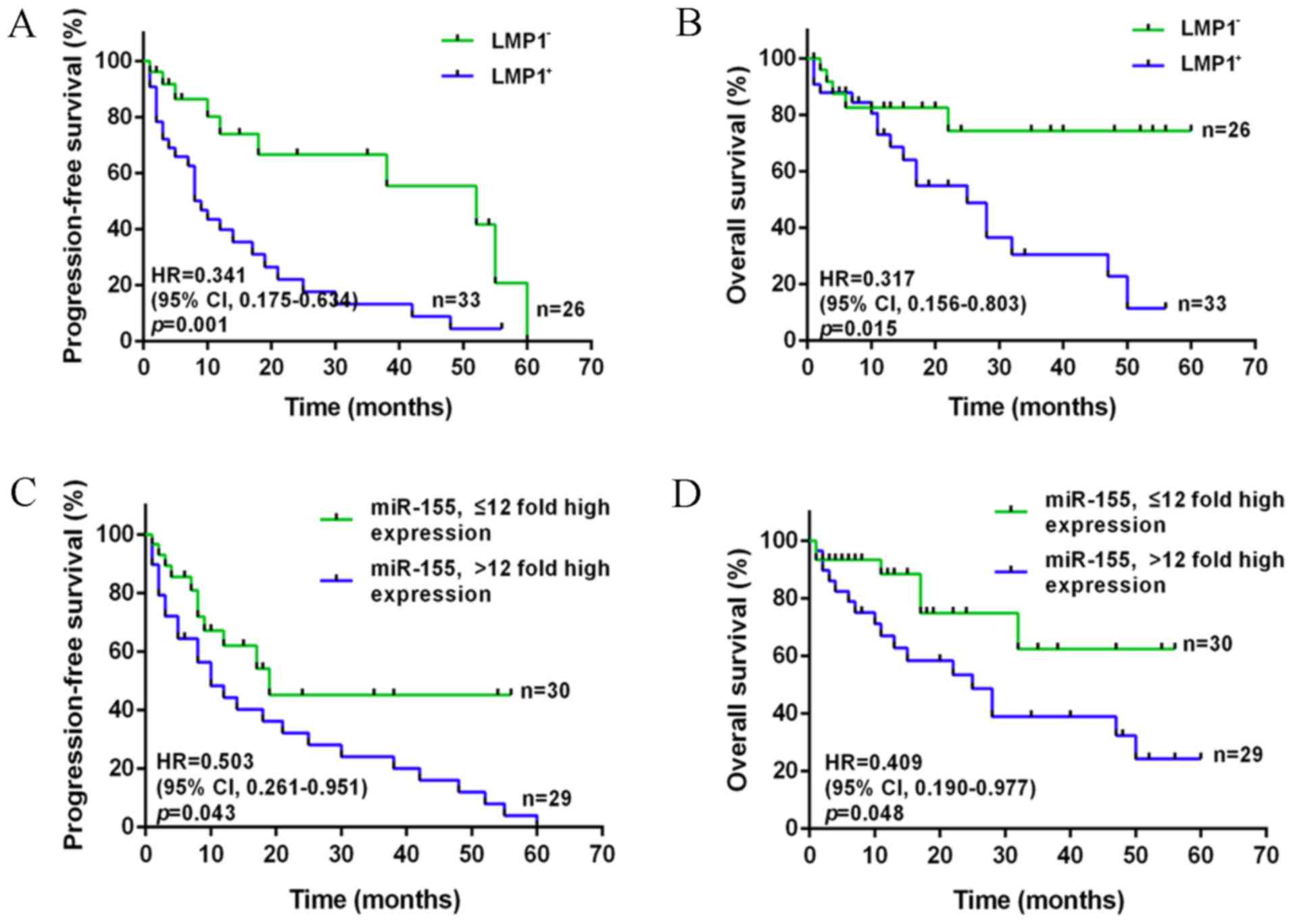 | Figure 5.PFS and OS of patients with lymphoma
treated with CHOP according to the expression of LMP1 and miR-155.
(A) PFS and (B) OS by LMP1. The difference between patients with
LMP1+ (n=33) and LMP1- (n=26) was statistically significant in PFS
(P=0.001) and OS (P=0.015). (C) PFS and (D) OS by miR-155. The
difference between the group of high expression of miR-155 (≤12
fold, n=30) and the group of very high expression of miR-155
(>12 fold, n=29) was statistically significant in PFS (P=0.043)
and OS (P=0.048). PFS, progression free survival; OS, overall
survival; CHOP, cyclophosphamide, vincristine, doxorubicin and
prednisone; miRNA/miR, microRNA; HR, hazard ratio; CI, confidence
interval; LMP-1, latent membrane protein 1. |
| Table III.Univariate analysis for PFS and OS in
diffuse large B cell lymphoma patients treated with CHOP. |
Table III.
Univariate analysis for PFS and OS in
diffuse large B cell lymphoma patients treated with CHOP.
|
| PFS | OS |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, ≤60/>60
years | 0.802 | 0.412–1.562 | 0.528 | 0.410 | 0.196–1.037 | 0.065 |
| Sex, M/F | 1.278 | 0.672–2.494 | 0.458 | 1.731 | 0.744–3.875 | 0.215 |
| LDH, ≤200/>200
U/l | 1.063 | 0.553–2.069 | 0.849 | 0.761 | 0.321–1.744 | 0.508 |
| B symptom,
yes/no | 0.720 | 0.364–1.338 | 0.308 | 0.716 | 0.288–1.671 | 0.423 |
| Stage,
I–II/III–IV | 0.861 | 0.442–1.637 | 0.644 | 0.873 | 0.376–2.024 | 0.753 |
| IPI, 0–2/3–4 | 0.647 | 0.310–1.193 | 0.165 | 0.211 | 0.085–0.461 |
<0.001b |
| ENE, yes/no | 0.608 | 0.309–1.123 | 0.120 | 0.688 | 0.302–1.552 | 0.372 |
| LMP1,
positive/negative | 0.341 | 0.175–0.634 | 0.001b | 0.317 | 0.156–0.803 | 0.015a |
| miR-155, ≤12/>12
fold high expression | 0.503 | 0.261–0.951 | 0.043a | 0.409 | 0.190–0.977 | 0.048a |
According to the results of the multivariate
analysis, LMP1 and miR-155 were independent factors for PFS (LMP1:
HR, 0.165; 95% CI, 0.063–0.435; P<0.001; miR-155: HR, 0.415; 95%
CI, 0.193–0.891; P=0.024; Table IV),
and IPI and LMP1 for OS (IPI: HR, 0.311; 95% CI, 0.113–0.856,
P=0.024; LMP1: HR, 0.208; 95% CI, 0.064–0.673; P= P0.009; Table IV). It was demonstrated that only
LMP1 was a stable predictor for PFS and OS.
| Table IV.Multivariate analysis for PFS and OS
in patients with diffuse large B cell lymphoma patients. |
Table IV.
Multivariate analysis for PFS and OS
in patients with diffuse large B cell lymphoma patients.
|
| PFS | OS |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, ≤60/>60
years | 1.529 | 0.586–3.984 | 0.385 | 1.432 | 0.428–4.797 | 0.560 |
| Sex, M/F | 0.908 | 0.443–1.859 | 0.791 | 0.521 | 0.192–1.415 | 0.201 |
| LDH, ≤200/>200
U/l | 0.583 | 0.256–1.330 | 0.200 | 0.405 | 0.140–1.171 | 0.095 |
| B symptom,
yes/no | 1.081 | 0.451–2.591 | 0.861 | 1.077 | 0.373–3.108 | 0.890 |
| Stage,
I–II/III–IV | 2.130 | 0.922–4.922 | 0.077 | 2.043 | 0.784–5.320 | 0.144 |
| IPI, 0–2/3–4 | 0.719 | 0.333–1.550 | 0.400 | 0.311 | 0.113–0.856 | 0.024a |
| ENE, yes/no | 0.979 | 0.473–2.027 | 0.954 | 0.877 | 0.441–2.611 | 0.877 |
| LMP1,
positive/negative | 0.165 | 0.063–0.435 |
<0.001c | 0.208 | 0.064–0.673 | 0.009b |
| miR-155, ≤12/>12
fold high expression | 0.415 | 0.193–0.891 | 0.024a | 0.445 | 0.174–1.136 | 0.090 |
Discussion
The results of the present study demonstrated that
the expression of LMP1 was an independent factor for both PFS and
OS, whereas miR-155 was significantly associated with PFS. IPI was
a predictor for OS in newly diagnosed DLBCL patients, whether they
received Rituximab therapy or not. Excluding the influence of other
clinical factors, IPI was able to predict the PFS of the patients
who were treated with RCHOP, and the OS of the patients who were
only treated with CHOP without Rituximab. Furthermore, miR-155 had
differing roles in OS according to Rituximab, and the effect of
miR-155 on OS was observed in the group of patients treated with
Rituximab. Just like it was considered as an independent factor for
OS of DLBCL patients. Therefore, it may be concluded that Rituximab
resulted in the varied role of IPI and miR-155 in predicting
patient outcomes. In the era of Rituximab, the assessment of
therapy and prognosis has become a complex procedure. Therefore, in
combination with clinical features, biomarkers will play an
important role in the prediction of patient outcomes.
Previous studies have presented a variety of
conclusions regarding which clinical factors truly affect patient
outcomes, with various contradictions among them (19,20). IPI,
the only globally used prognostic indicator in B cell lymphoma, was
verified to be associated with OS. However, in the Rituximab era,
it has failed to predict prognosis in a considerable proportion of
patients with B cell lymphoma (21).
Therefore, biomarkers seem to be more reliable in evaluating
survival along with clinical features. Various factors have
previously been identified to alter patient outcomes, including
gene mutations in B cell lymphoma-2, MYC, TP53 (22–24), the
regulation of miRNAs including miR-155, miR-21 and miR-124
(25–27), and the expression of virus-infected
relative genes (28,29). Accumulating evidence has revealed that
the expression of miR-155 may be a key biomarker in the development
of lymphoma (25). miR-155-5p was
also observed to be increased in Hodgkin's lymphoma, and
contributed to development of the disease (30). Additionally, in indolent primary
cutaneous B-cell lymphoma, Monsálvez et al (31) evaluated the association between
miR-155 expression and PFS (31).
In addition to miRNAs, the expression of LMP1, which
results from EBV infection, may induce the development of lymphoma
(32,33). The prognostic value of LMP1 remains
controversial, as the majority of studies are limited to a small
number of recruited patients. In 2012, a study including 16
extranodal natural killer (NK)/T-cell lymphoma (ENKTL) patients
demonstrated that LMP1 exhibited a significant correlation with
patient OS, thus LMP1 may be a prognostic indicator of survival in
lymphoma patients (34). Furthermore,
Bi et al (35) indicated that
LMP1 upregulated PD-L1 through the nuclear factor-κB pathway
(induced by EBV), and this was associated with the poor prognosis
of lymphoma. This result suggested that LMP1 may act as a
prognostic predictor.
Notably, these studies presented a partial
association as they focused primarily on the mechanisms regarding
LMP1 and miR-155 functioning in the process of lymphoma
development. Hence, in order to evaluate the effect of these
biomarkers on prognosis, further data from patients should be
recruited and evaluated. The present retrospective analysis was
designed to collect information from DLBCL patients and give a
general conclusion regarding the association between particular
biomarkers and patient survival outcomes. The results verified that
the expression levels of LMP1 and miR-155 were associated with poor
prognosis of patients, indicating these two biomarkers as efficient
predictors of PFS and OS, supported by their oncogenic
functions.
The present study demonstrated the favorable impact
and clinical value of LMP1 and miR-155 expression on the PFS and OS
of patients with newly diagnosed lymphoma, suggesting that LMP1 and
miR-155 should be analyzed to evaluate patient prognosis as
integral biomarkers. The limitations of the present study included
the relatively small number of patients included and the lack of
available data on the EBV-DNA in cells. Furthermore, the expression
of LMP1 was based on EBV infection, whereas not all EBV infected
lymphomas would induce LMP1. In addition, in China there are
different and more aggressive LMP1 variants, which may occur due to
genetic polymorphisms of the LMP1 oncogene. Specific sets of point
mutations I124 V/I152L and F144I/D150A/L151, associated with high
nuclear factor-kB activation, may occur (36), as well as the presence of 30 and 69 bp
deletions (37). The genetic
polymorphisms of the LMP1 oncogene were not analyzed here. These
should be considered in an in-depth analysis of the exact function
of LMP1 in DLBCL in the future. The prognostic values of LMP1
expression appear to be more sensitive and accurate and after more
patients are enrolled in the future studies, a comparison between
EBV and LMP1 may be performed. Samples will also be collected
samples from other places, making it a multiple center study, in
order to obtain a more reliable result.
Acknowledgements
Not applicable.
Funding
The present study was supported by The National
Natural Science Foundation of China (grant no. 81370673), Key
Medical Subjects of Jiangsu Province (grant no. BL2014078), Key
Discipline of Jiangsu Province (2016–2020) and and Jiangsu
Provincial Medical Youth Talent (grant no. QNRC2016812).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XW and FW collected the patient data associated with
hematological disease. XW and YL analyzed the microarray data. XW
and XYW collected the FFPE samples, performed the histological
examination and analyzed the data. PL, ZG and XPZ conducted the
statistical analysis. BC contributed to the conception and design
of the study, and gave final approval for the manuscript to be
published. CG performed the collection of patient information, and
HJZ assisted with the IHC analysis. BC, CG and HJZ were responsible
for revising the manuscript. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The present study was undertaken with written
informed consent from each patient, and the collection of tissues
and clinical data of patients was approved by the Affiliated
Zhongda Hospital, Southeast University institutional review
board.
Consent for publication
The patient provided written informed consent for
the publication of any associated data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Westin JR, McLaughlin P, Romaguera J,
Hagemeister FB, Pro B, Dang NH, Samaniego F, Rodriguez MA, Fayad L,
Oki Y, et al: Paclitaxel, topotecan and rituximab: Long term
outcomes of an effective salvage programme for relapsed or
refractory aggressive B-cell non-Hodgkin lymphoma. Br J Haematol.
167:177–184. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lee GW, Go SI, Kim SH, Hong J, Kim YR, Oh
S, Kim SY, Do YR, Lee H, Lee SI, et al: Clinical outcome and
prognosis of patients with primary sinonasal tract diffuse large
B-cell lymphoma treated with rituximab-cyclophosphamide,
doxorubicin, vincristine and prednisone chemotherapy: A study by
the Consortium for Improving Survival of Lymphoma. Leuk Lymphoma.
56:1020–1026. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Park JH, Yoon DH, Kim DY, Kim S, Seo S,
Jeong Y, Lee SW, Park CS, Huh J and Suh C: The highest prognostic
impact of LDH among international prognostic indices (IPIs): An
explorative study of five IPI factors among patients with DLBCL in
the era of rituximab. Ann Hematol. 93:1755–1764. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cohen JB, Behera M, Thompson CA and
Flowers CR: Evaluating surveillance imaging for diffuse large
B-cell lymphoma and Hodgkin lymphoma. Blood. 129:561–564. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jones K, Nourse JP, Keane C, Bhatnagar A
and Gandhi MK: Plasma microRNA are disease response biomarkers in
classical Hodgkin lymphoma. Clin Cancer Res. 20:253–264. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Eis PS, Tam W, Sun L, Chadburn A, Li Z,
Gomez MF, Lund E and Dahlberg JE: Accumulation of miR-155 and BIC
RNA in human B cell lymphomas. Proc Natl Acad Sci USA.
102:3627–3632. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Iqbal J, Shen Y, Huang X, Liu Y, Wake L,
Liu C, Deffenbacher K, Lachel CM, Wang C, Rohr J, et al: Global
microRNA expression profiling uncovers molecular markers for
classification and prognosis in aggressive B-cell lymphoma. Blood.
125:1137–1145. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gracias DT, Stelekati E, Hope JL,
Boesteanu AC, Doering TA, Norton J, Mueller YM, Fraietta JA, Wherry
EJ, Turner M and Katsikis PD: The microRNA miR-155 controls CD8(+)
T cell responses by regulating interferon signaling. Nat Immunol.
14:593–602. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Huskova H, Korecka K, Karban J, Vargova J,
Vargova K, Dusilkova N, Trneny M and Stopka T: Oncogenic
microRNA-155 and its target PU.1: An integrative gene expression
study in six of the most prevalent lymphomas. Int J Hematol.
102:441–450. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zeng Q, Tao X, Huang F, Wu T, Wang J,
Jiang X, Kuang Z and Cheng B: Overexpression of miR-155 promotes
the proliferation and invasion of oral squamous carcinoma cells by
regulating BCL6/cyclin D2. Int J Mol Med. 37:1274–1280. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lv L, An X, Li H and Ma L: Effect of
miR-155 knockdown on the reversal of doxorubicin resistance in
human lung cancer A549/dox cells. Oncol Lett. 11:1161–1166. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
McLaughlin LP, Gottschalk S, Rooney CM and
Bollard CM: EBV-directed T cell therapeutics for EBV-associated
lymphomas. Methods Mol Biol. 1532:255–265. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Roy Ghosh S, Robertson ES and Saha A:
Epigenetic Impact on EBV Associated B-Cell Lymphomagenesis.
Biomolecules. 6:pii: E46. 2016.
|
|
15
|
Mackrides N, Campuzano-Zuluaga G,
Maque-Acosta Y, Moul A, Hijazi N, Ikpatt FO, Levy R, Verdun RE,
Kunkalla K, Natkunam Y, et al: Epstein-Barr virus-positive
follicular lymphoma. Mod Pathol. 30:519–529. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Raab-Traub N: EBV-induced oncogenesisHuman
Herpesviruses: Biology, Therapy and Immunoprophylaxis. Arvin A,
Campadelli-Fiume G, Mocarski E, Moore PS, Roizman B, Whitley R and
Yamanishi K: Cambridge University Press 2007; Cambridge: 2007,
View Article : Google Scholar
|
|
17
|
Huang YC, Lin SJ, Lin KM, Chou YC, Lin CW,
Yu SC, Chen CL, Shen TL, Chen CK, Lu J, et al: Regulation of EBV
LMP1-triggered EphA4 downregulation in EBV-associated B lymphoma
and its impact on patients' survival. Blood. 128:1578–1589. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shen Y, Zhang R, Liu L, Shen Y, Song W, Qi
T, Tang Y, Wang Z, Guan L and Lu H: Clinical and prognostic
analysis of 78 patients with human immuno-deficiency virus
associated non-Hodgkin's lymphoma in Chinese population. Infect
Agent Cancer. 12:72017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mukhtar F, Boffetta P, Risch HA, Park JY,
Bubu OM, Womack L, Tran TV, Zgibor JC and Luu HN: Survival
predictors of Burkitt's lymphoma in children, adults and elderly in
the United States during 2000–2013. Int J Cancer. 140:1494–1502.
2016. View Article : Google Scholar
|
|
21
|
Öztürk E, Özbalak M, Berk S, Erdoğan I,
Avşar E, Dolgun A, Çetiner M, Mandel NM, Yalnız FF, Elverdi T, et
al: Comparison of international prognostic index and NCCN-IPI in
324 patients with de novo diffuse large B-cell lymphoma: A
multi-center retrospective analysis. Leuk Lymphoma. 57:1211–1214.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sesques P and Johnson NA: Approach to the
diagnosis and treatment of high-grade B-cell lymphomas with MYC and
BCL2 and/or BCL6 rearrangements. Blood. 129:280–288. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cao Y, Zhu T, Zhang P, Xiao M, Yi S, Yang
Y, Li Q, Ling S, Wang Y, Gao L, et al: Mutations or copy number
losses of CD58 and TP53 genes in diffuse large B cell lymphoma are
independent unfavorable prognostic factors. Oncotarget.
7:83294–83307. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zamani-Ahmadmahmudi M, Aghasharif S and
Ilbeigi K: Prognostic efficacy of the human B-cell lymphoma
prognostic genes in predicting disease-free survival (DFS) in the
canine counterpart. BMC Vet Res. 13:172017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Due H, Svendsen P, Bodker JS, Schmitz A,
Bøgsted M, Johnsen HE, El-Galaly TC, Roug AS and Dybkær K: miR-155
as a Biomarker in B-Cell Malignancies. Biomed Res Int.
2016:95130372016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li J, Fu R, Yang L and Tu W: miR-21
expression predicts prognosis in diffuse large B-cell lymphoma. Int
J Clin Exp Pathol. 8:15019–15024. 2015.PubMed/NCBI
|
|
27
|
Jeong D, Kim J, Nam J, Sun H, Lee YH, Lee
TJ, Aguiar RC and Kim SW: MicroRNA-124 links p53 to the NF-κB
pathway in B-cell lymphomas. Leukemia. 29:1868–1874. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chang KC, Chen PC, Chang Y, Wu YH, Chen
YP, Lai CH, Medeiros LJ, Su IJ and Wang HW: Epstein-Barr virus
latent membrane protein-1 up-regulates cytokines and correlates
with older age and poorer prognosis in Hodgkin lymphoma.
Histopathology. 70:442–455. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Olszewski AJ, Fallah J and Castillo JJ:
Human immunodeficiency virus-associated lymphomas in the
antiretroviral therapy era: Analysis of the National Cancer Data
Base. Cancer. 122:2689–2697. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Paydas S, Acikalin A, Ergin M, Celik H,
Yavuz B and Tanriverdi K: Micro-RNA (miRNA) profile in Hodgkin
lymphoma: Association between clinical and pathological variables.
Med Oncol. 33:342016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Monsálvez V, Montes-Moreno S, Artiga MJ,
Rodríguez ME, Sanchez-Espiridion B, Lozano M, Fernández-de-Misa R,
Rodríguez-Peralto JL, Piris MA and Ortíz-Romero PL: MicroRNAs as
prognostic markers in indolent primary cutaneous B-cell lymphoma.
Mod Pathol. 26:171–181. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lajoie V, Lemieux B, Sawan B,
Lichtensztejn D, Lichtensztejn Z, Wellinger R, Mai S and Knecht H:
LMP1 mediates multinuclearity through downregulation of shelterin
proteins and formation of telomeric aggregates. Blood.
125:2101–2110. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bollard CM, Gottschalk S, Torrano V, Diouf
O, Ku S, Hazrat Y, Carrum G, Ramos C, Fayad L, Shpall EJ, et al:
Sustained complete responses in patients with lymphoma receiving
autologous cytotoxic T lymphocytes targeting Epstein-Barr virus
latent membrane proteins. J Clin Oncol. 32:798–808. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Mao Y, Zhang DW, Zhu H, Lin H, Xiong L,
Cao Q, Liu Y, Li QD, Xu JR, Xu LF and Chen RJ: LMP1 and LMP2A are
potential prognostic markers of extranodal NK/T-cell lymphoma,
nasal type (ENKTL). Diagn Pathol. 7:1782012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bi XW, Wang H, Zhang WW, Wang JH, Liu WJ,
Xia ZJ, Huang HQ, Jiang WQ, Zhang YJ and Wang L: PD-L1 is
upregulated by EBV-driven LMP1 through NF-κB pathway and correlates
with poor prognosis in natural killer/T-cell lymphoma. J Hematol
Oncol. 9:1092016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zuercher E, Butticaz C, Wyniger J,
Martinez R, Battegay M, El Amari Boffi E, Dang T, Egger JF, Fehr J,
Mueller-Garamvögyi E, et al: Genetic diversity of EBV-encoded LMP1
in the Swiss HIV Cohort Study and implication for NF-Κb activation.
PLoS One. 7:e321682012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Knecht H, Berger C, Rothenberger S,
Odermatt BF and Brousset P: The role of Epstein-Barr virus in
neoplastic transformation. Oncology. 60:289–302. 2001. View Article : Google Scholar : PubMed/NCBI
|