Introduction
Among patients with lung cancer, ~40% develop bone
metastasis with a relatively short median survival time in Japan in
1981, and the metastatic disease currently lacks an effective
therapeutic strategy (1).
Bone-modifying agents (diphosphonates) reduce skeletal-associated
events (pathologic fracture, spinal cord compression and radiation
or surgery to bone), however, they do not significantly improve
overall survival (1). Therefore,
novel and effective therapeutic approaches for the metastatic
disease are urgently required.
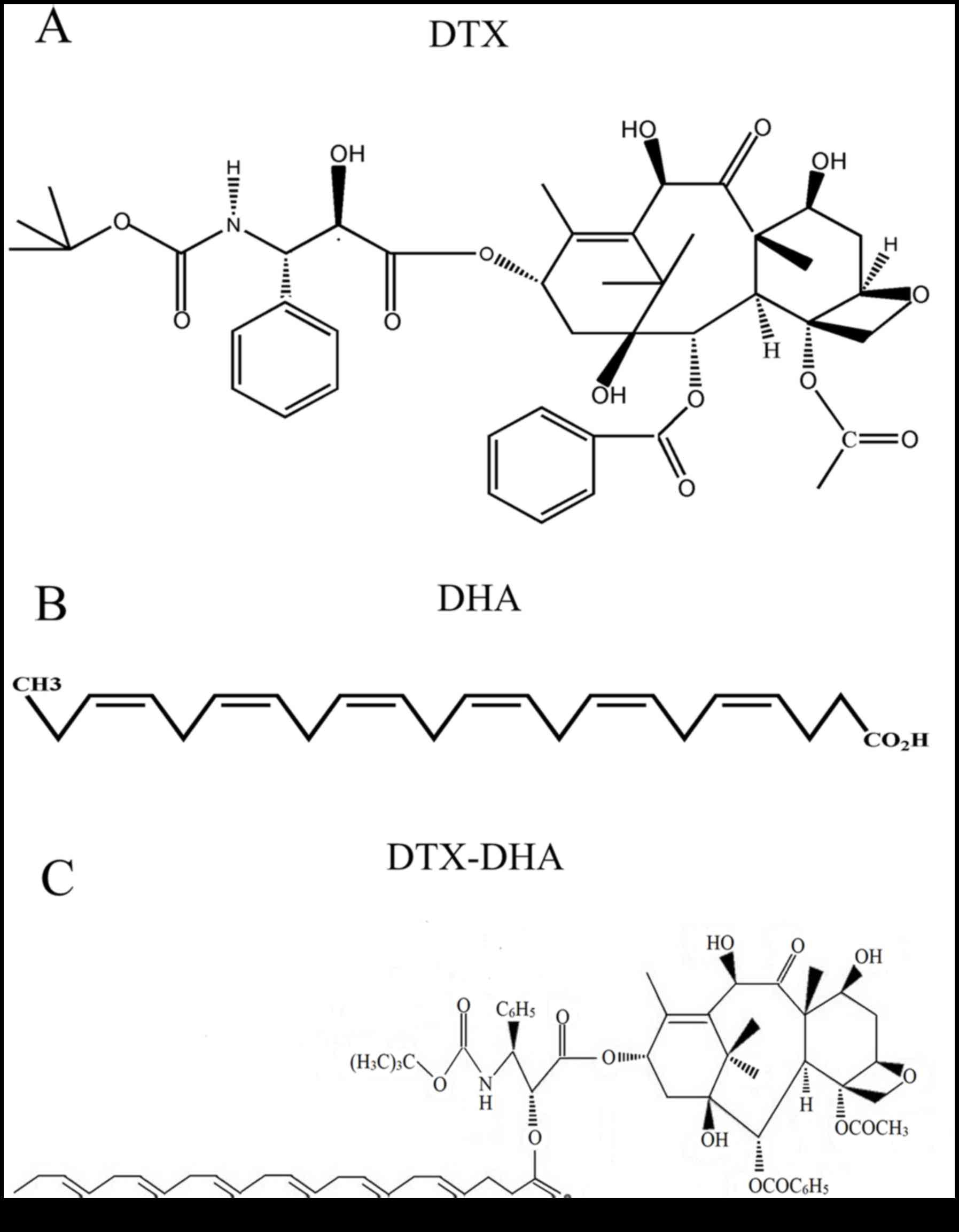
Docetaxel (DTX; Fig.
1A) is currently used as a first- or second-line treatment for
patients with lung cancer, however, it is less effective for the
treatment of patients with bone metastasis of lung cancer (2,3). Since DTX
may cause serious bone marrow inhibition in patients, it is unable
to reach a therapeutic concentration at the lesion sites of
skeletal metastases (4). Therefore,
the lack of discrimination of DTX between neoplastic and healthy
cells is a key reason that it demonstrates poor efficacy in the
treatment of lung cancer metastasis to bone.
Lung cancer is highly heterogeneous histologically
and molecularly, and as a result, only a small number of drug
targets for lung cancer have been identified (5,6).
Fortunately, phosphatidylethanolamine becomes exposed on the tumor
vascular endothelium of lung tumors, and not on normal vessels and
cells (7,8). Notably, it has been identified that
docosahexaenoic acid (DHA; Fig. 1B)
is a ligand of phosphatidylethanolamine (9). Furthermore, DHA is safe for clinic
application as it is an endogenous compound (10).
It has previously been identified that DHA is an
inhibitor of breast cancer metastasis to bone (11). It has also been demonstrated that DHA
supplementation increases first-line chemotherapy efficacy in
patients with advanced non-small cell lung cancer (12,13). A
possible underlying molecular mechanism is that DHA significantly
reduces E-selectin expression at the endothelial cell surface
(14,15). Since DTX, which is conjugated to DHA,
may be hydrolyzed back to DTX and DHA in vivo, DHA is not
only a tumor-targeting ligand, but also a synergist of DTX for
inhibiting lung cancer metastasis to bone (12,16).
An innovative DTX-loaded bovine serum albumin
(BSA)-coupled DHA nanoparticle (DTX-DHA-BSA-NP) for inhibiting lung
cancer metastasis to bone was successfully prepared by the authors'
research group. A previous study identified that the mean survival
of the nanoparticles was longer than that of DTX (17). However, due to the immunogenicity of
BSA, intravenous administration of DTX-DHA-BSA-NPs in humans may
cause allergic reactions. Furthermore, DTX-DHA-BSA-NPs are
difficult to produce on an industrial scale due to their complex
preparation process (18,19). Based on the clinical studies on
DHA-paclitaxel for the treatment of metastatic malignant melanoma,
esophago-gastric cancer and advanced non-small cell lung cancer,
DHA was conjugated to DTX (DTX-DHA, Fig.
1C) by chemical means, in order to explore its effect on lung
cancer metastasis to bone (20–23).
Materials and methods
Materials
DHA was purchased from Nu-Chek Prep Inc. (Elysian,
MS, USA). DTX was provided by Shanghai Jinhe Bio-Technology Co.,
Ltd. (Shanghai, China). 1,3-dicyclohexylcarbodiimide was purchased
from J&K Scientific Ltd. (Beijing, China). Methylene chloride
and 4-dimethylaminopyridine were purchased from Aladdin Bio-Chem
Technology Co., Ltd. (Shanghai, China). A tartrate-resistant acid
phosphatase (TRAP) kit (cat. no. CS0740-1KT) was purchased from
Sigma-Aldrich (Merck KGaA, Darmstadt, Germany). Macrophage
colony-stimulating factor (M-CSF) and receptor activator of nuclear
factor-κB ligand (RANKL) were provided by R&D Systems, Inc.
(Minneapolis, MN, USA). C57BL/6 mice were purchased from Harbin
Veterinary Research Institute (Harbin, China). Dulbecco's modified
Eagle's medium (DMEM) and RPMI-1640 media were purchased from
HyClone (GE Healthcare Life Sciences, Logan, UT, USA). A549 human
lung carcinoma cells and LLC murine Lewis lung carcinoma cells were
purchased from the Affiliated Tumor Hospital of Harbin Medical
University (Harbin, China). RAW 264.7 murine macrophage cells were
purchased from Shanghai Institutes for Biological Sciences
(Shanghai, China). An alkaline phosphatase (ALP) assay kit (cat.
no. AP0100-1KT) was purchased from Sigma-Aldrich (Merck KGaA). All
other materials were purchased from Beyotime Institute of
Biotechnology (Haimen, China).
Synthesis of DTX-DHA
DTX-DHA was synthesized from DTX and DHA with a
one-step reaction that coupled DHA to DTX at the 2′-hydroxyl
position. In brief, DHA (13.5 mg), 1,3-dicyclohexylcarbodiimide
(16.9 mg) and 4-dimethylaminopyridine (5 mg) were added to the
solution of DTX (33 mg) in dichloromethane (2.5 ml) under nitrogen.
The reaction mixture was stirred at room temperature for 2 h.
Following dilution with ethyl ether (1:10), the reaction mixture
was washed with 5% aqueous hydrochloric acid, distilled water and
saturated aqueous sodium chloride in turn at room temperature. The
mixture was concentrated by evaporating under a vacuum at 40°C with
anhydrous sodium sulfate as the desiccant. Column chromatography
(10 g silica gel stationary phase; 60 ml acetic ether-hexane mobile
phase) of the residue produced 43 mg (95%) solid DHA-DTX at room
temperature. In all experiments described subsequently, DTX and
DTX-DHA were formulated in a 50% Tween-80/ethanol/normal saline
mixture (2:1:97, respectively) (24).
Cell lines
A549 and LLC cells were used to perform cell
migration and cell proliferation assays. RAW 264.7 and LLC cells
were used to perform the osteoclast-induced formation assay. All
cells were cultured in RPMI-1640 or DMEM with 10% heat-inactivated
fetal bovine serum (FBS) and 0.1% antibiotics, and incubated in a
humidified 5% CO2 atmosphere at 37°C.
Determination of anti-cancer activity
in vitro
DHA-DTX was evaluated in vitro for
anti-proliferative activity against LLC and A549 cells using an MTT
assay. Tumor cells were seeded into sterile 96-well plates
(1×104 cells/well) in RPMI-1640 or DMEM (10% FBS) medium
and incubated at 37°C for 24 h. The DTX-DHA and DTX were first
dissolved in dimethyl sulfoxide (DMSO), then diluted in RPMI-1640
or DMEM medium culture solution with final DMSO concentration of
0.5% (v/v). The tumor cells were treated with DTX or DTX-DHA at
five different concentrations (0, 0.005, 0.05, 0.5 and 5 µM), with
three replicates, and incubated for 48 or 72 h. Then, 10 µl MTT was
added to the cell culture medium prior to incubation for a further
4 h. Subsequently, the supernatants were replaced with DMSO. The
optical density was determined using a Microplate Reader (MD
SpectraMax M5) at 490 nm (25).
Cell migration assay
A Transwell migration assay was performed using LLC
cells. First, LLC cells (1×105) were seeded in the upper
cell chamber with 600 µl serum-free DMEM, 50 nM DTX or 50 nM
DTX-DHA, and incubated at 37°C for 48 h before fixing with 4%
paraformaldehyde at 4°C for 30 min. LLC cells that migrated from
the cell upper chamber to the 6-well plates were observed under a
light microscope (magnification, ×200) following staining with
crystal violet at room temperature for 30 min (26). The transmittance was calculated
according to the following equation:
Transmittance=(cellscontrol group-cellsdrug
group)/cellscontrol group ×100%.
Osteoclast-induced formation
assay
In vitro osteoclastogenesis assays were
performed to assess the effects of DTX-DHA on osteoclast
differentiation. A total of 2.5×105 RAW 264.7 cells and
LLC cells (10:1) were incubated at 37°C for 48 h in 48-well plates.
Subsequently, the cells were incubated at 37°C in complete cell
culture medium containing 10 ng/ml murine recombinant RANKL and 10
ng/ml murine recombinant M-CSF following proliferation in 48-well
plates for 24 h. Then, the cells were treated with RPMI-1640
culture medium, 50 nM DTX, 50 nM DTX-DHA or 250 nM DTX-DHA for 72
h. Subsequently, TRAP staining was performed according to the
manufacturer's protocol (26).
Evaluation of maximum tolerated dose
(MTD)
All animal procedures were performed following the
protocol approved by the Institutional Animal Care and Use
Committee at The State Engineering Laboratory of Bio-Resources
Eco-Utilization, Northeast Forestry University (Harbin, China).
Initial evaluation of tolerability of DTX-DHA and DTX were
determined in healthy 6-week-old female C57BL/6 mice (18–22 g). A
total of 42 mice were caged in groups of three, provided with ad
libitum commercial mouse chow and water, and maintained on a 12
h light-dark cycle at a temperature of 23±1°C. The dose of DTX in
the in vitro assay for anti-cancer activity was 5 µmol/kg,
and 5 µmol/kg was selected as the minimum dose for the DTX-DHA to
indicate the MTD. Furthermore, 10, 15, 20, 25, 30 and 35 µmol/kg
were selected as the other six doses. Mice were administered
intravenously with DTX or DTX-DHA. Drug effects were determined
daily by monitoring of survival, body weight and overall health.
The MTD was defined as the highest dose that caused neither toxic
mortality nor >10% body weight loss within a week of
administration (27). The health of
the mice was monitored daily via bodyweight measurement and
observation of signs of distress, including apathy, loss of
appetite, catatonia and prostration. Humane endpoints for this
study included body weight loss >20% and excessive signs of
toxicity (pica behavior, lethargic or unresponsive).
In vivo assay of anti-cancer efficacy
on lung cancer metastasis to bone
Ten female C57BL/6 mice (as described above) were
used as a blank group for this study. All mice were injected with
LLC cells (10 µl, 1×106 cells/ml) in the tibia of the
right hind limb, then divided randomly into five groups (n=20 per
group): Control group, DTX group (5 µmol/kg), DTX-DHA group (5
µmol/kg) and DTX-DHA group (10 µmol/kg). The treatments were
administered intraperitoneally once daily for 10 days. The status
of the mice was observed every day and the mice were weighed every
4 days. Tumors were measured daily using a caliper until the mice
succumbed. Tumor volumes were estimated from two-dimensional
measurements using the formula: Tumor volume
(mm3)=[length (mm) × width2
(mm2)]/2. A total of 14 days subsequent to injection
with LLC cells, 3 mice from each group had blood extracted from
their tails. Serum ALP concentration in the mice was determined
according to the ALP activity detection kit (100T) protocol prior
to sacrificing the mice (11,27). Humane endpoints include body weight
loss >20% and excessive signs of toxicity (Pica behavior,
lethargic, unresponsive).
X-ray radiography
Four weeks after the initial dose, mice were imaged
using an X-ray machine (BL-X5, Zhengzhou Tianjie Electronic
Equipment Co., Ltd., Zhengzhou, China) and the X-ray radiography
images (4×3 cm) revealed the bone injuries. The radiolucent
osteolytic areas of bone metastasis were quantified for murine
Lewis lung carcinoma cells using Quantity One 1-D analysis Software
(version 4.6.9; Bio-Rad, Laboratories, Inc. Hercules, CA, USA)
(11,28).
Histopathological identification
Four weeks after the initial dose, the right hind
limb bone of mice from the four groups was excised, fixed in 10%
formalin in PBS (pH 7.2) at 4°C for 48 h, then decalcified in 14%
EDTA solution with agitation at room temperature for 2 weeks.
Subsequently, samples were dehydrated in a graded series of ethanol
(70, 80, 96 and 100%) for 1 h each at 4°C, embedded in paraffin and
cut into 4.5-µm thick sections. Samples were then deparaffinized in
xylene at room temperature for 30 min, stained with Mayers
hematoxylin solution at room temperature for 15 min and washed in
water at room temperature for 20 min. Then, samples were
counterstained with 0.5% eosin for 1 min, dehydrated in 95% ethanol
and absolute ethanol for 4 min at room temperature, and cleared in
xylene at room temperature for 4 min. Then, the samples were
observed under a light microscope (magnification, ×200) and tumor
areas were quantified using Image-Pro Plus software (version 6.0;
Media Cybernities, Silver Spring, MD, USA) (27,28).
Statistical analysis
Data are presented as the mean ± standard deviation.
Data were analyzed using one-way analysis of variance with
Newman-Keuls post-hoc test. P-values were calculated using log-rank
(Mantel-Cox) tests on Kaplan-Meier survival curves. All statistical
analysis was performed using SPSS software (IBM SPSS 19.0;
http://myibm.ibm.com/products-services/products).
P<0.05 was considered to indicate a statistically significant
difference.
Results
Determination of anti-cancer activity
in vitro
The IC50 values of A549 cells and LLC
cells treated with DTX and DTX-DHA were calculated and are
presented in Table I (OD data not
shown). The IC50 values of DTX-DHA were similar to those
of DTX for A549 and LLC cells, indicating that the in vitro
anti-cancer activities of DTX-DHA were similar to those of DTX
(24).
 | Table I.Cytotoxic effects of DTX and DTX-DHA
on LLC and A549 cell lines. |
Table I.
Cytotoxic effects of DTX and DTX-DHA
on LLC and A549 cell lines.
|
| IC50
(µM) ± SD, time=48 h |
|---|
|
|
|
|---|
| Sample | LLC | A549 |
|---|
| DTX | 0.054±0.002 | 9.780±0.046 |
| DTX-DHA | 0.045±0.001 | 8.160±0.029 |
|
|
| IC50
(µM) ± SD, time=72 h |
|
| DTX | 0.023±0.002 | 5.813±0.022 |
| DTX-DHA | 0.018±0.001 | 4.951±0.015 |
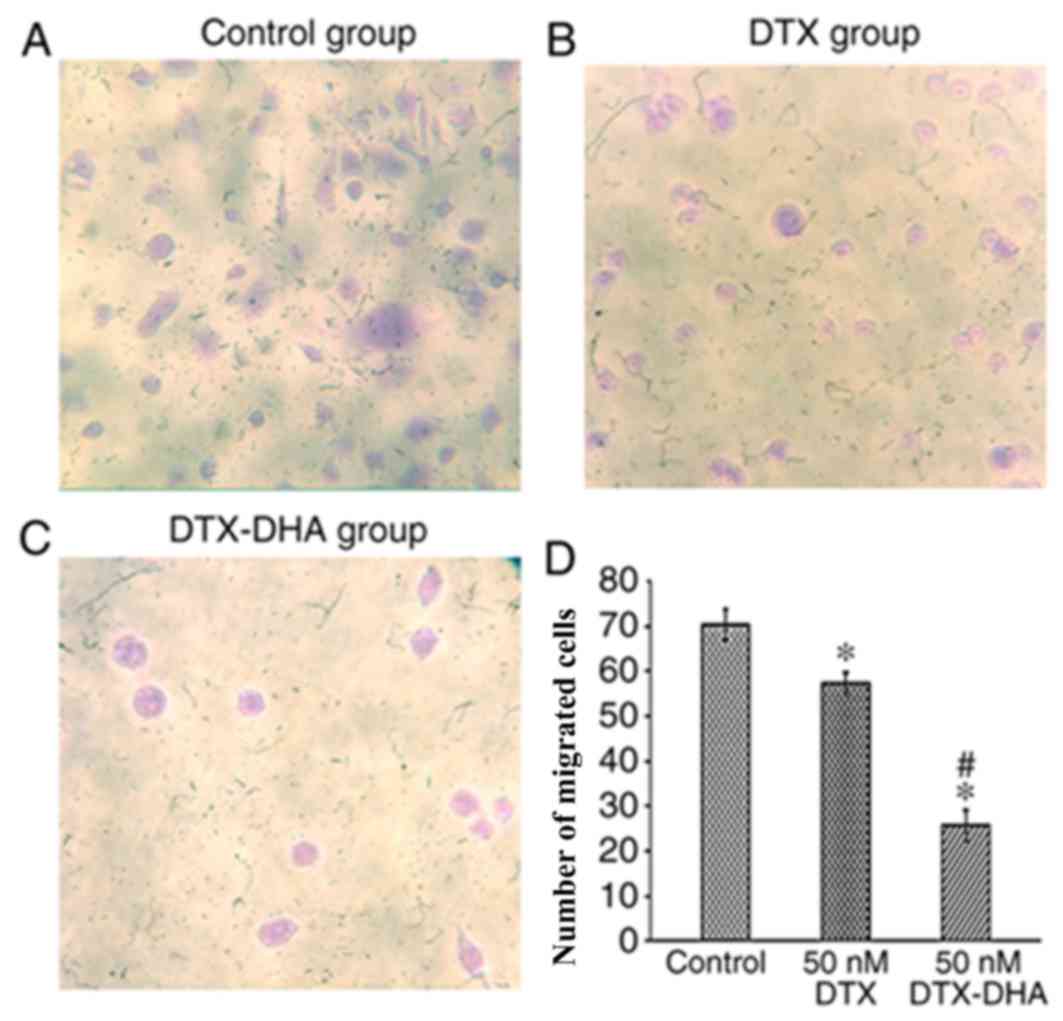
Cell migration assay
Migration ability was measured in LLC murine Lewis
lung carcinoma cells and compared with tumor cells administered
with 50 nM DTX or DTX-DHA using a Transwell migration assay
(Fig. 2A-C). Treatment with DTX-DHA
significantly inhibited tumor cell migration (*P<0.01 vs.
control). The cell transmittance of the 50 nM DTX-DHA group was
36.46±3.56%, and that of the 50 nM DTX group was 81.62±3.52%
(Fig. 2D).
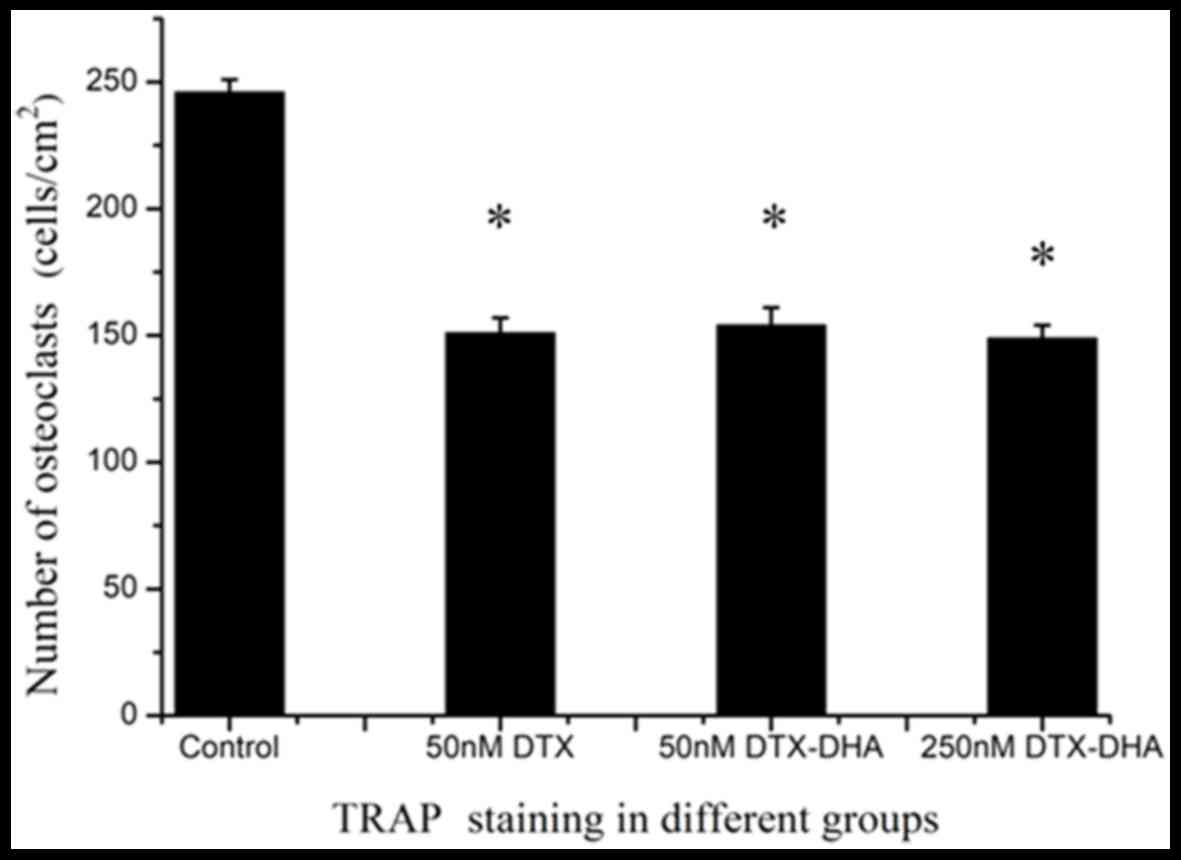
Osteoclast-induced formation
assay
The osteoclast-induced formation assay was performed
with TRAP staining. The majority of cells in the negative control
group were stained light red, and the majority of cells in the 50
nM DTX group, 50 nM DTX-DHA group and 250 nM DTX-DHA group were
stained purple. In total, 246±5, 151±6, 154±7 and 149±5 osteoclast
cells/cm2 were generated in the negative control group,
50 nM DTX group, 50 nM DTX-DHA group and 250 nM DTX-DHA group
respectively. This indicated that DTX and DTX-DHA exerted similar
inhibiting effects on RAW 264.7 murine macrophage cells forming
osteoclasts (Fig. 3).
Evaluation of MTD
In order to further develop the targeted drug into a
clinically applicable form, a series of preclinical animal studies
were performed. The MTD of DTX-DHA and DTX administered
intravenously was determined in C57BL/6 mice. The MTD of DTX-DHA
was determined by a dose escalation study followed by daily body
weight measurement and observation of general signs of toxicity.
The results indicated that the MTD of DTX was 15 µmol/kg and the
MTD of DTX-DHA was 25 µmol/kg (Table
II). The MTD of DTX-DHA was increased by 1.5-fold compared with
DTX.
| Table II.Determination of MTD following
intravenous injection of DTX or DTX-DHA. |
Table II.
Determination of MTD following
intravenous injection of DTX or DTX-DHA.
| Compound | Dosage,
µmol/kg | Observation post
injection | Lethality | Weight change,
% | MTH, µmol/kg |
|---|
| DTX | 5 | Well tolerated | 0/3 | +1.1 | 15 |
|
| 10 | Loss of
appetite | 0/3 | −3.2 |
|
|
| 15 | Apathy,
Catatonia | 0/3 | −5.8 |
|
|
| 20 | Apathy,
Catatonia | 0/3 | −10.5 |
|
|
| 25 | Prostration | 1/3 | −14.5 |
|
|
| 30 | Apathy,
prostration | 3/3 | >-20 |
|
|
| 35 | Apathy, Catatonia,
prostration | 3/3 | >-20 |
|
| DTX-DHA | 5 | Well-tolerated | 0/3 | +30.9 | 25 |
|
| 10 | Well-tolerated | 0/3 | +28.4 |
|
|
| 15 | Well-tolerated | 0/3 | +25.6 |
|
|
| 20 | Well-tolerated | 0/3 | +11.6 |
|
|
| 25 | Well-tolerated | 0/3 |
+2.6 |
|
|
| 30 | Loss of
appetite | 0/3 | −10.8 |
|
|
| 35 | Apathy,
Catatonia | 1/3 | >-20 |
|
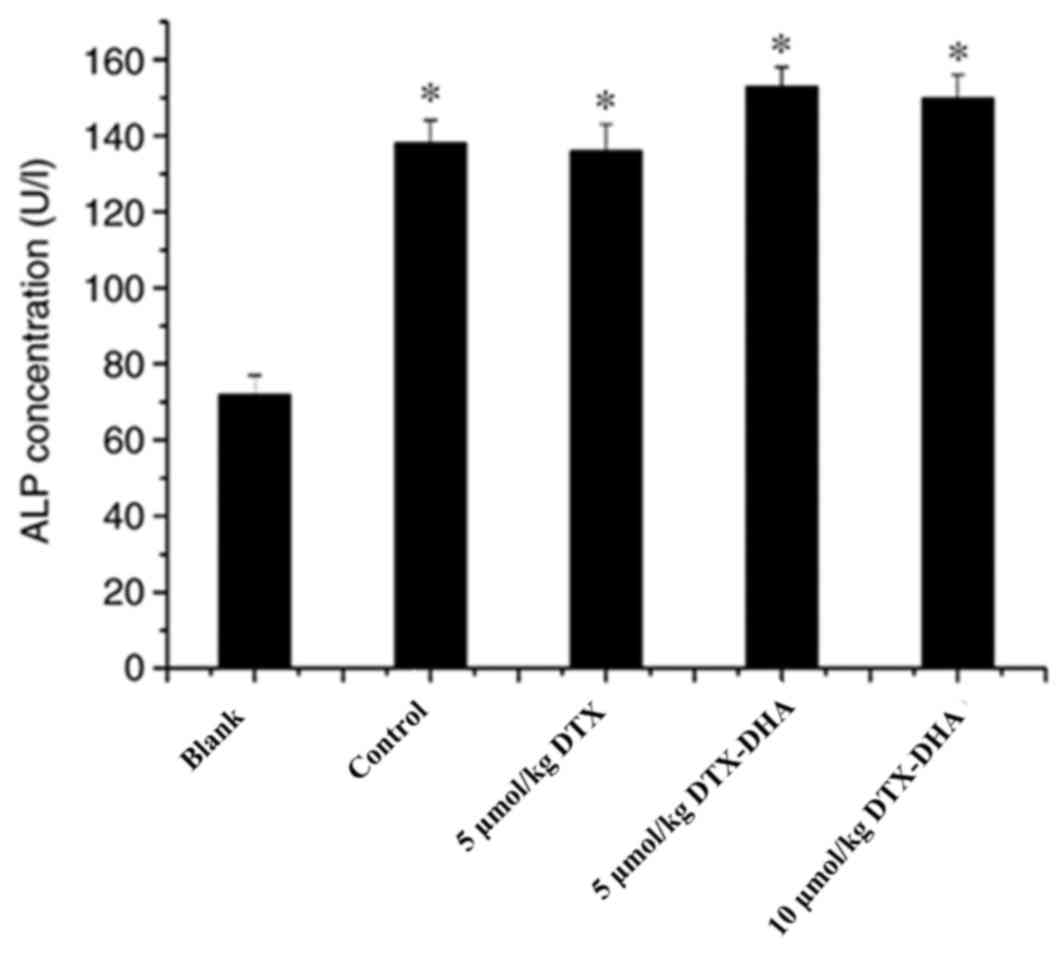
In vivo assay of anti-cancer efficacy
on lung cancer metastasis to bone
Serum ALP functions as a sensitive index for
evaluating whether a bone metastasis model has been successfully
established. The ALP concentration in each group is presented in
Fig. 4. The results indicated that
the serum ALP concentration of the four model groups (negative
control group, DTX group, 5 µmol/kg DTX-DHA group and 10 µmol/kg
DTX-DHA group) was increased compared with the blank group (not
implanted with LLC cells). Mice implanted with LLC cells exhibited
an increased ALP concentration, which suggested that the model of
bone metastasis of lung cancer in the C57BL/6 mice had been
successfully established.
To investigate the activity of the targeted drug on
lung tumor growth and metastasis, the aforementioned bone
metastasis of lung tumor model was employed. The observations of
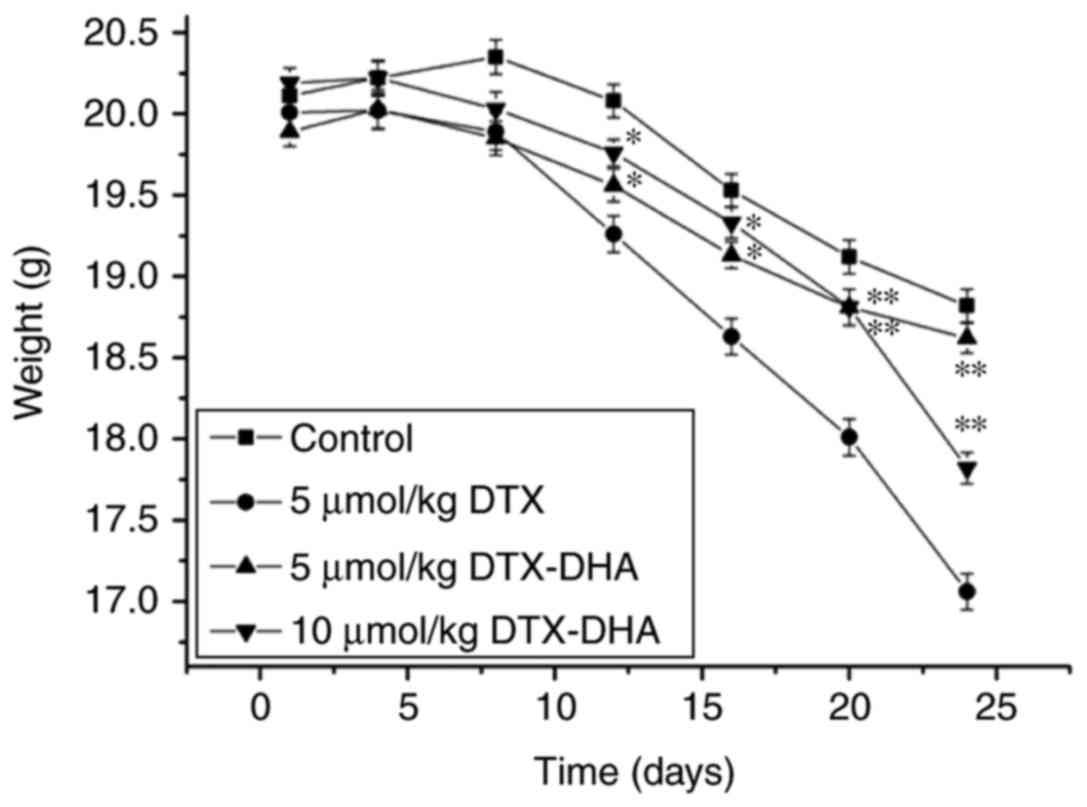
mice indicated that they started losing hair at day 7, beginning
with the right hind limb. The mice moved less with swollen right
hind limbs. There was no obvious weight loss in the mice in the
DTX-DHA-treated group during the administration period. However,
DTX significantly decreased the body weight of animals on day 12,
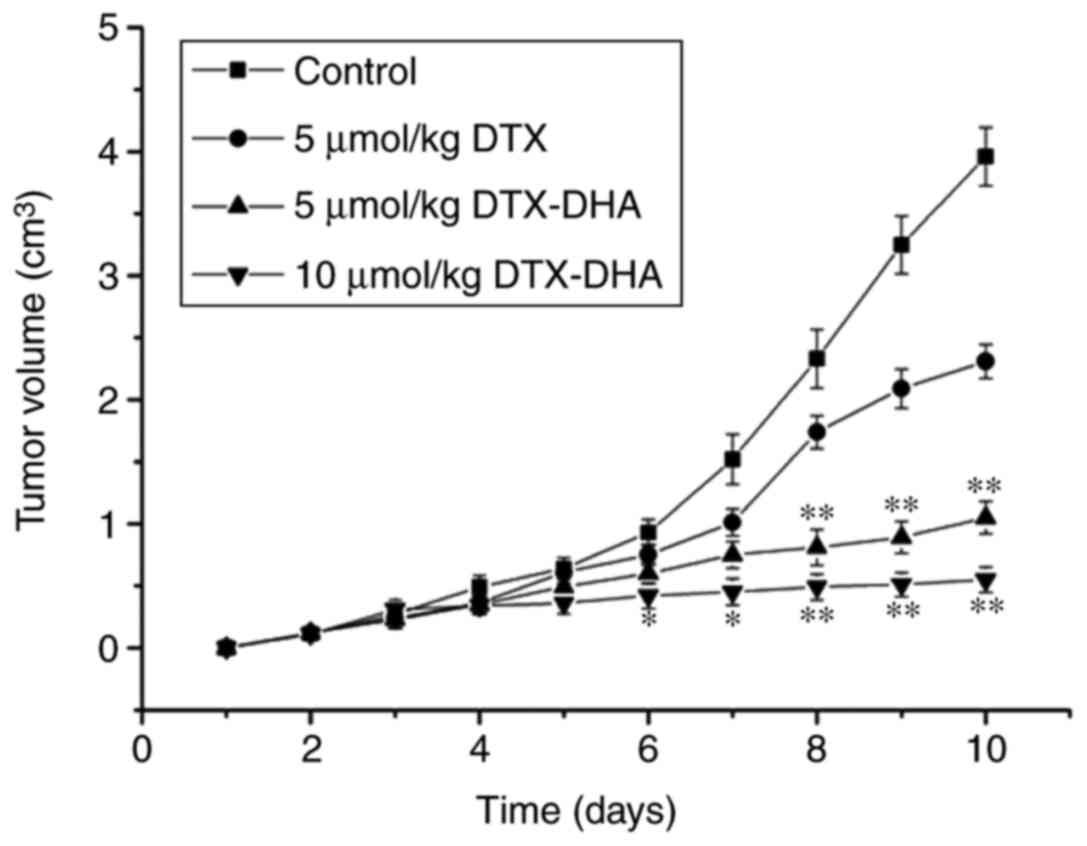
indicating that DTX was toxic to the animals (Fig. 5) (P<0.01 vs. control). The tumor
volumes in the untreated control group were increased compared with
the drug-treated control group and the DTX group (Fig. 6). Once the mice had been
intraperitoneally administered for 10 days, the mean tumor weight
of the control group (3.96±0.24 cm3) was greatest,
followed by the 5 µmol/kg DTX group (2.31±0.14 cm3),
then the 5 µmol/kg DTX-DHA group (1.05±0.13 cm3). The
lowest tumor weight was in the 10 µmol/kg DTX-DHA group (0.55±0.10
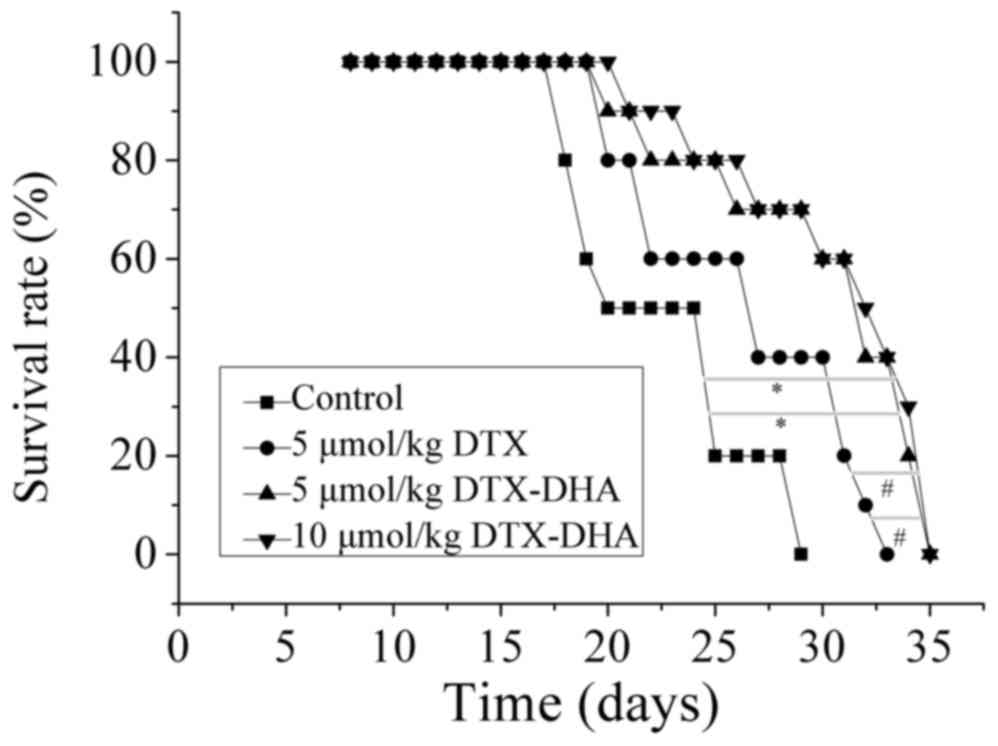
cm3). The mean survival of the mice in the negative
control group, 5 µmol/kg DTX group, 5 µmol/kg DTX-DHA group and 10
µmol/kg DTX-DHA group was 20.7±4.17, 26.1±5.68, 29.6±5.28 and
30.6±4.76 days, respectively (Fig.
7). The overall survival of the DTX-DHA group was increased
compared with that of the positive control (DTX) group. The results
demonstrated that the mice with bone metastasis of lung cancer
treated with DTX-DHA survived significantly longer compared with
those treated with DTX (*P<0.01 vs. DTX group).
X-ray radiography
Four weeks after the initial dose, the X-ray
radiography images of the four model groups were captured (Fig. 8A-D). A total of 20, 12, 8 and 7 mice
had severe tissue injury in the negative control group, positive
control group (5 µmol/kg DTX group), 5 µmol/kg DTX-DHA group and 10
µmol/kg DTX-DHA group, respectively (Fig.
8; white arrow). The radiolucent osteolytic areas of bone
metastasis were quantified for murine Lewis lung carcinoma cells
using a computer-assisted Quantity One analysis program (Fig. 8E). The results demonstrated that
DTX-DHA exerts a greater anti-cancer efficiency on bone metastasis
compared with DTX.
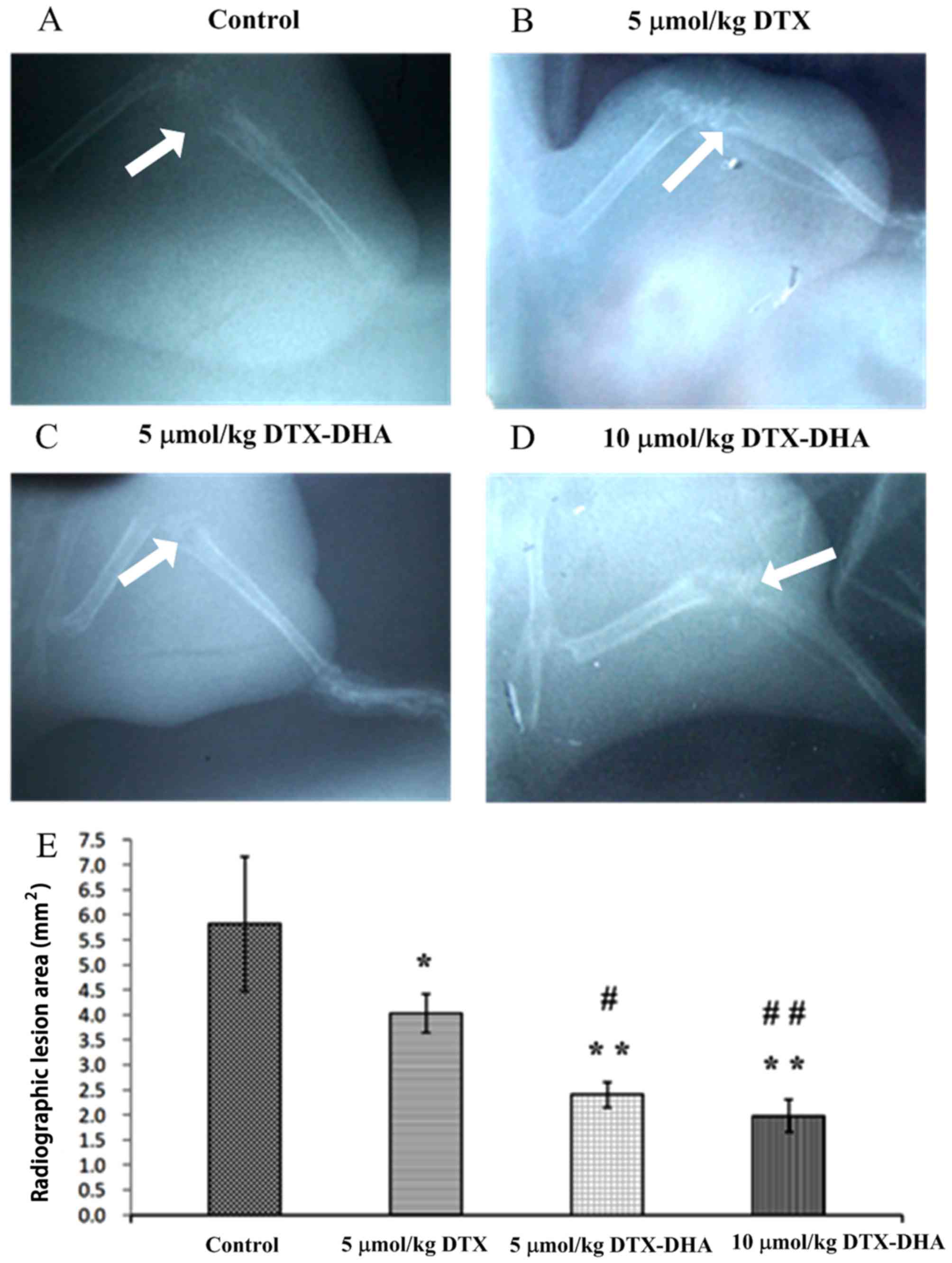 | Figure 8.X-ray radiography images of the four
model groups, indicating osteolytic lesions. Four weeks after the
initial injection, mice were imaged using X-ray machines and
representative images from the (A) control, (B) 5 µmol/kg DTX, (C)
5 µmol/kg DTX-DHA and (D) 10 µmol/kg DTX-DHA groups are presented.
Magnification, ×1. (E) The radiolucent osteolytic areas of bone
metastasis were quantified for LLC murine Lewis lung carcinoma
cells using a computer-assisted Quantity One analysis program.
n=4/group. Each value represents the mean ± standard deviation.
Data were analyzed using a one-way analysis of variance with
Newman-Keuls post-hoc test. *P<0.05 vs. control group,
**P<0.01 vs. control group, #P<0.05 vs. 5 µmol/kg
DTX group, ##P<0.01 vs. 5 µmol/kg DTX group. DTX,
docetaxel; DTX-DHA, docosahexaenoic acid-conjugated docetaxel. |
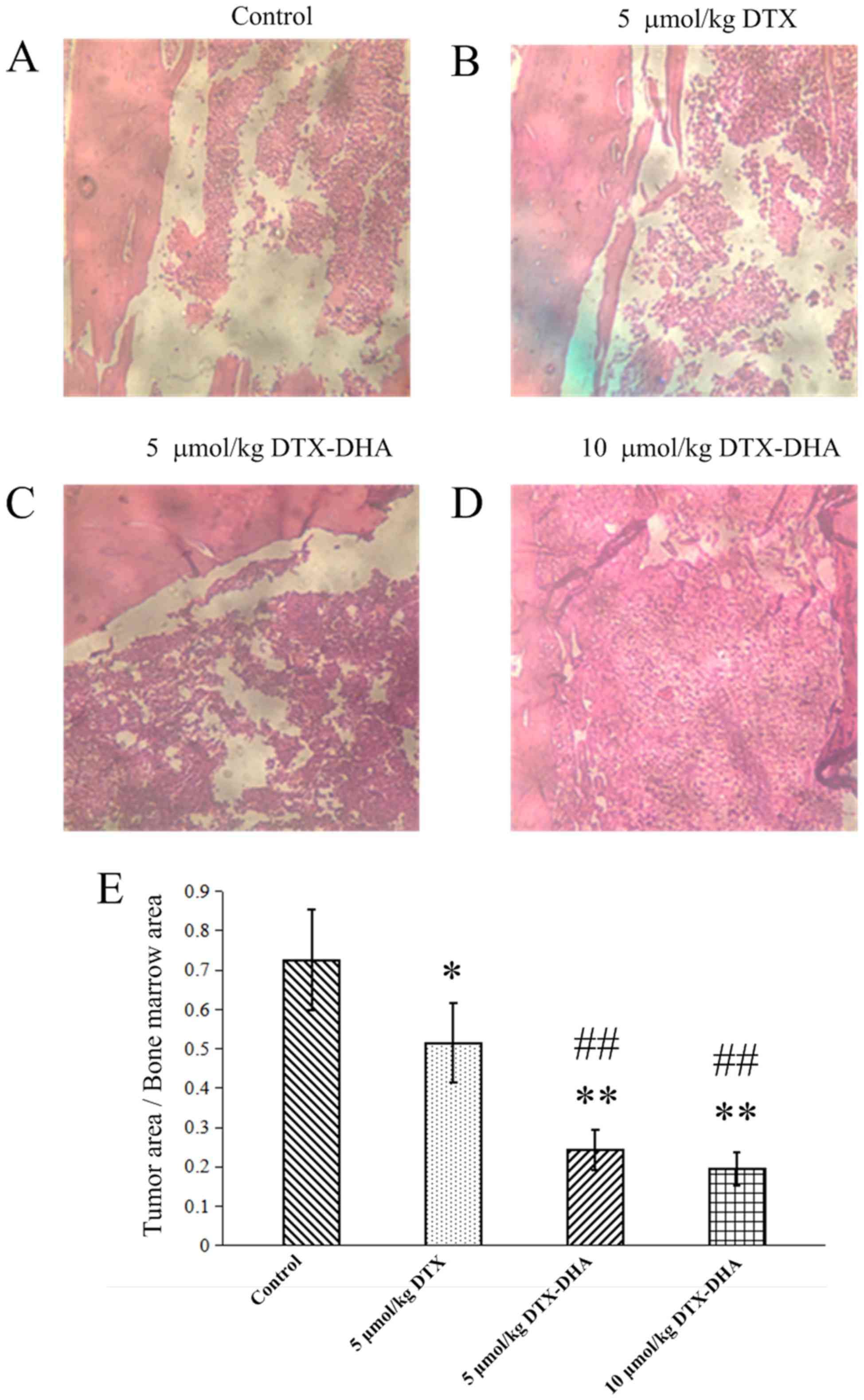
Histopathological identification
Four weeks after the initial dose, mice were
sacrificed and bones were collected and fixed in formalin.
Following decalcification, paraffin-embedded bone sections were
prepared and stained with H&E to determine the lung tumor
burden in bones. The images obtained from H&E staining are
presented in Fig. 9A-D. Tumor areas
were quantified using Image-Pro Plus software. There were fewer
healthy cells in the negative control group and positive control
group (5 µmol/kg DTX group) compared with the two DTX-DHA groups
(Fig. 9E), which further suggested
that the mice with bone metastasis of lung cancer treated with
DTX-DHA had less bone tissue damage.
Discussion
DTX exhibits a broad spectrum of activity against a
variety of tumor types, particularly non-small cell lung cancer,
breast cancer and esophago-gastric cancer (29). However, DTX is nonspecific and toxic;
and its efficacy is dose-dependent and is primarily limited by
hematological and cardiac toxicities. A tumor-targeted drug
delivery system that enhances cytotoxicity of DTX to tumor tissue
while sparing normal tissues has the potential to increase survival
(29).
Phosphatidylethanolamine, a DHA receptor, is
overexpressed on tumor cells (9).
Furthermore, phosphatidylethanolamine becomes exposed on the tumor
vascular endothelium of lung tumors, but not on normal vessels and
cells (7,8). Therefore, DHA was selected as a
targeting ligand, and DHA-conjugated DTX was prepared through an
ester bond to the DTX 2′-hydroxyl for inhibiting lung cancer
metastasis to bone (24,30).
Paclitaxel exhibits cytotoxic effects against
multiple cancer cell lines in the nM range, but DHA-paclitaxel is
active at the µM range (24,25). By contrast, the IC50 values
of DTX-DHA were similar to those of DTX for A549 and LLC cells
(Table I). A possible reason for this
is that a longer retention time of DTX-DHA in tumor cells is
beneficial to hydrolyze DTX-DHA back to DTX (24,31). The
MTD of DTX-DHA in vivo was increased compared with DTX, thus
it is speculated that DTX-DHA is primarily confined to the plasma
compartment of mice and DTX is released slowly (3).
The mice with bone metastasis from lung cancer that
were treated with DTX-DHA lived significantly longer compared with
those treated with DTX. It is possible that DTX-DHA exerts its
effects not only by targeting tumor tissues, but also via its
hydrolysis products (DHA and DTX), which may exhibit a synergistic
antitumor effect (12,13).
Lung cancer cells growing in bone cannot directly
destroy the bone tissue, but they may induce osteoclasts to
participate in bone resorption by releasing specific cell
stimulating factors (32,33). In order to further identify the
targeting cells of DTX-DHA, osteoclast-induced formation and tumor
cell migration assays were performed (33). LLC cell migration was inhibited to a
greater extent in the DTX-DHA group compared with the positive
control group (DTX group), but DTX and DTX-DHA possessed a similar
inhibitory effect induction of RAW 264.7 cells to osteoclasts.
DTX-DHA inhibited bone metastasis of lung cancer primarily through
affecting lung cancer cell migration, which indicated that DTX-DHA
could target the tumor cells (34,35).
Therefore, it is not surprising that DTX-DHA significantly improved
overall survival and exhibited decreased bone tissue damage
(P<0.01 vs. DTX group). For a bone-modifying agent targeting
osteoclast cells instead of tumor cells, the bone-modifying agent
can reduce skeletal-associated events but not improve overall
survival significantly (36).
In the present study, DTX-conjugated DHA was
successfully prepared using a chemosynthesis technique. The
toxicity studies performed in mice indicated that DTX-DHA is less
toxic than DTX. DTX-DHA had an increased tumor-targeting capacity,
stronger anti-cancer activity in vivo and superior
efficiency for inhibiting lung cancer metastasis to bone compared
with DTX. Furthermore, the overall survival of the DTX-DHA group
was significantly increased compared with the DTX group. These
results suggest that DTX-DHA may provide a promising therapeutic
approach for treating lung cancer metastasis to bone.
Acknowledgements
Not applicable.
Funding
The present study was funded by the Fundamental
Research Funds for the Central Universities (grant no.
2572018BU03), the Science Foundation of Heilongjiang Province,
China (grant no. H2018001) and the Heilongjiang Postdoctoral (grant
no. LBH-Z10282).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SJ, ZL and YZ were the principal investigators, and
were responsible for the conception and design of the study. SJ was
a major contributor in writing the manuscript. LWu performed the
synthesis, cell migration assay and osteoclast-induced formation
assay. YY performed the determination of anti-cancer activity in
vitro. LWu and YH performed the assay of anti-cancer efficacy
in vivo. XZ performed the histological examination of the
bone. LWe performed the statistical analysis. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
All animal procedures complied with the revised
Animals (Scientific Procedures) Act 1986 in the UK and Directive
2010/63/EU in Europe and were performed following a protocol
approved by the Institutional Animal Care and Use Committee at The
State Engineering Laboratory of Bio-Resources Eco-Utilization,
Northeast Forestry University (Harbin, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
LeVasseur N, Clemons M, Hutton B, Shorr R
and Jacobs C: Bone-targeted therapy use in patients with bone
metastases from lung cancer: A systematic review of randomized
controlled trials. Cancer Treat Rev. 50:183–193. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lazzari C, Bulotta A, Ducceschi M, Viganò
MG, Brioschi E, Corti F, Gianni L and Gregorc V: Historical
evolution of second-line therapy in non-small cell lung cancer.
Front Med (Lausanne). 4:42017.PubMed/NCBI
|
|
3
|
Socinski MA: Update on taxanes in the
first-line treatment of advanced non-small-cell lung cancer. Curr
Oncol. 21:e691–e703. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kenmotsu H and Tanigawara Y:
Pharmacokinetics, dynamics and toxicity of docetaxel: Why the
japanese dose differs from the western dose. Cancer Sci.
106:497–504. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kan C, Vargas G, Pape FL and Clézardin P:
Cancer cell colonisation in the bone microenvironment. Int J Mol
Sci. 17:E16742016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Popper HH: Progression and metastasis of
lung cancer. Cancer Metastasis Rev. 35:75–91. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stafford JH and Thorpe PE: Increased
exposure of phosphatidylethanolamine on the surface of tumor
vascular endothelium. Neoplasia. 13:299–308. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fahrmann JF, Grapov D, Defelice BC, Taylor
S, Kim K, Kelly K, Wikoff WR, Pass H, Rom WN, Fiehn O and Miyamoto
S: Serum phosphatidylethanolamine levels distinguish benign from
malignant solitary pulmonary nodules and represent a potential
diagnostic biomarker for lung cancer. Cancer Biomark. 16:609–617.
2016.PubMed/NCBI
|
|
9
|
Li S, Qin J, Tian C, Cao J, Fida G, Wang
Z, Chen H, Qian Z, Chen WR and Gu Y: The targeting mechanism of DHA
ligand and its conjugate with gemcitabine for the enhanced tumor
therapy. Oncotarget. 5:3622–3635. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Riediger ND, Othman RA, Suh M and
Moghadasian MH: A systemic review of the roles of n-3 fatty acids
in health and disease. J Am Diet Assoc. 109:668–679. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rahman MM, Veigas JM, Williams PJ and
Fernands G: DHA is a more potent inhibitor of breast cancer
metastasis to bone and related osteolysis than EPA. Breast Cancer
Res Treat. 141:341–352. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Murphy RA, Mourtzakis M, Chu QS, Baracos
VE, Reiman T and Mazurak VC: Supplementation with fish oil
increases first-line chemotherapy efficacy in patients with
advanced nonsmall cell lung cancer. Cancer. 117:3774–3780. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sánchez-Lara K, Turcott JG,
Juárez-Hernández E, Nuñez-Valencia C, Villanueva G, Guevara P, De
la Torre-Vallejo M, Mohar A and Arrieta O: Effects of an oral
nutritional supplement containing eicosapentaenoic acid on
nutritional and clinical outcomes in patients with advanced
non-small cell lung cancer: Randomised trial. Clin Nutr.
33:1017–1023. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mai J, Huang Y, Mu C, Zhang G, Xu R, Guo
X, Xia X, Volk DE, Lokesh GL, Thiviyanathan V, et al: Bone marrow
endothelium-targeted therapeutics for metastatic breast cancer. J
Control Release. 187:22–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yates CM, Tull SP, Madden J, Calder PC,
Grimble RF, Nash GB and Rainger GE: Docosahexaenoic acid inhibits
the adhesion of flowing neutrophils to cytokine stimulated human
umbilical vein endothelial cells. J Nutr. 141:1331–1334. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chauvin L, Goupille C, Blanc C, Pinault M,
Domingo I, Guimaraes C, Bougnoux P, Chevalier S and Mahéo K: Long
chain n-3 polyunsaturated fatty acids increase the efficacy of
docetaxel in mammary cancer cells by downregulating Akt and
PKCε/δ-induced ERK pathways. Biochim Biophys Acta. 1861:380–390.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zu Y, Hu Y, Yu X and Jiang S:
Docetaxel-loaded bovine serum albumin nanoparticles conjugated
docosahexaenoic acid for inhibiting lung cancer metastasis to bone.
Anticancer Agents Med Chem. 17:542–551. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jiang S, Gong X, Zhao X and Zu Y:
Preparation, characterization, and antitumor activities of
folate-decorated docetaxel-loaded human serum albumin
nanoparticles. Drug Deliv. 22:206–213. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bölükbas DA and Meiners S: Lung cancer
nanomedicine: Potentials and pitfalls. Nanomedicine (Lond).
10:3203–3212. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bedikian AY, DeConti RC, Conry R, Aqarwata
S, Papadopoulos N, Kim KB and Ernstoff M: Phase 3 study of
docosahexaenoic acid-paclitaxel versus dacarbazine in patients with
metastatic malignant melanoma. Ann Oncol. 22:787–793. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Payne M, Ellis P, Dunlop D, Ranson M,
Danson S, Schacter L and Talbot D: DHA-paclitaxel (Taxoprexin) as
first-line treatment in patients with stage IIIB or IV non-small
cell lung cancer: Report of a phase ii open-label multicenter
trial. J Thorac Oncol. 1:984–990. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jones RJ, Hawkins RE, Eatock MM, Ferry DR,
Eskens FA, Wilke H and Evans TR: A phase II open-label study of
DHA-paclitaxel (Taxoprexin) by 2-h intravenous infusion in
previously untreated patients with locally advanced or metastatic
gastric or oesophageal adenocarcinoma. Cancer Chemother Pharmacol.
61:435–441. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Harries M, O'Donnell A, Scurr M, Reade S,
Cole C, Judson I, Greystoke A, Twelves C and Kaye S: Phase I/II
study of DHA-paclitaxel in combination with carboplatin in patients
with advanced malignant solid tumours. Br J Cancer. 91:1651–1655.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bradley MO, Webb NL, Anthony FH, Devanesan
P, Witman PA, Hemamalini S, Chander MC, Baker SD, He L, Horwitz SB
and Swindell CS: Tumor targeting by covalent conjugation of a
natural fatty acid to paclitaxel. Clin Cancer Res. 7:3229–3238.
2001.PubMed/NCBI
|
|
25
|
Sparreboom A, Wolff AC, Verweij J,
Zabelina Y, van Zomeren DM, McIntire GL, Swindell CS, Donehower RC
and Baker SD: Disposition of docosahexaenoic acid-paclitaxel, a
novel taxane, in blood: In vitro and clinical pharmacokinetic
studies. Clin Cancer Res. 9:151–159. 2003.PubMed/NCBI
|
|
26
|
Chu J and Ding J: Plumbagin prevents bone
metastasis of lung adenocarcinoma cell line PC9 by inhibiting
migration and osteolysis. Med Innovation China. 11:11–13. 2014.(In
Chinese).
|
|
27
|
Liu F, Feng L, Zhang L, Zhang X and Zhang
N: Synthesis, characterization and antitumor evaluation of CMCS-DTX
conjugates as novel delivery platform for docetaxel. Int J Pharm.
451:41–49. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hoang B, Ernsting MJ, Tang WS, Bteich J,
Undzys E, Kiyota T and Li SD: Cabazitaxel-conjugated nanoparticles
for docetaxel-resistant and bone metastatic prostate cancer. Cancer
Lett. 410:169–179. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yared JA and Tkaczuk KH: Update on taxane
development: New analogs and new formulations. Drug Des Devel Ther.
6:371–384. 2012.PubMed/NCBI
|
|
30
|
Ray A, Larson N, Pike DB, Grüner M, Naik
S, Bauer H, Malugin A, Greish K and Ghandehari H: Comparison of
active and passive targeting of docetaxel for prostate cancer
therapy by HPMA copolymer-RGDfK conjugates. Mol Pharm. 8:1090–1099.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gligorov J and Lotz JP: Preclinical
pharmacology of the taxanes: Implications of the differences.
Oncologist. 9 Suppl 2:S3–S8. 2004. View Article : Google Scholar
|
|
32
|
Roato I: Bone metastases: When and how
lung cancer interacts with bone. World J Clin Oncol. 5:149–155.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Luo Q, Xu Z, Wang L, Ruan M and Jin G:
Progress in the research on the mechanism of bone metastasis in
lung cancer. Mol Clin Oncol. 5:227–235. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Siddiqui RA, Harvey KA, Xu Z, Bammerlin
EM, Walker C and Altenburg JD: Docosahexaenoic acid: A natural
powerful adjuvant that improves efficacy for anticancer treatment
with no adverse effects. Biofactors. 37:399–412. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Merendino N, Costantini L, Manzi L,
Molinari R, D'Eliseo D and Velotti F: Dietary ω-3 polyunsaturated
fatty acid DHA: A potential adjuvant in the treatment of cancer.
Biomed Res Int. 2013:3101862013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Vicent S, Perurena N, Govindan R and
Lecanda F: Bone metastases in lung cancer. Potential novel
approaches to therapy. Am J Respir Crit Care Med. 192:799–809.
2015. View Article : Google Scholar : PubMed/NCBI
|