Introduction
Chordomas are rare malignant tumors exhibiting
notochordal differentiation (1). The
most common sites of tumor development include the sacrococcygeal
region (50–60%), spheno-occipital region (25–35%) and mobile spine
(15%) (2). Lesions of the cervical
spine are rare, comprising between 3 and 7% of all chordomas, and
between 20 and 50% of spinal chordomas (3). Lesions of the cervical spine are often
overlooked as a diagnostic possibility in patients with neck pain
or mass. The present study retrospectively reviewed the computed
tomography (CT) and magnetic resonance imaging (MRI) results of 11
patients with chordoma of the cervical spine in an effort to
evaluate the typical imaging features of these unusual lesions and
to facilitate improved differential diagnosis from other
lesions.
Materials and methods
Patients
The present study was approved by the Institutional
Review board of the Affiliated Hospital of Qingdao University. From
between July 2008 and 2016, 11 cases of histologically proven
cervical chordomas were selected and retrospectively reviewed.
Pathological and clinical information including age at presentation
and sex was also recorded.
Imaging techniques
CT scans were obtained using a standard CT protocol
for the spine with multi-detector spiral CT scanner (LightSpeed;
General Electric Healthcare Corporation, Waukesha, WI, USA). Scan
type was helical (pitch/speed, 1.375:1, 13.75 mm). CT sections were
imaged at 2.5 mm thickness with 2.5 mm space. MRI examinations were
performed using a 3.0T magnetic resonance scanner (Signa HDx; GE
Medical Systems Ltd., Little Chalfont, UK). Pre-contrast
T1-weighted spin-echo images with and without fat saturation, and
T2-weighted fast spin-echo images, and short T1 inversion recovery
were obtained, followed by post-contrast T1-weighted spin-echo
images with fat saturation following intravenous injection of 0.1
mmol/kg gadolinium dimeglumine. Images were obtained in at least
two planes with 3 mm section thickness and 1 mm intersection
gap.
Imaging analysis
CT and MRI studies were evaluated by two experienced
radiologists using an image archiving and communication system, and
results were determined by consensus. The following parameters were
evaluated: Location of spine involvement, extension of soft tissue
mass (anteriorly, laterally or posteriorly towards vertebrae),
morphology (uni-lobular, multi-lobular or collar button),
enlargement of transverse and intervertebral foramina, arterial
encasement, disk involvement, bone destruction, status of cortical
bone, periosteal reaction, attenuation and the presence of
calcification by CT, signal intensity and enhancement pattern by
MRI. Artery encasement was defined as circumferential contact of
tumor with vessel >270°. The CT density was rated as hypodense,
isodense or hyperdense compared with adjacent muscle. MRI signal
intensity (SI) for the available sequences was compared with that
of spinal cord and fat on T1-weighted images, with that of spinal
cord and cerebrospinal fluid (CSF) on T2-weighted images. On
T1-weighted images, it was classified as hypointense (SI<spinal
cord), intermediate (spinal cord≤SI<fat) or hyperintense
(SI=fat). On T2-weighted images, it was classified as hypointense
(SI<spinal cord), intermediate (spinal cord≤SI<CSF),
hyperintense (SI=CSF). The presence of hypointense septa was
evaluated on T2-weighted images. On post-contrast MRI images, the
degree of enhancement was subjectively assessed as mild enhancement
(less than or equal to that of muscle) or marked enhancement
(greater than that of muscle). The patterns of contrast enhancement
were also recorded.
Results
There were 5 female and 6 male patients. The
patients' ages ranged from between 15 and 75 years, with a mean age
of 45.3 years and a median age of 48 years. Overall, the males
(mean, 50.8 years; range, 18–64 years) were older than the females
(mean, 44.5 years; range, 15–51 years). Tumors were identified from
level of the C1 vertebra to C6. Vertebral body involvement was
limited to a single level in 5 patients and were multi-level in 5
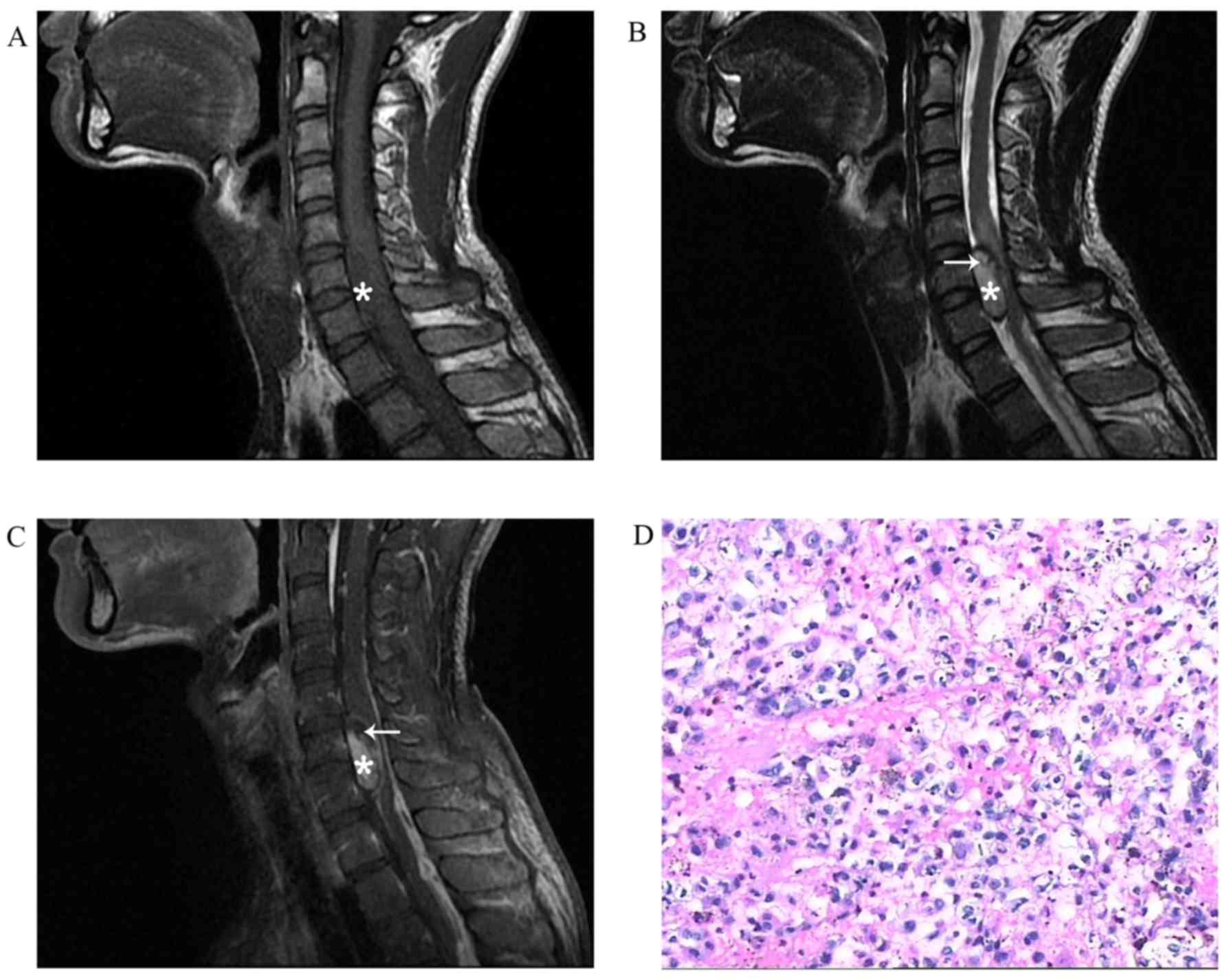
patients. Only 1 patient did not exhibit any vertebral body
involvement, exhibiting only a uni-lobular intradural soft tissue
mass (Fig. 1). Of the 10 patients
with vertebral involvement, 9 exhibited soft tissue masses extended
from adjacent vertebrae and 1 did not reveal any soft tissue mass.
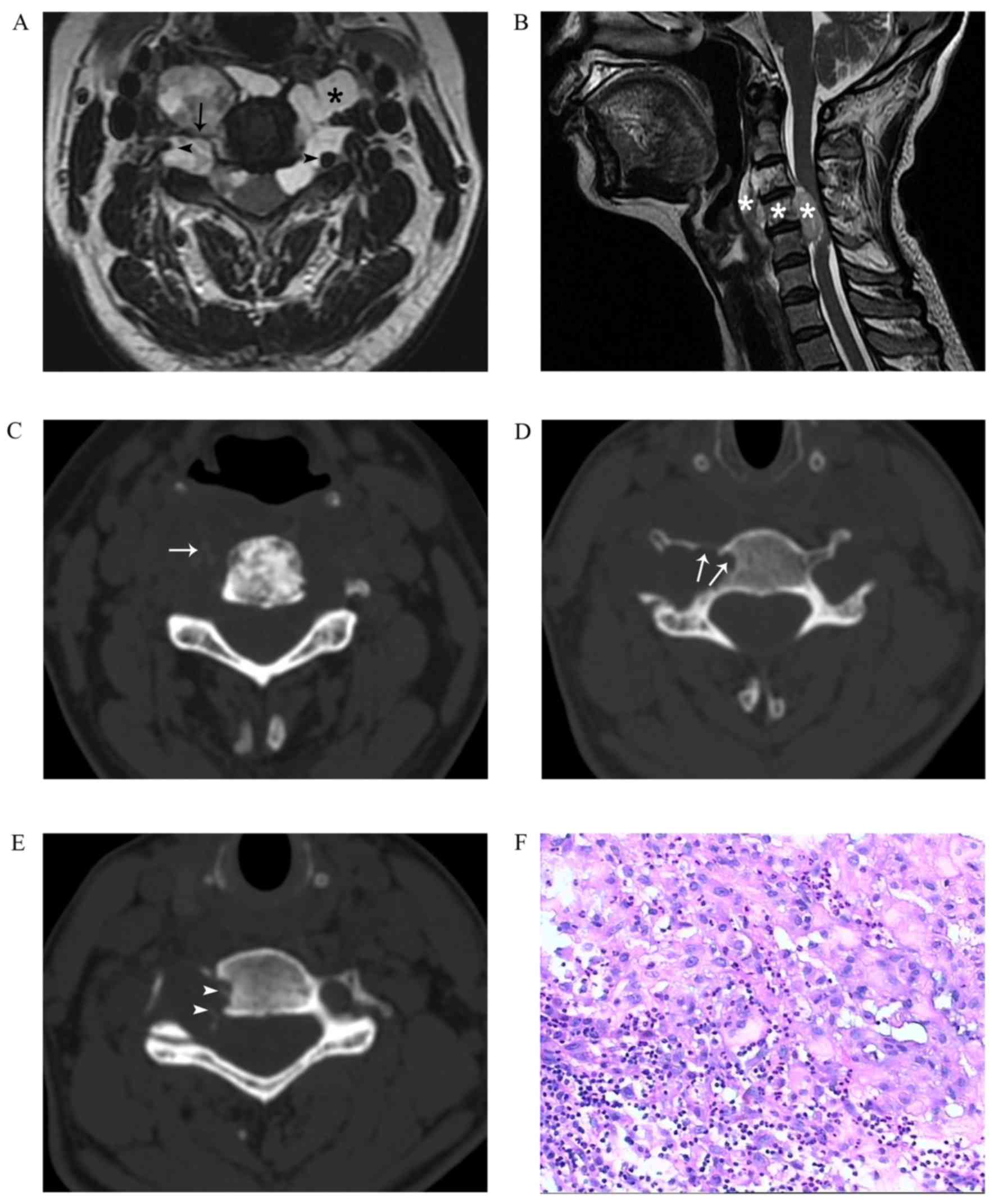
The soft tissue masses occurred anteriorly, laterally and
posteriorly (n=5); anteriorly and laterally (n=3); and laterally
and posteriorly (n=1) towards vertebrae in the axial plane
(Fig. 2A). All 9 cases exhibited a
multi-lobular soft tissue component which extended over the
vertebrae involved and revealed a collar button appearance in the
sagittal plane (Fig. 2B). Widening of
the transverse foramen and intervertebral foramina was produced in
7 patients, and widening of only the transverse foramen in 2
patients. The vertebral artery was encased in 7 cases (Fig. 2A). Intervertebral disks were not
affected in any of the cases.
Of the 7 cases with CT scans available, 6 revealed
lytic-sclerotic bone destruction, 1 without distinct vertebral
destruction. The feature of lytic-sclerotic bone destruction was
similar to the melting ice or sequestrum within osteomyelitis
(Fig. 2C). A total of 5 cases
exhibited pressure erosion of the outer cortex (Fig. 2D), 3 of which had spiculated
periosteal reaction (Fig. 2E).
Pressure erosion is bone remodeling by a mass outside the bone. A
total of 2 cases exhibited compression fractures. Calcification was
demonstrated in 3/7 cases (Fig. 2C).
All cases were heterogeneous and hypodense compared with adjacent
muscle.
Of 10 cases with pre-contrast MRI images available,
tumors were hypointense (n=6) or isointense (n=4) on T1-weighted
images (Fig. 1A). Tumors were
revealed to be hyperintense (n=5), intermediate (n=2) or
intermediate-hyperintense (n=3) on T2-weighted images (Figs. 1B, 2A and
B). Hypointense septa between lobules (n=5) and stripes in
cases (n=3) were observed on the T2-weighted images (Fig. 2A). Of the 6 cases with post-contrast
MRI images, 3 cases were heterogeneous and 3 cases exhibited
ring-like enhancement (Fig. 1C).
The pathological results of all cases revealed a
typical histological pattern of large cells with copious vacuolated
cytoplasm separated by fibrous septa into lobules (Figs. 1D and 2F).
Discussion
Chordomas are considered to be aggressive, albeit
slow growing, invasive and locally destructive (4). It has been hypothesized that chordomas
arise from embryonic remnants of the primitive notochord (5). The tumor degenerates and disappears
where it is surrounded by the vertebral bodies, but persists as the
nucleus pulposus of each intervertebral disk. Remnants of the
notochord may give rise to chordoma and usually remain in or close
to the midline, entrapped within bone (5). However, there are a number of reports
that chordoma may develop from a benign notochordal cell tumor
(6–9).
The tumor may occur at any age, but is usually observed in the
fifth to seventh decades of life with male predilection (1).
Spinal chordomas typically develop within the
vertebral body, primarily due to the association of the notochord
with the developing axial skeleton (10). CT scanning may possess a potential
advantage in detecting bone destruction, status of cortical bone,
periosteal reaction and calcification. The majority of the present
study demonstrated mixed lytic-sclerotic bone destruction which
exhibited an appearance of melting ice or sequestrum within
osteomyelitis (86%). Sclerosis may be due to reactive change of
trabecular architecture (40–60%) (6,11,12). It has been identified that vertebral
sclerosis may be a feature of chordoma (13). Lytic bone destruction with retention
of trabecular architecture is a feature of aggressive yet slow
growth, which is also frequently observed in vertebral hemangiomas
(13). Furthermore, the extending
soft tissue masses caused pressure erosion of the outer cortex and
a spiculated periosteal reaction, as observed in the majority of
the cases reviewed. The lesions typically produced widening of
transverse and intervertebral foramina. These results also suggest
aggressive but slow growth as a feature of the tumor. Calcification
of the soft tissue mass occurred in 40% of cases as in the present
series (14). The intratumoral
calcifications were hypothesized to represent bone sequestrae from
bone destruction or real calcifications of chondroid variant.
The presence of an accompanying soft tissue mass,
spanning several vertebral levels, is characteristic of chordomas
(15). Soft tissue mass without bone
involvement, as observed in 1 of the cases reviewed, has been
previously described (15–18). MRI is useful in demonstrating the soft
tissue mass. Extension of the soft tissue mass was larger than the
involved vertebral body which produces a collar button appearance
in the sagittal plane. The lesions typically spare intervertebral
disks, which may be involved in certain cases (2,19).
Intervertebral disks were not affected in any of the cases
reviewed. The soft tissue mass is usually multi-lobular and may
occur anteriorly, laterally and posteriorly towards vertebrae in
the axial plane. In the present study, the tumor occurred
circumferentially (56%), anteriorly and laterally towards vertebrae
(33%), and laterally and posteriorly towards vertebrae (11%).
Encasement of the vertebral artery has been described previously
(20). None of the tumors
demonstrated vessel constriction (14). Signal intensity was heterogeneous and
hyperintense with hypointense septa on T2-weighted images. The
hyperintense signal intensity is the result of physaliphorous cells
in myxomatous stroma of the chordoma. Hemorrhages, necrotic areas,
calcification and sequestered bone fragments may explain the signal
heterogeneity (15). The hypointense
septa on T2-weighted images correspond to fibrous septa that divide
the tumor. This feature is characteristic for diagnosing chordoma
according to the literature and has been reported in 70% of tumors
(21). Fibrous septa were identified
in only 50% of the cases reviewed. However, stripes were identified
in 30% of the patients. Enhancement patterns were heterogeneous or
ringed. The cartilaginous components in the tumor may be
responsible for the ringed enhancement pattern (15).
On the basis of the results of the present study and
available literature, there are certain distinctive features of
cervical chordoma including: Lytic and sclerotic bone destruction
with soft tissue mass (collar button appearance in sagittal plane
and multi-lobular surrounding the vertebrae in the axial plane);
pressure erosion of outer cortex and spiculated periosteal
reaction; widening of transverse and intervertebral foramina;
encasement of the vertebral artery; calcification; heterogeneous
and hypodense composition compared with the adjacent muscle on CT;
heterogeneous and hyperintense composition equal to the CSF with
hypointense septa on magnetic resonance T2-weighted images.
The aforementioned features above may be useful to
distinguish chordoma from other lesions of the cervical spine.
Benign notochordal cell tumor (BNCT) should be recognized for
differential diagnosis of chordoma. Previous studies have
documented the existence of BNCT within the axial skeleton
(8,22). However, experience with these lesions
is limited and distinction of BNCT from chordomas may not always be
possible (23). Maintenance of
trabecular architecture without bone destruction or expansion, lack
of soft tissue extension and a lack of enhancement following
contrast administration have been reported as the most reliable
means of distinguishing between BNCT and chordoma radiographically
(24,25). However, one study dispelled the
hypothesis that any single radiological criterion used to
distinguish between chordoma and BNCT is reliable (26). Hemangiomas may exhibit similar
features; however, they may readily be distinguished by their CT
appearances. Hemangiomas exhibit a polka dot appearance on axial
images or a corduroy vertebra on sagittal images on CT scans. A
number of cases without bone involvement have been described
previously (15–18). In such cases, differentiation between
chordoma and nerve sheath tumor may be difficult. However, a number
of stripes may be identified in chordoma on magnetic resonance
T2-weighted images (18).
Furthermore, the location of the paravertebral tumor mass lateral
and anterior to the vertebral body was not indicative of a tumor of
nerve root origin (27). Tumor
extension into the transverse foramina has not been reported in
nerve sheath tumor (28).
Chondrosarcoma exhibits similar MRI features with respect to
chordoma, although it involves the neural arch more frequently than
the vertebral body and the chondroid matrix is often evident as
characteristic rings and arcs (27).
Osteosarcoma may also demonstrate lytic-sclerotic destruction, but
soft tissue mass of osteosarcoma often contains amorphous,
cloud-like immature bone (11).
Myeloma, lymphoma and spinal metastases may also be considered in
the differential diagnosis. However, these tumors are often
revealed to be more heterogeneous on T2-weighted images, and often
occur in multifocal spinal localizations (11).
In conclusion, CT and MRI each have respective
advantages in the diagnosis of chordoma. CT images have advantage
of evaluating calcification and bone abnormalities that may narrow
down the differential diagnosis to aggressive but slow-growing
lesions, including mixed lytic-sclerotic bone destruction, pressure
erosion of outer cortex and spiculated periosteal reaction. MRI
scanning highlights features including multi-lobular hyperintensity
on T2-weighted imaging with hypointense septa and soft tissue mass
fully or partially surrounding vertebral body which may aid in the
exclusion of the majority of lesions in the differential diagnosis.
It is necessary to combine CT and MRI examinations for patients
with suspected cervical chordoma.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
JFC was involved in designing of the study, analysis
of data, drafting the manuscript and revising it. WJX and JHL made
substantial contributions to conception, acquisition of data, and
interpretation of data. DPH and HSC were responsible for the
evaluation of CT and MRI images. FH was responsible for the
associated pathological analysis. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review board of the Affiliated Hospital of Qingdao University and
informed consent was waived for this retrospective study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Christopher D, Fletcher JA and Krishnan U:
WHO classification of tumours of soft tissue and boneInternational
agency for research on cancer. 4th edition. WHO; Lyon: pp. 110–111.
2013
|
|
2
|
Wippold FJ II, Koeller KK and
Smirniotopoulos JG: Clinical and imaging features of cervical
chordoma. AJR Am J Roentgenol. 172:1423–1426. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bjornsson J, Wold LE, Ebersold MJ and Laws
ER: Chordoma of the mobile spine. A clinicopathologic analysis of
40 patients. Cancer. 71:735–740. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sundaresan N, Boriani S, Rothman A and
Holtzman R: Tumors of the osseous spine. J Neurooncol. 69:273–290.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Erdem E, Angtuaco EC, Van Hemert R, Park
JS and Al-Mefty O: Comprehensive review of intracranial chordoma.
Radiographics. 23:995–1009. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yamaguchi T, Yamato M and Saotome K: First
histologically confirmed case of a classic chordoma arising in a
precursor benign notochordal lesion: Differential diagnosis of
benign and malignant notochordal lesions. Skeletal Radiol.
31:413–418. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nishiguchi T, Mochizuki K, Tsujio T,
Nishita T and Inoue Y: Lumbar vertebral chordoma arising from an
intraosseous benign notochordal cell tumour: Radiological findings
and histopathological description with a good clinical outcome. Br
J Radiol. 83:e49–e53. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Deshpande V, Nielsen GP, Rosenthal DI and
Rosenberg AE: Intraosseous benign notochord cell tumors (BNCT):
Further evidence supporting a relationship to chordoma. Am J Surg
Pathol. 31:1573–1577. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yamaguchi T, Watanabe-Ishiiwa H, Suzuki S,
Igarashi Y and Ueda Y: Incipient chordoma: A report of two cases of
early-stage chordoma arising from benign notochordal cell tumors.
Mod Pathol. 18:1005–1010. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
D'Haen B, De Jaegere T, Goffin J, Dom R,
Demaerel P and Plets C: Chordoma of the lower cervical spine. Clin
Neurol Neurosurg. 97:245–248. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ross JS and Moore KR: Diagnostic imaging:
spine. 3rd edition. Elsevier Health Sci; 2015
|
|
12
|
Murphey MD, Andrews CL, Flemming DJ,
Temple HT, Smith WS and Smirniotopoulos JG: From the archives of
the AFIP. Primary tumors of the spine: Radiologic pathologic
correlation. Radiographics. 16:1131–1158. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Darby AJ, Cassar-Pullicino VN, McCall IW
and Jaffray DC: Vertebral intra-osseous chordoma or giant
notochordal rest? Skeletal Radiol. 28:342–346. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Soo MY: Chordoma: Review of
clinicoradiological features and factors affecting survival.
Australas Radiol. 45:427–434. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Smolders D, Wang X, Drevelengas A,
Vanhoenacker F and De Schepper AM: Value of MRI in the diagnosis of
non-clival, non-sacral chordoma. Skeletal Radiol. 32:343–350. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vaz RM, Pereira JC, Ramos U and Cruz CR:
Intradural cervical chordoma without bone involvement. Case report.
J Neurosurg. 82:650–653. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dow GR, Robson DK, Jaspan T and Punt JA:
Intradural cerebellar chordoma in a child: A case report and review
of the literature. Childs Nerv Syst. 19:188–191. 2003.PubMed/NCBI
|
|
18
|
Zhou H, Liu Z, Liu C, Ma Q, Liu X, Jiang L
and Wei F: Cervical chordoma in childhood without typical vertebral
bony destruction: Case report and review of the literature. Spine
(Phila Pa 1976). 34:E493–E497. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Firooznia H, Pinto RS, Lin JP, Baruch HH
and Zausner J: Chordoma: Radiologic evaluation of 20 cases. AJR Am
J Roentgenol. 127:797–805. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mortelé B, Lemmerling M, Mortelé K,
Verstraete K, Defreyne L, Kunnen M and Vandekerckhove T: Cervical
chordoma with vertebral artery encasement mimicking neurofibroma:
MRI findings. Eur Radiol. 10:967–969. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Murphy JM, Wallis F, Toland J, Toner M and
Wilson GF: CT and MRI appearances of a thoracic chordoma. Eur
Radiol. 8:1677–1679. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yamaguchi T, Suzuki S, Ishiiwa H, Shimizu
K and Ueda Y: Benign notochordal cell tumors: A comparative
histological study of benign notochordal cell tumors, classic
chordomas, and notochordal vestiges of fetal intervertebral discs.
Am J Surg Pathol. 28:756–761. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yamaguchi T, Iwata J, Sugihara S, McCarthy
EF Jr, Karita M, Murakami H, Kawahara N, Tsuchiya H and Tomita K:
Distinguishing benign notochordal cell tumors from vertebral
chordoma. Skeletal Radiol. 37:291–299. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nishiguchi T, Mochizuki K, Ohsawa M, Inoue
T, Kageyama K, Suzuki A, Takami T and Miki Y: Differentiating
benign notochordal cell tumors from chordomas: Radiographic
features on MRI, CT, and tomography. AJR Am J Roentgenol.
196:644–650. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kyriakos M: Benign notochordal lesions of
the axial skeleton: A review and current appraisal. Skeletal
Radiol. 40:1141–1152. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kreshak J, Larousserie F, Picci P, Boriani
S, Mirra J, Merlino B, Brunocilla E and Vanel D: Difficulty
distinguishing benign notochordal cell tumor from chordoma further
suggests a link between them. Cancer Imaging. 14:42014.PubMed/NCBI
|
|
27
|
Elefante A, Caranci F, Del Basso De Caro
ML, Peca C, Guadagno E, Severino R, Mariniello G and Maiuri F:
Paravertebral high cervical chordoma. A case report. Neuroradiol J.
26:227–232. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Karakida O, Aoki J, Seo GS, Ishii K, Sone
S, Nakakouji T and Otsuka K: Epidural dumbbell-shaped chordoma
mimicking a neurinoma. Pediatr Radiol. 26:62–64. 1996. View Article : Google Scholar : PubMed/NCBI
|