Introduction
Esophageal cancer is one of the most common
diseases, it had a very high morbidity and mortality in the world.
More than 90% of esophageal cancer are squamous cell carcinomas.
The main clinical manifestations of advanced esophageal cancer are
progressive dysphagia. Patients often died of failure to eat
accompanied by organ failure. At present, the commonly used
treatment methods include local surgical resection and palliative
treatment. Local surgical excision has a large injury, patients
often cannot tolerate. Common palliative treatment methods include
endoscopic dilatation, placement of esophageal stents, endoscopic
chemical therapy for slow-release particle implantation and
nasogastric feeding (1). In 1983,
Frimberger first applied metal stents in the treatment of patients
with esophageal stenosis (2), the
method has been gradually recognized and widely used (3,4). Some
scholars believed that stent implantation should be the first
choice for inoperative malignant stenosis, which is currently an
effective method to relieve dysphagia caused by advanced esophageal
cancer (5–7). Radiofrequency ablation, as an approach
of treating malignant tumors, was primarily used in the treatment
of tumors in hollow viscera, such as biliary tumors and colorectal
cancers (8–11). Its working mechanism is mainly through
thermal damage on tumor tissue, thus destroying tumor tissues.
Radiofrequency ablation in the treatment of esophageal stenosis is
still rare. This study was designed to explore the radiofrequency
ablation combined with esophageal stent in the treatment of
advanced esophageal stenosis. Therefore, a single-center
prospective study of radiofrequency ablation combined with
esophageal stent was designed for treatment of malignant esophageal
stenosis.
Patients and methods
Patients
A total of 70 patients with malignant esophageal
obstruction undergoing gastroenterology in our hospital from April
2013 to April 2015 were enrolled, including 36 males and 34
females, aged from 43 to 82 years, with an average of 64.4 years.
Inclusion criteria: i) Advanced esophageal squamous cell carcinoma
confirmed by ugi, enhanced CT scan of the chest, gastroscopy and
biopsy, abdominal and neck ultrasound. ii) The tumor was located in
the thoracic esophagus. iii) Expected survival time >3 months
before stenting. iv) No esophageal cancer radical indications. v)
In addition to stent placement treatment, follow the patient's
subjective intention, radiotherapy and chemotherapy were not
performed. Exclusion criteria: i) Advanced esophageal cancer
patients with cachexia, coma and give up treatments. ii)
Perforation of the esophagus caused by esophageal fistula and other
causes of cancer. This study was approved by the Ethics Committee
of China-Japan Union Hospital of Jilin University (Jilin, China).
Patients and their families signed an informed consent form before
treatment.
Methods
Included patients in the study were randomly
assigned to the treatment group (radiofrequency ablation combined
with esophageal stent) and control group (esophageal stent), each
group included 35 patients. In the treatment group, 19 were males
and 16 were females, aged 43–79 years, the mean age was 63.5 years.
In the control group, 17 were males and 18 were females, aged 52–82
years, the mean age was 64.9 years. Procedure in the treatment
group was: i) Under the guidance of digital subtraction angiography
(DSA), the guide wire was inserted through the esophageal stenosis,
the endoscope was placed over the obstruction site through the oral
cavity, and the radiofrequency ablation catheter was inserted
through the working channel, 2 electrodes of the radiofrequency
ablation catheter were in touch with the tumor surface under the
endoscope, circumferential radiofrequency ablation therapy was then
performed. ii) Retain the guide wire, stent was placed into the
lesions guided by the guide wire. Release the stent according to
the marking position so that the upper and lower edges of the stent
were exceeded the lesion by 2.0 cm. After releasing the stent, the
carrier and guidewire was taken out. Procedure in the control group
was the second step in the treatment group guided with DSA. The
main equipment: Habib EndoHPB RFA endoscope (EMcision, London, UK),
Olympus GIF-Q260J endoscopy (Olympus, Tokyo, Japan) esophageal
stent coated with silicone (N-SE-G-20/100-A-8/650).
Complication management
Intraoperative hemorrhage patients in the treatment
group were treated with local injection of norepinephrine for
hemostasis under endoscopy, and then esophageal stent implantation
was performed. Intraoperative perforation patients were given to
the covered stent to block the perforation site. Patients with
intraoperative stent displacement achieved the predicted position
after adjusting the stent by placing forceps into the working
channel under endoscope. All patients successfully completed the
treatment, no major complications which needed surgically treatment
were occurred.
Efficacy evaluation
According to the evaluating standards of WHO and
Stooler classification of dysphagia and esophageal stenosis
(12): Grade 0 means be able to eat
normal diet, grade 1 means be able to eat soft rice, grade 2 means
be able to eat semi-liquid, grade 3 means be able to eat the
liquid, grade 4 means inability to eat or inflow. The degree of
esophageal stenosis before and after treatment was measured by
upper gastrointestinal angiography. When the contrast medium passed
through the stenosis, the stenosis diameter was measured and
recorded. The time of inability to eat after the operation was
recorded. All patients were followed-up for 24 months. Improvement
of dysphagia at 1, 3, and 6 months after surgery was followed-up in
Outpatient Department. The stenosis of esophageal stenosis and the
incidence of complications were measured by upper gastrointestinal
angiography.
Statistical analysis
We used Statistical Product and Service Solutions
(SPSS) 16.0 software (SPSS, Inc., Chicago, IL, USA) for statistical
analysis. Measurement data of normal distribution were expressed as
mean ± standard deviation (mean ± SD), two independent samples were
compared using t-test. Regarding the comparision of the readmission
time in treat and control groups, Student's t-test was employed.
Counting data were expressed as the number of cases and percentage,
comparison of them was analyzed with Chi-square test or rank sum
test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
In the treatment group, 19 were males and 16 were
females, aged 43–79 years, the mean age was 63.5 years old. In the
control group, 17 were males and 18 were females, aged 52–82 years,
the average age was 64.9 years old. There was no significant
difference in sex, pre-treatment esophageal stenosis and esophageal
stenosis (P>0.05). Results were listed in Table I.
 | Table I.Basic characteristics of patients. |
Table I.
Basic characteristics of patients.
| Characteristics | Treatment group | Control group | P-value |
|---|
| Sex |
|
| 0.632 |
| Male | 19 | 17 |
|
|
Female | 16 | 18 |
|
| Esophageal stenosis
diameter (mm) |
| 2 | 5 | 3 | 0.452 |
| 3 | 12 | 10 | 0.607 |
| 4 | 8 | 11 | 0.420 |
| 5 | 6 | 8 | 0.550 |
| 6 | 4 | 3 | 0.690 |
| Section |
| Neck | 0 | 0 |
|
| Upper
chest | 7 | 4 | 0.324 |
| Middle
chest | 20 | 22 | 0.626 |
| Lower
chest | 8 | 9 | 0.780 |
Comparison of dysphagia degree
In the present study, no significant difference in
preoperative dysphagia degree between the treatment group and the
control group was found (P>0.05). One month after treatment, the
relief rate of dysphagia in both groups was the same. Three months
after treatment, no significant difference in the dysphagia degree
was observed between the two groups (P>0.05). However, dysphagia
degree in the treatment group was better than that in the control
group 6 months after the treatment. Patients whose Stooler grade
was 0–2 in the treatment group were more than the control group,
the difference was statistically significant (P=0.018 and
P<0.05). Detailed results were shown in Table II.
| Table II.Postoperative dysphagia degree
comparison between the treatment group and control group according
to Stooler classification. |
Table II.
Postoperative dysphagia degree
comparison between the treatment group and control group according
to Stooler classification.
| Grades | Treatment group | Control group | P-value |
|---|
| Before the
surgery |
|
| 0.289 |
| Grade 0,
1, 2 | 12 | 8 |
|
| Grade 3,
4 | 23 | 27 |
|
| Postoperative 1
month |
|
| 1 |
| Grade 0,
1, 2 | 35 | 35 |
|
| Grade 3,
4 | 0 | 0 |
|
| Postoperative 3
months |
|
| 0.643 |
| Grade 0,
1, 2 | 33 | 32 |
|
| Grade 3,
4 | 2 | 3 |
|
| Postoperative 6
months |
|
| 0.018 |
| Grade 0,
1, 2 | 29 | 20 |
|
| Grade 3,
4 | 6 | 15 |
|
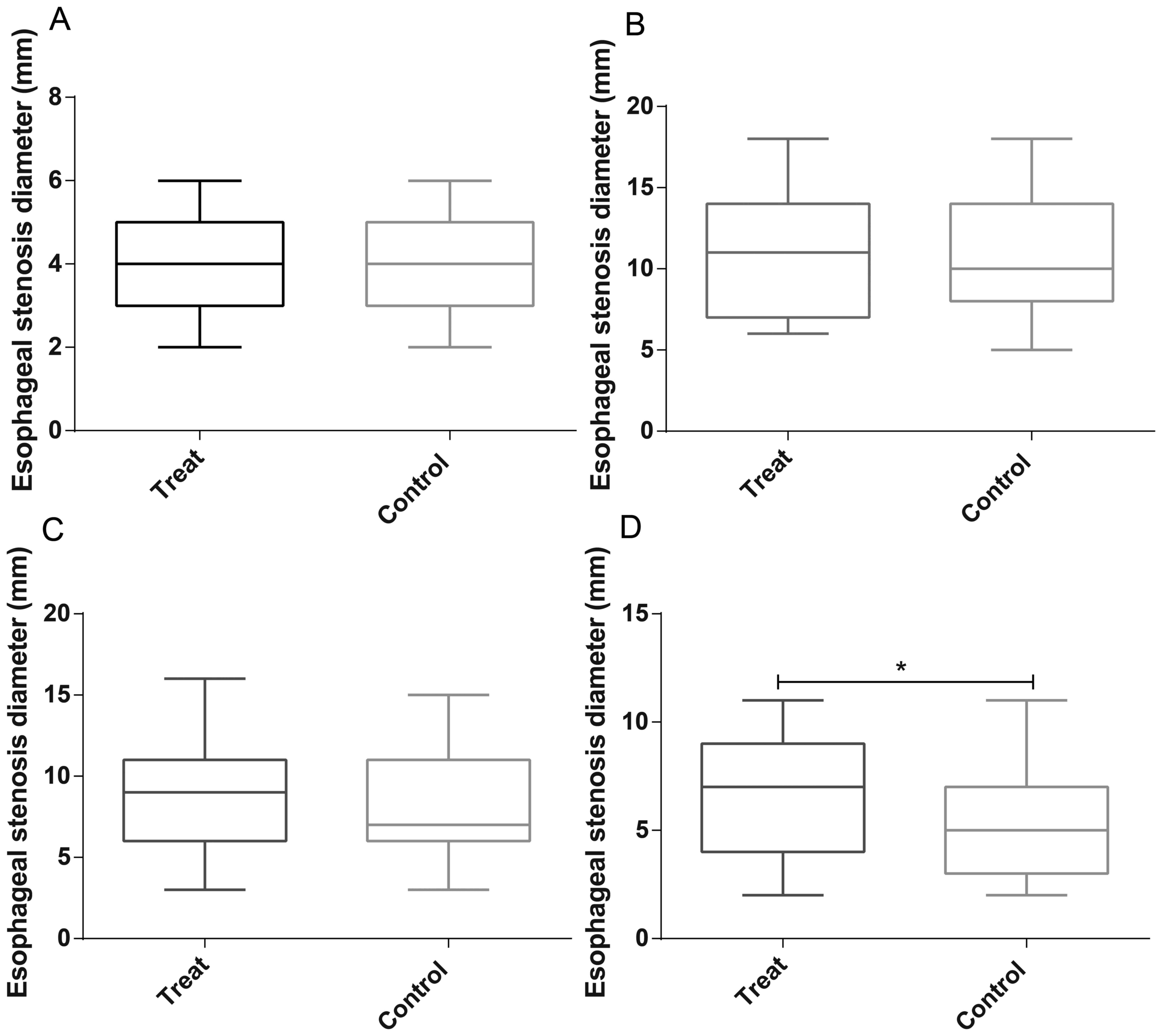
Comparison of postoperative esophageal
stenosis
In our report, we performed gastroscopy to evaluate
the degree of esophageal stenosis before treatment and at 1, 3 and
6 months after treatment. The results illustrated that no
significant difference in esophageal stenosis was exerted between
the two groups before treatment (P=0.544), the improvement of
esophageal stenosis 1 and 3 months after treatment in the treatment
group was better than that in the control group, but the difference
was not statistically significant (P=0.730 and 0.393,
respectively). However, the degree of esophageal stenosis 6 months
after treatment improved better in the treatment group in
comparison with those in the control group, the difference was
statistically significant (P=0.038). Results were illustrated in
Fig. 1.
Adverse events
In this study, no deaths during hospitalization
occurred in all enrolled patients. The treatment group had 6 cases
of bleeding, and the control group had 7, local spray of
norepinephrine for hemostasis was performed. There were 2 cases of
esophageal perforation in the treatment group and 1 in the control
group, the perforation was <5 mm. Perforation was covered with
the stent to block the wounds, and these patients were not sent for
surgical treatment. Three patients occurred stent displacement
occurred in the treatment group and 2 in the control group. There
were no significant differences between the two groups in all the
above adverse events (P>0.05). Specific information was listed
in Table III.
| Table III.Adverse events of the enrolled
patients in treatment and control groups. |
Table III.
Adverse events of the enrolled
patients in treatment and control groups.
|
| Treatment group | Control group | P-value |
|---|
| Hemorrhage | 6 | 7 | 0.758 |
| Perforation | 2 | 1 | 0.556 |
| Stent
displacement | 3 | 2 | 0.643 |
Prognosis
During the 2 years of follow-up, 12 patients in the
treatment group died, with a mortality rate of 34.3%. Seventeen
patients in the control group died, with a mortality rate of 48.6%.
No significant difference in mortality was found (P=0.225 and
P>0.05). After treatment, the patient was readmitted to the
hospital again because of the inability to eat, and the Stooler was
graded 4. Readmission in the treatment group was superior to that
in the control group, the difference was statistically significant
(P=0.021). The above results were demonstrated in Fig. 2.
Discussion
The 5-year survival rate of esophageal cancer is
only 15–25% (12). An important
problem faced by patients with advanced esophageal cancer is
dysphagia resulted from malignant esophageal obstruction. Unable to
eat brings great suffering to patients, inadequate nutrient intake
and malignant tumor consumption gradually lead to organ failure and
even death in patients. Esophageal stent was originally developed
to address the surgical treatment of esophageal cancer stenosis,
reconstruct the channel, solve patient's nutritional problems and
improve the life quality of patients with advanced esophageal
cancer. With the development of stent technology, development of
covered stent, esophageal stent has been more and more applied in
various esophageal fistulas, such as esophageal mediastinal
fistula, esophageal tracheal fistula, etc., and achieved good
effect (13–15).
Radiofrequency ablation technology is an expanding
field in clinical application. In 1990, McGahan et al
(16) and Rossi et al
(17) first proposed the application
of radioactive ablation inactivation to treat cancer patients. In
recent years, radiofrequency ablation was gradually applied to
digestive tract cancer, its mechanism was emitting high-frequency
radio waves through electrodes, stimulating plasma shock of cells
and tissues to generate 80–120°C heat, rapidly to form tissue
gasification and finally, tumor tissues were solidified and
necrosis. A reaction zone around the necrosis tumor cut off the
blood supply of the tumor to prevent tumor growth and
metastasis.
All the 70 patients included in this study
successfully completed the corresponding treatment. The success
rate of operation was 100%. No serious complications occurred
during the operation. In the treatment group, there were 6 cases of
hemorrhage, the incidence was 17.1%, 2 cases of perforation, the
incidence was 5.7%, 3 cases of stent displacement, the incidence
rate was 8.6%, these patients were all improved after conservative
treatment. In the control group, there were 7 cases of hemorrhage,
the incidence rate was 20.0%, 1 case of perforation, the incidence
was 2.9%, 2 cases of stent displacement, the incidence was 8.6%,
these patients were all improved after conservative treatment. No
significant difference in the incidence of complications was found
between the two groups. Although no serious complication occurred
in this study, endoscopists still need to pay attention to possible
complications associated with radiofrequency ablation, including
esophageal perforation, vascular injury, esophageal leakage,
esophageal leakage, and sepsis. Among them, the most dangerous and
the most common one is the iatrogenic heat injury of the
surrounding tissues by radiofrequency ablation, mainly manifested
as esophageal perforation and vascular injury.
For exploring the effectiveness of radiofrequency
ablation combined with esophageal stent implantation in the
treatment of malignant esophageal stenosis, 35 patients with
esophageal cancer who underwent esophageal stent placement alone
were enrolled in this study as the control group. Followed-up for 2
years, the observation time was postoperative 1, 3 and 6 months,
patient's symptoms and esophageal stenosis were accessed. Results
showed that within 1–3 months after surgery, there was no
difference in the effect between the radiofrequency ablation
combined with esophageal stent and esophageal stent alone in
treatment of malignant esophageal stenosis (P>0.05). However, in
long-term efficacy over 6 months, radiofrequency ablation combined
with esophageal stent was superior to esophageal stent alone in the
treatment of malignant esophageal stricture (P<0.05). In
addition, readmission time due to dysphagia in the treatment group
was significantly longer than the control group, the difference was
statistically significant (P<0.05).
It is worth mentioning that esophageal stent for
malignant esophageal stenosis caused by dysphagia and the treatment
of esophageal fistula is safe and effective. There are metal and
plastic stents. However, they are only served as a palliative
treatment to improve the life quality of patients with advanced
stage. There have been no reports that significantly prolonged the
survival of patients (18–20). Two-year follow-up was conducted in
this study, mortality of radiofrequency ablation combined with
esophageal stent and esophageal stent alone was similar, the
difference was not statistically significant, suggesting that it
could not prolong the survival time of patients.
In conclusion, the short-term efficacy of
radiofrequency ablation combined with esophageal stent treatment
was similar to that of esophageal stent alone. However, the
long-term efficacy of which was superior to esophageal stent alone,
it prolonged the readmission time, but no influences were observed
in the survival time. Limited to the small sample of this study,
single-center study, radiofrequency ablation combined with
esophageal stent in the treatment of malignant esophageal stenosis
still need prospective randomized controlled trials with a large
sample to verify.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YZ was for study design, MZ and KL were for data
collection and analysis. YZ and LB were for preparation of
manuscript, RH was for literature search, ZW was for funds
collection. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Animal Ethics
Committee of China-Japan Union Hospital of Jilin University (Jilin,
China). Signed written informed consents were obtained from the
patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Katsanos K, Sabharwal T and Adam A:
Stenting of the lower gastrointestinal tract: Current status.
Cardiovasc Intervent Radiol. 34:462–473. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Frimberger E: Endoscopic treatment of
benign esophageal stricture. Endoscopy. 15 Suppl 1:199–202. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sheikh RA and Trudeau WL: Expandable
metallic stent placement in patients with benign esophageal
strictures: Results of long-term follow-up. Gastrointest Endosc.
48:227–229. 1998.PubMed/NCBI
|
|
4
|
Zelenák K, Mistuna D, Lúcan J and Polácek
H: Broken esophageal stent successfully treated by interventional
radiology technique. Cardiovasc Intervent Radiol. 33:643–645. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kawai T, Miyazaki I, Yagi K, Kataoka M,
Kawakami K, Yamagishi T, Sofuni A, Itoi T, Moriyasu F, Osaka Y, et
al: Comparison of the effects on cardiopulmonary function of
ultrathin transnasal versus normal diameter transoral
esophagogastroduodenoscopy in Japan. Hepatogastroenterology.
54:770–774. 2007.PubMed/NCBI
|
|
6
|
Allum WH, Griffin SM, Watson A and
Colin-Jones D: Association of Upper Gastrointestinal Surgeons of
Great Britain and Ireland; British Society of Gastroenterology;
British Association of Surgical Oncology: Guidelines for the
management of oesophageal and gastric cancer. Gut. 50 Suppl
5:v1–v23. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shin JH, Song HY, Ko GY, Lim JO, Yoon HK
and Sung KB: Esophagorespiratory fistula: Long-term results of
palliative treatment with covered expandable metallic stents in 61
patients. Radiology. 232:252–259. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Valle J, Wasan H, Palmer DH, Cunningham D,
Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira
SP, et al: ABC-02 Trial Investigators: Cisplatin plus gemcitabine
versus gemcitabine for biliary tract cancer. N Engl J Med.
362:1273–1281. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Moss AC, Morris E, Leyden J and MacMathuna
P: Malignant distal biliary obstruction: A systematic review and
meta-analysis of endoscopic and surgical bypass results. Cancer
Treat Rev. 33:213–221. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Soderlund C and Linder S: Covered metal
versus plastic stents for malignant common bile duct stenosis: A
prospective, randomized, controlled trial. Gastrointest Endosc.
63:986–995. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ohhigashi S, Nishio T, Watanabe F and
Matsusako M: Experience with radiofrequency ablation in the
treatment of pelvic recurrence in rectal cancer: Report of two
cases. Dis Colon Rectum. 44:741–745. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pennathur A, Gibson MK, Jobe BA and
Luketich JD: Oesophageal carcinoma. Lancet. 381:400–412. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee S, Osugi H, Tokuhara T, Takemura M,
Kaneko M, Tanaka Y, Fujiwara Y, Nishizawa S, Iwasaki H and Suehiro
S: Self-expandable metallic stent for unresectable malignant
strictures in the esophagus and cardia. Jpn J Thorac Cardiovasc
Surg. 53:470–476. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Maroju NK, Anbalagan P, Kate V and
Ananthakrishnan N: Improvement in dysphagia and quality of life
with self-expanding metallic stents in malignant esophageal
strictures. Indian J Gastroenterol. 25:62–65. 2006.PubMed/NCBI
|
|
15
|
Shim CS, Jung IS, Cheon YK, Ryu CB, Hong
SJ, Kim JO, Cho JY, Lee JS, Lee MS and Kim BS: Management of
malignant stricture of the esophagogastric junction with a newly
designed self-expanding metal stent with an antireflux mechanism.
Endoscopy. 37:335–339. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
McGahan JP, Browning PD, Brock JM and
Tesluk H: Hepatic ablation using radiofrequency electrocautery.
Invest Radiol. 25:267–270. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rossi S, Buscarini E, Garbagnati F, Di
Stasi M, Quaretti P, Rago M, Zangrandi A, Andreola S, Silverman D
and Buscarini L: Percutaneous treatment of small hepatic tumors by
an expandable RF needle electrode. AJR Am J Roentgenol.
170:1015–1022. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yajima K, Kanda T, Nakagawa S, Kaneko K,
Kosugi S, Ohashi M and Hatakeyama K: Self-expandable metallic
stents for palliation of malignant esophageal obstruction: Special
reference to quality of life and survival of patients. Dis
Esophagus. 17:71–75. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xinopoulos D, Dimitroulopoulos D,
Moschandrea I, Skordilis P, Bazinis A, Kontis M, Paraskevas I,
Kouroumalis E and Paraskevas E: Natural course of inoperable
esophageal cancer treated with metallic expandable stents: Quality
of life and cost-effectiveness analysis. J Gastroenterol Hepatol.
19:1397–1402. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xinopoulos D, Dimitroulopoulos D,
Tsamakidis K, Korkolis D, Fotopoulou A, Bazinis A, Kontis M,
Vasilopoulos P and Paraskevas E: Palliative treatment of advanced
esophageal cancer with metal-covered expandable stents. A
cost-effectiveness and quality of life study. J BUON. 10:523–528.
2005.PubMed/NCBI
|