Introduction
Uterine adenomyosis is a benign gynecological
condition characterized by the ectopic growth of the endometrial
tissue, including the endometrial glands and stroma, located at
least 2.5 mm below the endometrial-myometrial junction (1). The two main forms of adenomyosis are
diffuse and focal adenomyoma. Diffuse adenomyosis is more common
and characterized by the foci of endometrial mucosa scattered
throughout the uterine musculature. Adenomyoma is uncommon, but not
rare, and is defined as encapsulated foci including the two glands
and stroma implanted within the myometrium (2). Adenomyoma is mostly solid and rarely
manifests as cystic (2,3). In the majority of cases, the border
between the lesion and the surrounding myometrium is not clear.
Therefore, the term ‘adenomyoma’ may be interpreted as grossly
circumscribed adenomyotic masses (4).
Medical therapy for adenomyosis may be effective. Unfortunately,
the effects are often transient, and symptoms and signs usually
reappear when therapy is stopped (5).
For decades, hysterectomy was the most popular therapeutic option
for patients with symptomatic adenomyosis (6,7).
Hysterectomy may be a curative treatment, but it is not acceptable
to all women (8). Numerous women want
alternatives to traditional hysterectomy. However, there are no
evidence-based guidelines regarding the appropriate treatment of
symptomatic uterine adenomyosis in patients who want to preserve
the uterus (5). Furthermore, few
reports have focused on factors affecting recurrence following
laparoscopic adenomyomectomy. The present study aimed to help
physicians identify patients with adenomyoma who would benefit from
uterus sparing and those who should undergo hysterectomy to avoid a
secondary surgery.
Materials and methods
Patients
Ethical approval for the collection and publication
of patient data was obtained from the institutional review board of
Beijing Chao-Yang Hospital of Capital Medical University (Beijing,
China; reference no. EC1335097) and written informed consent was
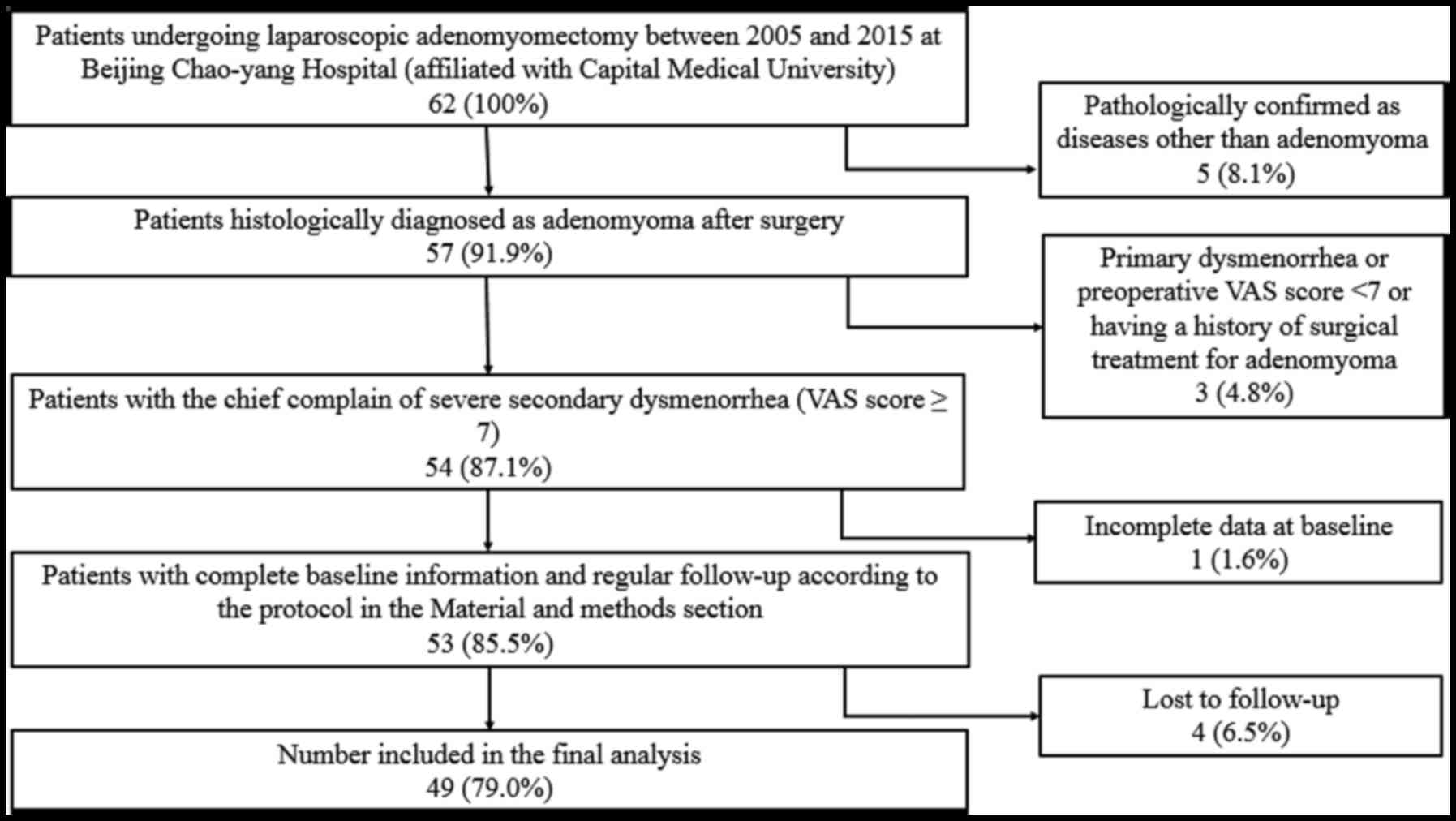
obtained from all participating patients. The medical records of 49
female patients (mean age, 40.6±5.2 years; age range, 26–51 years)
diagnosed with adenomyoma confirmed by postoperative pathology at
Beijing Chao-Yang Hospital of Capital Medical University, admitted
between November 2005 and November 2015, were retrospectively
reviewed. All inclusion and inclusion criteria are presented in
Fig. 1. The following baseline
information was collected: Age, body weight, body height, obstetric
history, gynecologic history, smoking history, drinking history,
pathological uterine volume (uterus volume was determined by the
following formula: a × b × c × π/6, where a, b and c indicate
maximum length, width and thickness of the uterus, respectively),
serum cancer antigen 125 (CA 125) level, visual analogue scale
(VAS) (9) score on admission, number
of adenomyomas, and other uterine or ovarian pathologies
accompanying adenomyosis. All patients received 3-course injections
of gonadotropin-releasing hormone agonist (GnRH-a) prior to surgery
to reduce the uterine volume and bleeding during surgery. If the
patients reported menorrhagia, diagnostic curettage was performed
to exclude any malignancy 2 weeks prior to surgery. All patients
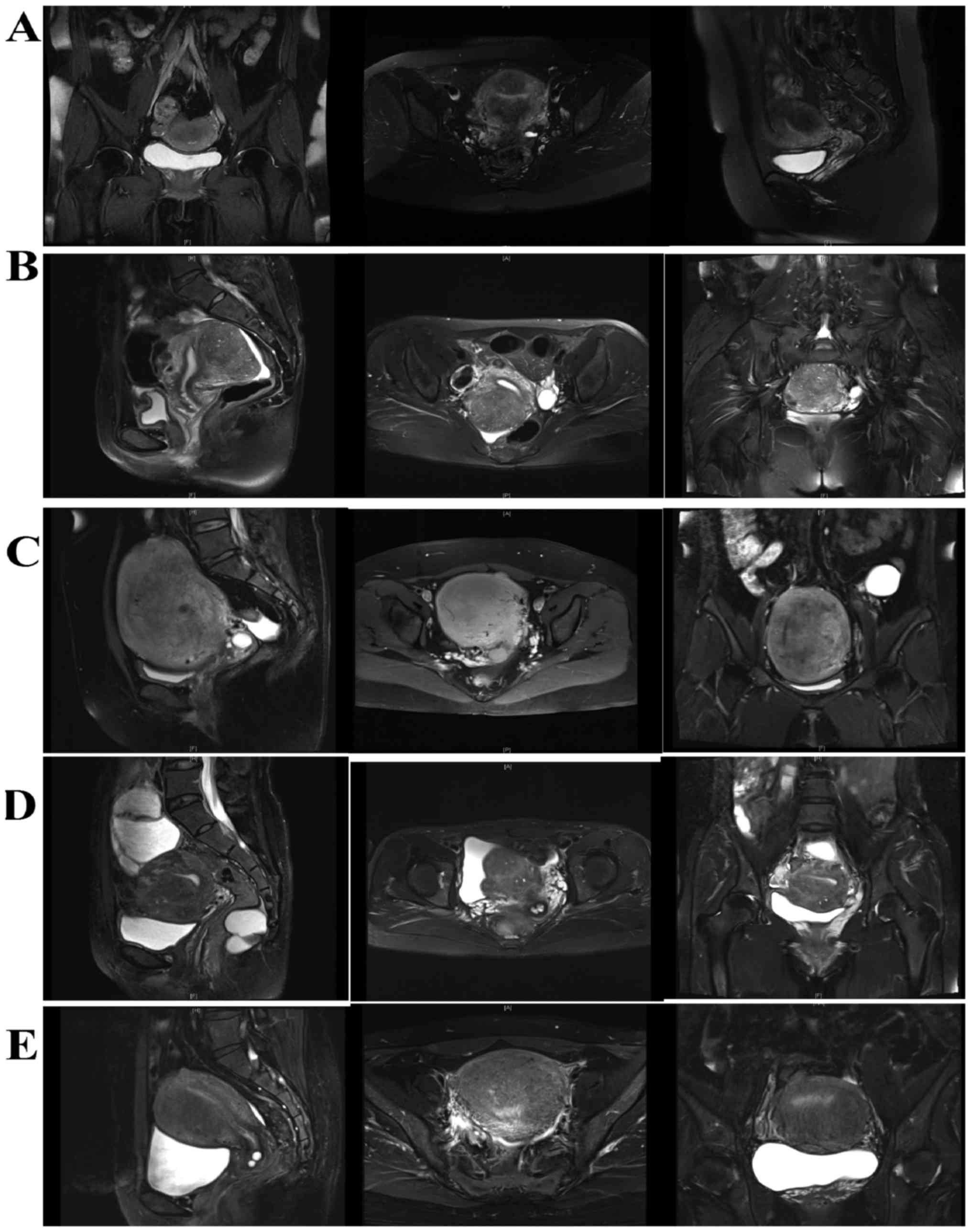
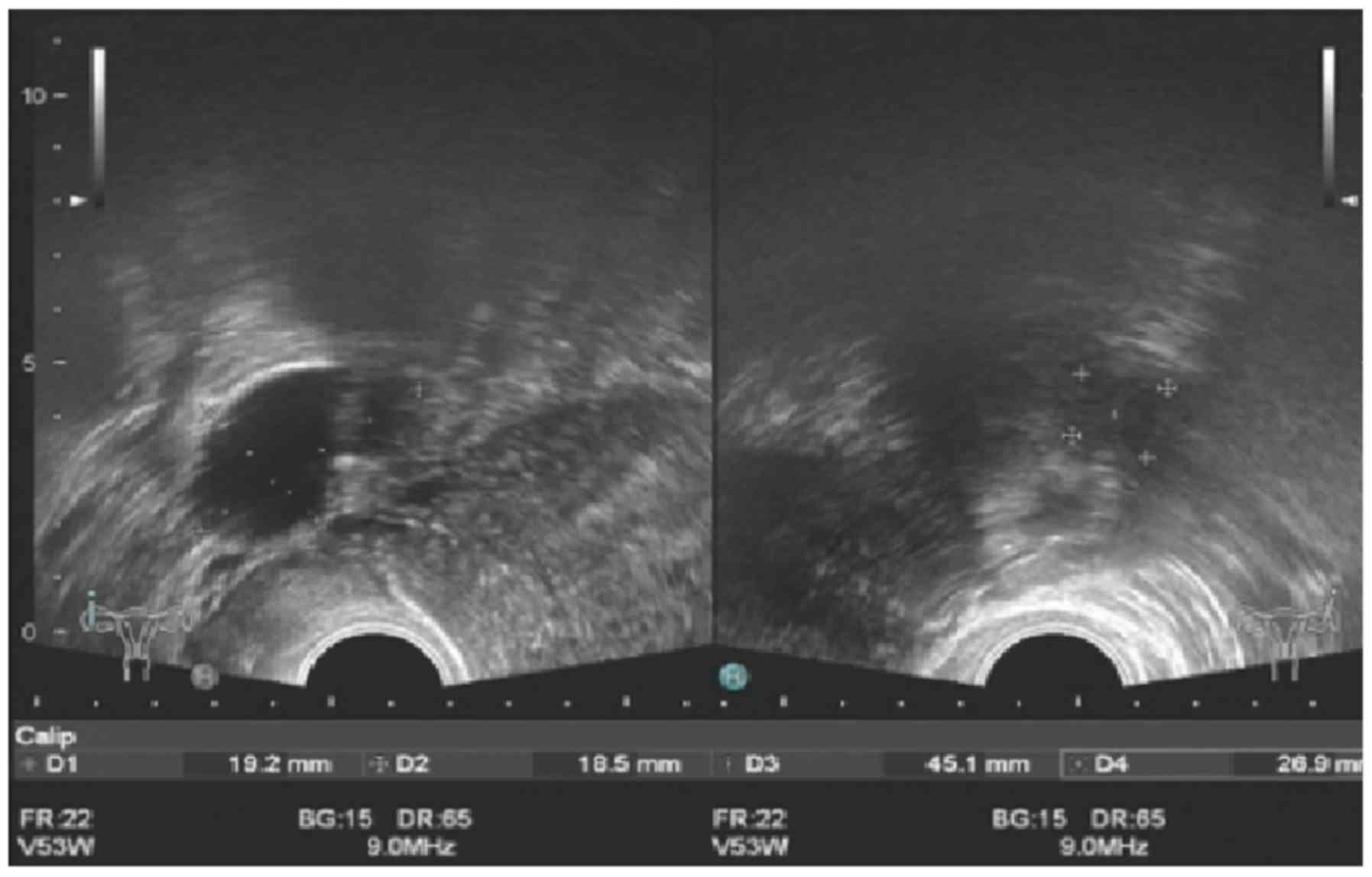
received transvaginal ultrasound evaluations prior to surgery. An
experienced ultrasound doctor was available, however, due to the
relatively high cost of the magnetic resonance imaging (MRI), only
14 patients underwent MRI prior to surgery. Representative
ultrasound and MRI images of adenomyomas are presented in Figs. 2 and 3.
Patients were asked to specify a VAS score for
dysmenorrhea 6 months subsequent to the completion of all
therapies. The patients were divided into 3 groups based on this
score: Mild or no pain (VAS score 0–2), moderate pain (VAS score
3–6) and severe pain (VAS score 7–10). All patients were followed
up at 6 and 12 months subsequent to completing all therapies during
a clinical visit. Thereafter, they were followed up at yearly
intervals starting from the second year through a phone
conversation or outpatient clinic visit, all the patients were
followed up till menopause or June 2017 in this article. The
endpoint is when the patients entered their menopause. The mean
follow-up period was 4.6 years. Reevaluations of the VAS rating and
transvaginal ultrasound examination were performed during the
outpatient clinic visit if they experienced reappearance or
aggravation of dysmenorrhea. As the time when dysmenorrhea relapsed
after surgery varied among patients, it was difficult to define a
cutoff time for the reappearance of dysmenorrhea the shortest
remission period was 7 months, while in some patients it was
several years or there was no relapse of dysmenorrhea at all.
Recurrence was determined by the subjective VAS score of the
patients throughout the follow-up duration following a period of
remission from surgery once all other potential causes were
excluded. A total of 53 patients fulfilled the inclusion criteria
and 4 patients were excluded due to loss to follow-up; therefore,
49 patients were eligible for analysis. Approximately 60% of the
leiomyomas and adenomyomas were located at the posterior wall of
uterus, 30% were located at the anterior wall and 10% were at the
fundus uteri. Tumor position was not included in the present study
as it was revealed that relapses did not always appear at the
original site where the adenomyosis was removed. Occasionally,
relapse occurred on the opposite side of the uterus to where the
surgery was performed. It was difficult to identify from where the
relapses originated from, particularly for patients with >1
lesion prior to surgery.
The operative technique involved the recognition of
the position of the lesion by careful inspection of the uterus.
This is usually difficult and requires adequate experience as the
borders of an adenomyoma are not well-defined compared with that of
a fibroid (1). Then, an incision was
created on the uterine wall with monopolar diathermy or tissue
scissors. Next, gradual dissection of the adenomyoma was performed
with scissors, monopolar diathermy and/or bipolar diathermy without
penetrating the endometrium. All recognizable lesions were removed.
Surrounding healthy myometrium was removed if necessary. Then,
closure of the uterine serosa and myometrium was performed.
Finally, intraoperative frozen biopsy was performed to exclude the
uterine sarcoma. A total of 8 patients underwent LPSN (Laparoscopic
presacral neurectomy) during laparoscopic adenomyomectomy. After
identifying the sacral promontory, the peritoneum overlying the
sacral promontory was elevated and incised vertically, the
retroperitoneal fatty tissue was then removed, the hypogastric
plexus was elevated to the lateral side, the nerve fibers are
coagulated and excised from the sacral promontory level. The
removed nerve tissue was sent for histologic examination.
Statistical analysis
Data are presented as the mean ± standard deviation.
Statistical analyses were conducted using SPSS statistical package
for Windows (version 21.0; IBM Corp., Armonk, NY, USA). An unpaired
Student's t-test and one-way analysis of variance with Fisher's
Least Significant Difference post hoc test were used to compare
continuous variables. Categorical variables were examined using a
χ2 test and a Kruskal-Wallis test. The optimum cut-off
points for CA 125 were determined by the receiver-operating
characteristic (ROC) curves for recurrence prediction. Univariate
relapse analyses results were evaluated using the Kaplan-Meier
method and compared using the log-rank test. Multivariate analyses
involving Cox regression models were performed to determine
independent factors associated with recurrence. P<0.05 was
considered to indicate a statistically significant difference.
Results
Prior to surgery, all patients reported severe
dysmenorrhea with a VAS score of 9.12±1.05, whereas 16 women had
simultaneous menorrhagia. Seven patients were nulliparous, and each
of the others experienced only 1 successful birth (except for 1
patient who gave birth twice). The patients had no previous history
of gynecological surgery except 13 patients who experienced
cesarean deliveries. The preoperative serum CA 125 level was
80.50±56.78 U/ml. Endometriosis was confirmed in 23 patients, and
14 had uterine leiomyoma confirmed by postoperative pathology
examination. Eight (16.3%) subjects underwent laparoscopic
presacral neurectomy (LPSN) and laparoscopic adenomyomectomy.
Twenty-six (53.1%) patients were prescribed 6 months of
postoperative GnRH-a therapy. Eight (16.3%) patients were
prescribed a levonorgestrel-releasing intrauterine system
(LNG-IUS). For patients who selected GnRH-a or LNG-IUS therapy
following surgery, the first injection of postoperative GnRH-a was
administered immediately following surgery. LNG-IUS was
administered at 3–6 months following surgery, depending on the
excision extent and depth of the uterine wall, to avoid
perforation. Adjuvant treatments were administered according to the
patients' personal preferences. There were no major complications
following surgery. Postoperative pain alleviation was evaluated by
the patient's self-assessment based on abatement of dysmenorrhea at
the 6-month follow-up visit. Forty-one patients experienced varying
degrees of reduced symptoms of dysmenorrhea, with an overall
effectiveness rate of 83.7% (41/49). Twenty-eight (57.1%) patients
had mild or no pain subsequent to treatment and had VAS scores
ranging between 0 and 2. Menorrhagia improved in 68.8% (11/16) of
patients. Associations between potential factors and the mitigation
of dysmenorrhea were evaluated by univariate analysis. The p-VAS
was significantly different among different groups while no factor
was found significantly related to mitigation of dysmenorrhea
following resection (Table I).
 | Table I.Factors influencing dysmenorrhea
relief as determined by p-VAS. |
Table I.
Factors influencing dysmenorrhea
relief as determined by p-VAS.
| Variables | No relief (n=8) | Partial relief
(n=13) | Near-complete relief
(n=28) | P-value |
|---|
| p-VAS | 9.38±0.74 | 4.46±0.97 | 0.46±0.69 | <0.001 |
| Age (years) | 41.4±6.8 | 40.6±4.7 | 40.3±5.1 | 0.884 |
| Body Mass Index
(kg/m2) | 22.3±3.5 | 22.8±2.5 | 23.1±3.3 | 0.831 |
| Menorrhagia |
|
|
| 0.369 |
| Yes, %
(n) | 12.5% (2) | 43.8% (7) | 43.8% (7) |
|
| No, %
(n) | 18.2% (6) | 18.2% (6) | 63.6% (21) |
|
|
Gravidity | 1.8±1.0 | 1.8±1.0 | 2.5±1.0 | 0.055 |
| History of cesarean
delivery |
|
|
| 0.558 |
| Yes, %
(n) | 23.1% (3) | 7.7% (1) | 69.2% (9) |
|
| No, %
(n) | 13.9% (5) | 33.3% (12) | 52.8% (19) |
|
| Preoperative serum
cancer antigen 125 level (U/ml) | 84.9±79.2 | 91.6±47.9 | 74.1±54.6 | 0.647 |
| Pathological
uterine size (cm3) | 127.0±58.2 | 145.9±68.3 | 145.5±93.1 | 0.845 |
| No of
adenomyomas |
|
|
| 0.919 |
| Single,
% (n) | 18.2% (4) | 22.7% (5) | 59.1% (13) |
|
|
Multiple, % (n) | 14.8% (4) | 29.6% (8) | 55.6% (15) |
|
| Coexisting
endometriosis |
|
|
| 0.203 |
| Yes, %
(n) | 8.7% (2) | 26.1% (6) | 65.2% (15) |
|
| No, %
(n) | 23.1% (6) | 26.9% (7) | 50.0% (13) |
|
| Accompanying
uterine leiomyoma |
|
|
| 0.344 |
| Yes, %
(n) | 14.2% (2) | 42.9% (6) | 42.9% (6) |
|
| No, %
(n) | 17.1% (6) | 20.0% (7) | 62.9% (22) |
|
| Laparoscopic
presacral neurectomy |
|
|
| 0.796 |
| Yes, %
(n) | 12.5% (1) | 37.5% (3) | 50.0% (4) |
|
| No, %
(n) | 17.1% (7) | 24.4% (10) | 58.5% (24) |
|
| Postoperative
gonadotropin-releasing hormone agonist therapy |
|
|
| 0.566 |
| Yes, %
(n) | 19.2% (5) | 26.9% (7) | 53.9% (14) |
|
| No, %
(n) | 13.0% (3) | 26.1% (6) | 60.9% (14) |
|
| Postoperative
levonorgestrel-releasing intrauterine system treatment |
|
|
| 0.503 |
| Yes, %
(n) | 25% (2) | 0% (0) | 75% (6) |
|
| No, %
(n) | 14.6% (6) | 31.7% (13) | 53.7% (22) |
|
Dysmenorrhea ratings during the follow-up period are
summarized in Table II. Of the 49
patients, 24.5% (12/49) experienced relapse at the end of the
follow-up period. The mean diagnosis of recurrence occurred 18.5
(6–34) months after resection. Of the
12 patients who relapsed, seven patients were in the mild or no
pain group and 5 were in the moderate pain group at 6 months of
follow-up. A total of 4 (33.3%) experienced relapse within the
first year following treatment, 3 (25%) experienced relapse during
the second year and 5 (41.7%) experienced relapse during the third
year subsequent to treatment. The VAS score of one patient
following the reappearance of dysmenorrhea reached 8, which was
higher compared with the preoperative assessment score. The patient
underwent uterine artery embolization at Peking Union Medical
College Hospital (Beijing, China). The VAS score of another patient
increased from 4 to 7 at 17 months following resection; therefore,
she underwent a hysterectomy. The degree of pain for the remaining
10 patients experiencing relapse did not reach or exceeded the
preoperative level, and they chose oral analgesics when required.
Of the 8 patients whose symptoms were not relieved following
surgery, 5 were referred for additional surgery (4 hysterectomies
and 1 laparoscopic adenomyomectomy). Potential risk factors
influencing postoperative recurrence were evaluated by univariate
analysis and reported in Table III.
Age at surgery (P=0.017), preoperative serum CA 125 level (P=0.012)
and postoperative GnRH-a therapy (P=0.025) were identified as
significant risk factors for relapse of dysmenorrhea. Patients in
the recurrence group tended to be younger, had higher preoperative
serum CA 125 level and fewer of them chose to receive GnRH-a
therapy following surgery compared with the recurrence free
group.
| Table II.Dysmenorrhea rating during the follow
up period. |
Table II.
Dysmenorrhea rating during the follow
up period.
|
|
|
| Groups (no. of
patients) |
|---|
|
|
|
|
|
|---|
| Follow-up period
(months) | No of patients | Visual analogue
scale rating | 0–2 (mild or no
pain) | 3–6 (moderate
pain) | 7–10 (severe
pain) |
|---|
| Preoperative | 49 | 9.12±1.05 | 0 | 0 | 49 |
| 6 | 49 | 2.98±3.42 | 28 | 13 | 8 |
| 12 | 49 | 3.16±3.27 | 25 | 15 | 9 |
| 24 | 44 | 3.32±3.38 | 21 | 15 | 8 |
| 36 | 35 | 4.11±3.54 | 13 | 13 | 9 |
| 48 | 30 | 3.97±3.41 | 11 | 13 | 6 |
| 60 | 22 | 3.77±3.18 | 8 | 11 | 3 |
| 72 | 12 | 3.33±2.64 | 4 | 7 | 1 |
| 84 | 8 | 4.38±2.13 | 1 | 6 | 1 |
| 96 | 5 | 5.20±1.48 | 0 | 4 | 1 |
| 108 | 2 | 4.00±1.41 | 0 | 2 | 0 |
| 120 | 1 | 5 | 0 | 1 | 0 |
| Table III.Univariate analysis of variables
influencing recurrence in enrolled patients. |
Table III.
Univariate analysis of variables
influencing recurrence in enrolled patients.
|
Characteristics | No recurrence
(n=37) | Recurrence
(n=12) | P-value |
|---|
| Age (years) | 41.6±5.2 | 37.5±4.1 | 0.017a |
| Body mass index
(kg/m2) | 23.1±2.7 | 22.1±4.1 | 0.302 |
| Menorrhagia |
|
| 0.315 |
| Yes, %
(n) | 25% (2) | 53.8% (7) |
|
| No, %
(n) | 75% (6) | 46.2% (6) |
|
|
Gravidity | 2.1±1.0 | 2.4±1.1 | 0.393 |
| History of cesarean
delivery |
|
| 0.999 |
| Yes, %
(n) | 37.5% (3) | 7.7% (1) |
|
| No, %
(n) | 62.5% (5) | 92.3% (12) |
|
| Preoperative serum
cancer antigen 125 level (U/ml) | 69.0±54.3 | 115.8±51.0 | 0.012a |
| Pathological
uterine size (cm3) | 135.4±84.0 | 164.5±70.1 | 0.285 |
| No of
adenomyomas |
|
| 0.683 |
| Single,
% (n) | 72.7% (16) | 27.3% (6) |
|
|
Multiple, % (n) | 77.8% (21) | 22.2% (6) |
|
| Coexisting
endometriosis |
|
| 0.363 |
| Yes, %
(n) | 69.6% (16) | 30.4% (7) |
|
| No, %
(n) | 80.8% (21) | 19.2% (5) |
|
| Accompanying
uterine leiomyoma |
|
| 0.156 |
| Yes, %
(n) | 92.9% (13) | 7.1% (1) |
|
| No, %
(n) | 68.6% (24) | 31.4% (11) |
|
| Laparoscopic
presacral neurectomy |
|
| 0.999 |
| Yes, %
(n) | 75% (6) | 25% (2) |
|
| No, %
(n) | 75.6% (31) | 24.4% (10) |
|
| Postoperative
gonadotropin-releasing hormone agonist therapy |
|
| 0.025a |
| Yes, %
(n) | 88.5% (23) | 11.5% (3) |
|
| No, %
(n) | 60.9% (14) | 39.1% (9) |
|
| Postoperative
levonorgestrel-releasing intrauterine system treatment |
|
| 0.190 |
| Yes, %
(n) | 100% (8) | 0% (0) |
|
| No, %
(n) | 78.4% (29) | 21.6% (12) |
|
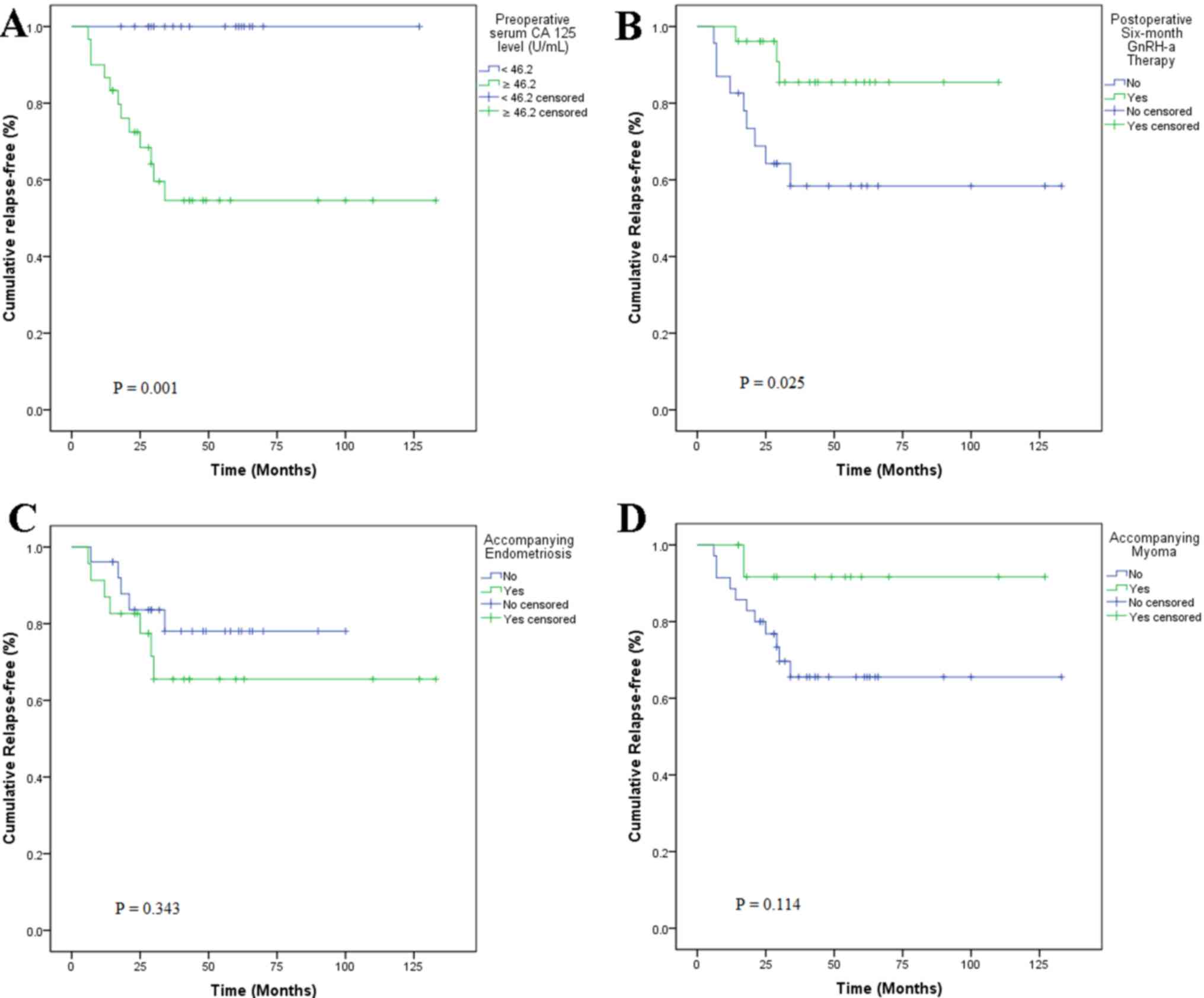
The optimum cut-off point of the preoperative serum
CA 125 level for the prediction of relapse was identified as 46.2
U/ml, with a maximum joint sensitivity of 100% and specificity of
54% using ROC curve analysis (Fig.
4). Based on this cut-off point, all recurrences were observed
for patients with preoperative serum CA 125 levels >46.2 U/ml,
and all recurrent cases had a baseline serum CA 125 level >46.2
U/ml (Fig. 5A). Furthermore, 53.1%
(26/49) of subjects received 6 courses of postoperative GnRH-a
injections as additional therapy; of these, 11.5% (3/26)
experienced relapse compared with 39.1% (9/23) of those who did not
undergo GnRH-a treatment. Kaplan-Meier curves revealed significant
differences (P=0.025) regarding recurrence between GnRH-a injection
group and non-GnRH-a injection group (Fig. 5B). Univariate Kaplan-Meier curves
revealed no significant association between accompanying
endometriosis or myoma and relapse (Fig.
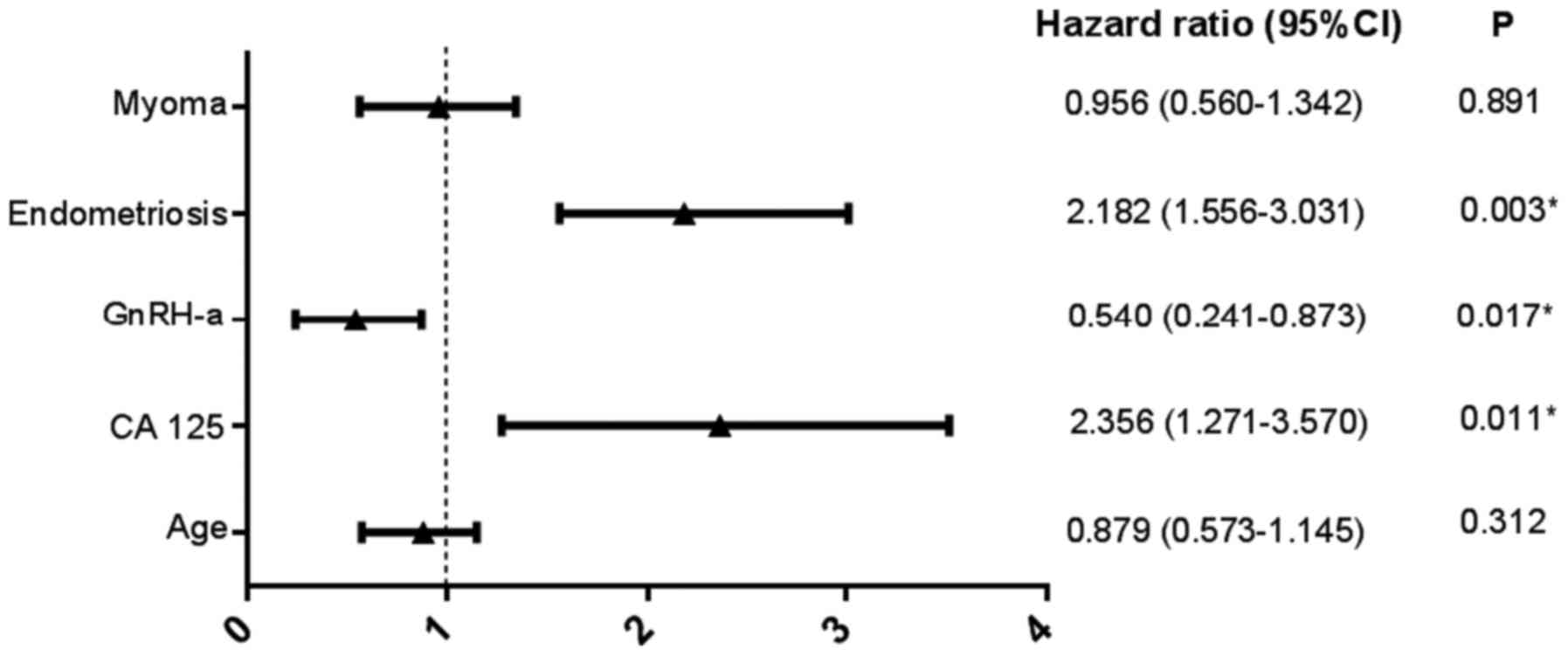
5C and D). A Cox proportional hazard model indicated that the
preoperative serum CA 125 level [hazard ratio (HR), 2.356; 95%
confidence interval (CI), 1.271–3.570; P=0.011], postoperative
GnRH-a treatment (HR, 0.540; 95% CI, 0.241–0.873; P=0.017) and
accompanying endometriosis (HR, 2.182; 95% CI, 1.556–3.031;
P=0.003) were significant risk factors associated with dysmenorrhea
relapse following laparoscopic adenomyomectomy (Fig. 6).
Of the 7 nulliparous women, 3 had no desire to have
children and 2 underwent in vitro fertilization that failed.
Two patients (28.6%) became pregnant and experienced successful
childbirth during the 2-year follow-up period. Other parous women
did not attempt to become pregnant.
Discussion
Adenomyomectomy includes steps similar to those of
myomectomy, except that the margin between the tumor and
surrounding normal myometrium may not be as substantial as those of
myomectomy (10). This procedure is
suitable for patients presenting with focal-type adenomyosis, which
may be relatively clearly separated from adjacent normal tissue.
This type of surgery was performed during the present study. Other
researchers have attempted modifications including U-shaped
suturing, overlapping muscle flap suturing and the triple-flap
method (11). Cytoreductive surgery
involves the excision of diffuse adenomyosis and is similar to the
treatment of advanced ovarian cancer types. This procedure is
primarily useful when it is difficult to remove all adenomyotic
foci (1). The boundary between the
adenomyoma and myometrium was ill-defined. A recent review
indicated that recurrence rates of adenomyosis differed depending
on the extent of excision (12).
Different modifications include the transverse H incision
technique, wedge resection of the uterus and asymmetric uterine
dissection (13–15).
There are few reports on the factors that influence
the recurrence of adenomyosis. In the present study, it was
revealed that patients with adenomyosis with higher CA 125 levels
and accompanying endometriosis were more likely to experience the
relapse of dysmenorrhea following adenomyomectomy. Preoperative
serum CA 125 appeared to be a promising predictor of relapse, with
a cut-off value of 46.2 U/ml in the present study. CA 125 is a
glycoprotein derived from the embryonic coelomic epithelium and is
expressed by certain normal tissue types. High-serum CA 125 has
been commonly used as a biomarker for epithelial ovarian cancer
(16,17). Increased serum CA 125 serves as a
diagnostic tool for screening adenomyosis; however, it lacks
specificity in its ability to differentiate adenomyosis from other
diseases (18). Kil et al
(16) measured serum CA 125 in 2,149
women diagnosed with adenomyosis who underwent total hysterectomy
and revealed that it was promising in the differential diagnosis of
adenomyosis and leiomyoma at 19 U/ml, with a sensitivity of 66% and
specificity of 79.3%. Using 19 U/ml as a reference, there may be a
proportion of patients suitable for adenomyomectomy screened with a
serum CA level of 46.2 U/ml in clinical practice. Although the
mechanism of increased CA 125 is not yet fully understood,
inflammatory reactions, peritoneal irritation or peritoneal stretch
that alter endothelial permeability may allow CA 125 to reach the
circulation, thereby resulting in higher CA 125 concentrations
(17). In addition, the ectopic
endometrium was confirmed to secrete significantly higher CA 125
concentrations compared with the normal endometrium in patients
with adenomyosis (18). Furthermore,
serum levels of CA 125 were higher in moderate to severe cases of
endometriosis compared with in mild cases (19). A previous study revealed that
suppressing CA 125 may suppress the adhesion, invasion and
migration of ovarian cancer cells (20), thereby implying that CA 125 may
facilitate ectopic endometrium migration and adhesion in the
surrounding myometrium during adenomyosis development.
Postoperative GnRH-a was identified as an
independent factor influencing relapse in the present study. GnRH-a
therapy results in the decreased secretion of gonadotropin, which
results in the suppression of the hypothalamic-pituitary-gonadal
axis and ovarian function, and additionally results in
hypoestrogenism, which inhibits the proliferative action of the
myometrium (5). Entopic and ectopic
types of endometria of adenomyosis exhibit a series of molecular
and metabolic changes that increase angiogenesis and proliferation,
enhance local progesterone resistance and augment estrogen
production (7). Thereby, increasing
infiltration and excessive growth of endometrial stromal cells in
the junctional zone facilitates the establishment of adenomyosis
(21). GnRH-a therapy has been
demonstrated to reduce angiogenesis and inflammation and to induce
apoptosis in women diagnosed with adenomyosis (21). In the present study, 26 of 49 women
received 6 courses of GnRH-a therapy; and of this group, 11.5%
(3/26) experienced relapse at the end of the follow-up period
whereas 39.1% (9/23) experienced relapse in the surgical-only
treatment group. Instead of surgery alone, 6 courses of
postoperative administration of GnRH-a should be suggested to
prevent relapse following adenomyomectomy. It was considered that
the development of adenomyosis may be the consequence of
interactions between promotive and inhibitive factors. Promotive
factors including higher serum CA 125 concentrations, higher
estrogen production and resistance to progesterone may facilitate
adenomyotic pathological processes including the migration of
ectopic endometrium and proliferation of endometrial stromal cells
in the junctional zone. Inhibitive factors including GnRH-a therapy
and decreased estrogen production prevent this process (7). Therefore, it was hypothesized that
GnRH-a may curb this process and delay time to recurrence. Relapse
may be a matter of time due to exposure to a pathological
environment prior to menopause (22).
Patients with adenomyosis with accompanying
endometriosis compared with patients with accompanying myoma were
revealed to be more likely experience relapse in the present study.
Endometriosis shares a range of common features with adenomyosis,
from clinical manifestations to etiology (7). It was hypothesized that they were
different forms of the same pathogenesis; however, previous
evidence revealed specific distinct pathogenic pathways for
adenomyosis, suggesting that they were two different entities
(23). Compared with adenomyosis,
endometriosis appeared to be more frequent in young nulliparous
women, but adenomyosis occurred in relatively older and parous
women. One previous report states that adenomyosis and deep
endometriosis often coexist, particularly in women with infertility
or dysmenorrhea (24); however,
opposing views were held that adenomyosis and deep endometriosis do
not necessarily coexist (25,26) and the exact incidence of endometriosis
in adenomyosis remains unknown. Eight patients received LPSN during
adenomyomectomy in the present study. The relapse rates in the two
groups that received or did not receive this procedure were
similar, and no significant associations between performing LPSN
and relapse of pain were identified. One strategy for treating
dysmenorrhea and pelvic pain was to prevent the conduction of pain
to the nerve center. Uterine nerve ablation (UNA) and PSN were the
two most commonly used procedures. UNA involves cutting the nerves
along the uterosacral ligament. Although pelvic endometriosis often
coexists with adenomyosis, the efficacy of UNA may decrease over
time due to limited denervation (27). PSN involves cutting the presacral
nerve from the sacral promontory level; therefore, cutting more
nerves compared with UNA may be more effective for pain control.
Eight patients in the present study underwent PSN during the first
several years of the present study. Although PSN and UNA are
effective for alleviating pain, technical difficulties and
complications arise from affected visceral functions including
constipation or urinary urgency. Therefore, these procedures were
cautiously applied as adjuvant therapy in the present study.
The present study had a number of limitations. There
was the potential for patient selection bias due to the nature of
retrospective analysis. Patients with incomplete data were
excluded. Not all potentially confounding factors that may have
affected the outcomes were obtained from the onset. As a tertiary
referral institution, Beijing Chao-Yang Hospital of Capital Medical
University admitted patients with relatively complex conditions
more easily, whereas other less complicated patients may were
referred to other non-tertiary hospitals due to a referral bias.
Due to the degree of dysmenorrhea was based on the patient's
subjective judgment, and therefore differences in the experiences
of patients may have affected the results. In addition, a
relatively small number of samples and heterogeneity among subjects
may have limited the power of the statistical tests, resulting in
false conclusions.
In conclusion, adenomyomectomy may be the treatment
of choice in patients with adenomyoma who have lower preoperative
serum CA 125 levels and without accompanying endometriosis.
Acknowledgements
Not applicable.
Funding
The present study was supported by the International
Science & Technology Cooperation Program of China (grant no.
2012DFR30490).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WY and CL conceived and designed the study. WY, GL,
CL and ZZ acquired, analyzed and interpreted the raw data. ZZ
revised the manuscript critically for important intellectual
content. ZZ provided final approval of the version to be
published.
Ethics approval and consent to
participate
Approval for collection and publication of patient
data was obtained from the institutional review board of Beijing
Chao-Yang Hospital of Capital Medical University (Beijing, China;
reference no. EC1335097), and written informed consent was obtained
from all participating patients.
Patient consent for publication
The patient, or parent, guardian or next of kin
provided written informed consent for the publication of any
associated data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CA 125
|
cancer antigen 125
|
|
GnRH-a
|
gonadotropin-releasing hormone
agonist
|
|
LNG-IUS
|
levonor-gestrel-releasing intrauterine
system
|
|
LPSN
|
laparoscopic presacral neurectomy
|
|
ROC
|
receiver-operating characteristic
|
|
UNA
|
uterine nerve ablation
|
|
VAS
|
visual analogue scale
|
References
|
1
|
Struble J, Reid S and Bedaiwy MA:
Adenomyosis: A clinical review of a challenging gynecologic
condition. J Minim Invasive Gynecol. 23:164–185. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brosens I, Gordts S, Habiba M and
Benagiano G: Uterine cystic adenomyosis: A disease of younger
women. J Pediatr Adolesc Gynecol. 28:420–426. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Takeuchi H, Kitade M, Kikuchi I, Kumakiri
J, Kuroda K and Jinushi M: Diagnosis, laparoscopic management, and
histopathologic findings of juvenile cystic adenomyoma: A review of
nine cases. Fertil Steril. 94:862–868. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tahlan A, Nanda A and Mohan H: Uterine
adenomyoma: A clinicopathologic review of 26 cases and a review of
the literature. Int J Gynecol Pathol. 25:361–365. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pontis A, D'Alterio MN, Pirarba S, de
Angelis C, Tinelli R and Angioni S: Adenomyosis: A systematic
review of medical treatment. Gynecol Endocrinol. 32:696–700. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yavuzcan A, Başbuğ A, Baştan M, Çağlar M
and Özdemir İ: The effect of adenomyosis on the outcomes of
laparoscopic hysterectomy. J Turk Ger Gynecol Assoc. 17:150–154.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Garcia L and Isaacson K: Adenomyosis:
Review of the literature. J Minim Invasive Gynecol. 18:428–437.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Alabiso G, Alio L, Arena S, di Prun AB,
Bergamini V, Berlanda N, Busacca M, Candiani M, Centini G, Cello
AD, et al: Adenomyosis: What the patient needs. J Minim Invasive
Gynecol. 23:476–488. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Langley GB and Sheppeard H: The visual
analogue scale: Its use in pain measurement. Rheumatol Int.
5:145–148. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang PH, Liu WM, Fuh JL, Cheng MH and Chao
HT: Comparison of surgery alone and combined surgical-medical
treatment in the management of symptomatic uterine adenomyoma.
Fertil Steril. 92:876–885. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Grimbizis GF, Mikos T and Tarlatzis B:
Uterus-sparing operative treatment for adenomyosis. Fertil Steril.
101:472–487. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Younes G and Tulandi T: Conservative
surgery for adenomyosis and results: A systematic review. J Minim
Invasive Gynecol. 25:265–276. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fujishita A, Masuzaki H, Khan KN, Kitajima
M and Ishimaru T: Modified reduction surgery for adenomyosis. A
preliminary report of the transverse H incision technique. Gynecol
Obstet Invest. 57:132–138. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sun AJ, Luo M, Wang W, Chen R and Lang JH:
Characteristics and efficacy of modified adenomyomectomy in the
treatment of uterine adenomyoma. Chin Med J (Engl). 124:1322–1326.
2011.PubMed/NCBI
|
|
15
|
Nishida M, Takano K, Arai Y, Ozone H and
Ichikawa R: Conservative surgical management for diffuse uterine
adenomyosis. Fertil Steril. 94:715–719. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kil K, Chung JE, Pak HJ, Jeung IC, Kim JH,
Jo HH and Kim MR: Usefulness of CA125 in the differential diagnosis
of uterine adenomyosis and myoma. Eur J Obstet Gynecol Reprod Biol.
185:131–135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Seeber B, Sammel MD, Fan X, Gerton GL,
Shaunik A, Chittams J and Barnhart KT: Panel of markers can
accurately predict endometriosis in a subset of patients. Fertil
Steril. 89:1073–1081. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kobayashi H, Ida W, Terao T and Kawashima
Y: Molecular characteristics of the CA 125 antigen produced by
human endometrial epithelial cells: Comparison between eutopic and
heterotopic epithelial cells. Am J Obstet Gynecol. 169:725–730.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mihalyi A, Gevaert O, Kyama CM, Simsa P,
Pochet N, De Smet F, De Moor B, Meuleman C, Billen J, Blanckaert N,
et al: Non-invasive diagnosis of endometriosis based on a combined
analysis of six plasma biomarkers. Hum Reprod. 25:654–664. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bast RC Jr, Hennessy B and Mills GB: The
biology of ovarian cancer: New opportunities for translation. Nat
Rev Cancer. 9:415–428. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Khan KN, Kitajima M, Hiraki K, Fujishita
A, Sekine I, Ishimaru T and Masuzaki H: Changes in tissue
inflammation, angiogenesis and apoptosis in endometriosis,
adenomyosis and uterine myoma after GnRH agonist therapy. Hum
Reprod. 25:642–653. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jee BC, Lee JY, Suh CS, Kim SH, Choi YM
and Moon SY: Impact of GnRH agonist treatment on recurrence of
ovarian endometriomas after conservative laparoscopic surgery.
Fertil Steril. 91:40–45. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vannuccini S, Tosti C, Carmona F, Huang
SJ, Chapron C, Guo SW and Petraglia F: Pathogenesis of adenomyosis:
An update on molecular mechanisms. Reprod Biomed Online.
35:592–601. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gonzalez-Ramos R, Rocco J, Rojas C, Sovino
H, Poch A, Kohen P, Alvarado-Díaz C and Devoto L: Physiologic
activation of nuclear factor kappa-B in the endometrium during the
menstrual cycle is altered in endometriosis patients. Fertil
Steril. 97:645–651. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Naftalin J, Hoo W, Pateman K, Mavrelos D,
Holland T and Jurkovic D: How common is adenomyosis? A prospective
study of prevalence using transvaginal ultrasound in a gynaecology
clinic. Hum Reprod. 27:3432–3439. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Benagiano G, Brosens I and Habiba M:
Structural and molecular features of the endomyometrium in
endometriosis and adenomyosis. Hum Reprod Update. 20:386–402. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Johnson NP, Farquhar CM, Crossley S, Yu Y,
Van Peperstraten AM, Sprecher M and Suckling J: A double-blind
randomised controlled trial of laparoscopic uterine nerve ablation
for women with chronic pelvic pain. BJOG. 111:950–959. 2004.
View Article : Google Scholar : PubMed/NCBI
|